2002 Sept/October
36
Sept/October 2002 CANDIDATES VIEWS on Health Care Issues CANDIDATES VIEWS on Health Care Issues
-
Upload
twin-cities-medical-society -
Category
Documents
-
view
237 -
download
1
description
Candidates Views on Health Care Issues
Transcript of 2002 Sept/October

Sep
t/O
cto
ber
2002
C A N D I D AT E S V I E W Son Health Care Issues
C A N D I D AT E S V I E W Son Health Care Issues

The Group
The MMIC Group can orchestrate an array of finely tuned products and services.
We offer you complete malpractice insurance services as well as employee benefits planning, expert healthcare information
systems planning and implementation and an Internet-based medical services portal designed to meet your unique needs.
MMIC, making your life a little simpler...isn’t it about time. Call 1–800–328–5532, or visit us at www.midmedical.com
I N S U R A N C E E M P L O Y E E B E N E F I T S C O N S U L T I N G ( Technology & Strategic) T E C H N O L O G Y S O L U T I O N S
“THE FUSION OF DESIGNAND TECHNOLOGY”
IT’S NOT YOUR DADDY’SCADDY ANYMORE!
CONTACT STEVE ALLEN FOR DETAILS
2325 Prior Avenue North, Roseville, MN
(651) 636-6060
2003 CTS
2002 ESCALADE345 HP — The most powerful SUVon the road today!

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 1
V O L U M E 4 , N O . 5 S E P T E M B E R / O C T O B E R 2 0 0 2
Physician Co-editor Thomas B. Dunkel, M.D.Physician Co-editor Richard J. Morris, M.D.Physician Co-editor David L. Swanson, M.D.Managing Editor Nancy K. BauerAssistant Editor Doreen M. HinesHMS CEO Jack G. DavisRMS CEO Roger K. JohnsonProduction Manager Sheila A. HatcherAdvertising Representative Kirsten SchoellerCover Design by Susan Reed
MetroDoctors (ISSN 1526-4262) is published bi-monthly by the Hennepin and Ramsey MedicalSocieties, 3433 Broadway Street NE, BroadwayPlace East, Suite 325, Minneapolis, MN 55413-1761. Periodical postage paid at Minneapolis,Minnesota. Postmaster: Send address changes toMetroDoctors, Hennepin and Ramsey MedicalSocieties, 3433 Broadway Street NE, BroadwayPlace East, Suite 325, Minneapolis, MN 55413-1761.
To promote their objectives and services, theHennepin and Ramsey Medical Societies printinformation in MetroDoctors regarding activitiesand interests of the societies. Responsibility is notassumed for opinions expressed or implied insigned articles, and because of the freedom givento contributors, opinions may not necessarilyreflect the official position of HMS or RMS.
Send letters and other materials for considerationto MetroDoctors, Hennepin and Ramsey MedicalSocieties, 3433 Broadway Street NE, BroadwayPlace East, Suite 325, Minneapolis, MN 55413-1761. E-mail: [email protected].
For advertising rates and space reservations,contact: Kirsten Schoeller14953 Appaloosa Trail NEPrior Lake, MN 55372phone: (952) 440-2997fax: (952) 440-9662e-mail: [email protected].
MetroDoctors reserves the right to reject anyarticle or advertising copy not in accordance witheditorial policy.
Non-members may subscribe to MetroDoctors at acost of $15 per year or $3 per issue, if extra copiesare available. For subscription information,contact Doreen Hines at (612) 362-3705.
2 SOAPBOXClinical Skills Assessment Exam: A Student Perspective
3 Editor’s Message
U.S. Senate and Congressional Candidates’ Views on Health Care4 • Sen. Paul Wellstone
6 • Norm Coleman
7 • John Kline/and Index to Advertisers
8 • Rep. Bill Luther
9 • Rep. Jim Ramstad
10 • Rep. Betty McCollum
11 • Clyde E. Billington, Ph.D
12 • Rep. Mark Kennedy/and United Way
13 • Janet Robert
Candidates for Governor14 • Tim Pawlenty
15 • Tim Penny
16 • Ken Pentel
17 COLLEAGUE INTERVIEWTheodore Loftness, M.D.
20 Emerging from Immunization Chaos
22 Retirement Plan Options for Independent Medical Groups
RAMSEY MEDICAL SOCIETY
25 President’s Message
26 Benefits of Membership
27 New Members/In Memoriam/Free Hmong Audiotapes
28 RMS Alliance
HENNEPIN MEDICAL SOCIETY
29 Chair’s Report
30 Community Internship
31 HMS in Action
32 HMS Alliance
On the cover: Candidates for U.S.Senate, Congress and Governorpresent their views on healthcareissues. Related articles begin onpage 3. Photo by Tom Olmscheid,MN House Information Office.
MetroDoctorsT H E B U L L E T I N O F T H E H E N N E P I N A N D R A M S E Y M E D I C A L S O C I E T I E S
DoctorsC O N T E N T S
Sep
t/O
cto
ber
2002
C A N D I D AT E S V I E W Son Health Care Issues
C A N D I D AT E S V I E W Son Health Care Issues

2 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
P H Y S I C I A N ' S S O A P B O X
A
Clinical Skills Assessment Exam:A Student Perspective
AS AN ACTIVE MEMBER of the University of Minnesota AMAstudent group and the Hennepin Medical Society, I am privileged tobe on the cutting edge of issues facing students throughout theirmedical training. It is becoming apparent to me that my fellowstudents, as well as currently practicing physicians, are not up to speedon many of the same issues.
In particular, the discussions about the Clinical Skills AssessmentExam (CSAE) are slipping under the radar of many health careprofessionals. It is a model example of the need to be actively involvedwithin my profession.
The CSAE is a national standardized patient exam proposed bythe National Board of Medical Examiners (NBME). It utilizes aminimum of 10 scored cases, each lasting 30 minutes. The examassesses data gathering and communication skills as part of Step 2 ofthe United States Medical Licensing Examination (USMLE).
The NBME cites studies that find that poor communication,interpersonal skills, and general clinical skills have been correlated withmalpractice suits, lower treatment compliance, and lower patientsatisfaction. The CSAE is intended to reinforce the teaching of thesetraits as well as screen out physicians lacking competence in this area.
As of 2004, affecting the graduating class of 2005, the NationalBoard of Medical Examiners proposes a national standardized patientexam using the CSAE.
As a student, I agree with the National Board of MedicalExaminers’ concerns but not their approach to solving this problem. Ihave several points of contention:
• To do nothing but sit for the examination, there is a proposedcost of $975. In addition, students who must travel to one of fivenational testing sites nationwide (Minneapolis is NOT one ofthem) will incur other substantial costs.
• The cost-benefit analysis has yet to be empirically shown by theNBME. The data shown so far is from the mid to late 1980s andthe rest of their data is considered privileged and unavailable.
• Many medical schools have made significant curriculum changes(including the U of M) since the time of these studies. Mostnotably, more than 75 percent of LCME accredited schoolsalready offer a comprehensive Objective Structured ClinicalExamination (OSCE) that serves a similar purpose.
The AMA-Medical Student Section has offered its continuedsupport for the development of standardized curricula addressingclinical skills assessments, but we oppose the current NBME proposaluntil further research can be done with respect to the proposal’sefficacy and validity. I stand with my fellow students in this respect.
In my opinion, having the test incorporated into the accreditationof the medical school holds the school accountable for its educationalpractices as well as the individual student. When testing revealsindividuals who have not acquired their necessary clinical skills, it maybe important to examine the school’s teaching practices as well as theindividual. The national exam proposal does not offer this sameduality. Instead, it focuses merely on the individual student.
Even if the sole goal of the CSAE were to test individualshortcomings, an exam offered by the school would be able to servethe same ends without the extra cost burden to the students at large.
I do not intend to suggest that the comprehensive testing ofclinical skills is unimportant, but the current CSAE proposal stands along way from its intended goal. Instead, the current proposal ends upmerely adding financial burdens to students without improvingmedical education and care for our profession and the generalcommunity. It would seem rash to implement a program withoutaddressing these issues.
The background information in this article can be found in theAMA-Medical Student Section official statement on the CSAE at theAMA website at www.ama-assn.org. Opinions offered are notrepresentative of the University, the AMA-Medical Student Section, oranyone else but myself. Additional questions on this or other issues canbe sent directly to me at [email protected].✦
B Y A N D R E W D I E T Z ,M . D . / P h . D S t u d e n t , U n i v e r s i t y o f M i n n e s o t a

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 3
T
Editor’s Message
THIS EDITION of MetroDoctors focuses onthe candidates for governor and national office.It is fascinating to compare the candidates’ opin-ions. One gains insight to their opinions aboutissues, but also a feeling for how committedthey are to the issues. Are they for us, or againstus, and to what degree and with what passion?
As I review the responses to our surveysof the candidates, I find myself challenging mytraditional political allegiances. I think that Imight vote somewhat differently this Novem-ber than I have in years past.
Casting a vote in an election is the mostimportant task imposed upon us by our citi-zenship in this great land. I suspect that nearlyall of us who are physicians vote.
There is another duty of citizenship thatrepresentative democracy calls for that most ofus avoid. It is the duty of advocacy. We need tocommunicate with those who represent us.
Why don’t we do this? I think it is be-cause of the following two myths surroundinglegislative advocacy.
Myth 1: It is gonna cost me money.It is definitely true that giving money to a can-didate buys access, but not for you. You aren’tArthur Anderson, the NRA, or Planned Par-enthood. Your bucks are small change on theirgrand scale.
That’s OK. It doesn’t matter if you do notgive a candidate money. In fact, it is a violationof ethics for legislators to refer to donation listsin making their voting decisions.
What does matter, more than anythingelse, is that you vote. Your opinion, and that ofyour voting neighbors, is in fact the only thingthat matters when the vote is cast by your leg-islator. Truly, if you write to a legislator andyour zip code is not in the district served byyour legislator, your letter or e-mail is discarded
without even a look-see. If the zip code is right,your opinion is noted and seriously regarded.
What your legislator wants is to be elected.The only thing that gets him or her elected isvotes. The only way he or she gets votes is byresponding to the wishes of the voters.
Your power of influence is completely free.It costs you nothing.
(On the other hand, if your legislator isgood to you, there is nothing wrong with toss-ing in a few dollars for the next campaign.)
Myth 2: It is gonna require confrontation. I’mcompassionate! I hate confrontation!Getting your opinion registered is ridiculouslysimple. You can e-mail your legislator throughthe AMA website (even if you aren’t a mem-ber). You need simply to go to their legislativepage and enter your zip code.
Even easier is to call the local office of yourlegislator. Both Dayton and Wellstone, for ex-ample, have Twin Cities’ offices staffed by eageryoung workers anxious to justify their existence
by forwarding any message you give them. Theyare friendly (they want to leave a good impres-sion on the voters) and very accommodating.They want to hear from you, whether you arefor an issue or against. After a few calls, you mayeven get to know them on a first name basis.
Give them a call! It is so simple! You donot need to give any long-winded explanationof why you do or do not support something.They already have heard the arguments. Theyjust want to know how you think their bossshould vote. And you can tell them in two min-utes or less.
The truth be told, it is easier to call yourlegislator than it is to vote and takes less time.So when you hear of some issue affecting yourpatients or your practice, whether from HMSor RMS, the MMA or the AMA, the TV, or a“by the way” in the doctor’s lounge, hit yourlegislator’s phone number on your speed dialerand do your duty as a citizen. ✦
David L. Swanson M.D., can be reached at:[email protected]
Two Myths about Legislative AdvocacyDavid L. Swanson M.D.
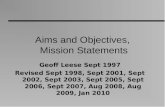
On July 10, 2002, the Hennepin and Ramsey Medical Societies co-sponsored an educational seminar titled,“Provider Roundtable: Public Policy Issues Affecting Consumers and Fair Provider Contracting.” Above arepictured from left, Jack Davis, Senator Dallas Sams, T. Michael Tedford, M.D., Representative Fran Bradley, andRoger Johnson. Senator Sams and Representatives Bradley and Lynda Boudreau (not pictured) were presentedcertificates of appreciation for their work and support of the fair health plan contracting legislative effort.

4 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Sen. Paul Wellstone(DFL)Candidate for re-electionto the U.S. Senate
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician re-imbursement?
I have long fought to fix the Medicare physi-cian payment system that is so terrible for Min-nesota. Currently, the physician fee schedule isprojected to lead to a decrease of nearly 20 per-cent over three years. This would have catastrophicconsequences for the Minnesota health caresystem, and the payment cuts must be restored.
Because of the devastating impact of thephysician fee schedule cuts, I am cosponsoringS.1707, the Medicare Physician Payment Fair-ness Act. This legislation would stop the cur-rent physician payment cuts for 2002. I am also
working with my colleagues on the Senate Fi-nance Committee to make sure that future pay-ment cuts don’t happen. More importantly, Iam fighting to increase physician reimburse-ment. I do not support H.R. 4954 because theprescription drug benefit is inadequate. I supportthe physician fee schedule provisions included inthe bill and am advocating for an increase in phy-sician payment of at least 6 percent.
H.R. 4954 includes a prescription drug benefitfor Seniors. Do you support the drug benefitprovisions of H.R. 4954? Please explain yourposition and if you do not support H.R. 4954,please describe an alternative drug benefit thatyou could support.
I strongly support providing a prescription drugbenefit under Medicare, as was promised whenMedicare was created more than 40 years ago.In the Senate, many of my colleagues and I haveworked to develop a prescription drug benefitthat provides meaningful coverage to seniors.The Medicare Outpatient Drug Act (S. 2625)adds complete coverage of prescription drugsto Medicare – with no gaps or limits. The cov-erage would begin in 2004, the first year thebenefit is offered.
The benefit under S. 2625 would be inte-grated into the Medicare program to ensure itsavailability to all beneficiaries. Access to pre-scription medicines is guaranteed by S. 2625to every region of the country.
Seniors would pay a low monthly pre-mium of $25. Assistance would begin with thefirst prescription filled – beneficiaries would payno more than $10 for generic medications, and$40 for medically necessary brand-name medi-cations. And it’s possible that these co-payscould be even lower through price negotiationswith pharmaceutical makers. After a seniorspends $4,000 on medicine out of his/her own
pocket, Medicare would pick-up any remain-ing expenses – he/she would pay nothing more.
Beneficiaries with incomes below 135 per-cent, of poverty, about $12,000, would receivefull assistance for their drug premiums and cost-sharing. Those with incomes from 135 percentto 150 percent of poverty would pay a reducedpremium on a sliding scale basis.
Under S. 2625, seniors know what they’llpay and they know what benefits they’ll get.This plan is the real prescription drug benefitthat seniors need.
I do not support the drug benefit in theH.R. 4954 plan. In my view, it fails in threeways to provide seniors with the help they needto buy their medicines. First, this plan does notadd a prescription drug benefit to Medicare.Instead, H.R. 4954 throws money at privatehealth insurance plans and Medicare HMOs,trying to induce them to offer prescription drugcoverage to seniors. Yet the insurance industryhas repeatedly stated that it does not want toprovide a drug-only insurance product. Evenif some insurers do offer coverage, they wouldlikely come in and out of the market or moveto profitable market areas. It is highly probablethat this would result in the same pullouts anduncertainty that we see in Medicare managedcare today.
Second, nowhere in H.R. 4954 does itstate that the monthly premium is $35 or thatthe deductible will be $250. These are meresuggestions, and the plans could charge seniorswhatever premium and deductible they want.That means seniors would not be able to counton a guaranteed premium or even a guaran-teed plan.
Third, H.R. 4954 does not provide com-plete coverage. Seniors would be forced to paythe full cost of their medicines when their outof pocket spending reaches $2,000. The govern-ment would only pick up the cost of their pre-scriptions when their spending reaches $3,700.So seniors would continue to pay a monthlypremium when their spending reaches $2,000,yet they would receive no help from the gov-ernment to pay their medicine bills until theyspend $3,700 out of their own pockets.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you support
U.S. Senate and CongressionalCandidates’ Views on Health Care
Editor’s Note: Following are the responses pro-vided by the candidates for U.S. Senate andCongress. Representative Martin Sabo is not rep-resented here as he did not respond to our nu-merous requests.

