15 Gallbladder, pancreas, liver & spleen - primary surgery · 15 Gallbladder, pancreas, liver &...
28
285 285 15 Gallbladder, pancreas, liver & spleen 15.1 Introduction The gallbladder may be diseased due to stones, ascaris (15.6), infection per se, tumour or volvulus. The frequency of these diseases varies from region to region, but stones are more common in women than in men, and especially in obese, parous women >40yrs (fat, fertile, female over forty). Gallstones are found in c.80% of adults with sickle cell disease. Many patients are found at postmortem to have gallstones which have caused no symptoms. Just because someone has gallstones, they may not be the cause of dyspepsia! Stones or thick biliary sludge may however pass into the common bile duct and cause biliary colic, or obstructive (cholestatic) jaundice. Stones can promote infection of the gallbladder and cause acute or chronic cholecystitis, although this can arise de novo especially with HIV disease. Stones, especially in the form of gravel (sludge), can also promote infection in the biliary tree, especially in association with obstruction (cholangitis, 15.7) though this may also arise de novo; they can also obstruct drainage of the pancreas and cause pancreatitis. Rarely stones may fistulate into the small bowel and cause obstruction therein. You can usually treat acute cholecystitis non-operatively (15.3), but if this fails, you can drain the gallbladder by doing a cholecystostomy. If you are experienced enough, you can treat chronic cholecystitis by removing the gallbladder (15.8). If obstructive jaundice is due to carcinoma of the head of the pancreas, you may be able to relieve the symptoms by bypassing the obstruction and performing a cholecysto-jejunostomy (15-5), but the situation is more complicated if the obstruction is due to gallstones, ascaris, clonorchis sinensis (Chinese liver fluke) or tumour obstructing the bile duct. You can usually treat acute pancreatitis non-operatively (15.13), but a pancreatic abscess (15.15), and a large pancreatic pseudocyst (15.14) need drainage. You will not be able to remove a pancreatic carcinoma, which may be very difficult to differentiate from chronic pancreatitis. Likewise you will not be able to remove tumours of the liver whether primary (hepatoma) or secondary except with sophisticated equipment, and only when presenting early. However you will be able to treat hepatic tuberculosis. You may have to drain liver cysts, and may need to remove large hydatid cysts carefully (15.12). You may need to drain liver abscesses especially if they are large (15.10), and likewise splenic abscesses (15.18), which you can usually best deal with by splenectomy. This is also indicated for a number of diseases, other than for trauma (15.17). Splenic tuberculosis is usually only diagnosed after you have removed the spleen! 15.2 Biliary colic Biliary colic is due to a stone or sludge impacting in the cystic duct. Very rarely it may be due to volvulus of the gallbladder. There is severe colicky epigastric pain which radiates to the right subcostal region and right scapula. The patient wants to bend herself double, she rolls around, and rarely keeps still. Intense pain comes in waves against a background of a dull ache, typically in attacks lasting about ½hr, 1-3hrs after a fatty meal. Pain makes breathing difficult and may be accompanied by nausea and vomiting. Attacks occasionally last as long as 6hrs. If unrelieved >24hrs, cholecystitis develops. There may be tenderness in the hypochondrium or the right epigastrium, and be a +ve Murphy's sign (15.3). ULTRASOUND is a simple, cheap and accurate way of finding stones in the gallbladder, whether or not there is jaundice: they cast an ‘acoustic shadow’ behind them (38-5). Occasionally you might find ascaris in a bile duct (15.6). N.B. RADIOGRAPHS. Most gallstones do not show up, so a plain film is unlikely to help. DIFFERENTIAL DIAGNOSIS OF BILIARY COLIC Suggesting ureteric colic: pain radiating towards the groin and genitalia. Blood in the urine on microscopy. Radio-opaque calcifications on abdominal radiographs along the line of the ureter. Suggesting right basal pneumonia: cough, fever, and lung signs at the right base. Suggesting upper small bowel obstruction: central colicky pain with profuse unrelieved vomiting. NON-OPERATIVE TREATMENT OF BILIARY COLIC. Treat with pethidine 50-100mg 3-hrly IV or IM, for 24-48hrs. Hyoscine 20mg may help. Restrict to clear fluids only by mouth. If vomiting ensues, replace fluids IV. Normally, pain will stop in 24-48hrs, and you can start feeding cautiously, avoiding oily or fatty foods. If symptoms persist >24hrs with tenderness in the right hypochondrium, acute cholecystitis has developed. 15.3 Acute cholecystitis Symptoms are often initially those of biliary colic (15.2), but they last >24hrs and pain becomes constant. There is a very good chance of recovery in 10days, even without treatment. There is a 5% chance that (1) the infection will build up in the gallbladder to produce an empyema, (2) peritonitis will develop, (3) a fistula into bowel will occur from a perforation of the gallbladder. Recurrent episodes of cholecystitis are likely in >50%.
Transcript of 15 Gallbladder, pancreas, liver & spleen - primary surgery · 15 Gallbladder, pancreas, liver &...

285
285
15 Gallbladder,
pancreas, liver &
spleen
15.1 Introduction
The gallbladder may be diseased due to stones, ascaris
(15.6), infection per se, tumour or volvulus. The frequency
of these diseases varies from region to region, but stones
are more common in women than in men, and especially in
obese, parous women >40yrs (fat, fertile, female over
forty). Gallstones are found in c.80% of adults with sickle
cell disease. Many patients are found at postmortem to
have gallstones which have caused no symptoms.
Just because someone has gallstones, they may not be the
cause of dyspepsia! Stones or thick biliary sludge may
however pass into the common bile duct and cause biliary
colic, or obstructive (cholestatic) jaundice. Stones can
promote infection of the gallbladder and cause acute or
chronic cholecystitis, although this can arise de novo
especially with HIV disease. Stones, especially in the form
of gravel (sludge), can also promote infection in the biliary
tree, especially in association with obstruction
(cholangitis, 15.7) though this may also arise de novo;
they can also obstruct drainage of the pancreas and cause
pancreatitis. Rarely stones may fistulate into the small
bowel and cause obstruction therein.
You can usually treat acute cholecystitis non-operatively
(15.3), but if this fails, you can drain the gallbladder by
doing a cholecystostomy. If you are experienced enough,
you can treat chronic cholecystitis by removing the
gallbladder (15.8). If obstructive jaundice is due to
carcinoma of the head of the pancreas, you may be able to
relieve the symptoms by bypassing the obstruction and
performing a cholecysto-jejunostomy (15-5), but the
situation is more complicated if the obstruction is due to
gallstones, ascaris, clonorchis sinensis (Chinese liver
fluke) or tumour obstructing the bile duct.
You can usually treat acute pancreatitis non-operatively
(15.13), but a pancreatic abscess (15.15), and a large
pancreatic pseudocyst (15.14) need drainage.
You will not be able to remove a pancreatic carcinoma,
which may be very difficult to differentiate from chronic
pancreatitis. Likewise you will not be able to remove
tumours of the liver whether primary (hepatoma) or
secondary except with sophisticated equipment, and only
when presenting early. However you will be able to treat
hepatic tuberculosis. You may have to drain liver cysts,
and may need to remove large hydatid cysts carefully
(15.12). You may need to drain liver abscesses especially
if they are large (15.10), and likewise splenic abscesses
(15.18), which you can usually best deal with by
splenectomy. This is also indicated for a number of
diseases, other than for trauma (15.17).
Splenic tuberculosis is usually only diagnosed after you
have removed the spleen!
15.2 Biliary colic
Biliary colic is due to a stone or sludge impacting in the
cystic duct. Very rarely it may be due to volvulus of the
gallbladder. There is severe colicky epigastric pain which
radiates to the right subcostal region and right scapula.
The patient wants to bend herself double, she rolls around,
and rarely keeps still. Intense pain comes in waves against
a background of a dull ache, typically in attacks lasting
about ½hr, 1-3hrs after a fatty meal. Pain makes breathing
difficult and may be accompanied by nausea and vomiting.
Attacks occasionally last as long as 6hrs. If unrelieved
>24hrs, cholecystitis develops. There may be tenderness in
the hypochondrium or the right epigastrium, and be a
+ve Murphy's sign (15.3).
ULTRASOUND is a simple, cheap and accurate way of
finding stones in the gallbladder, whether or not there is
jaundice: they cast an ‘acoustic shadow’ behind them
(38-5). Occasionally you might find ascaris in a bile duct
(15.6).
N.B. RADIOGRAPHS. Most gallstones do not show up,
so a plain film is unlikely to help.
DIFFERENTIAL DIAGNOSIS OF BILIARY COLIC
Suggesting ureteric colic: pain radiating towards the
groin and genitalia. Blood in the urine on microscopy.
Radio-opaque calcifications on abdominal radiographs
along the line of the ureter.
Suggesting right basal pneumonia: cough, fever,
and lung signs at the right base.
Suggesting upper small bowel obstruction: central
colicky pain with profuse unrelieved vomiting.
NON-OPERATIVE TREATMENT OF BILIARY COLIC.
Treat with pethidine 50-100mg 3-hrly IV or IM,
for 24-48hrs. Hyoscine 20mg may help.
Restrict to clear fluids only by mouth. If vomiting ensues,
replace fluids IV.
Normally, pain will stop in 24-48hrs, and you can start
feeding cautiously, avoiding oily or fatty foods.
If symptoms persist >24hrs with tenderness in the right
hypochondrium, acute cholecystitis has developed.
15.3 Acute cholecystitis
Symptoms are often initially those of biliary colic (15.2),
but they last >24hrs and pain becomes constant.
There is a very good chance of recovery in 10days, even
without treatment. There is a 5% chance that
(1) the infection will build up in the gallbladder to produce
an empyema,
(2) peritonitis will develop,
(3) a fistula into bowel will occur from a perforation of the
gallbladder. Recurrent episodes of cholecystitis are likely
in >50%.

286
286
In HIV disease, the gallbladder can be markedly inflamed
without the presence of stones (acalculous cholecystitis).
This is due to cryptosporidia or cytomegalovirus in 20%,
and produces an ischaemia of the gallbladder wall.
Infection may also be present with salmonella; in typhoid,
organisms infect the gallbladder but cholecystitis is often
masked by generalised peritonitis. Cholecystitis without
stones may also be caused by brucellosis, dengue,
leptospirosis & campylobacter.
Stones may be in the gallbladder but also in the bile duct
and cause partial or complete obstruction with jaundice or
cholangitis. Biliary débris at the sphincter of Oddi may
result in pancreatitis.
Operate if:
(1) there is cholangitis which is life-threatening,
(2);the gallbladder forms a gradually enlarging acute
inflammatory mass,
(3);there are repeated attacks leading to chronic
cholecystitis.
The acutely inflamed gallbladder is oedematous,
and perhaps gangrenous, and often adherent to
surrounding structures, so do not try to remove it unless
you are experienced. Instead, drain it (cholecystostomy).
This may be life-saving and is simple and safe, but it may
not cure the disease permanently, so you may have to think
of a cholecystectomy later.
N.B. Never try to repair a perforation in an inflamed
gallbladder.
Repeated attacks of acute inflammation are usually less
severe than a typical acute attack. Symptoms may subside
without infection and leave the gallbladder shrunken and
fibrosed. However, if a stone remains impacted in
Hartmann’s pouch (15.4, 15-3M), the gallbladder will
distend with fluid (mucocoele of the gallbladder) and if
this becomes infected, the subsequent distension with pus
(empyema of the gallbladder) may cause it to burst.
SIGNS.
The patient is febrile, looks sick, and lies still. There is
well localized tenderness in the right upper quadrant.
There may be exquisite tenderness (unlike biliary colic),
with guarding and rigidity. Murphy's sign is usually +ve:
MURPHY'S SIGN. Put your hand under the ribs on the right side, and ask the patient to take
a deep breath. If she feels pain as the gallbladder moves down on to your
hand, the sign is +ve and indicates cholecystitis.
A well-localized mass sometimes forms a few days after
the start of the attack, just below the right costal margin.
Mild jaundice does not always mean that the common bile
duct is obstructed by a stone. If there is jaundice, swinging
fever, chills and rigors, however, suspect cholangitis.
SPECIAL TESTS. There is a leucocytosis, unless there is
untreated HIV disease. The serum bilirubin and alkaline
phosphatase will only be raised if there is obstruction of
the biliary tree. The amylase & lipase are raised in
pancreatitis.
ULTRASOUND. Gallstones readily show up with an
‘acoustic shadow’. With experience you will be able to
see if the common bile duct is dilated and if more stones
are found inside the duct. The presence of stones may
imply cholecystitis, but does not prove it. To confirm the
diagnosis, you need to see a thickened gallbladder wall
and/or fluid around the gallbladder (38.2B).
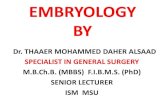
Fig 15-1 CHOLECYSTOSTOMY.
A, right subcostal (Kocher’s) incision. B, insert a purse string suture.
C, aspirate the gallbladder. D, remove the stones. E, insert a Foley
catheter. Kindly contributed by Gerald Hankins.
DIFFERENTIAL DIAGNOSIS OF ACUTE CHOLECYSTITIS
Suggesting liver abscess (15.10): tender hepatomegaly
with fever and previous diarrhoea and dry cough.
Suggesting perforated peptic ulcer (13.3): sudden onset
of extreme constant pain, with previous dyspepsia.
Suggesting acute pancreatitis (15.13): pain radiating to
the back, with alcohol abuse.
287
287
Suggesting acute pyelonephritis: pain in the flank
associated with urinary frequency, haematuria and
previous ureteric colic or schistosomiasis.
Suggesting volvulus of the small bowel with
strangulation (12.8): initial colicky pain which then
became constant, associated with abdominal distension,
tenderness and guarding.
Suggesting perihepatitis (Curtis-Fitzhugh syndrome):
previous episodes of PID, especially with HIV disease.
Suggesting haemorrhage in a liver tumour: tender knobbly hepatomegaly with weight loss and
anorexia.
NON-OPERATIVE TREATMENT FOR ACUTE
CHOLECYSTITIS Make sure of the diagnosis with ultrasound (38.2B) and
repeated examination. Perform an OGD (13.2) if you can,
to exclude reflux oesophagitis, gastritis or peptic
ulceration as differential diagnoses.
Treat pain with enough opioid: e.g. pethidine (50-100mg
3hrly). Nasogastric suction is not essential, but it will keep
the stomach empty and so relieve nausea and vomiting.
Keep nil orally. Correct the initial fluid loss with IV saline.
Antibiotics are less necessary than you might expect,
because the inflammation in the gallbladder is primarily
chemical. However they probably reduce complications:
treat with chloramphenicol (or gentamicin), ampicillin,
or doxycycline. Continue this treatment till the pain and
pyrexia settle; then introduce oral fluids and after this
allow a fat-free diet. Symptoms should start to improve
after 24hrs, and disappear in 3wks. Advise a low-fat diet,
and review after 2-3 months.
If symptoms recur, repeat the treatment for acute
cholecystitis. When things have settled, think about an
elective cholecystectomy, usually six weeks afterwards,
if stones are definitely present. Do not operate for
acalculous cholecystitis unless there is marked tenderness
and you fear imminent perforation.
15.4 Empyema of the gallbladder
When cholecystitis gets worse, the gallbladder enlarges
and becomes a tense inflammatory mass. This may occur
if the cystic duct is obstructed with a gallstone, or
secondary to carcinoma. The gallbladder fills with pus
and so becomes an empyema; it then may perforate
resulting in septic biliary peritonitis which is frequently
fatal.
The patient is sick, pyrexial, lies still and has a painful
tender mass in the right hypochondrium below the liver.
There may be a known history of gallstones, but usually
not of jaundice.
SPECIAL TESTS. Leucocytosis progresses from earlier in
the disease. Amylase is usually normal.
ULTRASOUND. The gallbladder is filled with turgid
fluid, and often gallstones; its wall is thickened (38.2B).
Aspiration may relieve some symptoms in a very sick
patient, but is not a lasting solution.
CHOLECYSTOSTOMY (GRADE 3.3)
INDICATIONS. Drain the gallbladder if:
(1) intense pain persists with swinging fever,
(2) abdominal tenderness gets worse, the area of guarding
extends, or the mass increases in size both suggesting an
empyema of the gallbladder,
(3) there is cholangitis with a distended gallbladder (15.7),
(4) the patient is too sick to undergo a cholecystectomy.
ANAESTHETIC. If the patient is very sick or very old you
can operate under LA, especially if the gallbladder is tense
and easily palpable under the abdominal wall.
PREPARATION. Make sure your suction is working
properly. Treat with gentamicin and metronidazole.
INCISION. Feel for the area of maximum tenderness,
an ill-defined mass, or both (15-1A). Centre the incision
over this area, and cut through all layers of the abdominal
wall 2cm below and parallel to the line of the costal
cartilages. You will probably find the gallbladder easily.
If you do not find it, carefully separate the adherent
omentum and transverse colon by pushing them away with
your finger. Pack away the rest of the abdominal contents
away from the inflamed gallbladder. This will be easier if
you tilt the table feet down. Handle the gallbladder
carefully; it easily ruptures and spills infected bile into the
peritoneal cavity.
If the structures below the right lobe of the liver are matted
together in an oedematous haemorrhagic mass, so that the
gall bladder is difficult to find, insert your hand over the
upper surface of the liver, and draw your fingers down
until you reach its edge. Then move your hand medially
over the convex surface of the liver until you reach the
falciform ligament, joining the liver to the diaphragm.
At its lower edge is the ligamentum teres. About 5cm to
the right of this, you should be able to feel the tense,
turgid, elongated mass of the fiery-red, acutely inflamed,
oedematous, and perhaps partly necrotic gallbladder.
Try to expose enough of the fundus of the gallbladder to
allow you to drain it. Use your finger, or a 'swab on a stick'
(4-9A), to 'peel' the omentum, the hepatic flexure of the
colon, and the transverse mesocolon carefully out of the
way. Avoid sharp dissection. If there is bleeding, control
the haemorrhage with packs.
Put a purse-string suture on the gallbladder fundus
(15-1B), incise it and aspirate the pus (15-1C).
Then enlarge the opening and extract as many stones as
you can (15-1D); if they are very adherent in Hartmann’s
pouch (15-3M), leave them, rather than perforating the
gallbladder. Do not attempt to explore the common bile
duct.

288
288
Place a wide-bore catheter, which you have inserted
through a separate stab incision in the lateral abdominal
wall, in the gallbladder, and close the opening around the
catheter snugly with 2 purse-string sutures, one 5mm away
from the other (15-1E). Secure the catheter drain and
attach it to a drainage bag. Lavage the abdomen with warm
water.
DIFFICULTIES WITH EMPYEMA OF THE GALLBLADDER
If you cannot reach the inflamed gallbladder,
extend your incision across the midline as an inverted-V.
If you do not find a tense inflamed gallbladder at operation, look for differential diagnoses and act
appropriately.
If the gallbladder is not that seriously inflamed,
and you are able to do so, perform a cholecystectomy
(15.8).
If you rupture the gallbladder at Hartmann’s pouch (15-3M), which is a mucosal fold between the neck of the
gallbladder and the cystic duct, sometimes caused by
adhesions between them, where gallstones commonly get
stuck. It may be present in both normal and pathological
gallbladders. Try to remove any impacted stone (which
should be freed up by your manipulations) and if possible
put a ligature around the cystic duct remnant. Remove as
much of the inflamed gallbladder as you can (if the
posterior wall is very adherent to the liver, leave it)
and insert a wide-bore drain through a separate stab
incision in the abdominal wall.
If the gallbladder is so tense and inflamed and a suture
causes it to leak profusely, apply suction and remove as
much of the inflamed gallbladder as you can, as above.
If the gallbladder has already perforated, there is
already effectively a cholecystostomy and friable tissues
will make cholecystectomy too difficult. Aspirate septic
fluid from the abdomen and pack away the bowels.
Remove as much of the gallbladder wall as possible: you
can leave the posterior wall adherent on the liver surface.
Remove any debris and stones. Try to close the cystic duct
with an absorbable suture if you can. Leave a drain
brought out through a separate stab incision.
Fold some omentum into the bed of the gallbladder.
POSTOPERATIVELY, expect bile to start draining in a
day or two. Chart the daily amount of bile draining.
Plan to remove the tube in 14days. If the bile is still
discharging after 2wks however, leave the catheter in situ
for a month at least before removing it. If the bile loss is
significant, replace fluid and electrolytes IV. You can try
to return the bile to the intestines via a nasogastric tube if
the patient will tolerate it. The fistula will slowly close
unless a stone has been left in Hartmann’s pouch (when a
small mucous fistula will result, 15-3M).
N.B. The cholecystectomy needed to cure this problem
may be difficult indeed.
15.5 Cholangitis
Ascending cholangitis describes infection in the bile duct,
which if untreated, may be followed by multiple abscesses
in the liver, or by septicaemia. IV antibiotics are
necessary, but if stones are the underlying cause,
the common bile duct should be explored, and any stones
removed. This is difficult and needs special instruments
and on-table radiography. If it is impractical, and the stone
is distal, you may still be able to decompress
the common bile duct by inserting a T-tube
(choledochostomy), or by opening the duodenum and
opening the sphincter of Oddi wide, but this is difficult
surgery.