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 5
legislation that equalizes the balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans. Why or why not?
The managed care system desperately needs tobe reformed. Physicians and consumers are frus-trated with a managed system that takes deci-sions out of the hands of medical professionals.It is not healthy for any group to have virtuallyunlimited power over a matter as significantand sensitive as the kind of medical treatmentneeded by an individual with an illness or in-jury. I support legislation that equalizes thebalance of power and that would put medicaldecision-making in the hands of physicians andpatients rather than large health plans prima-rily interested in profits.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
A real prescription drug benefit, parity in cover-age for mental health, and helping small busi-ness provide health coverage for their employeesare major areas I am working in now. Some ofthis work may indeed continue into the newyear, and then the outcome will depend onwhich party controls the U.S. Senate.
But perhaps the most pressing issue fac-ing us in the future is finally figuring out a wayto cover the medically uninsured. Researchshows that people with health care coverage arefar more likely to receive necessary care andhigher quality care, yet 39 million Americansdo not have any health insurance to help paytheir medical bills.
My contribution to the debate about howwe achieve universal coverage is the Health Se-curity for All Americans Act (S. 2888). This leg-islation is designed to reach the goal of universalhealth care coverage by allowing states to decidehow to provide affordable and comprehensivehealth care coverage to all Americans within aspecific timetable. The bill insures the unin-sured and guarantees affordable health care bylimiting out-of-pocket expenses. A central fea-ture of the Health Security for All AmericansAct is the promise of comprehensive care byguaranteeing a minimum benefit package equalto that enjoyed by Members of Congress. Thebill also ensures quality of care by providingstrong patient protections. ✦
Sen. Wellstone can be reached at 651/310-9831.
MARK YOUR CALENDAR
SEPTEMBER 200226-27 Advanced Life Support in Obstetrics
(ALSO)Chair: Kimberly Petersen, MDPillsbury Auditorium, HCMC17.0 Credit Hours
OCTOBER3-4 18th Annual Forensic Science Seminar
Chair: Kathryn Berg, MDPillsbury Auditorium, HCMCApprox. 12.0 Credit HoursJointly sponsored with MN Coroner’s Assoc. and Hennepin County Medical Examiner
17-19 32nd Annual Orthopaedic and Trauma SeminarChair: Richard Kyle, MDMinneapolis Convention Center20.0 Credit Hours
NOVEMBER 1 HIV Care Conference
Co-Chairs: Hanan J. Rosenstein, MDRonald L. Schut, MD
Abbott Northwestern Hospital7.0 Credit HoursJointly sponsored with Allina Hospitals & Clinics
22 Paradox of PrematurityCo-Chairs: Richard Lussky, MD
Virginia Lupo, MDRadisson Metrodome, Minneapolis6.0 Credit HoursJointly sponsored with March of Dimes, MN Chapter
DECEMBER 13 11th Annual Family Practice Update
Chair: Charles Anderson, MDRadisson Hotel, RosevilleApprox. 7.0 Credit Hours
For more information, please call HCMC Continuing Medical Education
at (612) 347-2075. Fax (612) 904-4210. Toll Free 888-263-4262.
www.hcmc.org

6 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Norm Coleman (R)Candidate to the U.S. Senate
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician reim-bursement? Please explain your position.
We need to strengthen our Medicare system toreflect the growing needs of today’s seniors andto prepare the program for us aging babyboomers.
America has the greatest medical systemin the world. We have the best physicians, bestmedicines, best hospitals and best clinics. It isno coincidence that in the last decade, Ameri-cans won 17 of the 22 Nobel Prizes in Medi-cine.
Our Medicare system should maximize se-niors’ access to medicine and doctors. It shouldstrengthen physicians’ ability to do their jobsand increase choices without allowing the gov-ernment to intrude on the physician-patientrelationship. I support H.R. 4954 but there aregaps in coverage and we need to move forwardin a bipartisan manner to provide a universal,comprehensive prescription drug benefit forMinnesota seniors.
Increasing physician reimbursement iscritical to maintaining the high quality of carewe expect from our medical profession. Min-nesota physicians are at a distinct disadvantageto other parts of the country under the currentsystem and consistently struggle just to coverthe cost of care.
While H.R. 4954 raises the physician re-imbursement rate over the next three years,there remain systemic issues concerning howthe reimbursement is distributed that must beaddressed. I will fight to ensure that future re-
imbursement rates reflect a more equitable, rea-sonable rate relative to return.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefitprovisions of H.R. 4954? Please explain yourposition and if you do not support H.R. 4954,please describe an alternative prescription drugbenefit that you could support.
In July, I joined President Bush at a special eventin Minneapolis where the President emphati-cally declared: “Too many of our seniors areforced to choose between paying for their pillsor paying basic bills. That’s not right in America.”
I couldn’t agree more. With my two par-ents on prescription drugs, this is a very realissue for me.
Medicare is almost 40 years old, yet itsnever faced a major improvement of provisions.And it shows. The program is no longer ad-equately equipped to address the growing pre-scription drug needs of Minnesota seniors.
For a prescription drug benefit to reallymake a difference, it must be accessible, afford-able, and empower Minnesota seniors and theirdoctors. Our Medicare system should allowseniors and doctors to make health care deci-sions by maximizing choices and filling indi-vidual needs.
To this end, H.R. 4954 is a good first steptoward strengthening Medicare.
As of this writing on July 31, it is unfor-tunate that partisan politics has hindered evena modest solution for seniors dealing with ris-ing drug costs.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you supportlegislation that equalizes that balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not.
I am interested in this issue and want to learnmore about it. There are concerns with amend-ing anti-trust laws for physicians and how thatwill impact access and health care costs for con-sumers. I understand there are options such asclinical integration that may help provide col-
lective bargaining leverage for physicians. I amopen to working with physician groups to im-prove and strengthen their position with respectto health care corporations. My record as Mayorof St. Paul is one of bringing people togetherand getting things done.
The people at the table may not alwaysagree, and they may not always agree with me,but I am willing to work with all the parties todo what is best for Minnesota.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
While I hope Congress will address the issue ofprescription drugs before it recesses this year,many senators have been unable to work to-gether, jeopardizing the hope for reform this year.
The issue of prescription drugs has rami-fications for everyone involved in Americanmedicine, whether it is the seniors that receivecare or the doctors that provide it. We needleaders who can bring everyone to the table andget the job done.
I think the prescription drug plan passedby the House is a good first step towards strength-ening Medicare. But, more must to be done.Future legislation should encourage marketsolutions and promote private-public partner-ships. The government should give doctors andpatients, not bureaucrats in Washington, thepower to decide what kind of health care is best.
It is also time Washington address the re-gional discrepancies in Medicare reimbursementthat unfairly discriminate against Minnesota.This discrepancy disproportionately affects ac-cess and quality of care in rural Minnesota.
Also on the table should be the patientbill of rights and cost containment. One of themajor factors contributing to health care costsis medical malpractice liability. Congress needsto address comprehensive tort reform, includ-ing capping attorneys’ fees and limiting puni-tive damage awards, that will help restore somebalance and reduce health care costs. These areissues that will change the shape of thehealthcare system. They are issues that requiremore thought than partisanship which I willbring to Washington. ✦
Norm Coleman can be reached at 651/645-0766.

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 7
We want you to.For over 20 years, Minnesota Healthcare Network has servedphysician groups throughout the Twin Cities and neighboringcommunities. We represent the interests of our member clinics in acompetitive and increasingly complex marketplace. We provide avehicle for independent clinics to contract and have good workingrelationships with health plans and other purchasers. We haveinnovative and comprehensive data systems that provide soundinformation, which allows our physicians to make wise medical andbusiness decisions.
Our members are independent primary care (FP/GP, IM, Peds) andmulti-specialty medical groups. We are physician-owned andgoverned. Over 50,000 health plan members have their careprovided and coordinated by our independent physicians. Thisallows us to meaningfully advocate for our physician members andtheir patients in an era of health care where advocacy for theseconstituents is increasingly necessary.
If you are in private practice, or were and may be reconsidering thatoption, please contact us to find out how MHN may benefit you.
If your medical practice is interestedin information about joining the MHN
care system please contact:
Minnesota Healthcare Network, LLC
7900 International Dr.,
Suite 1080
Bloomington, MN 55425-1510
Phone (952) 883-3150
Fax (952) 883-3134
E-mail [email protected]
www.mhcn.com
Doctors — do you want to be independent?
Do you want to stay independent?
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician re-imbursement? Please explain your position.
I support the direction that H.R. 4954 is try-ing to take Medicare, but I would like to seemore direct payments to hospitals in rural areasto ensure that they can keep up with changing
John Kline (R)Candidate in the2nd Congressional District
medical improvements. I am also in favor ofpersonal accounts for seniors that can havefunds roll over year to year. I do support physi-cian reimbursement. Our care providers needto be compensated for the work they performand need to have the confidence that they willbe paid for services rendered.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefitprovisions of H.R. 4954? Please explain yourposition and if you do not support H.R. 4954,please describe an alternative prescription drugbenefit that you could support.
We need to do something to help seniors withthe rising costs of prescription drugs. Prescrip-tion drugs ought to be covered by Medicare.What we have today is ridiculous. Medicare willcover surgery to fix an ulcer or other stomachproblems. But it won’t cover the drugs thatwould prevent the ulcer. That just doesn’t makesense and we need to change it. Medicare wasdesigned decades ago and we need to take ad-vantage of significant advances made in health,like the benefits of preventative drugs.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you supportlegislation that equalizes that balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not.
While I understand that physician anti-trustlaws are an important and complicated issuethat must be studied and analyzed, I have notyet finalized my position on this issue.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
We need to find a way to help more Americansfind affordable health insurance to protectthemselves and their families. ✦
John Kline can be reached at 952/846-0808.
September/OctoberIndex to Advertisers
Allina Education Services .......................... 16
Brainerd Medical Center ........................... 21
Classified Ads ........................................... 10
Crutchfield Dermatology .......................... 13
DAMARCO ............................................... 8
HCMC CME ............................................. 5
HealthEast Vascular Center ....................... 23
Methodist Hospital .................................... 9
Minnesota Healthcare Network .................. 7
MMIC ............................. Inside Front Cover
Multicare Associates ................................... 24
NIH web-based CME ............................... 11
Raymond James Financial .... Inside Back Cover
RCMS Inc. ............................................... 15
RiverWay Clinics ...................................... 19
U of M CME ................. Outside Back Cover
Wally McCarthy Cadillac ... Inside Front Cover
Wally McCarthy Hummer .... Inside Back Cover
Weber Law Office ..................................... 11

8 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Rep. Bill Luther (DFL)Formerly represented the 6th
District, and now is a Candidatein the 2nd Congressional District
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician re-imbursement? Please explain your position.
I support a 6 percent increase in physician reim-bursement to help ensure physicians’ contin-
ued ability to provide high quality care underMedicare. That is why I am an original co-sponsor of the Medicare Physician PaymentFairness Act, which would amend the currentpayment structure and require a study to designa new formula without the current flaws. I didnot support H.R. 4954 because it failed to pro-vide seniors with an affordable, reliable prescrip-tion medicine benefit.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefit pro-visions of H.R. 4954? Please explain your posi-tion and if you do not support H.R. 4954, pleasedescribe an alternative prescription drug ben-efit that you could support.
I have serious concerns with H.R. 4954’s pre-scription benefit. For example, this bill wouldcover less than 25 percent of Medicare benefi-ciaries’ estimated prescription drug costs overthe next 10 years and would pay nothing forcosts between $2,000 and $3,700. Addition-ally, there is no guaranteed premium so actualpremiums could vary among plans. It would
allow private plans to vary price, benefit de-sign, and availability of drug coverage all acrossthe country. This means that a senior in Floridamay pay a different premium than a senior inMinnesota for the exact same benefit. Instead,I support an alternative that offers all seniors abenefit that truly assists them with prescrip-tion drug costs, without any gaps in coverageor geographic disparities.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you supportlegislation that equalizes the balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not?
I believe that Congress must approach changesto antitrust laws very carefully, as these lawswere designed to protect individual consum-ers. At the same time, I also believe it is impor-tant that physicians are not forced to signcontracts that are unfair to them and to pa-tients. Therefore, I would need to study thedetails of any specific proposal before I couldsupport or oppose it.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
It is difficult to say what will be the most impor-tant health care issue in the new year becausethere is still important work to be accomplishedthis year. It is my hope that we will be able towork out an acceptable compromise on a pre-scription medicine benefit before Congress ad-journs, but if we cannot, this will be even morecritical next year.
I am committed to continuing my workon eliminating the current geographical dispari-ties in Medicare rates next year. Until Minne-sota seniors enjoy the same benefits at the samelow cost as seniors nationwide, this will be atop health care priority for me. ✦
Rep. Luther can be reached at 651/730-4949.
� ��������� ���������������������
�������������� �������������
��������������� ��������
���� ��������������������!���
���������������� "
� ������������� �#����
�$������������� ������������� �
����##�����##�������$����� �
����%�##�������������"
� &��� ����������������������
���!�������� "
� '������������� �#�������������#�$
��������������"
� (� �#������������������������
�����������������������#�������
�!���������� �����������������
�����������#��������� ��$������"
� ���������������)**�***���+���
�������� ������������"
Need HelpManaging
YourMaterial
Safety DataSheets
(MSDS)?
������������������
������
������������
���������������������
��������
�������������
����� ���!"#"$%&'
(�) �����
(((����������

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 9
Rep. Jim Ramstad (R)Candidate for re-election in the3rd Congressional District
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician reim-bursement? Please explain your position.
I strongly support H.R. 4954 and the 6 percentincrease in payments to physicians included inthe bill. We all know the current formula isnot an accurate measure of physician costs andleads to arbitrary and irrational reimbursementrates. I believe the provisions in H.R. 4954 area good first step in moving toward fair reim-bursement for physicians and set the stage forcomprehensively reforming the physician reim-bursement formula.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefit provi-sions of H.R. 4954? Please explain your positionand if you do not support H.R. 4954, pleasedescribe an alternative prescription drug ben-efit that you could support.
I strongly support the prescription drug benefitincluded in H.R. 4954. Out-of-pocket drugcosts for the average senior will be reduced by$940 under this plan, or 44 percent less thanwhat they are currently paying. Additionally, 17percent of beneficiaries use 55 percent of allthe prescription drugs consumed by the Medi-care population, which makes the “stop-loss”coverage in the bill very significant to this smallgroup of high spending individuals. And par-ticipation in this plan is completely voluntary, soseniors with nominal drug expenses can decidefor themselves whether to participate in the plan.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you supportlegislation that equalizes the balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not?
While well intentioned, I do not believe collec-tive bargaining is the best method for improv-ing the quality of health care in this country.
In testimony before the Judiciary Com-mittee during Congressional debate on this is-sue, Joel Klein, former Assistant AttorneyGeneral, Antitrust Division at the Departmentof Justice (DOJ), said, “It has become clear overthe years that consumer welfare and patientchoice are best preserved by relying on anti-trust principles to assure the proper operationof health care markets just as they are in other
markets. Permitting providers to form bargain-ing groups in response to perceived bargainingleverage by insurers will not decrease the costof health care or increase the quality of patientcare.”
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
The health agenda for the next Congress willbe largely determined in the upcoming months,as the Senate continues to struggle to pass aprescription drug benefit. If prescription druglegislation is not signed into law this year, pro-viding prescription drug coverage under Medi-care will continue to be our top priority. Also,although we are closer than we’ve ever been toseeing a Patients’ Bill of Rights enacted, it ap-pears this issue will continue in the next Con-gress and remain a leading health care priority.✦
Rep. Ramstad can be reached at 952/738-9100.
Think you have an eating disorder?We can help.
The Eating Disorders Institute (EDI) offersinpatient, partial-day and outpatient programsin a newly expanded space. EDI is a partnershipwith Methodist Hospital and University ofMinnesota physicians.
Call for information — 952-993-6200
6490 Excelsior Blvd.St. Louis Park, MN 55426www.parknicollet.com

10 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Rep. Betty McCollum(DFL)Candidate for re-election in the4th Congressional District
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician reim-bursement? Please explain your position.
I voted against H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act, the Re-publican proposal to subsidize private insuranceplans in hopes that they will offer prescriptiondrug coverage to Medicare beneficiaries. Thislegislation included several Medicare reimburse-ment changes, including the 6 percent increasein physician reimbursement.
While I couldn’t support H.R. 4954 be-cause it failed to provide a guaranteed Medi-care prescription drug benefit for all seniors, Istrongly support an increase in physician reim-bursement.
I am a cosponsor of H.R. 5019, the Demo-cratic Medicare Prescription Drug Benefit and
Discount Act, which included the same 6 per-cent increase in physician reimbursement, aswell as H.R. 3351, the Medicare Physician Pay-ment Fairness Act. H.R. 3351 would reduce thescheduled 5.4 percent cut to 0.9 percent instead,and would order the Medicare Payment Advi-sory Commission to come up with a new pay-ment formula in time for 2003. I also joinedseveral of my colleagues in sending a letter toSpeaker Hastert requesting that he ensure thatthe House take steps to prevent these devastat-ing cuts from going into effect next year. Con-gress must act to freeze the current physicianpayment rate or reduce the scheduled cut untila new, more appropriate formula can be devel-oped. If the House leadership is serious abouttaking action on this measure, we must passthis increase in physician reimbursement out-side of controversial legislation like H.R. 4954,to ensure that the bill will pass both Housesand be signed by the President. Please knowthat I will continue to work with my colleaguesin Congress to keep these cuts from going intoeffect.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefit pro-visions of H.R. 4954? Please explain your posi-tion and if you do not support H.R. 4954, pleasedescribe an alternative prescription drug ben-efit that you could support.
I voted against H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act becauseI oppose the proposed House Republican drugplan to provide prescription drug benefits toMedicare members through private insurers.Half of Minnesota seniors today have no pre-scription drug coverage because private insur-ers won’t offer policies because it is unprofitablefor companies to do so. Due to unfair reim-bursement formulas for health care providers,Medicare beneficiaries in other parts of thecountry enjoy substantially more benefits fromMedicare HMOs, such as prescription drug cov-erage or eyeglasses. Unfortunately, the Republi-can plan does nothing to address this inequityand will simply ensure that Florida seniors con-tinue to enjoy prescription drug benefits whileinsurance companies refuse to offer a compre-hensive benefit for Minnesota seniors.
The Democratic bill I’m a sponsor of pro-vides that for a voluntary drug premium of $25
per month the government will pay 80 percentof drug costs after a $100 deductible. And nosenior will have to pay more than $2,000 incosts per year. On top of that, we will be arm-ing seniors with real protection from soaringdrug costs. With forty million seniors bandedtogether under the buying power of Medicare,we can begin to use the bargaining power torein in high drug prices. Unfortunately, theHouse Republican leadership continues to denymembers a vote on this legislation.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you supportlegislation that equalizes the balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not?
I support legislation to allow physicians to col-lectively negotiate contracts with health plans.The dangers posed by the ever-increasing con-solidation in the health insurance and managedcare market are exacerbating the practice ofhealth insurers engaging in heavy-handed ne-gotiating tactics and requiring exclusionarycontractual commitments from health care pro-viders. These restrictive contractual terms arefrequently proffered on a “take it or leave it”basis to health care providers, under the threatof the loss of the provider’s patients or exclusionfrom their access to other patients. By allowingphysicians to negotiate with health plans, wecan improve patient care and return medicaldecision making to physicians and patients,where it belongs.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
Unfortunately, the most important health careissues facing Congress next year will likely bethe same issues facing our nation this year.Patient’s rights legislation remains stalled overpartisan issues and the House Republican pre-scription drug legislation is simply an emptypromise. ✦
Rep. McCollum can be reached at 651/603-1505.
Billing Headaches? We Can Help!Medical Billing Professionals is a fullpractice management billing center,providing professional, comprehensiveand cost-effective billing services tohealthcare providers. Call (320) 963-8034 today — and take control of yourbilling! Visit us at:www.medical-billing-professionals.com.
Classified Ads

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 11
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician reim-bursement? Please explain your position.
I do support H.R. 4954, the Medicare Mod-ernization and Prescription Act. Physician re-imbursement has been frozen for several yearsas a way of controlling Medicare costs. Thereare other means of keeping costs under controlwithout denying physicians fair compensationfor their work. Many young doctors have hugestudent loans that they must pay back, andmany of them have also delayed having fami-lies and buying houses while in medical school.They must be fairly compensated once they fin-ish their years of education and internships.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefit pro-visions of H.R. 4954? Please explain your posi-tion and if you do not support H.R. 4954, pleasedescribe an alternative prescription drug ben-efit that you could support.
I do support the prescription drug benefit inH.R. 4954. My father died of cancer three yearsago, and I know how expensive drugs can be.My mother’s only income is from Social Secu-rity. She is now healthy, but I do worry abouthigh prescription drug costs, if she should be-come ill.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair toboth patients and physicians. Will you supportlegislation that equalizes the balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not?
Yes, I strongly support the right of physiciansto negotiate contracts with these huge healthcare organizations. Even though I am a Repub-lican, I come from a union family. I look onthe right to negotiate a labor contract as a basicright. Antitrust laws that limit the right to ne-gotiate should be repealed. My daughter is aregistered nurse working in a hospital, and shehas frequently complained about the heavy –and growing– workload placed on nurses. Shealso says that R.N.s often have such a heavyworkload that it poses a danger to patients. Iknow that the same is true of physicians and oftheir workloads at many of these huge healthcare organizations. The right to negotiate wouldsolve many of these problems.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
I am concerned about the intrusion of thesehuge health care organizations into the physi-cian-patient relationship. About eight years ago,my sister-in-law had cancer, and her physicianprescribed a treatment that was not covered byher medical plan. She appealed to her healthcare organization and was turned down. Sheeventually discovered that the person whoturned down her request was an administratorin another state who had no medical educa-tion at all. After a great effort, she got the pre-scribed treatment and is still alive today. I amalso concerned about the growing cost of liti-gation for the entire medical profession. Somemethod, other than lawsuits, must be devel-oped to compensate those who are accidentallyinjured. The many lawsuits being filed todayare driving up health care costs. Physicians arebeing forced to practice defensive medicine asa way of protecting themselves, and this alsocontributes to higher medical costs. ✦
Clyde E. Billington, Ph.D can be reached at651/493-6541.
Clyde E. Billington, Ph.D(R)Candidate in the4th Congressional District
WEBER LAW OFFICE
Focusing on the legal needs of the
health professional! • Licensure • Employment Law • Trial Work • Wills and Estates
• Regulatory Compliance
Michael J. Weber, J.D. • Former Attorney for the Board of Medical Practice
• Over Six Years as an Assistant Attorney General
612-296-8080
www.weber-law.com
“Committed to the Best Legal Outcome Possible Through Diligence and Resourcefulness!”
will be available on the NIH Clinical CenterWeb Conference Hall between June 17 andDecember 6, 2002. The course is co-presented by NIH Institutes – NHLBI andHIAID. Faculty from NHLBI are Joel Moss,M.D., Ph.D. and Stewart J. Levine, M.D.Faculty from NIAID is Calman Prussin,M.D. The course will discuss the most currentguidelines for diagnosing asthma andclassifying its severity, the stepwise approachto asthma management, the appropriate useof new asthma medications, the latest NIHresearch and future treatment trends.Participants must have an Internetconnection, a Web browser, and AdobeAcrobat Reader (which can be downloadedfree of charge on the conference centerwebsite). There is no charge to participate.Up to 4.5 AMA PRA category 1 credits willbe awarded electronically. To complete thecourse, go to www.frontlinemeded.org. Formore information, call 1-800-393-5936 orTTY line 301-572-0202.
A web-based CME course,“Gaining Control of Asthma:
Diagnosis, Management,and New Therapies”

12 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician re-imbursement? Please explain your position.
Yes, I am a co-sponsor of H.R. 4954, whichthe House passed in June. This provides a re-
sponsible approach, within budget, to help curbthe expense for prescription drug costs andhelps with reimbursement rates for providers,including physicians. There is more to do tostrengthen Medicare, but this bill is a good start.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefitprovisions of H.R. 4954? Please explain yourposition and if you do not support H.R. 4954,please describe an alternative prescription drugbenefit that you could support.
I am a member of the Speaker’s PrescriptionDrug Action Team and am proud to havehelped craft the prescription drug benefit in-cluded in H.R. 4954. This bill ensures that se-niors will not be forced to choose between foodand medicine and deplete their life savings tobuy life-saving prescriptions.
Antitrust laws now prevent physicians fromcollectively negotiating contracts with healthplans. Physicians are forced to sign contractswith billion dollar, giant health care corpora-tions that include provisions that are unfair to
Rep. Mark Kennedy (R)Formerly represented the 2nd
District, and now is a Candidatein the 6th Congressional District
both patients and physicians. Will you supportlegislation that equalizes the balance of powerby providing relief from antitrust and allow-ing physicians to collectively negotiate contractswith health plans? Why or why not.
I support restoring the doctor/patient relation-ship in a way that does not raise costs or reducethe physicians’ ability to provide quality care.In order to achieve this, I will evaluate legisla-tion that gives physicians the freedom to carefor their patients.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
The most important health care issues facingCongress are strengthening Medicare and add-ing a prescription drug benefit for seniors, elimi-nating the payment disparities that haveplagued Medicare for years, and enacting com-mon sense medical liability reform that is chas-ing too many physicians out of the professionand driving up health costs. ✦
Rep. Kennedy can be reached at 763/682-6898.
FOR YEARS, GREATER TWIN CITIES UNITED WAY has beencommitted to fortifying the health of the local community by help-ing patients before they arrive at your waiting room.
The support of both HMS and RMS physicians is essential inUnited Way’s many health initiatives, because the hard work we do isonly as strong as the doctors that help us share knowledge with thecommunity. For this reason, United Way has several health-relatedinitiatives that depend on the expertise of health care professionals.• United Way Success By 6® is an early childhood development
initiative, focused on providing parents the necessary tools toraise healthy children.
• The Healthy Learners “No Shots, No School” partnership withMinneapolis public schools dramatically increased the immu-nization levels of school-age children in two years.
• New Vistas High Schools connects pregnant teenagers withPediatric Resident volunteers who teach them prenatal care whilestressing the importance of personal physicians.
• Healthspeak™ is a health education curriculum, begun byUnited Way, that brings health care professionals into classrooms
to educate students on health matters. In 2000, almost 200medical professionals volunteered, reaching approximately110,600 fourth-grade and fifth-grade students. United Waypartner, the Minnesota Red Cross, now handles its operations.Nurses from the Minnesota Visiting Nurse Agency visit thou-
sands of seniors and people with disabilities every year. United Wayalso funds health-based programs through its network of agencies.
We know that you see hundreds of people in your waiting roomsevery day. We want to help the ones you don’t see. Without assis-tance from doctors like you, we could never have begun to servethose people. And without help from donors like you, we will neverbe able to continue helping those people.
Past donations from physicians like you have been instrumentalin the procedure and maintenance of the programs mentioned. Pleasecontinue to help your community. You can mail your gift to UnitedWay Gifts, 404 South Eighth Street, Minneapolis, MN 55404 orgive a secure gift online at www.unitedwaytwincities.org. Call (651)290-4590 to donate by phone. Help us help those outside the wait-ing room. Thank you. ✦
Continue Your United Way Giving

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 13
Janet Robert (DFL)Candidate in the6th Congressional District
Do you support H.R. 4954, the Medicare Mod-ernization and Prescription Drug Act whichincludes a 6 percent increase in physician reim-bursement? Please explain your position.
I believe the provision of H.R. 4954 to increasephysician reimbursements must be done becauseit is essential, but I do not support a bill thatwould create a “stand alone” prescription drugprogram from the existing Medicare program.
H.R. 4954 includes a prescription drug benefitfor seniors. Do you support the drug benefit pro-visions of H.R. 4954? Please explain your posi-tion and if you do not support H.R. 4954, pleasedescribe an alternative prescription drug ben-efit that you could support.
While I support the spirit of H.R. 4954 to cre-ate affordable prescription drug coverage, I be-lieve Congress should enact a prescription drugplan that is under the existing Medicare pro-gram.
Any attempt to enact a prescription drugbenefit under Medicare is complicated by thefact that we are once again running deficits dueto a slowed economy. Any honest discussion ofcreating affordable prescription drug coveragefor seniors will need to address where sources ofrevenue to fund the new benefit will be found.This will be a difficult task in our current bud-get environment but we must find a way to doit even if it is a scaled down version.
Antitrust laws now prevent physicians from col-lectively negotiating contracts with health plans.Physicians are forced to sign contracts with bil-lion dollar, giant health care corporations thatinclude provisions that are unfair to both pa-tients and physicians. Will you support legisla-tion that equalizes the balance of power byproviding relief from antitrust and allowingphysicians to collectively negotiate contracts withhealth plans? Why or why not.
I appreciate that physicians are concerned aboutthe increasing influence of HMOs in health care.Furthermore, I understand that this dynamicmay make it difficult for physicians to best ad-vocate for their patients. Where patients arebeing harmed by lack of access to health care,
physicians must have some recourse perhapsthrough a stronger patient’s bill of rights.
What do you think will be the most importanthealth care related legislative agenda facingCongress in the new year?
I believe that the Congress and the Presidentwill need to address the issues of providing af-fordable prescription drug coverage for seniorsif they do not manage to do it before the end ofthis year. The physician community is one ofthe first groups I would like to meet with as anewly elected Member of Congress so we canaddress these critical issues. ✦
Janet Robert can be reached at 763/712-4951.
Crutchfield Dermatology
Your Patients willLook Good & Feel Great
with Beautiful Skin
www.CrutchfieldDermatology.com
Charles E.Crutchfield III, M.D.Board Certified DermatologistExperienced BOTOX Provider
1185 Town Centre DriveSuite 101
Eagan, MN 55123
Appointments651-209-3600
Prompt Appointments via Physician Requests
“Exceptional care forall skin problems”