A patient with cholangitis usually has a previous history of
biliary colic and cholecystitis. Typically, an attack of colic
is followed the next day by fluctuating jaundice, dark
urine, pale stools, nausea and vomiting, fever and rigors.
The liver may be tender, but the gallbladder is not
palpable.
In HIV disease, cholangitis may occur intermittently
without the presence of stones, mimicking primary
sclerosing cholangitis. In East Asia, liver fluke infestation
often causes cholangitis (15.7). In endemic areas, consider
hydatid disease.
SPECIAL TESTS. Check if ascaris ova are in the stool:
this does not necessarily mean that worms are the cause of
cholangitis, but strongly suggests it (15.6).
ULTRASOUND (38.2) is very useful to confirm the
presence of stones, cysts or ascaris and their number and
position in a dilated common bile duct.
CHOLEDOCHOSTOMY (GRADE 3.5)
PREPARATION
Treat with IV ampicillin, gentamicin and metronidazole,
or substitute ampicillin & gentamicin with a
cephalosporin, ciprofloxacin, or mezlocillin.
If he is septicaemic, resuscitate the patient with Ringers
Lactate. Add Vitamin K 10mg IM. Insert a nasogastric
tube. Do not delay.
INCISION. Make an upper midline incision and follow the
initial steps to find the gallbladder (15.3), then expose the
subhepatic area, cystic duct, and common bile duct.
(The midline incision is better for exposure of the common
bile duct than a subcostal incision).
Expose the biliary tree as in a cholecystectomy (15.8),
but without grasping the gallbladder. Make sure you have
found the bile ducts before proceeding further.
Palpate them to be sure none of them pulsates! If in doubt,
aspirate the common duct to make sure it contains bile and
not blood. Then expose 2cm of the common bile duct,
which will probably be significantly dilated (>5mm)
(15-2A), and place two 3/0 stay sutures on its anterior
surface about 4mm apart (15-2B). With the tip of the
sucker close by, make a longitudinal incision, between the
stay sutures (15-2C). Suck out all the bile and exudate, and
take a swab for culture and sensitivity.

289
289
Using Desjardin's stone forceps, gently remove any stones
that you can easily see (15-2D). The curve on the forceps
may help you: the stones are probably well down the
common duct at its lower end, where it enters the
duodenum. Do not prolong this stage of the operation if it
is difficult: you can do much harm. If there is much
'sludge', wash out the common duct by irrigating it with
plenty of saline using a plain rubber catheter and a 20mL
syringe.
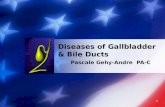
Fig. 15-2 CHOLEDOCHOSTOMY.
A, expose the common bile duct. B, insert stay sutures. C, incise the
common bile duct. D, remove the stones. E, insert a Fogarty catheter.
F, T-tube sewn in place. G, a T-tube.
EQUIPMENT. FORCEPS, gallstone, Desjardin's. Use these long slender forceps for removing stones from the biliary system.
If you do not have Desjardin's stone forceps, a Fogarty balloon catheter,
pushed past the stone, inflated, and withdrawn is often as effective and less traumatic. You may possibly be able to use a tiny Foley catheter.
Find 2 assistants in addition to the scrub sister.
Insert a T-tube (15-2E), and close the opening in the duct
snugly round the drainage tube with a transverse
absorbable 4/0 suture (15-2F).
Bring the tube out through a stab incision, leaving some
slack inside, in case it is pulled on. Anchor it securely to
the skin with a non-absorbable suture. (You can make your own T-tube by slitting the end of a piece of ordinary suction tubing, and cutting away ⅓ the circumference of the tubing.)
Close the abdominal wall carefully: the wound is likely to
break down or become infected, so consider leaving the
skin open (11.10, 11-20).
POSTOPERATIVELY, connect the T-tube to a bedside
bottle, and allow it to drain freely until the jaundice and
fever subside. Perform a tube cholangiogram 10-14days
postoperatively using 25% sodium diatrizoate (‘hypaque’)
or similar aqueous contrast medium diluted 1:2 with 0·9%
saline. Make sure you do not inject any air with the
contrast medium. If you see no stones, and the medium
flows nicely into the duodenum, clamp the tube.
Provided that there is no pain, fever, or jaundice after 1wk,
remove the tube.
If the cholangiogram shows blockage of flow into the
duodenum or any residual stones as filling defects,
try flushing the duct with 1l of warm saline suspended 1m
above the patient, after treating with hyoscine 20mg IM.
If this fails, check what pressure builds up. It should not be
higher than 8-10cm of water. If after 24hrs no higher
pressure develops, try clamping the tube. Remove it after
2wks if no discomfort develops. If pressure does build up
in the tube, do not remove it. You may then be able to
remove residual stones by dilating the T-tube tract
and pulling them out with endoscopy forceps
(the Burhenne technique), or they can be removed by an
expert by passing a side-viewing fibre-optic endoscope
into the duodenum and slitting the sphincter of Oddi,
or by opening the duodenum at laparotomy.
TRANSDUODENAL ODDI SPHINCTEROTOMY
(GRADE 3.5)
INDICATION. When a stone is impacted at the distal end
of the common bile duct; when antegrade extraction or
lavage has failed to dislodge a stone.
INCISION. Expose the biliary tree as before; then
mobilize the duodenum by the Kocher’s manoeuvre (13.5).
Make a 4cm longitudinal incision in the lateral surface of
the duodenum at the junction of first and second parts, and
feel the papilla with your finger through the duodenotomy.
If you can’t find it, pass a bougie or catheter down through
the common bile duct. Then insert a fistula probe into the
papilla and open it upwards with a #11 blade (4-1) to free
any impacted stones. When you see bile flowing freely
you know you have relieved the obstruction.
Carefully spatulate the edges of the papilla open with
absorbable 4/0 sutures. Be careful not to damage the
pancreatic duct (usually visible at the 5 o’clock position).
Close the duodenotomy transversely in 2 layers with
long-lasting absorbable 2/0 sutures, and cover this with
omentum if possible.
If the bile duct has been opened, place a T-tube as above.

290
290
15.6 Cholangitis caused by ascaris Ascaris worms sometimes crawl up into the common bile
duct and gallbladder, where they can cause biliary colic,
acute cholecystitis, obstructive jaundice, cholangitis,
and pancreatitis. This most often happens when a child has
been given an antihelminthic. So, if a child has cholangitis,
or if an adult does not fit the usual clinical picture for
biliary disease, suspect ascariasis. Finding ascaris ova
should arouse your suspicion, but does not confirm the
diagnosis. Get an ultrasound scan. Do not operate, except
on the indications below.
Nasogastric suction will empty the upper intestinal tract.
Systemic antibiotics will help to control the cholangitis.
Later, treat with levamisole 120mg stat, or piperazine 4g
stat, or if there is multiple parasitic infestation,
mebendazole 100mg od for 3 days, repeated after 15 days.
N.B. Dead ascaris worms may still block the bile duct!
SPECIAL TESTS. There is a microcytic hypochromic
anaemia, a leucocytosis with >50% eosinophilia; bilirubin
is raised in cholestatic obstruction and amylase in
pancreatitis. Ascaris lumbricoides eggs can be found in the
stool.
ULTRASOUND is best to determine if the ascaris worm
is no longer in the bile duct (38.2B).
INDICATIONS FOR SURGERY. Deepening jaundice,
spiking fever, chills and rigors which do not respond to
antibiotics; nausea and vomiting, toxaemia, dehydration,
tachycardia, and perhaps hypotension; together with a
leucocytosis. If there are these symptoms, explore and
drain the bile ducts (choledochostomy, 15.5) after
appropriate preparation. Remove any worms you find.
Avoid a sphincterotomy as ascaris may then more easily
crawl into the pancreatic duct subsequently.
15.7 Other causes of cholangitis
(1).In East Asia, liver flukes, opisthorchis, found in fish
and snails, are extremely common. Many thousands of
flukes can live for many years in the bile ducts causing
inflammation. Resulting fibrosis leads to stricturing and
dilation, secondary bacterial infection and stone
development. Recurrent cholangitis can lead to biliary
cirrhosis, liver failure, hepatorenal syndrome, portal
hypertension or septicaemia, as well as pancreatitis.
Recurrent inflammation may result in cholangiocarcinoma,
and chronic infestation can lead to a salmonella carrier
state if secondarily infected.
Presentation is usually at 20-40yrs (males more
commonly), initially with non-specific malaise but then
with a high swinging fever, chills, and rigors, a gnawing
right upper abdominal pain, and mild jaundice (Charcot's
triad), usually with a history of previous attacks.
The liver is tender and enlarged and the gallbladder may
be palpable. The urine is dark, but the stools are seldom
clay-coloured; complete obstruction of the common bile
duct is rare.
(2).Around the Mediterranean, in East Asia, Latin
America, sheep liver flukes, fasciola hepatica, are found.
These flukes are large and tend to remain in extrahepatic
bile ducts. The flukes may actually eat into the wall of the
ducts, which leads to haemobilia, presenting as
haematemesis and melaena, or more rarely perforate the
duct causing peritonitis. Inflammation leads to similar
complications as with opisthorchis, but because the extra-
hepatic ducts are preferentially involved, gallbladder
distension and empyema are more common
(3).Primary sclerosing cholangitis is an inflammatory
condition affecting both intra- and extra-hepatic bile ducts,
in men and women equally of 25-40yrs. Fatigue, weight
loss, right upper abdominal pain, intermittent jaundice and
itching are usual; an acute attack of cholangitis is rare.
A similar picture can arise in HIV disease (5.6), with or
without papillary stenosis. No medication has been found
helpful.
(4).Rupture of a hepatic hydatid cyst into the bile ducts
(15.12).
SPECIAL TESTS.
There is a leucocytosis (and eosinophilia with fluke
infestation); the serum bilirubin and alkaline phosphatase
are raised. If infection is severe and liver cells are
involved, the transaminases are raised. Measure the serum
amylase, because there is a 10% chance that there is also
pancreatitis. You may find ova and dead flukes in the
faeces and in duodenal aspirates.
RADIOGRAPHS.
A plain radiograph may show air in the biliary tract due to
an incompetent sphincter of Oddi.
ULTRASOUND often shows dilation of intra-hepatic
before extra-hepatic ducts, and may actually detect mobile
flukes (38.2B).
NON-OPERATIVE TREATMENT.
If the disease is mild, take blood cultures and treat with
antibiotics (cefradine or gentamicin, 2.8). Add vitamin K
10mg IM. Start intravenous fluids, restrict oral fluids and
aspirate the stomach through a nasogastric tube.
Praziquantel 25mg/kg tid for 2days is the most effective
treatment for opisthorchis but is ineffective against
fasciola, for which bithionol 1g tid alternate days for
5days is 100% effective.
INDICATIONS FOR OPERATION.
(1) Failure of non-operative treatment.
(2) A palpable, tender, enlarged gallbladder.
(3) Septicaemia.
LAPAROTOMY. Aim to remove all biliary débris by
washing out the extra- and intra-hepatic bile ducts with
copious amounts of saline. Prepare the patient (15.5).
Perform a choledochostomy (15.5), and insert a T-tube.
In the presence of septicaemia and an enlarged gallbladder,
perform a cholecystostomy (15.3).
When acute symptoms have settled, treat any liver flukes.

291
291
15.8 Cholecystectomy (GRADE 3.3)
Removing the gallbladder is the standard method of
treating chronic gallbladder disease, but it is not an
operation for the occasional surgeon, so unless you
are experienced, it is better to treat cholecystitis
non-operatively (15.2,3). However, if symptoms and signs
get worse, and you cannot refer the patient, and have
sufficient experience, it is best to operate early on an
acutely inflamed gallbladder than later when it becomes
hopelessly stuck down.
If symptoms persist, consider the option of
cholecystostomy (15.4) before deciding on
cholecystectomy which can be difficult and the
complications can be serious. The main dangers are
bleeding and injuring the common bile or hepatic ducts.
Do not try to remove a fibrotic, contracted gallbladder.
Unfortunately, you will not be able to predict if the
operation is going to be easy or difficult. So, be prepared
to bail out: abandon the operation, or limit yourself to a
cholecystostomy after all. We describe 2 methods of
removing the gallbladder: (i) the retrograde in which you
first dissect and tie its neck, and (ii) the antegrade in which
you start at the fundus.
The commonest cause of an injured bile duct or hepatic
artery is an ‘easy’ operation done quickly. Another cause
is anatomical variability (15-3).
ELECTIVE CHOLECYSTECTOMY
INDICATIONS.
(1) Gallstones causing several attacks of cholecystitis.
(2) A carrier of salmonella typhi.
CONTRAINDICATIONS
N.B. These are relative, but important:
(1) Inexperience.
(2) Uncertain diagnosis and failure to exclude other causes
of dyspepsia.
(3);Insufficient symptoms and signs which justify the
operation.
(4);Complicating factors, e.g. HIV disease or excessive
obesity.
(5);The need to bail out, or perform a cholecystostomy,
if it is too dangerous to proceed.
ANTIBIOTICS. The main cause of death in gallbladder
surgery is postoperative sepsis. Use a perioperative
antibiotic (2.9) unless the case is a completely elective
one.
PREPARATION.
A self-retaining and a Deaver's retractor are almost
essential. You will need two assistants as well as the scrub
nurse. If you have facilities for radiography in theatre,
make sure the patient lies on a suitable table so that
radiographs can be taken of the upper abdomen.
Check for sickle cell disease if this is common in your
area.
INCISION. Make a right subcostal (Kocher’s) or midline
incision (11-1) extending up to the costal margin.
The Kocher’s incision gives better access to the
gallbladder itself, but the midline incision better access to
the bile duct, and any other pathology that may be present.
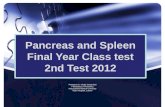
Fig. 15-3 ANATOMY OF THE BILIARY SYSTEM.
A, normal relationships of structures in this region. B-F, relations of
the right hepatic artery. In B, (and A) it runs posterior to the
common hepatic duct (64%). In C, it runs anterior (24%), and in D,
it arises from the superior mesenteric artery (9%). In E, it runs
anterior to the portal vein (91%) and in F, posterior (9%).
G-L, variations in the bile passages (>50%). Note the accessory
hepatic ducts in positions of surgical danger. M, a small pouch
(Hartmann's pouch) may project from the right wall of the neck of a
diseased gallbladder downwards and backwards towards the
duodenum. When it is well marked the cystic duct arises from its
upper left wall and not from what appears to be the apex of the
gallbladder.
(1) fundus of the gallbladder. (2) neck of the gallbladder. (3) cystic
duct. (4) common bile duct. (5) common hepatic duct. (6) right
hepatic duct. (7) left hepatic duct. (8) portal vein. (9) right branch of
the portal vein. (10) left branch of the portal vein. (11)porta hepatis.
(12) aorta. (13) some fibres of the diaphragm. (14) coeliac artery.
(15) left gastric artery. (16) splenic artery. (17) right gastric artery.
(18) gastroduodenal artery. (19) hepatic artery. (20) right hepatic
artery. (21) left hepatic artery. (22) Hartmann's pouch. (23) cystic
artery. (24) epiploic foramen (entrance to the lesser sac).
After Basmajian JV, Grant's Method of Anatomy, Williams & Wilkins 9th
ed 1975 with kind permission.

292
292
Feel for the gallbladder. Feel for stones in the gallbladder
and in the bile ducts. Feel both lobes of the liver to be sure
they are smooth and normal. Examine the stomach and
duodenum. Feel the pancreas.
If the gallbladder seems far up under the rib cage,
run your hand over the right lobe of the liver, divide the
falciform ligament across the dome of the liver, and draw
it down. Put some large packs between the diaphragm and
the liver - do not forget to remove them afterwards!
Insert a self-retaining retractor, and try to see the
gallbladder. Get the anaesthetist to empty the stomach with
a nasogastric tube. Use long tissue forceps to place large
moist abdominal packs over the hepatic flexure of the
colon, the duodenum, and the stomach. Ask your first
assistant to draw these downwards and medially.
You should now be able to see under the liver clearly.
Protect the liver with a pack, and ask your second assistant
to retract it upwards and laterally with a large Deaver's
retractor (15-4B). Look at the gallbladder. Divide any
omental adhesions to the gallbladder, if present.
If the gallbladder is acutely inflamed, perform a
cholecystostomy (15-1).
If it is very small, shrunken, thick-walled, contains
stones, and is firmly stuck to nearby structures, leave it
alone, or take out the stones and perform a
cholecystostomy. Removing such a gallbladder will be
very difficult.
If it looks and feels reasonably normal, apart from a few
stones, and is attached by fine adhesions only, it should be
safe to proceed.
A. THE RETROGRADE (‘DUCT FIRST’) APPROACH.
Use this if you can readily find the cystic duct, the
common bile duct, and the hepatic artery, in the free edge
of the lesser omentum. The epiploic foramen (of Winslow)
lies behind it; you should be able to pass one or two
fingers through it into the lesser sac.
Place a gallbladder clamp, or sponge-holding forceps on
Hartmann's pouch (15-4C). This is a widened area in the
lower part of the patient's gallbladder, just before it tapers
off into the cystic duct. Pull gently upwards on these
forceps, so as to stretch the tissues and make dissection
easier.
Incise Calot’s triangle of peritoneum between Hartmann's
pouch and the common hepatic duct. This will appear
when you apply traction to the sponge-holding forceps on
Hartmann's pouch. It is a most important step. Start by
making a small nick in the peritoneum with a long pair of
Metzenbaum scissors. Carefully insert the tips of the
scissors, then, using 'the push and spread technique' (4-9),
or a Lahey dissecting swab, open up enough of the
patient's peritoneum to expose the deeper structures.
CAUTION! Be careful not to cut any small blood
vessels. Bleeding will make the operation difficult.
By spreading the blades of the scissors (but not too far!)
before you cut, or using a Lahey dissecting swab, you
should be able to separate peritoneum only.
Take a Lahey swab (15-4C,E), and gently push apart the
peritoneum, so that you see the junction of the common
bile duct, hepatic and cystic arteries. This is most
important. Do not proceed unless you are certain of the
anatomy!
CAUTION! There are some important anatomical
variations:
(1) The common bile duct and the cystic duct may join
high or low (15-3G-L). The cystic duct may be very short
and the common bile duct is then dangerously tented by
traction on the gallbladder.
(2) The right hepatic artery may pass behind the common
hepatic duct (15-3A, B, more common) or in front of it
(15-3C, less common).
(3) The cystic artery may be closely bound to the common
hepatic duct.
(4) The cystic artery usually (64%) arises from the right
hepatic artery. It may cross behind (usually) or in front of
(unusually) the common hepatic and cystic ducts to reach
the gallbladder. Sometimes, it arises from the common
hepatic (27%) or the left hepatic artery (5%), or from other
arteries in the region (rare).
Be sure of your landmarks before you start to divide
anything. Use a Lahey swab and dissect by the 'push and
spread' method and thereby find the junction of the
patient's cystic and common bile ducts, as described
above. Be sure to identify 2cm of the common duct, both
proximal and distal to the junction. This will give you an
idea of its course and direction. The common bile duct lies
to the right of the structures going to the porta hepatis, and
is a greenish colour: identifying it is one of the keys to safe
gallbladder surgery.
If the cystic artery runs posterior to the common
hepatic and cystic ducts (usual), take extra care. Using
traction with your left hand on the gallbladder, follow the
cystic artery onto the gallbladder. Do not expect to feel any
pulsation in such a small vessel. If a strand of tissue runs
to the gallbladder, assume it is the cystic artery, pass
2 mounted ties around it, and divide between them. Expect
to find other branches and deal with them in the same way.
If the cystic artery runs anterior to the common
hepatic and cystic ducts (unusual), define it by blunt
dissection, and make sure that it is indeed going to the
gallbladder.
CAUTION! Do not tie the right hepatic artery by
mistake.
If you are sure you have found the cystic artery,
tie it doubly proximally and then close to the gallbladder
with 2/0 silk (15-4D), and divide it leaving a short cuff of
tissue, distal to the tie.
If you have found the junction of the cystic and
common bile ducts, and you are sure that what you
presume is the cystic duct is going to the gallbladder,
and nowhere else, define it further, using blunt dissection
(15-4E). This is the time to perform an operative
cholangiogram if you can and you are still not sure.
Using a long pair of Lahey forceps, gently open up the
cleft between the cystic and common hepatic ducts.
Pass a mounted tie of '0' absorbable suture through this
cleft, and around the cystic duct, but not too close to the
junction to cause a kink there. Tie it and for safety’s sake,
tie a 2nd suture around the cystic duct (15-4F).

293
293
Place another Lahey clamp on the cystic duct, close to
the gallbladder, above the ties. Cut the cystic duct just
flush with the Lahey clamp, leaving enough tied cystic
duct behind, so your ligature will not slip off.
If the cystic duct is very large, transfix it (15-4G).