14 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Tim Pawlenty (R)
Do you support requiring health plans to dis-close contract terms that affect the cost andquality of care to consumers and to providers?
Yes, I support requiring health plans to disclosecontract terms that affect the costs and qualityof care to consumers and to providers. Some ofthe contracting practices of some of the Min-nesota health plans have been very unfair tothe contracting providers of Minnesota. How-ever, it is the expectation of the legislature thatprovider groups and health plans will work to-gether to come up with some common groundon this issue.
Do you support holding health plans account-able for decisions that deny care and result inadverse effects on the enrollee?
Yes, I believe health plans should be held ac-countable for decisions they make that directlyapprove or reject health care decisions and havean adverse effect on patients.
One important point is that there is cur-rently appeal options for people who are deniedmedical care or would like to appeal a health
Candidates for Governor
plan decision. They can file an appeal with thehealth plan, file a complaint with the State,obtain an external review of the health plan de-cisions, and/or file a lawsuit with the court.
Do you support prohibiting health plans fromextending the participating provider’s contractterms to additional health plan products with-out the provider’s consent?
Yes, I support prohibiting health plans fromextending the participating provider’s contractterms to additional health plan products with-out the provider’s consent.
Do you support allowing providers to have avoice in establishing the termination, indem-nification, and arbitration language of healthplan contracts?
Yes, I support allowing providers to have a voicein establishing the termination, indemnification,and arbitration language of health plan contracts.
Do you support requiring that providers mustbe notified by the health plans of any codingchanges that are made to submitted claims inadvance of the payment of the claim to allowfor an appeal?
Yes, I support requiring providers to be noti-fied by the health plans of any coding changesthat are made to submitted claims in advance ofthe payment of the claim to allow for an appeal.
Do you support requiring the health plans toprovide low cost, accessible means for providersto obtain required pre-authorization approvals?
Yes, I support requiring the health plans to pro-vide low cost, accessible means for providers toobtain the required pre-authorization approvals.
Do you support legislation that would allowproviders to collectively negotiate contracts withthe large health plans in an effort to level theplaying field?
No, I have significant concerns about legisla-tion that would allow providers to collectivelynegotiate contracts with the large health plans.
What is the health care issue that is of the high-est priority to you as a candidate?
My priorities in health care include: providingcompetition; patient access and connectionwith health care providers; addressing the ris-ing cost of health care and prescription drugs;and issues related to medical malpractice. ✦
Tim Pawlenty can be reached at 651/905-0555.
There is evidence that policymakers in Minnesota will have to respond to increasing health care costseven though physicians and other providers are surviving on very low reimbursement from Medicareand the large health plan payers. The demand for high tech care by the consumer is rapidly increasingwhich places more demands on a system that is economically squeezed. Shortages in the health carework force such as nursing and some medical specialties such as infectious disease and neurosurgerywill continue to create extreme pressures within the health care system in Minnesota.
A significant problem with our current system is that three large health plans control much ofthe health care financial structure in Minnesota. These health plans determine what services will becovered and the reimbursement that providers will receive. The high operating costs of these largehealth systems are also eating up dollars that should go to patient care.
The following questions relate to the Minnesota Fair Healthplan Contracting bill that wasintroduced in the 2002 Session of the Minnesota Legislature.
Editor’s Note: MetroDoctors provided the following background information to the gubernatorialcandidates. Please note that Roger Moe was given the opportunity to answer the questions as well,but did not provide responses.

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 15
Tim Penny (IND)“I have made it a policy of my campaign not toanswer questionnaires. Rather than answer ques-tions on this specific piece of proposed legislation,I would like to share with your readers my overallthoughts on health care reform.
“Given the extreme cost pressures on thehealth care system, and the state of our state bud-get deficit, health care reform will be an impor-tant issue for the next Governor. As Governor, Iwill work with the entire health care communityto come to a bipartisan solution on how we re-form our health care system for the future.”
Common Sense and StraightTalk on Health Care Reform
Tim Penny has been a leader on health careissues, both as an elected official and a privatecitizen. He recently moderated 24 town hallmeetings across Minnesota on health care andlong-term care reform. He was the nationalspokesperson for the Health Care LeadershipCouncil, and had a close relationship with doc-tors and nurses throughout his elected years.In Congress, he was proud to represent andwork closely with the Mayo Clinic.
Health care needs Tim Penny’s strong,nonpartisan leadership from the top, especiallyin a time of budget crisis.
Health Care CostsAll Minnesotans, including employers, consum-ers and state government, are experiencing ex-traordinary premium increases, costs whichthreaten to undermine the progress Minnesotahas made in providing affordable health care.
Tim Penny believes it’s time for thought-ful legislative changes in Minnesota’s health care
system. As Governor, Tim Penny will developbipartisan, long-term reform proposals with theparticipation of the entire health care commu-nity. These changes must engage consumers inhealth care decisions, allowing them to makechoices for themselves and their families. It alsomust drive toward making the delivery of healthcare more safe, effective and efficient.
PreventionMinnesota is the healthiest state in the nationand we should be proud. Prevention and edu-cation about staying healthy saves us money inthe long-term. Tim Penny supports continuedinvestment in prevention, including tobacco-prevention programs.
Long Term CareOur population is aging, especially in ruralMinnesota. Older Minnesotans should be ableto stay independent as long as possible and haveaccess to community-based care. Tim Penny willwork to ensure that older and chronically illMinnesotans have quality and affordable care.
Health Disparitiesand Covering KidsMinnesota does a good job insuring most Min-nesotans, but we have serious racial and ethnicdisparities in health care coverage – and we stillhave uninsured kids. Tim Penny believes that weshould continue to find ways to cover the unin-sured, with a focus on children and minorities.
Prescription Drug CoverageTim Penny will keep pressure on Washingtonto include a Medicare benefit for prescriptiondrugs while ensuring that poor senior Minne-sotans have help accessing the prescriptiondrugs they need.
Workforce ShortageThe growing shortage of nurses and otherhealth professionals in Minnesota threatens thequality of care in health care institutions anddrives up health care costs. As Governor, TimPenny will work with the education and healthcare community to forge a creative solution tothis pressing problem. ✦
Tim Penny can be reached at 1/888/507-3669.
For more information call 612-362-3704.
RMS Membership Advantages forPhysicians and their Practices
Products Offered to RMS Members by RCMS, Inc.
Business AdvantEdge is a local company that offers discounts on:office supplies; Sprint PCS cell phones and plans; Compaq computers;copiers; fax machines; payroll processing (ADP); local and long distancephone service; courier services; travel; and discounts on overnight deliveries.
DAMARCO Solutions provides OSHA compliance through theirMaterial Safety Data Sheet (MSDS) management service. MSDS areavailable to clinics 24/7/365 for a minimal fee.
MBNA America Credit Card offers one of the highest credit linesavailable (up to $100,000) through its Platinum Plus card; an introductory0% APR on balance transfer and all cash advances; Year End Summaryof charges; and around the clock Customer Service. Call 1-877-518-9007.
MLT vacations is offering physicians and their staff members andfamilies discounts on vacation packages.
World Medical Leaders is a free internet based CME programconducted by physicians who are recognized leaders in their respectivefields of medicine. Check out their website at www.wml.com.

16 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Ken Pentel (GP)Do you support requiring health plans to dis-close contract terms that affect the cost and qual-ity of care to consumers and to providers?YES
Do you support holding health plans account-able for decisions that deny care and result inadverse effects on the enrollee?YES
Do you support prohibiting health plans fromextending the participating provider’s contractterms to additional health plan products with-out the provider’s consent?YES
Do you support allowing providers to have avoice in establishing the termination, indemni-fication, and arbitration language of health plancontracts?YES
Do you support requiring that providers mustbe notified by the health plans of any codingchanges that are made to submitted claims inadvance of the payment of the claim to allowfor an appeal?YES
Do you support requiring the health plans toprovide low cost, accessible means for providersto obtain required pre-authorization approvals?YES, providing it is secure and verifiable.
Do you support legislation that would allowproviders to collectively negotiate contracts withthe large health plans in an effort to level theplaying field?YES
What is the health care issue that is of the high-est priority to you as a candidate?A universal, one-payer healthcare system. ✦
Ken Pentel can be reached at 612/728-3734.
September 20026 Pulmonary Update
PRESENTED BY: Pulmonary Critical Care Associates and United Hospital
LOCATION: United Hospital, St. Paul, Minnesota
25-26 A.C.L.S - Advanced Cardiac Life Support InstructorPRESENTED BY: Allina Hospitals & Clinics
LOCATION: United Hospital, St. Paul, Minnesota
28 The Management of Ear and Skull Base DiseasePRESENTED BY: Ear, Nose and Throat SpecialtyCare of Minnesota, P.A.
LOCATION: DoubleTree Grand Hotel, Bloomington, MN
October 200212 Retina Update
PRESENTED BY: Phillips Eye Institute
LOCATION: Wyndham Minneapolis Airport Hotel, Bloomington, MN
24-25 Frontline NeurologyPRESENTED BY: Minneapolis Neuroscience Institute of Abbott Northwestern
Hospital; the American Association of Neuroscience
Nurses – Twin Cities Area Chapter
LOCATION: Wyndham Minneapolis Airport Hotel, Bloomington, MN
November 20021 HIV Care Conference
PRESENTED BY: Allina Hospitals & Clinics, Hennepin County Medical
Center and Midwest AIDS Training & Education
LOCATION: Abbott Northwestern Hospital, Minneapolis, Minnesota
18-19 A.T.L.S - Advanced Trauma Life SupportPRESENTED BY: Allina Hospitals & Clinics
LOCATION: United Hospital, St. Paul, Minnesota
December 20025-6 B.L.S - Basic Life Support Instructor
PRESENTED BY: Allina Hospitals & Clinics
LOCATION: United Hospital, St. Paul, Minnesota
For more information contact:Allina Education Services at
(612) 775-9626
or toll-free (800) 605-3744
ContinuingMedical Educationsponsored by Allina Hospitals & Clinics
®Allina Health System

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 17
AQ
Theodore Loftness, M.D.
Editor’s Note: Theodore (Ted) J. Loftness, M.D. became vice presidentand medical director of provider relations for Medica in August 2001.From 1994 to August 2001, Dr. Loftness held a number of key posi-tions with Allina Health System. Dr. Loftness continues to practiceinternal medicine at Litchfield Medical Clinic, where he first enteredprivate practice in 1987 and where he was managing partner and leadphysician from 1989 to 1994. He received his medical degree from theUniversity of Minnesota.
C O L L E A G U E I N T E R V I E W
What are your top three priorities at Medica?
For the first part of 2002, Medica was focused on becoming an indepen-dent health plan. To that end, the Board of Directors has been workingon completing strategic planning from the ground up, including creat-ing comprehensive business plans for 2003. These plans are still beingdeveloped. A major priority for Medica continues to be improving pro-vider relationships. Going forward, Medica will be focusing on success-fully running the business by meeting its business goals and complyingwith the Memorandum of Understanding with the Attorney General’sOffice. In addition, Medica will be implementing the self-funded Electproduct to give our self-insured customers a greater range of options andwe will be re-examining the roles, responsibilities and resources for caremanagement and utilization management.
What are the common goals that health plans andpracticing physicians share, and what are the obstacles toachieving those goals?
A common goal that health plans and practicing physicians share is deliv-ering the highest quality medical care to patients and members. I believethe variation in how health care is delivered to our patients and memberswho have chronic conditions is one of our biggest opportunities. His-torically, the health care system built and relied on an infrastructure thatwas better suited to manage acute rather than chronic conditions. Chronicconditions often require around the clock support, motivation and educa-tion. We need to have more systems in place that address these concerns.
Which mechanisms are in place at Medica to assure theinput of practicing physicians during policy development?
Medica solicits input from providers on a variety of topics through severaldifferent mechanisms, including focus groups, provider forums, face-to-face meetings and a number of committees. The Medical Policy Com-mittee is made up of board-certified, practicing physicians in familypractice, internal medicine, obstetrics and gynecology, and pediatrics, aswell as a consumer representative. I assist in the appointment of thesecommittee members. Local specialist input is requested upon creation ofnew utilization management policies and throughout the annual revi-sion process. We also receive input from the Medical Advisory Commit-tee, the Physician Specialty Panel, the Pharmacy and TherapeuticsCommittee and a Quality Improvement subcommittee. More than 100external practicing physicians serve on these committees. In addition,there are three physicians that serve on Medica’s Board of Directors. And,physicians can always call me and give me their input. I can be reached atMedica at 952/992-8456.
How will you direct quality improvement initiatives nowthat Allina and Medica are separate entities?
Medica has an annual process for establishing quality improvement pri-orities that is led by Medica’s Vice-President and Medical Director forQuality and Care Management. This process involves assessing the needsof the various populations insured through Medica and comparing thoseneeds to the resources available in existing programs.
The past association between Medica and Allina did not affect thisprioritization process or the establishment of clinical priorities for anygiven year.
(Continued on page 18)