CAUTION! Only divide and tie structures that are
passing to the gallbladder. Don’t leave too long a
stump of cystic duct behind as it may it form a stone.
You should now be able to strip the gallbladder from
its bed by pulling it gently upwards on the clamps.
Cut any peritoneal bands that join it to the liver
(15-4H), but tie off anything else: there may be a
vessel or an anomalous bile duct inside a strand.
If the bed of the gallbladder oozes, press a warm
pack into it. If small veins continue to bleed, cauterize
them. It is unnecessary and dangerous to close the
peritoneum over the bed of the gallbladder.
CAUTION! Check to make sure that the stump of the
cystic duct is secure and that no bile is leaking.
B. THE ANTEGRADE (‘FUNDUS FIRST’)
APPROACH. Use this if you cannot readily find the
cystic duct, common bile duct, and hepatic artery.
Place a gallbladder clamp or sponge-holding forceps
on the fundus of the gallbladder, and divide the
peritoneum between the fundus and the liver. You may
need to tie any larger vessels that bleed. Mobilize the
gallbladder in this way anteriorly and posteriorly,
continuing till you reach the neck of the gallbladder.
Locate the cystic duct and trace it to the junction with
the common bile duct. Then continue as above.
OPERATIVE CHOLANGIOGRAPHY (38.1)
is important if there has been a history of jaundice,
if ultrasound shows dilated extra-hepatic bile ducts
with or without showing a stone, and if a stone is
palpable in the common bile duct.
CLOSING THE WOUND. Place a soft rubber drain
through a stab wound down to the porta hepatis if
tissues are inflamed or you are not certain that the
cystic duct ligature will hold: a controlled bile leak is
better than an uncontrolled one! Close the abdominal
wound (11.8); do this in layers if you have used a
Kocher incision.
Fig.15-4 REMOVING THE GALLBLADDER.
A, incisions. B, expose the gallbladder. C, expose the cystic duct.
Note that the second forceps holds a Lahey swab. D, tie the cystic
artery. E, free the cystic duct. F, tie the cystic duct. G, if the
cystic duct is very large and thickened, transfix and tie it like
this. H, separate the gallbladder from the liver. N.B. if the liver
bed bleeds, pack it.
After Rob C, Smith R. Operative Surgery, Butterworth 2nded 1969,
Vol4, p.404, with kind permission.
294
294
DIFFICULTIES REMOVING THE GALLBLADDER
If you find an adherent inflammatory mass around the
gallbladder, withdraw and close the wound.
Consider operating later, when the inflammation has
subsided. Rarely this is a malignant mass, which is forever
inoperable.
If you palpate stones in the common bile duct, or find
them on an operative cholangiogram, perform a
choledochostomy (15-2) and try to extract them with
Desjardin’s forceps, or perform a transduodenal Oddi
sphincterotomy (15.5). Perform a post-extraction operative
cholangiogram, if you can.
If the cystic artery bleeds from the depths of the
wound, this can be alarming. Do not clamp blindly.
(1);Insert warm moist packs, apply pressure and wait
5mins by the clock. The spurting vessel will then be easier
to find and control. Or,
(2);Put your index finger into the epiploic foramen
and squeeze the structures (portal vein, bile ducts, and
hepatic artery) in the free edge of the lesser omentum
between your index finger and your thumb (the Pringle
manoeuvre). This will control bleeding from the stump of
the cystic artery. When you have suction and instruments
ready, remove the packs and try to visualize the vessel,
and clamp it. Transfix it carefully with 3/0 silk. Do not use
diathermy in the depths of the wound especially if you
can’t see properly! If exposure is poor, enlarge your
incision.
If you suspect you have injured the cystic duct early on,
make sure your suction is working properly and aspirate
bile so you have a good view. If necessary, enlarge your
incision. Get a cholangiogram if you cannot interpret the
anatomy. If the cystic duct is incompletely divided, hold
the part near the gallbladder in a Lahey clamp, and pass a
mounted tie around it at the common bile duct end and
complete the division of the cystic duct. If you injure it
very near its union with the common bile duct, transfix it
and carefully tie it, dividing it distally. Make sure you
haven’t kinked or narrowed the common bile duct.
If you find that you have damaged the common bile
duct you will have done so in one of three ways:
(1) By a ligature or by a clamp; undo the ligature or take
off the clamp and inspect the damage. Perform a
choledochostomy (15-2) higher up, and pass a T-tube limb
inside through the damaged area.
(2) By partly dividing it; leave a T-tube threaded up and
down the duct and proceed as for choledochostomy.
Try to repair the hole in the bile duct using interrupted 4/0
absorbable sutures, taking care not to narrow it. Keep the
T-tube in for 6wks, and then get a T-tube cholangiogram
and remove it if there is free flow into the duodenum.
(3) By completely dividing it; then try to drain the bile by
passing a tube into the severed proximal end of the bile
duct and secure it. You can leave this to drain externally
into a bag. Or you can try to insert a T-tube into both ends
of the severed duct, tie it so it doesn’t slip out and manage
the T-tube as before.
If you cannot find the distal end of the bile duct,
however, insert the distal limb of the T-tube directly into
the duodenum and secure it with a purse-string absorbable
suture. (To make a permanent by-pass, the definitive
operation of choledochojejunostomy-en-Y using a Roux
loop, is a very demanding procedure.)
N.B. Learn from your mistakes, seek to be able to
forgive yourself, and carry on.
DIFFICULTIES AFTER CHOLECYSTECTOMY
if fresh blood discharges from the drain, the pulse rises,
the blood pressure falls, and there are signs of a
haemoperitoneum, the cystic artery is probably bleeding.
Reopen the abdomen, extend the incision, suck out all the
blood and insert packs to control the haemorrhage.
Then try to visualize the bleeding vessel, clamp it and tie it
off.
If bile comes from the drain, with fever, severe pain
and a leucocytosis, suspect that infected bile and exudate
are pooling under the liver. Treat with gentamicin or a
cephalosporin. Perform an ultrasound if you can to locate
and quantify the amount of liquid. If there is no
improvement, reopen the abdomen, extend the incision,
suck out all the bile and inspect the cystic duct stump.
If this is obviously leaking and you can hold it in a clamp,
transfix it. Usually the whole area is grossly inflamed
and you will not be able to identify structures easily;
make sure the area is adequately drained.
If the patient becomes jaundiced, suspect the bile duct
has been damaged or a stone has lodged in the distal bile
duct. Try to confirm this by finding a dilated proximal
biliary tree on ultrasound (38.2B). Unless you have access
to sophisticated endoscopy, arrange a re-exploration which
is difficult, and may mean a choledocho-jejunostomy-en-
Y. If you cannot manage this, you can try to drain the
proximal biliary system percutaneously through the liver
under ultrasound guidance, or insert a T-tube (15.5) in the
dilated part of the duct. Distal stones may pass on their
own; a specialized endoscopist may be able to remove
them from below.
15.9 Obstructive (cholestatic) jaundice
When jaundice is due to an obstruction in the flow of bile:
(1) The stools are pale.
(2);The urine is dark, and contains little or no
urobilinogen.
(3);The skin itches because of deposition of bile salts.
These features are most marked in complete obstruction,
as when carcinoma blocks the common duct. Pain and
fever are usually absent. Stones typically cause an
intermittent obstruction, and a less characteristic picture.
If a stone impacts in Hartmann's pouch (15.4, 15-3M) or in
the cystic duct, it causes pain but does not impede the flow
of bile down the common duct, so jaundice is absent.

295
295
If an older patient has a steadily deepening and usually
painless obstructive jaundice, and the gallbladder is
palpably enlarged, some tumour is probably obstructing
the common bile duct.
It is unlikely that there are gallstones (Courvoisier’s rule).
This is probably incurable, but a cholecystojejunostomy to
decompress the gallbladder, by diverting the bile into the
jejunum, may make the patient’s last days more bearable.
There are several causes, however, of obstructive jaundice:
(1) A secondary tumour in the porta hepatis, usually from
a primary in the stomach or gallbladder itself.
(2) Carcinoma of the head of the pancreas.
(3) Cholangiocarcinoma or other cholangiopathies (15.7).
(4) Metastatic liver carcinoma.
(5) Hepatoma (although this is a common disease,
presentation as obstructive jaundice is unusual).
(6) Drugs, e.g. antibiotics, contraceptives, chlorpromazine,
cimetidine, oestradiol, imipramine and many others.
In endemic areas other causes are liver flukes (15.7)
or hydatid disease (15.12).
In neonates, look for a congenital abnormality (33.9)
DIFFERENTIAL DIAGNOSIS. First try to decide what
kind of jaundice the patient has.
Haemolytic jaundice. The stools are dark. There is no
bilirubin in the urine, but the urinary urobilinogen is
increased. The blood shows increased levels of
unconjugated prehepatic bilirubin (leading to high
readings on the indirect van den Bergh test). The serum
transaminases (GPT & GOT) are normal, and so is the
alkaline phosphatase. There is a reticulocytosis. Look for
evidence of a haemoglobinopathy, especially sickle cell
disease, and malaria.
Check for consumption of medicines, especially dapsone
or sulphonamides. Check for a splenomegaly and insect or
snake bites.
N.B. Haemolysis may result in pigmented gallstones!
Obstructive jaundice. The stools are pale (clay-coloured
if obstruction is complete), and show no improvement in
colour in 10days. There is bilirubin in the urine, but little
or no urobilinogen. There is a high conjugated
(posthepatic) bilirubin level (giving high readings on the
direct van den Bergh test). The alkaline phosphatase is
very high. The transaminases are usually normal.
Hepatocellular jaundice. This is commonly viral hepatitis
with an obstructive phase lasting 7-10days, but sometimes
much longer. At this stage the stools are pale.
The urine contains bilirubin but little urobilinogen.
The serum bilirubin is moderately increased (mostly
conjugated). The alkaline phosphatase is usually only
moderately increased, but if cholestasis is a prominent
feature it can rise to levels seen in obstructive jaundice.
The transaminases are increased. As the oedema of the
cells settles, the stools become normal or even dark,
the serum bilirubin falls, the urinary urobilinogen rises or
reappears, and the transaminases fall gradually. The return
of stool colour is the most important sign. This form of
jaundice is not common >35yrs.
CAUTION! You may have difficulty distinguishing the
obstructive phase of hepatocellular jaundice from surgical
obstructive jaundice. Do all you can to make the
distinction.
A laparotomy for a stone may be life saving, but GA
(especially with halothane) and the trauma of surgery may
cause hepatocellular jaundice to deteriorate, perhaps
fatally.
ULTRASOUND (38.2B) is very useful. You need to show
extrahepatic bile duct dilation >7mm to make an operable
diagnosis.