18 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
Colleague Interview
(Continued from page 17)
How will Medica balance increased demand for medicalcare with business demands for lower health care costs?
Using resources to help prevent disease and to help prevent complica-tions in people that have chronic conditions are important ways that wecan help balance the demand. For example, in the management of diabe-tes, it is better to spend more on pharmacy costs now so future costs thatcould result from complications are avoided (myocardial infarction,amputations, etc.).
Contracts between physicians and health care plans havefavored the plans in the past. What are Medica’s plans forfairer contracts and more understandable reimbursementin the future?
Medica is in the process of reviewing and revising its standard physiciancontract with the goal of producing a contract document that clearlydelineates both parties’ rights and responsibilities — using standardizedcontract language. We have submitted our physician contract to the MMAfor their review and input and are incorporating feedback received directlyfrom physicians and clinic administrators.
Medica is also in the process of standardizing its reimbursementmethodologies. We are moving toward greater use of CMS reimburse-ment methodologies where possible, such as RVU-based fee schedules,professional/technical fee splits, lab fee schedules, etc.
Medica has also been working to get more information added toour web site to ensure that physicians have understandable detailed in-formation on a variety of topics. Our provider newsletters, medical policesand clinical guidelines, credentialing plan, administrative manuals, for-mulary, etc. can all be found on our web site. Log onto www.medica.comand then click on “Provider Resources.”
What will Medica be doing to deal with the 20 percent ofpatients who utilize 80 percent of costs?
Medica has a broad program in the area of care coordination that is ad-dressing the needs of the 20 percent of the patients utilizing 80 percentof the resources. Patients that need or potentially need significant re-sources are identified through a number of different mechanisms. Theseinclude, among others, health risk assessments, chronic disease registries,hospital admission rosters, hospital admission data, and/or referrals froma variety of sources. Once identified, patients may receive many differenthealth plan services. These could include coaching, teaching, coordina-tion of resources, referrals to disease management programs, referrals topractitioners, consultations with practitioners, and ongoing contact witha nurse case manager, among others. The mix and intensity of interven-tions varies with the patient and the identified needs.
Medica has been perceived as having contractual termsunfavorable to independent physicians, with thosephysicians having no options to negotiate more favorableterms. Will this change following the breakup of Allinaand formulation of a new Medica Board of Directors?
The aggregation of medical groups for contracting has created greaterleverage in today’s market for these groups. At the same time, Medica hasa long history of working with independent physicians to provide com-parable reimbursement for comparable services. We try to balance accessissues with the needs of our members. Medica has been moving towardmore standardized contracts because these types of contracts can helpensure that claims are paid quickly and accurately from an operationalstandpoint. We also believe that standardized contractual terms acrossspecialties are fairer to groups of like providers.
Minnesota doctors are fed up with behavioral carveoutsand want access to care and consultations. Medica hasbeen cutting its UBH clinics but not adding psychiatriststo its network. What are Medica’s plans in this area?
Medica recently signed a new three-year ASO (administrative servicesonly) contract with UBH. In this new agreement, Medica will be respon-sible for the cost of all mental health services. In the past year, UBHadded 48 psychiatrists and 30 clinical nurse specialists to its network. Inaddition, UBH pays a premium to certain psychiatrists to reserve appoint-ment slots each week for emergency cases to ensure access to care forMedica’s members. UBH has not owned or operated mental health clinicssince 1996.
Will Medica follow BCBSM and HealthPartners in usingthe 3-judge denial review panel set up in the June 2001Hatch/BCBSM mental health case settlement?
Yes. As of March 2002, Medica began voluntarily participating in theAdministrative Review Committee process. Medica members may con-tinue to follow the regular appeals process concurrently with the ARCreview process, thereby strengthening the claims-review process overall.
Medica continues to pay for out-of-network physician carebut not the prescriptions from out-of-network MDs. Canyou fix this?
It is fixed. Out-of-network physician care and prescriptions are coveredaccording to each member’s certificate of coverage if they have out-of-network benefits. Prior to the first of this year, however, out-of-networkpharmacy claims had to be filed on paper by the member. Effective Janu-ary 1, 2002, after working with our pharmacy benefit partner, MedImpact,our members can now have their out-of-network pharmacists electroni-cally process their claims for them. All members have to do is present

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 19
their Medica member ID card and provide the following numbers: BIN0003583 and PCN 99500 (The Billing Information Number and thePharmacy Carrier Number). This information allows the pharmacist toprocess these claims on line through MedImpact. This information wascommunicated to our members last fall.
What are you doing to reduce the “hassle factor” atMedica? How do you plan to speed up the payment ofclaims, especially claims for procedures?
Medica has implemented numerous operational improvements withinthe past year to reduce administrative hassle and speed up claims pay-ment. Since November 2000, Medica has reduced claims turnaroundtime by 40 percent. Claims payment has consistently been less than 10days from date of receipt to date paid for all claim types this year. Also,Medica automatically pays interest on fully insured claims that have notbeen processed and paid within 30 days.
We are also credentialing physicians faster. The average turnaroundtime to get provider numbers issued is now only 20 days. In addition,our coding team continues to actively engage providers in order to facili-tate common understanding of procedural coding practices and AMAguidelines, focusing on those specific areas that delay claims paymentand require re-work for providers.
As one of the largest providers/controllers of access tophysicians, hospitals and pharmaceuticals, how do youpropose to reduce the segment of our community that lacksthe access? Or, how do we achieve universal access toessential health care?
This is a problem where the solution lies well beyond Medica.Medica has worked to develop affordable health care solu-tions for a variety of populations across Minnesota. We havealso worked with a variety of state agencies to ensure thatMinnesotans have access to health care coverage and healthimprovement programs.
What are your plans to improve morale and developfeelings of partnership between Medica and participatingphysicians?
Medica is making a concerted effort to better connect withthe physician community. Lots of conversations are occur-ring between Medica and physicians to help Medica betterunderstand the issues physicians face. We are listening andwe are taking action on what we are hearing.
This market is unusual in that hospitals receive more totalhealth care dollars than physicians. Do you see that as anaberration that will change or will physicians continue tofall behind?
In 2001, hospitals received 41 percent of Medica’s medical expenses.Physicians received 39 percent. Medica contracts with all provider typesand reimburses based on where the service is performed. Physicians di-rect where a large amount of the care is received. If more hospital resourcesare utilized, more is paid to hospitals. Physician ordering patterns directlyinfluence how resources are allocated.
Health care premiums in Minnesota are higher than thenational average, yet the cost of health care in Minnesotais about 82 percent of the national average. Where is themoney going? (Source: Alan Baumgarten’s report onHMOs in 2001)
Dr. Loftness declined to answer this question at this time, however offeredto give it more attention in the future. ✦
The Perfect Place to Practice
An Equal Opportunity Employer
the noise, the traffic. But don’t get too secluded.We can offer you the best of both worlds—a small town atmosphere
within a short drive of the Twin Cities. Come to RiverWay.
We are expanding and have opportunities for Family Practice, OB/Gyn, Pediatrics, and Urgent Care Physicians
in the northern suburbs of Minneapolis.
RiverWay Clinics is a truly dynamic organization and is part of theHealthPartners family. Please send your C.V. to: RiverWay Clinics, Attn: Steven Endrud, 1833 Second Ave. S., Anoka, MN 55303.
Fax to: (763) 712-6264
Get awayfrom the distractions,

20 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
A
Emerging fromImmunization ChaosAFTER YEARS OF EDUCATING the commu-nity on the value of receiving vaccinations forinfluenza in the fall, delays in the vaccine’s arrivalover the past few years have created chaos for bothphysicians and their patients. Some concerns andrecommendations for supporting patients in re-ceiving this important preventive health serviceare addressed below. The single most effectivemethod of making sure patients are vaccinatedagainst influenza is still by a physician’s recom-mendation.
Q. With decreasing Medicare reimbursement,can a physician cover his/her costs for fluand pneumococcal immunizations?
A. Table 1 shows that the 2002 Medicare re-imbursement for the costs of administeringthe vaccine decreased by $.57 for both theinfluenza and pneumococcal vaccines. Vac-cine purchased directly from the manufac-turers averages approximately $6.50/dose,and since the Medicare reimbursement is$8.62, this may cover the cost. The mostimportant factor in keeping vaccine costslow is by ordering early. Pre-booking oftenbegins as early as January. Influenza vaccinethat is ordered at a later date may only befound through distributors and others that
charge inflated prices (>$100 per vial). Ac-cording to one manufacturer, the pneumo-nia vaccine will cost approximately $14.48/dose.
Q. If my clinic orders the vaccine early, why dosome organizations receive the vaccine ear-lier? Is my clinic not a priority?
A. During the past two influenza seasons, thetiming of vaccine shipments has been largelyinfluenced by the manufacturers’ ability toproduce the vaccine and with vendors.When vaccine first became available for the2001-02 flu season, the manufacturers be-gan shipping partial shipments to all of theirlarge volume customers and full shipmentsof smaller orders (e.g., <1,000 doses). Onoccasion, a partial shipment of vaccine to adistributor may have been subject to fur-ther adjustments.
Q. I want to vaccinate my patients, but needto make the process cost-effective and effi-cient. What should I do?
A. Standing orders programs constitute themost effective strategy for improving immu-nization rates for adults, according to Kristin
L. Nichol, M.D., of the Veterans AffairsMedical Center. Standing orders automatethe immunization process, removing thephysician from the loop for a more stream-lined system of care. (On August 1, 2002, anew law went into effect allowing LPNs toadminister vaccines based on such a stand-ing order protocol. Previously, only RNswere authorized to assess and administer vac-cines under a standing order protocol. Formore information about this new bill, visitthe following website: www.leg.state.mn.us/leg/legis.htm and search under Bill 3359.)
Q. Between the reimbursement and distribu-tion issues, my clinic can’t offer vaccines.What should we do?
A. It is anticipated that there will be enoughvaccine for this flu season, however, theremay be delays in delivery to some physicianoffices. To make sure that high-risk patientsreceive the vaccine early enough, even if thevaccine is unavailable at your site, send themto a non-traditional community site (e.g.,local senior centers, grocery stores). Remem-ber to follow the Minnesota Department ofHealth (MDH) Minnesota Flu VaccinationPlan for the 2002-2003 Season, which is asfollows:
Prioritize• October – Vaccinate high-priority patients,
those 65 and older, patients 6 months ofage and older with chronic medical condi-tions such as heart disease, diabetes, asthmaor HIV/AIDs—those most likely to experi-ence serious morbidity and death if theydevelop influenza. In addition, children 6to 23 months are encouraged to be vacci-nated when feasible.
Table 1: Adult Influenza and Pneumococcal Vaccine Medicare Reimbursement
Influenza Vaccine Pneumococcal Vaccine
2001 2002 2001 2002
Vaccine $4.92 $4.92 $15.24 $15.50
Administration fee $4.27 $3.70 $4.27 $3.70
TOTAL $9.19 $8.62 $19.51 $19.20
Source: Wisconsin Physician Services (WPS), Medicare Part B Carrier for Minnesota.
B Y J A N E P E D E R S O N , M . D . , M . S .

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 21
• November through the end of flu season –Continue to vaccinate high-priority patientsand begin to vaccinate healthy patients.
• Vaccinate through March or the end of the fluseason. Recent flu seasons have arrived inlate winter. It is never too late to get vacci-nated, even if flu is already in the commu-nity.In order for this plan to succeed, coopera-
tion from physicians statewide is essential. Forinfluenza updates, refer to the Minnesota FluVaccination Plan at www.health.state.mn.us/im-munize.
Q. Is vaccination for influenza and pneumo-coccal really effective? Given the fast pace inoffice practice, what should be highest pri-ority?
A Dr. Nichol recently noted, “compared withall other vaccine-preventable diseases, influ-enza and pneumococcal diseases kill morepeople in the United States, and 80 to 90percent of these deaths are in the elderlypopulation.” Dr. Nichol attributed this highpercentage to a lack of recommendationsfrom physicians and to patients’ misconcep-tions about vaccines. According to Dr. Gre-gory Poland, Director of the Mayo VaccineResearch Group at the Mayo Clinic andFoundation, “We measure the health of so-ciety by a number of indicators, one of thembeing immunization—and, clearly, we haveinadequate vaccination coverage in adults.By giving the influenza vaccination to eld-erly people, we can cut the rate of influenzadeaths in half.”
Q. What are the rates for the flu and pneumo-coccal immunization in Minnesota?
A. The Behavioral Risk Factor SurveillanceSurvey, a telephone survey conducted by theMDH in 2001, showed the following vac-cination rates for Minnesota adults, aged 65and older: 70.5 percent for influenza and64.0 percent for pneumococcal. TheHealthy People 2010 goal for influenza andpneumococcal immunization is 90 percent.Consequently, physicians can play a key rolein accomplishing these goals.
Q. Where can I get help setting up an immuni-zation program in my facility?
A. The Minnesota Partnership for Adult Immu-nization has developed resources to help. Formore information please contact SusanSeverson, Stratis Health, at (952) 853-8538.Please help to inform your patients about
the importance of getting their influenza andpneumococcal shot by recommending it to allyour patients! ✦
Jane Pederson, M.D., M.S., is the Director of Medi-cal Affairs at Stratis Health. This material was de-veloped under Contract Number 500-99-MN02,entitled “Operation of Utilization and QualityControl Peer Review Organization (PRO) for theState of Minnesota,” sponsored by the Centers forMedicare & Medicaid Services (CMS), Departmentof Health and Human Services. The contents donot necessarily reflect CMS policy.
Dermatology, Family Practice,Gastroenterology, Internal
Medicine, & Neurology
BBBBBRAINERDRAINERDRAINERDRAINERDRAINERD M M M M MEDICALEDICALEDICALEDICALEDICAL C C C C CENTERENTERENTERENTERENTER, P, P, P, P, P.A..A..A..A..A.• 44 Physician independent multi-specialty group• Located in a primary service area of 50,000 people• Almost 100% fee-for-service• Excellent fringe benefits• Competitive compensation• Exceptional services available at 162 bed local
hospital, St. Joseph’s Medical Center
BBBBBRAINERDRAINERDRAINERDRAINERDRAINERD, M, M, M, M, MINNESOINNESOINNESOINNESOINNESOTTTTTAAAAA• Surrounded by the premier lakes of Minnesota• Located in central Minnesota less than 2 1/2 hours
from the Twin Cities, Duluth, and Fargo• Large, very progressive school district• Great community for families
CCCCCALLALLALLALLALL COLLECTCOLLECTCOLLECTCOLLECTCOLLECT TTTTTOOOOO A A A A ADMINISTRADMINISTRADMINISTRADMINISTRADMINISTRATTTTTOROROROROR:::::Curt Nielsen(218) 828-7105 or (218) 829-4901Toll Free 800-677-82622024 South 6th StreetBrainerd, MN 56401
There are immediate openings at BrThere are immediate openings at BrThere are immediate openings at BrThere are immediate openings at BrThere are immediate openings at BrainerdainerdainerdainerdainerdMedical Center fMedical Center fMedical Center fMedical Center fMedical Center for the for the for the for the for the folloolloolloolloollowing specialties:wing specialties:wing specialties:wing specialties:wing specialties:DerDerDerDerDermatologymatologymatologymatologymatology, F, F, F, F, Family Pramily Pramily Pramily Pramily Practiceacticeacticeacticeactice, Gastroenterology, Gastroenterology, Gastroenterology, Gastroenterology, Gastroenterology,,,,,InterInterInterInterInternal Medicinenal Medicinenal Medicinenal Medicinenal Medicine, and Neurology, and Neurology, and Neurology, and Neurology, and Neurology.....
bmc@brbmc@brbmc@brbmc@brbmc@brainerd.netainerd.netainerd.netainerd.netainerd.netwwwwwwwwwwwwwww.br.br.br.br.brainerdmedicalcenterainerdmedicalcenterainerdmedicalcenterainerdmedicalcenterainerdmedicalcenter.com.com.com.com.com
Recruitment coordinated with St. Joseph’s Medical Centerwww.sjmcmn.org

22 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
P
Retirement Plan Options forIndependent Medical Groups
B Y J O E L G R E E N W A L D , M . D .
PHYSICIAN GROUPS HAVE a variety ofoptions when it comes to retirement plans. Se-lecting the best type, and structuring it to meetretirement goals, is as much art as science. Plandesign needs to be mindful of the practice’s ob-jectives. It might be to maximize tax deferredcontributions for the physician/owners or itmay be to attract and retain valuable employ-ees. The design also needs to factor in thingssuch as the income of the physicians, the incomeof other employees, the ages of the physiciansand other staff. Let’s look at examples of differ-ent retirement plan structures and in what situ-ations they make the most sense.
SIMPLE IRA:This is a retirement plan that might be consid-ered by a new practice. If the practice wants tohave a retirement plan in place for the physi-cians and employees, a SIMPLE IRA avoidsthe complexity and admin-istrative requirements of a401(k) plan. In essence it’sthe same as opening anIRA account for everyoneemployed by the practice.
Employees, includingthe physicians, can defer$7,000 tax free in 2002.For those 50 and over thereis an additional $500 al-lowed. The base amountwill increase by $1,000 peryear until it’s $10,000 in2005. The catch-up por-tion increases by $500 peryear, so that in 2005 those50 and over will be able todefer $12,000.
In addition to the employee deferral, thepractice must make an employer contributioneach year. This contribution goes into thephysician’s accounts as well as those of the otheremployees. The employer contribution mustbe either 2 percent of salary, or a dollar-for-dollar match on the first 3 percent of the salarythe employee elects to defer. (This 3 percentmatch can be reduced to 1 percent in two outof five years and would enable a practice todecrease their obligation to fund the retirementplan if times were lean.) Therefore, a 40-year-old physician earning $160,000 could save$11,800 in a SIMPLE plan in 2002. Not bad,but we can do better.
SEP IRAs(Simplified Employee Pension)SEPs are not considered qualified plans underERISA law. They are structurally IRAs with cer-
tain features of a qualified plan. Like SIMPLEplans they are easy to implement and operatebecause they essentially involve establishing IRAaccounts for each eligible employee.
A SEP allows physicians to defer up to 25percent of income, to a maximum of $40,000.A physician making $150,000 can defer$37,500 into their SEP and avoid income taxeson this amount. This yearly contribution is notmandatory so that each year the physicians candecide what the percentage of income to be con-tributed to the SEP will be.
There are significant drawbacks to SEPplans that make them somewhat unpalatablefor physician practices that have employees. Themain drawback is that the practice must con-tribute the same percentage of pay for the em-ployees as it does for the physicians. That is, ifthe physicians want to make the maximum con-tribution of 25 percent of income to their SEP
Acme Psychiatric ClinicSafe Harbor - Cross-tested Illustration
Plan Year Ending 12/31/02
Employer Cont. EmployerElective Catch-Up Includes 3% Contribution
Compensation Deferrals Elections Safe Harbor Percentage Totals
AA (Physician-25% owner) $ 200,000.00 $ 11,000.00 $ 1,000.00 $ 29,000.00 14.50% $ 41,000.00BB (Physician-25% owner) $ 180,000.00 $ 11,000.00 $ 29,000.00 16.11% $ 40,000.00CC (Physician-25% owner) $ 200,000.00 $ 11,000.00 $ 1,000.00 $ 29,000.00 14.50% $ 41,000.00DD (Physician-25% owner) $ 180,000.00 $ 11,000.00 $ 29,000.00 16.11% $ 40,000.00EE (Practice Manager) $ 80,000.00 $ 2,000.00 $ 5,280.00 6.60% $ 7,280.00FF $ 50,000.00 $ 2,000.00 $ 3,300.00 6.60% $ 5,300.00GG $ 40,000.00 $ 2,000.00 $ 2,640.00 6.60% $ 4,640.00HH $ 35,000.00 $ 2,000.00 $ 2,310.00 6.60% $ 4,310.00II $ 30,000.00 $ 2,000.00 $ 1,980.00 6.60% $ 3,980.00JJ $ 30,000.00 $ 2,000.00 $ 1,980.00 6.60% $ 3,980.00
$ 56,000.00 $ 2,000.00 $133,490.00 $191,490.00

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 23
accounts, they must put in 25 percent of incomefor each of the employees. In most practicesthis can be quite burdensome. For practiceslooking to allow the physicians to defer up to$40,000, without having to put exorbitantamounts in for the other staff, a 401(k) ProfitSharing Plan might make sense.
401(k) Profit Sharing Plan:The 401(k) portion allows employees to deferup to $11,000 this year, ($12,000 if they are50 or over.) This number will go up by $1,000per year for the next four year so that in 2006it will be $15,000. ($20,000 for those 50 andover.)
In addition to the amount that individualscan defer for themselves, the practice can makecontributions as well. This can allow a physi-cian earning $160,000 to put aside $40,000per year into their retirement plan. In order todo this the practice will have to make contri-butions for all the employees. But, unlike witha SEP plan, a higher percentage of income canbe contributed for the physicians as long as rulesare followed that are designed to prevent dis-crimination against non-highly compensatedemployees. These plan designs include age-weighted plans, cross-tested plans and newcomparability plans.
In addition to which plan design is used,the amounts that the practice can contributefor physicians relative to other employees willdepend to some degree on the ages of the phy-sicians and other employees, the incomes of thephysicians and other employees, as well as otherfactors.
Again, good plan design can help addressthe needs of the practice. In some cases it is toget the greatest amount of money to the physi-cians and one or two other valued employeeswhile minimizing the amounts being paid toother employees. In other groups the focus maybe on recruitment and retention of staff.
The illustration on page 22 shows what apractice might have to contribute in order toallow the physicians to be able to defer the maxi-mum allowed.
In this example there are four physicians,each a 25 percent owner of the practice. Theyare earning between $180,000 and $200,000.Their practice manager earns $80,000 and thereare five other employees who qualify to partici-pate in the 401(k). The physicians each defer
the maximum allowed to the 401(k), $11,000per year. (Two physicians over age 50 also con-tribute the extra $1,000 catch-up amount.) Thepractice contributes $29,000 per physician, al-lowing each physician to reach the $40,000,($41,000 for the two MDs over age 50,) al-lowed by law. To allow this amount to be con-tributed for the physician/owners, the practice
must contribute the amounts shown for the em-ployees in the column headed “employer con-tribution.” Therefore this practice wouldcontribute $17,490 for the employees so thatthe physician owners could maximize their pre-tax savings. This contribution is a tax-deduct-
(Continued on page 24)
SHARING A SINGLE FOCUS
®
HEALTHEAST® WOUND CARE IS NOW LOCATED AT THE HEALTHEAST® VASCULAR CENTER
As a disease management center, we offer an integrated program of diagnostics, treatment,
follow-up, disease prevention and education focused on vascular patients.
Partner with us to ensure your patients receive the best care possible.
651/232-2550www.healtheast.org/vascular
Gallery Professional Building, Suite 60017 W. Exchange St., St. Paul, MN 55102

24 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
ible expense for the clinic. As most physiciansare in a tax bracket close to 50 percent, the abil-ity to defer $40,000 of income free of taxes is asignificant benefit.
401(k) plans are more complicated to ad-minister and more expensive than the SIMPLEor SEP plans outlined above. These require-ments include the annual filing of 5500 formswith the IRS, fiduciary obligations to reviewthe performance of the investments offered toparticipants, making sure employees receivenotification and education on the plan, etc.
Another feature that is available since thepassage of the EGTRRA law is the advantageof employing a spouse in your practice. If yourspouse earns $11,000 this year working in yourpractice, they can have 100 percent of this gointo the 401(k). If there is a profit-sharing fea-ture then even more of their compensation cango into the plan tax-free.
Something for practices currently withouta retirement plan to keep in mind is the taxcredits that the 2001 EGTRRA tax law allowsfor a new plan. For the next three years the lawallows a tax credit of $500/year for the expensesof setting up a new plan. That’s a credit – dol-lar for dollar offset on taxes – not simply a de-duction.
Defined Benefit Plan:When people think of retirement plans theyusually think of defined contribution plans suchas 401(k) plans, SEPs, SIMPLEs, etc. In theseplans what is defined is the annual contribu-tion that the employer makes, say 3 percent ofsalary. Physicians often overlook defined ben-efit plans. These plans are somewhat more com-plicated, in part because they require theservices of an actuary. In these plans what isdefined is a projected payout in retirement. Theplan is then funded to the extent needed tomeet this future obligation which might be anannual payout of $150,000.
Defined benefit plans were more in voguein the past and fell out of favor because of taxlaw changes. The recent changes contained inEGTRRA have again made these great vehiclesin certain situations. Roughly speaking, if thephysicians in the practice are 45 or older andare looking to contribute more than the$40,000 allowed under defined contribution
plans, think defined benefit. It may allow tax-deductible contributions to the retirement planof over $100,000/year. These plans work bestthe older the physicians, and the younger theother employees. Above is an example of a 55-year-old physician with five staff people.
There are drawbacks to a defined benefitplan. One is that the contribution must bemade to the plan each year. For practices thathave uneven cash flow and profitability, thismight be a hardship. Another drawback is thegreater administrative complexity and expense.But for those looking to shelter income fromcurrent taxation, defined benefit plans can bean elegant solution.
Retirement plans for physician practicesis a broad topic. I’ve attempted to highlightsome of the things that physicians should beaware of as they establish or review theirpractice’s retirement plans. The right plan for apractice needs to take into account many fac-tors and it’s best to involve a team of indepen-dent specialists in retirement plan design andimplementation. Making smart choices aboutretirement plans can help physicians enjoy thefinancial success they deserve. ✦
Joel Greenwald, M.D. is a Certified EmployeeBenefits Specialist with Raymond James Finan-cial Services Inc., member NASD/SIPC, in Edina,Minnesota.
Employees Age Compensation Contribution
Doctor/Owner 55 $200,000 $120,000Staff 50 $40,000 $4,400Staff 50 $30,000 $3,300Staff 45 $25,000 $2,750Staff 21 $20,000 $2,200Staff 21 $20,000 $2,200
Total Staff Contributions $14,850
Defined Benefit - Cross-Tested Cash Balance Plan
Retirement Plan Options
(Continued from page 23)
����������� ����� �������
����� �������������� ����������
������������������ �����������
�������������������� ���� ����
��������� ��� �!��������������
� �� ���"���������#
���������������
� ���
������
���������
!$����������� ���������%�"
����������������������$���������
�����&'()��� ���������"�� �������"
������������ ��*���� ���������
� ���������� �����
� �����# +�����*��� �����
����������� �
,-,.����� �*��/!
��������/..&01
,-0�,2.�0002
������������ ������
AndreaFarina
Text Box
See updated contact information for Joel Greenwald, MD below
AndreaFarina
Text Box
Joel Greenwald, MD, is a CERTIFIED FINANCIAL PLANNER™ professional with Greenwald Wealth Management located at 1660 South Hwy 100, Suite 270, St. Louis Park, MN. 952-641-7595. http://www.joelgreenwald.com. Securities and advisory services offered through Commonwealth Financial Netork®, Member FINRA/SIPC, a Registered Investment Advisor. Fixed insurance products and services offered by Greenwald Wealth Management are separate and unrelated to Commonwealth.

PRESIDENT ’S MESSAGEP E T E R H . K E L L Y, M . D .
RMS-Officers
President Peter H. Kelly, M.D.President-Elect Michael Gonzalez-Campoy, M.D.Past President Robert C. Moravec, M.D.Secretary Jamie D. Santilli, M.D.Treasurer Peter J. Daly, M.D.
RMS-Board Members
Kimberly A. Anderson, M.D., Specialty DirectorJohn R. Balfanz, M.D., Specialty DirectorVictor S. Cox, M.D., Specialty DirectorGretchen S. Crary, M.D., At-Large DirectorCharles E. Crutchfield, III, M.D., At-Large DirectorLaura A. Dean, M.D., At-Large DirectorThomas B. Dunkel, M.D., MMA TrusteeJames J. Jordan, M.D., Specialty DirectorRobert V. Knowlan, M.D., At-Large DirectorCharlene E. McEvoy, M.D., At-Large DirectorRagnvald Mjanger, M.D., Specialty DirectorKenneth E. Nollet, M.D., Ph.D., At-Large DirectorStephanie D. Stanton, Medical StudentLyle J. Swenson, M.D., MMA TrusteeCharles G. Terzian, M.D., Specialty DirectorDavid C. Thorson, M.D., Specialty DirectorRussell C. Welch, M.D., At-Large Director
RMS-Ex-Officio Board Members &Council Chairs
Brent R. Asplin, M.D., AMA Young Physician SectionBlanton Bessinger, M.D., MMA Past PresidentKenneth W. Crabb, M.D., AMA Alternate DelegateRobert W. Geist, M.D., Ethics & Professionalism
Council Chair*Michael Gonzalez-Campoy, M.D., Education
Resource Council ChairRebecca Gonzalez-Campoy, Alliance PresidentFrank J. Indihar, M.D., AMA DelegateWilliam E. Jacott, M.D., U of MN RepresentativeMelanie Sullivan, Clinic AdministratorDonald B. Swenson, M.D., Sr. Physicians
Association President*Lyle J. Swenson, M.D., Public Policy Council Chair*Russell C. Welch, M.D., Communications
Council Chair*Also elected RMS Board Member
RMS-Executive Staff
Roger K. Johnson, CAE, Chief Executive OfficerDoreen M. Hines, Membership & Web Site CoordinatorSue Schettle, Director of Marketing & Member Services
MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 25
PThe Malpractice Insurance Crisis
PHYSICIANS IN MINNESOTA should feelfortunate. We have not been touched by a catas-trophe that has befallen many of our fellow phy-sicians across the United States. I am speakingof the malpractice crisis that has gripped manystates rendering medical services in many areasunobtainable. Our good fortune may not lastand now is the time to be proactive in order tostave off this fate.
Currently, physicians and hospitals instates such as Florida, West Virginia, Pennsyl-vania, Mississippi and Nevada are seeing sky-rocketing rate increases for liability insuranceor are unable to obtain insurance at all. TheUniversity of Nevada, Las Vegas recently closeddown its trauma center for 10 days for lack ofinsurance. Patients had to be transferred to Cali-fornia for their care. There are no neurosurgeonsleft in northern Mississippi due to skyrocket-ing rates, which is over $250,000 per year insome areas. In many states, such as Florida andVirginia, physicians are protecting their assetsand going “bare,” (going without any malprac-tice insurance). The St. Paul Companies hasrecently stopped underwriting medical mal-practice insurance, leaving many practitionersunable to obtain coverage.
Why is this occurring? There are severalreasons; chief among them is ever increasingjury awards in medical malpractice cases. Overthe past three years the median jury award hasincreased by 43 percent. Additionally, over 50percent of all jury awards now exceed one mil-lion dollars in these cases. To fully understandthis, one needs to know how the jury award isbroken down. Essentially, there are economicand non-economic components to the malprac-tice case. The economic components includelost wages and medical expenses. This portionof the award is straightforward in its determi-nation. The other component is non-economic;i.e., pain and suffering as well as punitive dam-ages. It is this portion of the award that juriescan arbitrarily determine and which turns manytrials into a lottery.
Several states have passed legislation thatlimits the non-economic damages that juriesmay award. Twenty years ago California passedthe Medical Injury Compensation Reform Act(MICRA) which caps non-economic damagesat $250,000, limits attorney’s fees in malprac-tice cases and has a three-year statute of limita-tions in non-pediatric cases. Malpracticepremiums in California are 40-50 percent lowerin many specialties compared to the same spe-cialties in other states.
The American Medical Association(AMA) has recognized this national dilemma.They have listed 12 states that are in a full-blown liability crisis and 30 more as having thepotential for a liability crisis in the near future.Minnesota is among this latter group. At thenational level, President Bush has come out infavor of federal legislation that would:• Limit non-economic damages to
$250,000 with no limits on economicdamages.
• Limit punitive damages to whichever is less:$250,000 or twice the economic damages.
• Include a statute of limitation on malprac-tice cases.
• Allow physicians to pay awards to patientsover time instead of in one lump sum.
• Require physicians to pay only the portionof damages for which they are responsible.The House of Representatives has intro-
duced the Help Efficient, Accessible, Low Cost,Timely Health Care (HEALTH) Act of 2002(H.R.400) which includes a national tort re-form based on the MICRA model.
Unfortunately, tort reform at a federal levelmay never happen or it may be years in themaking (example, the Patient Bill of Rights).Therefore, it is imperative that we take this up
(Continued on page 26)
Ra
ms
ey
Me
dic
al S
oc
ie
ty