Suggesting malignancy:
(1).Relentlessly progressive steadily deepening obstructive
jaundice, weight loss.
(2).A palpable gallbladder which you can feel as an
elongated, smooth, non-tender mass, normal in contour,
and slightly mobile, which may extend to the umbilicus or
even below it. If you can feel a distended gallbladder,
it strongly suggests a malignant obstruction at the lower
end of the common bile duct, but its absence does not
exclude this. Aspiration of green bile implies free drainage
from the common hepatic duct, but aspiration of ‘white
bile’ (i.e. mucus) suggests occlusion of the cystic duct.
Suggesting metastases in the liver or a hepatoma:
a large, hard, knobbly liver. A bruit is often present with a
hepatoma, ascites is common, and is often bloodstained.
Suggesting a carcinoma of the stomach with metastases
in the porta hepatis: pain, anorexia, vomiting, an upper
abdominal mass, and the visible peristalsis of pyloric
stenosis. Anaemia is common.
Suggesting carcinoma of the head of the pancreas:
vague epigastric pain, a palpable gallbladder and weight
loss.
Suggesting gallstones: a long history of intermittent
varying jaundice, severe intermittent colicky pain, fever,
chills, and rigors (suggesting cholangitis), little or no
weight loss, flatulent dyspepsia. A leucocytosis suggests
cholecystitis.
Suggesting tuberculosis: caseating nodes in the porta
hepatis, with signs of glandular tuberculosis elsewhere.
Suggesting stenosis of the bile ducts, either malignant
or benign: a tender, enlarged liver. A chronic history of
repeated attacks of cholangitis. The gallbladder may or
may not be palpable. Common where liver flukes are
endemic.
Suggesting carcinoma of the gallbladder: an enlarged
liver and a hard, irregular mass in the right
hypochondrium, usually in a female.
MANAGEMENT. If there are gallstones, the patient needs
a choledochostomy (15-2) unless you can remove the
gallstones endoscopically. If there is malignant disease
with obstruction at the lower end of the common bile duct,
a cholecysto-jejunostomy may help unless you can refer
the patient for endoscopic stenting.
296
296
CHOLECYSTO-JEJUNOSTOMY FOR OBSTRUCTIVE
JAUNDICE (GRADE 3.3)
INDICATIONS. In practice the presence of a smooth
enlarged gallbladder is the only clear indication to operate.
However, you may still achieve a good result in some
cases where the gallbladder is not distended.
CONTRAINDICATIONS. Cachexia, debility, a hard
irregular gallbladder mass, a hard craggy liver due to
metastatic deposits, hepatoma, a large gastric tumour,
ascites.
PREPARATION. Confirm suitability for operation by
aspirating green bile from the gallbladder (if necessary
under ultrasound control). Treat with vitamin K 10mg IM
od at least 48hrs preoperatively. This will reduce a
tendency to bleed. Patients with jaundice are prone to
acute renal failure if their glomerular filtration rate falls.
So make sure hydration is adequate preoperatively.
Treat with dextrose IV to combat hypoglycaemia when
starved pre-operatively.
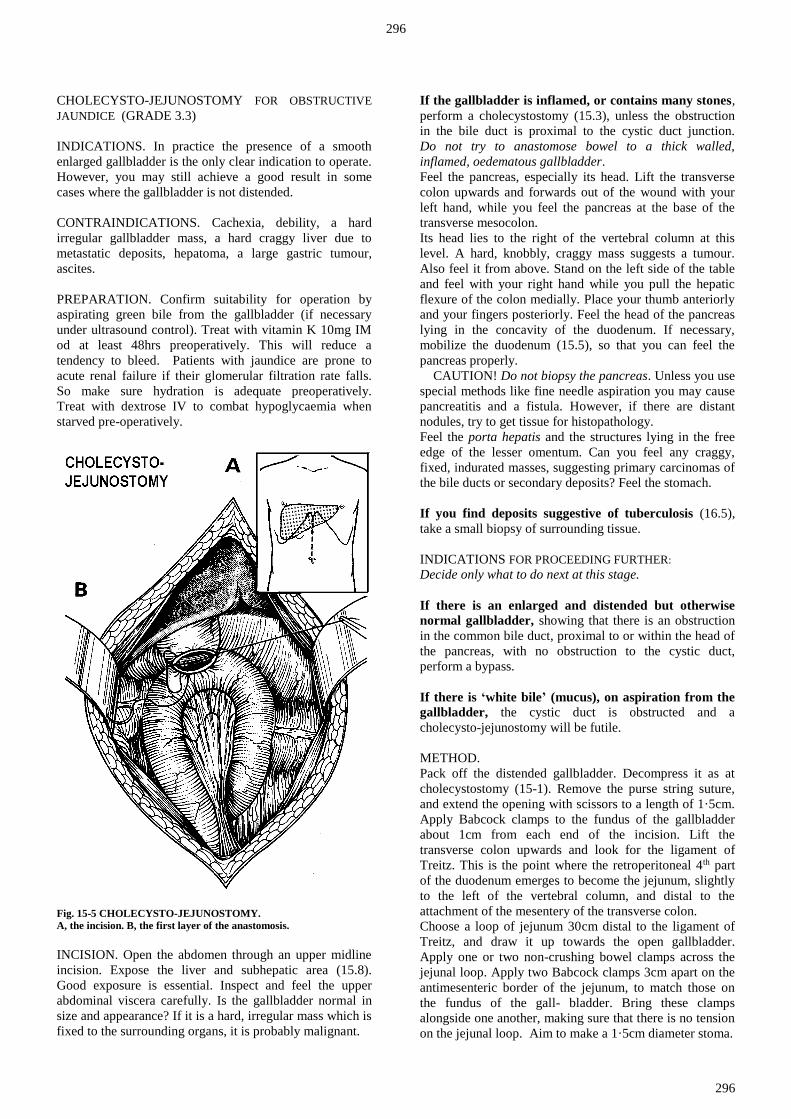
Fig. 15-5 CHOLECYSTO-JEJUNOSTOMY.
A, the incision. B, the first layer of the anastomosis.
INCISION. Open the abdomen through an upper midline
incision. Expose the liver and subhepatic area (15.8).
Good exposure is essential. Inspect and feel the upper
abdominal viscera carefully. Is the gallbladder normal in
size and appearance? If it is a hard, irregular mass which is
fixed to the surrounding organs, it is probably malignant.
If the gallbladder is inflamed, or contains many stones,
perform a cholecystostomy (15.3), unless the obstruction
in the bile duct is proximal to the cystic duct junction.
Do not try to anastomose bowel to a thick walled,
inflamed, oedematous gallbladder.
Feel the pancreas, especially its head. Lift the transverse
colon upwards and forwards out of the wound with your
left hand, while you feel the pancreas at the base of the
transverse mesocolon.
Its head lies to the right of the vertebral column at this
level. A hard, knobbly, craggy mass suggests a tumour.
Also feel it from above. Stand on the left side of the table
and feel with your right hand while you pull the hepatic
flexure of the colon medially. Place your thumb anteriorly
and your fingers posteriorly. Feel the head of the pancreas
lying in the concavity of the duodenum. If necessary,
mobilize the duodenum (15.5), so that you can feel the
pancreas properly.
CAUTION! Do not biopsy the pancreas. Unless you use
special methods like fine needle aspiration you may cause
pancreatitis and a fistula. However, if there are distant
nodules, try to get tissue for histopathology.
Feel the porta hepatis and the structures lying in the free
edge of the lesser omentum. Can you feel any craggy,
fixed, indurated masses, suggesting primary carcinomas of
the bile ducts or secondary deposits? Feel the stomach.
If you find deposits suggestive of tuberculosis (16.5),
take a small biopsy of surrounding tissue.
INDICATIONS FOR PROCEEDING FURTHER:
Decide only what to do next at this stage.
If there is an enlarged and distended but otherwise
normal gallbladder, showing that there is an obstruction
in the common bile duct, proximal to or within the head of
the pancreas, with no obstruction to the cystic duct,
perform a bypass.
If there is ‘white bile’ (mucus), on aspiration from the
gallbladder, the cystic duct is obstructed and a
cholecysto-jejunostomy will be futile.
METHOD.
Pack off the distended gallbladder. Decompress it as at
cholecystostomy (15-1). Remove the purse string suture,
and extend the opening with scissors to a length of 1·5cm.
Apply Babcock clamps to the fundus of the gallbladder
about 1cm from each end of the incision. Lift the
transverse colon upwards and look for the ligament of
Treitz. This is the point where the retroperitoneal 4th part
of the duodenum emerges to become the jejunum, slightly
to the left of the vertebral column, and distal to the
attachment of the mesentery of the transverse colon.
Choose a loop of jejunum 30cm distal to the ligament of
Treitz, and draw it up towards the open gallbladder.
Apply one or two non-crushing bowel clamps across the
jejunal loop. Apply two Babcock clamps 3cm apart on the
antimesenteric border of the jejunum, to match those on
the fundus of the gall- bladder. Bring these clamps
alongside one another, making sure that there is no tension
on the jejunal loop. Aim to make a 1·5cm diameter stoma.

297
297
CAUTION! Make the anastomosis neatly and carefully:
biliary peritonitis is a serious complication of a leak.
The end-to-side anastomosis is similar to that for a
gastroenterostomy (13.7). Make the seromuscular outer
layer of sutures of 3/0 on an atraumatic needle.
Insert 5 sutures, which should ideally pick up only the
seromuscular layer of the jejunum, but which will
probably be of full thickness, in the wall of the
gallbladder.
Place them about 2mm away from the cut edge of the
incision, and on the bowel side about 2mm back from the
antimesenteric border of the jejunum. Incise the jejunum
3mm back from the suture line. Trim away redundant
mucosa with fine scissors. Apply Babcock forceps
temporarily over any bleeding points. Insert a continuous
'all coats' posterior layer of 3/0 atraumatic absorbable
sutures, starting at one end; then continue to close the
anterior layer with the same suture. Finally, continue with
the previous 3/0 to insert an anterior layer of seromuscular
Lembert sutures. Cover the anastomosis with a layer of
omentum, and suture this in place.
Be careful to close the abdominal wall soundly (11.8.)
DIFFICULTIES WITH CHOLECYSTO-JEJUNOSTOMY
If you do find gallstones, make sure that the jaundice is
not caused by stones distally in the bile duct.
If it is, perform a choledochostomy (15-2), extract the
stones, and if you are experienced, remove the gallbladder
also. If the gallstones seem an incidental finding, the
gallbladder is not inflamed and there is tumour distally,
proceed with cholecystojejunostomy as above, but try to
remove the gallstones from the gallbladder itself.
If there is gastric outlet obstruction (<10% of patients),
shown by an enlarged stomach, and tumour obstructing the
duodenum, perform a gastrojejunostomy (13.7) as well.
To avoid bile refluxing into the stomach, you can make a
third anastomosis, a jejuno-jejunostomy (part of the
traditional ‘triple by-pass’) but this adds to the morbidity.
Remember you are doing palliative surgery only.
A Roux-en-Y (15.14) cholecysto-jejunostomy is probably
a better combination with a gastro-jejunostomy.
15.10 Liver abscess
A. Amoebic liver abscess:
extra-intestinal amoebiasis
When Entamoeba histolytica spreads outside the bowel,
it usually involves the liver. Here it can cause an 'abscess'
filled with liquid necrotic liver. To start with this is yellow
or yellow-green, later it becomes a syrupy dark reddish-
yellow. The central area of necrosis is surrounded by
zones of progressively less damaged tissue and amoebae.
The term amoebic 'abscess' is a bad one, because there is
no pus.
There is an 80% chance that the abscess is in the right lobe
of the liver, where you will be able to detect it clinically,
unless it is very deep. Collections in the liver are
sometimes multiple.
Metronidazole usually treats an uncomplicated liver
'abscess' very effectively, but it occasionally (if >5cm
diameter) needs aspiration, and rarely (if >10cm) drainage.
The major risk is that it will suddenly rupture into the
abdominal cavity, or through the diaphragm into the
pleural or pericardial space, or even into the lung.
Rupture into the abdominal cavity is a dramatic
catastrophe, with collapse and peritonitis, like the
perforation of a peptic ulcer.
Although the contents of an abscess are sterile, they cause
an acute inflammatory reaction in the peritoneum,
whether this is acute or chronic.
N.B. Common mistakes are:
(1) Not to perform a sigmoidoscopy.
(2) Not to recognize amoebic ulcers when you do see them.
(3) Not to remember the existence of acute necrotizing
amoebic colitis with perforation.
(4) Not to use all the evidence you can to diagnose a liver
abscess.
CLINICAL FEATURES.
The patient is usually male (8:1 chance), <30yrs, and may
be a child. In endemic areas (e.g. Kwazulu in South
Africa; Pakistan; Mexico) amoebic 'abscesses' are not
uncommon in babies, and also occur in the elderly.
The pain in the right upper quadrant, or the lower right
chest, is constant or intermittent, not colicky, and does not
radiate. It slowly gets worse, but is seldom severe.
Deep breathing and coughing often make the pain worse.
Fever, anorexia, weakness, and loss of weight steadily
progress. There is only a 30% chance of having had
diarrhoea with blood and mucus during the previous year.
Often, there is some associated disease, such as
tuberculosis, HIV, malnutrition, or alcoholism.
The liver is tender, smooth, diffusely enlarged,
and without an obvious lump. Palpation of the liver may
cause much distress. Pressure over the lower 5 ribs in the
right anterior axillary line is painful. Examine also for
evidence of a pleural effusion.
SPECIAL TESTS. Leucocytosis & anaemia. Raised ESR.
Check for hypoglycaemia & hyponatraemia.
Look for amoebic ulcers with a sigmoidoscope.
You are unlikely to find amoebae in the stools.
Use new PCR tests which are very sensitive if you can.
CHEST RADIOGRAPHY. Look for a pleural effusion,
and elevation of the right dome of the diaphragm.
ULTRASOUND is by far the most reliable diagnostic tool.
Look for a fluid-filled cavity in the liver (38.2A). Measure
how near the abscess is to rupture: <1cm liver tissue is
dangerous! You cannot differentiate an amoebic from a
pyogenic liver abscess except by aspiration.
DIFFERENTIAL DIAGNOSIS includes:
(1) hepatoma,
(2) cholecystitis,
(3) hydatid cyst,
(4) pyogenic liver abscess,
(5) perinephric abscess.

298
298
Suggesting a hepatoma (15.11): a hard nodular mass,
liver less painful and less tender, no fever or low fever
(fever only occurs with very rapidly growing tumours),
a bruit, bloody ascites.
Suggesting cholecystitis (15.3), perhaps with spreading
suppuration: pain and tenderness is localized to the
gallbladder region, there may be a history of intolerance to
greasy foods, and presence of jaundice, more commonly in
a female.
Suggesting a hydatid cyst (15.12): the mass arises from
one or other lobe, rather than enlarging it diffusely;
it grows slowly and is largely asymptomatic; it is smooth,
tense, and cystic; tenderness is minimal, there is no fever,
and the general condition is good. All this may change
rapidly, if the cyst becomes infected.
Suggesting a pyogenic liver abscess: a short history;
severely ill with a spiking fever.
Suggesting a perinephric abscess (6.15): the swelling is
low down over the liver on the right; the distinction may
be very difficult. Aspiration may establish the site.
MEDICAL TREATMENT FOR HEPATIC AMOEBIASIS:
metronidazole 800mg tid for 5days, and then
diloxanide furoate 500mg (children: 20mg/kg) tid for
10days or chloroquine 600mg od for 5days.
ASPIRATION FOR LIVER ABSCESS (GRADE 1.4)
INDICATIONS.
(1);To confirm the diagnosis.
(2);As a method of treatment if the abscess is >5cm
diameter, or if the patient fails to improve with medication
in 48hrs, or if the abscess is in the left lobe of the liver,
as this may perforate into the pericardium.
(3);If there is on ultrasound scan <1cm liver tissue
between the abscess and the liver surface (38.2A).
(4);If there is jaundice, suggesting involvement of the
biliary system.
METHOD. Treat with metronidazole for 48hrs before
aspirating. Check the prothrombin index if there is
jaundice; and correct a clotting defect with vitamin K
10mg IM. Using LA and full aseptic precautions,
preferably under ultrasound guidance, pass a wide-bore
(>1mm) long needle on a 50ml syringe, or better, a wide
bore pigtail catheter through healthy skin, over the site of
greatest swelling, or maximum tenderness.
If you obtain >250ml, introduce a multi-holed plastic
catheter on a trocar in the same direction, attach a 3-way
tap, and aspirate until the cavity is apparently empty.
Irrigate through the tube daily. Continue until the cavity is
empty and then remove the tube.
You have only c.10% chance of finding amoebae in the
fluid. They are more often found in the wall of the cavity.
OPEN DRAINAGE FOR LIVER ABSCESSES
(GRADE 2.4)
INDICATIONS. (This is rarely necessary if you have used
metronidazole, and aspirated the abscess adequately.)
(1) A deep-seated amoebic liver abscess which you have
not been able to aspirate, and the patient is deteriorating on
medical treatment.
(2) Fluid too thick to aspirate.
(3).Very large abscesses >10cm diameter, which recur
after repeated aspiration.
(4).A large abscess in the left lobe which may perforate
into the pericardium.
(5).Abscesses causing marked elevation of the diaphragm.
(6) Secondary infection of the abscess.
(7);A suspicion of a pyogenic liver abscess or an infected
hydatid cyst.
DRAINAGE. Make a subcostal incision, pack away the
rest of the abdominal contents and insert an aspirating
needle directly into the abscess cavity, to identify it.
Push an artery forceps into it, open it and suck out the pus.
Take some scrapings from the wall of the abscess,
and examine a warm wet specimen for trophozoites.
If there is much discharge, insert a tube drain, and bring
this out through a separate incision on the abdominal wall.
The liver may recede from the abdominal wall as you
drain it, and end up as a shrunken blob, in the right upper
abdomen. Remove the drain in 6-7days, to minimize the
risk of secondary infection.
DIFFICULTIES WITH EXTRAINTESTINAL AMOEBIASIS
If there is a sudden pain like a perforated peptic ulcer,
the abscess has probably ruptured into the abdominal
cavity. Resuscitate with IV fluids and start IV
metronidazole. As soon as the general state is satisfactory,
perform a laparotomy.
Make a midline incision. Explore the liver, as best you
can, and look for the site of the rupture: a ragged area with
chocolate-coloured fluid pouring from it. Suck out as
much of this you can. Mop up what you cannot aspirate.
Irrigate all the crevices of the peritoneum with several
litres of warm saline or water. Ensure a thorough lavage,
and close the abdomen. Treat postoperatively as peritonitis
(10.1)
If there are tender ill-defined masses in the abdomen,
suspect that the abscess has leaked into the abdominal
cavity. Start intensive medical treatment, and monitor the
abdomen closely. Mark the outline of any mass, and check
its size regularly. Perform a laparotomy if it gets bigger.
If an abscess presents on the chest wall, it will ultimately
rupture through the skin, which may become infected
with amoebae, and form a chronic ulcer (14-5A).
Treat with metronidazole.
If a severe cough and dyspnoea develops, this may, or
may not, mean that there is a pleural effusion.
If the effusion is small, it will resolve as the liver abscess
improves. If it is large insert an underwater seal chest
drain.

299
299
If there is an ulcerating skin lesion round a sinus from
the liver, caecum, or anus, remember the possibility of
CUTANEOUS AMOEBIASIS. Metronidazole cures
cutaneous amoebiasis so fast, that you can use it as a
diagnostic test. In the perianal area ulcerating skin lesions
are usually non-specific. Untreated the lesions spread fast;
biopsies show up the trophozoites.
N.B. Tuberculosis, malignancy, and fungi are often
commoner.
If the patient coughs up dark reddish-yellow fluid,
the liver abscess has ruptured into a bronchus.
Although this may drain the abscess, it may also fatally
flood the bronchial tree. Get a chest radiograph and treat
with IV metronidazole, aspirate the liver abscess,
and use postural drainage for the lung (11-24).
If the liver abscess discharges into the pericardium,
it usually does so from an abscess in the left lobe.
Pericardial rupture is not uncommon in endemic areas, is
often not recognized, and is usually fatal. Watch therefore
for abscesses in the left liver lobe, and aspirate them.
Try to aspirate the pericardium (9.2).
If there is no adequate response (<5%) to metronidazole
alone, treat with chloroquine 600mg loading dose and
150mg bd for 21days, and if necessary, dehydroemetine
65mg od IM for 10days. This drug is cardiotoxic, so you
cannot use it in heart failure.
If an epileptic fit ensues, there may be cerebral
amoebiasis. If there are no focal neurological signs, treat
with diuretics and steroids, as well as second-line therapy;
if there are, suspect a brain abscess.
B. Pyogenic liver abscess
A large pyogenic liver abscess is usually much less
common than an amoebic ‘abscess’. Organisms spread
mostly from the biliary tract, or via the portal vein from
the bowel (e.g. appendix abscess or intestinal salmonella
carried with chronic Schistosoma mansoni infestation or
HIV disease) or via the hepatic artery from a remote focus
(e.g. pyomyositis). Multiple small abscesses can result
from staphylococcal septicaemia or ascending cholangitis.