26 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
at a state level. The Ramsey Medical Society(RMS) is supporting a resolution at the up-coming annual Minnesota Medical Association(MMA) meeting which calls upon the MMAto develop and support tort reform legislationbased on California’s MICRA. It is imperativefor physicians in this state to lobby their repre-sentatives on this issue. It will be a tough fightas the trial lawyer lobby has been very effectivein the past and often lawyer and lawmaker areone in the same. However, we need to makethis a high priority in the 2003 Minnesota leg-islature if we are to avoid the skyrocketing li-ability insurance rates that are being seen acrossthis country. ✦
President’s Message
(Continued from page 25)
RAMSEY MEDICAL SOCIETY is a memberdriven organization that exists to promote andenhance the value of physicians as members ofthe community. We are continually striving toprovide value to our members and havelaunched a number of initiatives that we feelare beneficial to you as a practicing physicianand for your clinics. An example is our involve-ment with our partners in the Minnesota FairHealth Plan Contracting Coalition. The Coa-lition exists to advocate for fairness in healthplan contracting. We are pleased to introduceyou to some of the more recent relationshipsthat we have entered into through our for-profitsubsidiary, RCMS, Inc.
DAMARCO Solutions, LLC is a locallyowned company that offers clinics the abilityto outsource some of their OSHA compliance
requirements, namely the management of theirMaterial Safety Data Sheets (MSDS). The Haz-ard Communications Standard (HCS)(19CGR 1900, 1200) is the most cited OSHAstandard for non-compliance. The beauty ofDAMARCO is that they realize that the ma-jority of clinics that RMS deals with will havesimilar MSDS, therefore they are offering ourmembers a discounted rate for subscribingwith their program. To learn more, call GaryGraczyk at DAMARCO Solutions, LLC, at612-627-0997, or www.damarcosolutions.com.
Quest Card Services, LLC is a company thatoffers clinics discounts on credit card process-ing. If you accept credit card payments at youroffice then please read on. The reason we arepromoting this is that their rates are probablyless than what you are currently paying. Takeyour last statement from the credit card process-ing company that you are currently workingwith and compare it to Quest Card Services. Or,contact RMS at 612-362-3704 and we will fa-cilitate your request. Quest Card Services of-fers you:• 1.67 percent + $.20 for each swiped transaction;• 2.27 percent + $.30 for keyed transactions;• 3rd level charges eliminated by using AVS;• $3 monthly statement fee;• Voice authorization fee is $1.00;• Application fee of $95 is waived;• $25 one-time set-up fee; and• No reprogramming fee.
Through Quest Card Services, LLC weare also able to extend an offer for you to buyor lease the equipment necessary to processcredit card payments. Call the RMS office at612-362-3704 to learn more.
HIPAAdocs offers physicians a less costly andmore efficient method for complying with theupcoming Federal HIPAA regulations. The
deadline for complying is October 16, 2002.HIPAAdocs is a national company whose prod-ucts are created by industry experts to lessenthe burden on physicians as they try and ar-ticulate complex Federal regulations. There areon-line software and documents to help youcomply with HIPAA regulations quickly andeasily. They offer gap assessment tools, riskmanagement mitigation registers, policy docu-ment generation, on-line staff training and asystem for updating and alerting their custom-ers. Their price is based on the number of phy-sicians that you have at your clinic site. Eachclinic is given a Certificate Number that theycan use to utilize all of the products and ser-vices available through HIPAAdocs. Please notethat if you are interested in looking into thisfurther, you need to contact RMS directly sothat we can be assured that you are receivingthe discount that we have negotiated. Pleasecall 612-362-3704.
Business AdvantEdge, Inc. is an independentbusiness services contractor who specializes insmall to medium sized businesses. They are lo-cally owned and operated and have a relation-ship with a multitude of companies rangingfrom Office Depot, Compaq Computers,Hewlett Packard, Integrated Communications,Airborne Express, Savin Corporation, TravelCell and the list goes on. What they offer toRMS members is discounted prices. The dis-counts are greater than if you were to purchasethe products or services independently. To learnmore, contact Mary Hazzard at 651-486-8900,or visit their website at www.business-edge.net.Be sure to tell them that you are a member ofRamsey Medical Society, or that one of yourphysicians is a member.
For other tangible member benefits go towww.metrodoctors.com and click on RamseyMedical Society Member Benefits.
If you are not a member of Ramsey Medi-cal Society (RMS) and the Minnesota MedicalAssociation (MMA), you are invited to join.We are a strong member-driven organizationthat believes wholeheartedly in advocating forthe rights of physicians. If you would like tolearn more about RMS contact Sue Schettle,RMS Director of Marketing and Member Ser-vices. Her telephone number is 612-623-2889,or email: [email protected]. ✦
Benefits to Serve RMS Membersand Their Clinics

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 27
ActiveLisa Landon Anderson, M.D.Oral Roberts UniversityInternal MedicineAllina Medical Clinic - Internal MedicineSpecialties
Jorge A. Ferreiro, M.D.Tulane UniversityAnatomic & Clinical PathologyHospital Pathology Associates, P.A.
Harry F. Hull, M.D.John Hopkins UniversityPublic HealthMinnesota Department of Health
Michael K. Loushin, M.D.University of MinnesotaAnesthesiologyTwin Cities Anesthesia Associates
Robert S. Nesheim, M.D.University of MinnesotaPsychiatryHamm Memorial Psychiatric Clinic/DuluthFamily Practice Center
Maureen K. Reed, M.D.University of MinnesotaInternal MedicineHealthPartners
Susan J. Roe, M.D.University of TexasAnatomic & Clinical PathologyRegina Medical Center
Kevin T. Stieglbauer, M.D.University of MinnesotaAnatomic & Clinical PathologyHospital Pathology Associates, P.A.
John M. Toso, M.D.University of MinnesotaFamily PracticeFairmont Community Hospital
RMS UPDATE
In Memoriam
New MembersRMS welcomes these new members to the Society.
Schools listed indicate the institution where the
medical degree was received.
REYNOLD P. FLOM, M.D., died at the ageof 80. Dr. Flom graduated from the Universityof Minnesota Medical School in 1944 and wasa U.S. Navy Veteran. He specialized inNeuropsychiatry until 1970. Dr. Flom servedas Chief of Staff at Mounds-Midway Hospitalin 1965. He was currently serving as director ofDatron Corporation and the Treasurer andDirector of Health Care Group, Inc. He joinedRMS in 1949.
HUGO F. SCHROECKENSTEIN, M.D.,died on July 29 at the age of 90. He graduatedfrom the University of Minnesota in 1938 andcompleted his internship in general surgery atCharles T. Miller Hospital in St. Paul. Dr.Schroeckenstein served in the Armed Forcesfrom 1942-1946. He joined RMS in 1942.
JOHN J. STERNER, M.D., died at the age of86 on July 22. He graduated from theUniversity of St. Louis in 1942. Dr. Sterner wasa retired family physician and former Chief ofStaff at Bethesda Hospital. He served as theRamsey County Coroner for 29 years. Hejoined RMS in 1948.
RICHARD B. TREGILGAS, M.D., diedsuddenly on May 11 at the age of 77. Dr.Tregilgas graduated from the University ofMinnesota in 1947. He was a board certifiedinternist prior to his retirement. Dr. Tregilgasjoined RMS in 1954. ✦
Kyle L. Wahlstrom, M.D.University of MinnesotaGeneral SurgerySt. Paul Surgeons, Ltd.
Jason J. Wirtz, M.D.University of IowaInternal Medicine/Infectious DiseaseSt. Paul Infectious Disease Associates, Ltd.
1st Year PracticeDiane M. Palkert, M.D.University of MinnesotaOrthopedic SurgeryOrthopaedic Foot and Ankle Center
Medical Student(University of Minnesota)
Anna BuzhakerLevon D. Olson ✦
Ra
ms
ey
Me
dic
al S
oc
ie
ty
AUDIO TAPES - Health EducationFREE for the Hmong Community
Prepared by HealthEast Care System. Made possible through a grant from UCare Minnesota.
These tapes are bilingual, providing information in Hmong onthe first side and repeated in English on the second side.
To receive FREE copies of the audiotapes, contactMayly Lochungvu, Interpreter
St. Joseph’s Hospital69 West Exchange St., St. Paul, MN 55102
651-232-6257 or email [email protected]
“Caring for your Heart and Blood Pressure”and
“What happens when you go to the Hospital”
Please give your name, organization, address, phonenumber and the desired quantity of audio-tapes.

28 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
B
RMS ALLIANCE NEWSR E B E C C A G O N Z A L E Z - C A M P O Y
BY NOW, YOU SHOULD HAVE receivedyour updated voter registration card from thetreasurer/auditor of your county. The card tellsyou where to vote and identifies the variousdistricts in which you live. For instance, I livein Congressional District 02, Senate District39, House District 39B, County CommissionerDistrict 02 and School District 197. I keep mycard in my wallet, where I can easily find it.
The information on your voter registra-tion card is particularly important this fall. Eventhough it’s not a presidential election year, it’sgoing to be a hot election season, thanks to re-districting. Many legislators retired after lastsession, leaving seats open for new faces. Sev-eral legislative and congressional incumbentswill be in tight races. And many respected can-didates have joined the Independence Party outof sheer frustration with various factions of theirformer parties.
Physicians and spouses need to get in-volved – if only to cast informed votes – in theupcoming elections. Simply put, the future ofmedicine depends on it. If we don’t take partin shaping policy, someone else will decide howphysicians practice medicine. That’s largelywhat’s been going on up to now and we’ve seenthe dismal results. Any positive legislation – andthere is some – comes from physicians and theirfamilies working diligently together to make ithappen.
Register to voteFirst, be sure you’re registered to vote. It’s amaz-ingly easy in Minnesota. Just look in your tele-phone book in the Government Pages sectionunder Voter Registration Information – you’llfind step-by-step instructions. The require-ments are few and you can even register on Elec-tion Day at your polling place.
Learn about the candidatesBoth Twin Cities daily newspapers publish can-didate profiles. Community newspapers do aswell. Minnesota Public Radio invites candidatesin for interviews and debates. Newspapers also
publish the voting records of current electedofficials.
Organized medicine provides a wealth ofinformation that’s only a click away. You canjoin the Physicians Grassroots Network atwww.ama-assn.org/grassroots to monitor whatyour members of Congress are doing regard-ing health care issues. Be sure to sign up at thisweb site for timely updates on important legis-lation pending in Washington, as well.
Find out what’s going on at the Minne-sota Legislature by logging on to the Minne-sota Medical Association’s web site atwww.mmaonline.net. There you’ll find the lat-est on issues important to physicians and theirfamilies here at home and across the nation.Ramsey Medical Society also passes on timelylegislative information via e-mail. Contact RMSif you want to get on this mailing list.
Get involvedOne of the biggest reasons other groups are sosuccessful in their efforts to direct public policyis they band together and pool their money toback candidates with whom the groups believethey can work. We must do this too. I encour-age you to join MEDPAC, the MMA’s bi-par-tisan political action committee. MEDPACworks to educate legislators and Congress mem-bers about pressing issues concerning the prac-tice of medicine. (Individual physicianmembership is $150, Alliance membership is$40, or joint physician/spouse is $250.) Mem-bership dollars go to help candidates who sup-port medicine – on both sides of the aisle. Note:membership in MEDPAC doesn’t “buy” legis-lators, governors or members of Congress. Itgets us a seat at the table during important dis-cussions. And now, more than ever, physicianand spouse financial support is critical to the
preservation of what little remains of the phy-sician/patient relationship. It’s nothing short ofan investment in the future of medicine.
Build relationshipsOnce you’ve determined the candidates yousupport, get to know them. Host fundraisersor at least attend them. Volunteer to work ontheir campaigns. Thousands of people vie foran elected official’s attention. Anything you doto get to know your representatives will improveyour chances of being heard.
Where does the RMS Alliance fit into thispicture? One of our goals this year is to increasethe involvement of our members in the politi-cal process. We’re devoting our January meet-ing to a conversation with a legislative leaderwho will provide insight into how we can makea difference at the State Capitol. Each of ournewsletters will include information about howto get involved and develop political clout. Al-liance representatives serve on MEDPAC andthe MMA Legislative Committee and are valu-able resources to Alliance members.
A member of the Pennsylvania MedicalAssociation Alliance recently posted a great “goget ’em” letter on the AMA Alliance listserv –yet another great source of information! Hermessage was this: Physicians and their spousesneed to think of politics as “a prescription forthe future of medicine…Hate politics? Swal-low hard and consider it a pill we have to takein order to cure medicine’s myriad of ills.”
You might even find you enjoy it. ✦

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 29
THMS-Officers
Chair David L. Swanson, M.D.
President T. Michael Tedford, M.D.
President-Elect Michael B. Ainslie, M.D.
Secretary Richard M. Gebhart, M.D.
Treasurer Paul A. Kettler, M.D.
Immediate Past Chair Virginia R. Lupo, M.D.
HMS-Board Members
Michael Belzer, M.D.
Carl E. Burkland, M.D.
Jeffrey V. Christensen, M.D.
Drew Dietz, Medical StudentAndrea J. Flom, M.D.
Diane Gayes, Alliance Co-PresidentPeggy Johnson, Alliance Co-PresidentRonald D. Osborn, D.O.
James Peters, M.D.
James A. Rhode, M.D.
David F. Ruebeck, M.D.
Richard D. Schmidt, M.D.
Michael G. Thurmes, M.D.
D. Clark Tungseth, M.D.
Michael J. Walker, M.D.
Joan M. Williams, M.D.
HMS-Ex-Officio Board Members
Paul F. Bowlin M.D., Senior Physicians AssociationLee H. Beecher, M.D., MMA-TrusteeKaren K. Dickson, M.D., MMA-TrusteeJohn W. Larsen, M.D., MMA-TrusteeRobert K. Meiches, M.D., MMA-TrusteeHenry T. Smith, M.D., MMA-TrusteeDavid W. Allen, Jr., MMGMA Rep.
HMS-Executive Staff
Jack G. Davis, Chief Executive OfficerKathy Dittmer, Executive Assistant
CHAIR ’S REPORTD A V I D L . S W A N S O N , M . D .
Our Membership Challenge
THIS IS THE LAST of these columns that Iwill write as chairman of the Hennepin Medi-cal Society. It has been a rewarding past yearoverseeing the work of this very special organi-zation, whose mission dovetails seamlessly withits partner, Ramsey Medical Society. The effec-tiveness of both societies as advocates of presentand future physicians in the metro communitycontinues to grow. I believe that we are seeingour societies emerge as significant players in theever-changing local health care scene. I think,looking over this edition of MetroDoctors, any-body can see how true this is.
There remains much work to be done. Wecan embrace a great opportunity for us to re-claim the direction of health care. But we havea problem we must first resolve–membership.For the first time in its history, the HennepinMedical Society represents less than 50 percentof the practicing physicians in our service area.
Our societies can never achieve their fullpotential while less than half of metro physi-cians belong to the societies. I believe there arethree reasons why physicians, especially young,employed physicians, choose not to join ourorganizations.
The first has to do with the definition ofprofessionalism as opposed to employment. Ithink many physicians have not made the philo-sophical leap that defines medicine as more thana career. Medicine is a profession. Belongingto professional societies is a big part of being aprofessional. When physicians are asked to giveexpert witness, in court or before Congress forexample, one of the first questions they areasked is, “To what professional societies do youbelong?” The public recognizes the contextualvalue of physician membership in professionalsocieties. Fortunately, our young doctors-to-beare getting the message about professionalism.We have been very successful in recruitingmedical students in our organizations; they arevery active and professionally sophisticated andsee the value of membership. We have yet toaggressively pursue resident physicians, whomay not be internalizing the importance of pro-
fessionalism in their futures. Unlike the MayoClinic, where virtually all residents are mem-bers of the county medical society, our localtraining institutions have not emphasized thevalue of membership in professional societies.We hope to work with the new Dean, as wedid with the old, to change this.
The second reason is a perception thatthe societies may not be giving physicians anadequate return on their membership invest-ment. Physicians ask, “What are the societiesdoing on behalf of the physician?” Metro phy-sicians demand advocacy. We have addressedthis problem by changing our mission and stra-tegic plans, as readers of MetroDoctors know.When the nursing strike threatened the care ofour patients, our organization was there readyto help coordinate patient triage. When themetropolitan physician credentialing systemcollapsed, we filled the gap to ensure all physi-cians remained credentialed to practice. Whenbioterrorism loomed threateningly after 9/11,we sponsored programs to bring the providernetwork up to speed. We continue our workwith the plans advocating fair contracting, aproject which has been very successful so far.We remain committed to our advocacy at theCapitol, which has been a major focus over thepast year. With all that we do, our major short-coming is that we have done a poor job tellingour colleagues who are not society membershow valuable we are to them. It is time to ag-gressively market our successes and we will dothis.
Lastly, society membership is expensive,especially for young, salaried physicians withsmall kids and big debt, who pay membershipfees with after-tax dollars. Making membershipaffordable for them requires “out-of-the-box”
(Continued on page 30)
He
nn
ep
in
Me
dic
al S
oc
ie
ty

30 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
The following participated in the June Community InternshipProgram sponsored by the Hennepin Medical Society: Heidi Holste,Committee Administrator, Health & Human Services Policy Committee,Minnesota House of Representatives; M. Thomas Blum, M.D., GroupHealth, West Clinic, CIP Faculty; Patricia Riley, CEO, Stratis Health;Michael B. Miller, JD, Senior Assistant County Attorney, HennepinCounty; and Jack G. Davis, CEO, Hennepin Medical Society. Notpictured: Michael Grover, Health Care Workforce Analyst, MinnesotaDepartment of Health.
Drs. Eric Anderson (far left) and Daniel Dunn (far right) hostcommunity interns Michael Grover and Michael Miller in surgeryat Abbott-Northwestern Hospital.
Community Internship Program
HMS NEWS
thinking. We have proposed delinking themembership requirement we have with theMMA, giving young physicians a choice of join-ing either the MMA or county society. Cur-rently, a physician who wishes to join the MMAmust also join the county society, and vice versa.They must pay dues to both organizations inorder to belong to either one. Just as the MMAhas delinked its combined membership require-ment with the AMA, we have proposed thatthe MMA delink with the component societ-ies. This would allow physicians to join onesociety or the other if they cannot afford both.Our rationale is that professional membershipis much more attractive if it is affordable, andit is better for the state and local societies as awhole if together they represent a greater pro-portion of practicing physicians.
Professionalism and advocacy are whyphysicians must belong to HMS, RMS, andMMA. Affordability will make it possible tobring our lost lambs into the fold.
Please accept my sincere gratitude for hav-ing the opportunity to serve you in this leader-ship role. Also, thank you to the other physicianleaders and boards of HMS and RMS for theadvice and service they provide and the hoursthey have donated. Lastly, thank you to JackDavis, Nancy Bauer, Kathy Dittmer, RogerJohnson and all the staff of our professionalsocieties. You cannot imagine how much theycare about you and with what high regard theyhold you. ✦
David L. Swanson M.D., HMS Board Chair-man, can be reached at: [email protected].
Chair’s Report(Continued from page 29)
Dr. Walker Hinck, Bloomington LakeClinic, discusses family medicine withcommunity intern Heidi Holste.

MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies September/October 2002 31
HMS and RMS Staff met with the newleadership of the University ofMinnesota Medical School studentgroup. Planning took place regardingstudent activities for the upcoming schoolyear. Our plans include a welcoming picnicin August for all the first year students, theWhite Coat Ceremony in October, five or six“Lunch ’n Learn” programs, studentresolutions for the upcoming MMA AnnualMeeting, the “Connections” mentoringprogram, “Shadow a Physician” program,HMS and RMS board representation andmembership recruiting. We’re off andrunning for the 2002/2003 school year.
Jack Davis, HMS CEO, was recently electedChair of the Board for the aMinnesotaVisiting Nurses Agency (MVNA). Jackhas been a member of the Board of Directorsfor the last four years.
Benjamin Whitten, M.D., HennepinMedical Society member, was recentlynominated by the MMA Board of Trustees asAlternate Delegate to the AMA House ofDelegates. An election will take place at theAnnual Meeting of the MMA in September.
Stuart Hanson, M.D. and Nancy Bauer,former HMS Associate Director, have beenworking on the final draft of an AMAGuidebook titled Diagnosing andTreating Abusive Behavior in theMedical Workplace. The guidebook isthe result of efforts of HMS members and staffover the last decade to address the problem ofabuse in the medical workplace. A five-stageprocess has been created to address the issueand is the subject of the guidebook. Theguidebook will be published this coming falland is supported by a grant from MMIC.
The Hennepin Medical Foundationheld a meeting on June 4. Marvin Segal,M.D., board chair, was joined by other boardmembers, Joseph Tombers, M.D., PeggyJohnson, Diane Gayes, and Jack Davis. TheBoard reviewed the investment strategy andperformance of the Foundation and approvedthe 2001 audit. The Board also approved the2002 member solicitation campaign.According to Dr. Segal, “this year’s campaignwill be more important than ever. The softeconomy may affect members giving at thevery time when society’s needs areexpanding.” Watch for this year’s solicitationcampaign this fall.
Jack Davis was recently elected byhis peers to represent County MedicalSocieties in an upcoming and continuingdialog with Michael Maves, M.D. EVP ofthe AMA. These meetings are slated to beheld on a quarterly basis in Chicago.
The HMS Board of Directorswelcomes James “Jamie” Peters,M.D. as a new member. Dr. Peters representsthe medical staff of Fairview-UniversityMedical Center. He specializes in FamilyPractice and since 1995 has been a memberof the full time faculty of the University ofMinnesota Department of Family Practiceand Community Health. Dr. Peters is locatedat the Smiley’s Clinic Program inMinneapolis. Dr. Peters attended RushMedical College in Chicago and completedhis residency at the University of Minnesota.In 2000, Dr. Peters received a BushFellowship and pursued studies in healthpolicy and administration.
Lee Beecher, M.D. has been nominatedto a second term as a Hennepin MedicalSociety Trustee to the MMA Board ofTrustees. David Estrin, M.D. has also beennominated to a first term to the MMA Boardof Trustees representing HMS.
The HMS Executive Committee announcedthat the Shotwell Award, which
HMS IN ACTIONJ A C K G . D A V I S , C E O
HMS in Action highlights activities thatyour leadership and executive office staffhave participated in, or responded to,between MetroDoctors issues. We solicityour input on these activities and encour-age your calls regarding issues in which youwould like our involvement. originated at Metropolitan Medical Center in
1971, has found a permanent home atAbbott Northwestern Hospital. Since theclosure of Metropolitan-Mount SinaiMedical Center, the award has been housedat the Hennepin Medical Society offices. Themedical society will still be active in theannual selection of the award recipient, butthe commemorative plaque listing all thehonorees will be publicly displayed on theAbbott Northwestern Hospital campus.
David Swanson, M.D. and his wifeCatharine, along with two of their threechildren, attended the AMA StudentSection picnic at Como Park on August12. Joining the Swansons were MichaelAinslie, M.D. and his wife Kathryn, andMichael Gonzalez-Campoy, M.D., president-elect of the Ramsey Medical Society. Thepicnic occurs annually on the first day oforientation for the incoming first yearmedical students. The purpose of the event isto welcome the new medical students to theprofession and to introduce them to thebenefits of organized medicine.
Roger Johnson, CEO of the Ramsey MedicalSociety, and Jack Davis met with GregVercellotti, M.D., Senior Associate Dean forEducation at the University of MinnesotaMedical School, and representatives of theMinnesota Medical Foundation and theMedical Alumni Society to establish thisyear’s “Connections” MedicalStudent Mentoring Program. Eachmember of the Ramsey and HennepinMedical Societies will soon be receivinginvitations to participate in this valuableprogram. ✦
He
nn
ep
in
Me
dic
al S
oc
ie
ty

32 September/October 2002 MetroDoctors The Journal of the Hennepin and Ramsey Medical Societies
HMS ALLIANCE NEWS
Peggy JohnsonCo-President
Diane GayesCo-President
Only 230 tickets are available, and are for sale NOW! Please join HMSA members, families, and friends for thisHMSA sponsored event. After August 1, 2002, any remaining tickets will be available to the general public.Proceeds will benefit HMSA philanthropic endeavors such as Body Works and the AMA Foundation.
___ YES! Please send me ____ tickets at $160 each for dinner & Gerald Charles Dickens’ performance ofA Christmas Carol on December 20, 2002 at the Interlachen Country Club, Edina, Minnesota.• I have enclosed a check payable to HMSA Philanthropic for $_____
$100 of each ticket is tax-deductible.• Sorry, we cannot attend but enclosed please find a tax-deductible donation to HMSA Philanthropic Fund.
Your name: ________________________________________________________Mailing address: _____________________________________________________Phone number:______________________________________________________Send your check and this completed form to:HMSA – Peggy Johnson, 6229 Fox Meadow Lane, Edina, MN 55436
Gerald Charles DickensGreat-great grandson of Charles Dickens
presents “A Christmas Carol”
A world-acclaimed one-man performance! Gerald Charles Dickensbrings to life the Charles Dickens’ Christmas classic in 26 voices.
His performances have been described as “powerful, energetic, andinteractive.” His audiences are enthralled and respond with standingovations.
Dickens books, gifts, and collectibles offered by Jackson Enterprises,Inc. will be available for sale and signing by Mr. Dickens.
Questions? Contact Diane Gayes or Peggy Johnson at HMSA, 612/623-3030.Event details are available at: www.jackprises.com
Date: Friday evening, December 20, 2002Place: Interlachen Country Club, EdinaTime: 6:00 p.m. Social Hour (cash bar)
7:00-10:00 p.m. Dinner and Performance

FOR DETAILS AND TEST DRIVES CONTACTSTEVE ALLEN AT MCCARTHY’S HUMMER.
2325 Prior Avenue North, Roseville, MN
(651) 636-6060
BRED FROM THE VEHICLESYOUR MILITARY BUYS! H2, THENEW 2003 KID ON THE BLOCK! (available July 2002)
THE FEW, THE PROUD,THE SUCCESSFUL!

�������������� ������ ��������� ������������ ������ ��������
����������������� �����������������������������
��������������� ���!�������!�"�� �###$%&$ %�$& '(%
)*�+��,���-��.����������������/ �������� ���-�& (������&�%���-
C O N T I N U I N G M E D I C A L E D U C A T I O NContinuing Education and Extension, University of Minnesota
������� ������ ������ ���
���%0���� �1�&�����
1�,.����2���� ���$�3� �
��������������������
���%0���� �1�&�����
1�,.����2���'1�,��&�3�,�(
4����5��� ���$�3� �
����������� ������� ��
!�� ��������
���%0������� �1�&�����
1�,.���� ���$�3� �
! ��������"##"$���� ����
%� ����
���%0������� �1�&�����
2�������&�%� �����$
� ���� �������������
�����
���%0������� �6�(��1����
1���� �6�(��1������47
&'��������� � �����������
��������� ���
���%0�����!� �4� �3�����
�*��������&�%� �����$
������� ����� �������(��)�� �
���%0��!� �1�&������2���
���&�%� �����$
*����&�� �������&��� ���
+�������
�(��0�"� �2������8�����
6���%��9���
, ���� ��)�� ��$������� ��
� ����������
�(��0����� �1�&������2���
���&�%� �����$
������ ����!��'$�%�����
!� ���)�������
�(��0���!� �1�&������2���
���&�%� �����$
� ��� ��"##"����� ��� �
%���� ��������!��'
�(��0������ �1�&������2���
���&�%� �����$
������ ��� ������������
�(��0��!� �1�&������2���
���&�%� �����$
�������'���-� ���&����
���������
�(��0���� �:� 0���2���
������.�8%�(�� �6���%��9���
.���� ���� ������ ��
�������.�����*���-�����
�(��0������&���,%0���
6�������-��6�&9$� �+��.��
5�%� �� �����$
+/�������� ���0��������
�(��0��!���� �1�&�����
2�������&�%� �����$
�1&1�-���� ���� �������
���������
��,%0��� �1�&������2���
���&�%� �����$
�� ��� ��,���� ����$
���������� ��������� �����
��,$�!���� �2-����19�(-� �����$
��������(��� ���$
��� ��
��,%0��� �4� �3�����
�*�����5������� ���$�3� �
��������%� ���������
������ ���� ����� �������2
����� ����&�� ��
��,$���� �2-����19�(-� �����$
� ����� ������������$
��� ����� ����� �����
��,$��"� �8�����2������ �6�%9��$