Occasionally the abscess may arise from penetrating
trauma, or infection in a hydatid cyst (15.12).
The history is usually shorter than with amoebiasis.
Jaundice suggests infection from an obstructed bile duct.
Although signs of a large abscess are like those of the
amoebic variety, much more commonly there is a fever of
unknown origin. Ultrasound is the easiest way of making
the diagnosis, and aids in liver aspiration.
Until cultures are available, use broad spectrum
antibiotics: metronidazole, gentamicin, cloxacillin and
ampicillin.
Try to aspirate the abscess completely; if you fail, proceed
to open drainage (as above). Open a large abscess to
prevent rupture into the abdominal cavity!
Test for sickle cell disease and schistosomiasis, if these are
common in your area.
15.11 Hepatoma (Hepatocellular carcinoma)
Hepatoma is the one of world's common malignant
tumours, mostly because it is so common in China,
Southeast Asia, the Amazon region and Peru, Sub-Saharan
Africa, where it is even more common than secondary
tumours of the liver. In Africa, there is a 90% chance that
a liver with a hepatoma is also cirrhotic, due to the strong
association of hepatoma with hepatitis B, C & D infection,
and with the aflatoxin produced by the aspergillus fungus
growing in damp stored food. Prevalence of hepatitis B is
also high in Greenland, Alaska and Northern Canada, and
hepatitis C is a global problem.
A hepatoma often arises simultaneously as multiple
nodules in many parts of the liver. Sometimes, a huge
mass deforms one lobe. The other primary liver tumour,
cholangiocarcinoma, is a problem in Southeast Asia.
The patient is usually male (8:1), and 30-50yrs.
He complains of pain, anorexia, weight loss, or a mass;
jaundice is a late sign. The pain is usually constant, and
sharp or burning, and is in the upper abdomen, usually on
the right.
Fig. 15-6 HEPATITIS B, C AND HEPATOMA.
The geographical distribution of the hepatitis B virus, based on
incidence of HbsAg in blood samples, correlates with hepatoma
incidence. Hepatitis C has a much broader spread in the world.

300
300
It is commonly made worse by food, which causes an
inappropriate feeling of fullness after only a small meal.
Typically, the pain is made much worse by alcohol;
so much so that it may have caused abstinence.
Usually, presentation is late with a large, or even a huge,
firm, irregular, tender liver. Quite a small tumour may
cause prostration but normal activity may continue with a
large tumour. There may be cachexia, but not always.
Look for ascites and a large spleen.
Look for collateral veins running vertically over the
anterior costal margin, or parallel to the spinous processes.
Listen over the tumour for a bruit or friction rub; this may
be intermittent, so listen on several occasions.
If there is any room for doubt, do all you can to confirm
the diagnosis. Several diseases present as swellings of the
upper abdomen. Try to distinguish those you can treat,
such as liver abscesses, hydatid cysts, and tuberculosis,
from those you can only palliate.
The best and most non-invasive tool by far is an
ultrasound: do all you can to get such a machine and get
acquainted with it (38.2A). If you have any hope of
sending specimens for cytology, use this method.
Otherwise you need to biopsy the liver to get histology.
This can be dangerous, so use ultrasound guidance if you
can. If you cannot get histology, aspiration with a fine
needle may still be useful to detect pus or tuberculosis.
In children the primary liver malignancy is
hepatoblastoma. Usually the child is severely anaemic.
The liver may rupture with a minor injury. Chemotherapy
is the only option.
SPECIAL TESTS. Serum α-fetoprotein >500μg/l is
present in 70-80% of cases. Though this test is unlikely to
be available locally, it may be easier to get a laboratory to
do it rather than get histology on a potentially dangerous
liver biopsy. The bilirubin rises late, and is often not raised
on presentation. If it is >40μmol/l, life expectancy is
weeks only. The bilirubin and alkaline phosphatase levels
rise parallel with one another. The transaminases are
normal, unless there is also chronic active hepatitis.
If there is ascites, aspirate a sample of the fluid and
examine it. Blood-stained fluid supports the diagnosis of
malignancy, not necessarily of the liver. Anaemia is
seldom a marked feature.
Do not forget to test the bleeding and clotting times.
RADIOGRAPHS. Chest radiography usually shows that
the right lobe of the diaphragm is raised. Metastases rarely
show up but are present in 50% of patients post mortem.
ULTRASOUND is extremely useful and will show
solitary or multiple lesions, or fluid cavities (38.2A).
Use it to help guide a needle biopsy.
NEEDLE, liver biopsy, Menghini, 1∙6mm, normal Menghini point, with
adjustable stop. NEEDLE, liver biopsy, Vim-Silverman, adult size, 23mm x 88.5mm, with
Franklin modification.
NEEDLE BIOPSY OF THE LIVER (GRADE 1.4)
INDICATIONS.
An enlarged liver when the diagnosis is unknown.
Fig. 15-7 LIVER BIOPSY NEEDLES.
A, Menghini needle. This has a sharp stout end (a), with an
adjustable guard (b), and a Luer lock (c). B, viewed in cross section,
the assembly has an obturator outside the needle, and a blocking pin,
which slips loosely inside the needle and prevents the biopsy
fragment from falling back, and breaking up in the syringe.
To take a biopsy using a Menghini needle: (1) insert it through the
skin, (2) expel skin fragments, (3) aspirate, (4) advance the needle
into the liver, with the patient holding his breath, and gently suck up
tissue by holding the syringe steady, (5) extract the needle whilst
gently maintaining suction.
After King M. Medical Care in Developing Countries, OUP 1967.
(A) MENGHINI NEEDLE Fit the Menghini needle to a well-fitting 10ml syringe, set the guard at
about 4cm, and draw up 3ml of sterile saline. Pass the needle point
through the anaesthetized track through the intercostal space. Inject 2ml
of saline to clear the needle point of any skin fragments.
CAUTION! Now, ask the patient to hold his breath in expiration.
Start to aspirate, and while continuing to aspirate, rapidly push the needle into the liver perpendicular to the skin, then, immediately pull it out
again. Apply pressure to the site of the biopsy. Continue aspirating until you have placed the needle point under some saline in a glass dish.
Discharge the saline remaining in the syringe. The biopsy specimen will
appear. Rescue it and transfer it to formol saline. Clear the needle with the obturator.
(B) VIM-SILVERMAN NEEDLE. Fit the inner obturator into the sheath. With firm, but well-controlled
pressure, push the needle through the abdominal wall while the patient
holds his breath. You will feel the peritoneum 'give' as you go through it. Do not push the needle in too far at this stage. Ask the patient to take a
deep breath. If the needle moves with respiration, its tip is already in the
liver; if not, ask him to hold his breath again, and gently push it 3cm further in, or until it moves.

301
301
This has hollowed-out biopsy jaws, a sleeve which fits over them, and an obturator to discharge the specimen. The inner jaws grasp a core of
tissue, after which you slide the sleeve over them to trap it. Surgeons vary
in the needle they prefer. A Menghini needle is in a patient's liver for a shorter time, so it is safer. Its disadvantage is that it is less likely to
withdraw a satisfactory specimen in a cirrhotic. This is important because
cirrhosis is common in areas where hepatoma is common.
CAUTION! Do not manipulate the needle during regular breathing,
or you may tear the liver. Ask him to hold his breath, then remove the inner obturator and replace it
with the biopsy jaws. Steady the needle with your left hand, and push the
jaws with your right hand into the needle as far as they will go. Ask him to hold his breath again. Hold the biopsy jaws firmly with your
right hand, and slide the outer jaws 3cm further into the liver.
This will wedge the jaws and the tissue firmly in the outer sheath. Rotate the needle once or twice, to break off any tissue which is attached
at the tip, and then quickly withdraw it. Ask him to breathe again.
You can do everything in a few seconds. Long breathholding is unnecessary. Slide the sheath over the biopsy jaws and open them. Use a
fine needle to remove the core of tissue from the jaws into formol saline.
CONTRA-INDICATIONS.
(1);Do not do this if your histology service is dubious in
quality, or if the results are unlikely to arrive for weeks!
(2);Deep jaundice, severe anaemia, or any bleeding
tendency, as shown by petechiae, ecchymoses,
or haemorrhages.
(3);Hydatid disease, where needle biopsy may lead to fatal
anaphylaxis or dissemination.
(4);Do not attempt this if you cannot transfuse blood in an
emergency. Correct coagulation problems first!
CAUTION! Measure the bleeding time (normal
<3mins) and clotting time (normal <8mins) before taking a
biopsy and treat with vitamin K 10mg IM till the bleeding
& clotting times are normal.
ANAESTHESIA. Use LA in an adult; a child may need
ketamine.
METHOD. Before you use either needle for the first time,
try it out by doing the biopsy on a mango (for example),
and if possible practise on a cadaver.
CAUTION! To avoid tearing the liver, tell the patient to
hold his breath when you are pushing the needle in,
pushing it in further, or pulling it out. There are also times
when you will want him to breathe deeply to check the
position of the needle. Before you start, make quite sure
that he understands what is being done. If you are using
LA, get him to practise holding his breath.
This is important, because you must perform the puncture
itself while he holds his breath at the end of expiration.
Lay the patient supine near to the right side of the bed,
and place a firm pillow against the left side in the hollow
of the bed. Place his right arm behind the head, and turn
his face to the left.
Choose a point in the mid or anterior axillary line in the
8th, 9th, or 10th intercostal spaces, or over the palpable mass
that you want to biopsy. Clean the skin with iodine, and
anaesthetize the chosen site with LA solution, down to the
parietal peritoneum.
Pierce the anaesthetized area with a scalpel (or with the
special trocar).
If you have not succeeded, try again in a different place.
If you fail after several attempts, there is probably no solid
tissue that can be biopsied. If the needle goes in without
any resistance, attach a 20ml syringe to it and aspirate:
you may withdraw pus of a liver abscess (15.10), or blood
from a haemangioma, or clear fluid of a hydatid (15.12).
POSTOPERATIVELY, (both methods), keep the patient
supine for 12hrs. Monitor the pulse and blood pressure
during this time, just in case there is bleeding into the
peritoneal cavity. A hepatoma is very vascular, and
occasionally bleeds when you biopsy it.
DIFFERENTIAL DIAGNOSIS. Try to exclude treatable
diseases. Some of these are inflammatory, and so produce
fever, but this also occurs in primary hepatoma (8%), so it
is not a reliable guide.
Fig. 15-8 LIVER SEGMENTS.
Each side of the liver is divided into 2 sectors: paramedian and
lateral. N.B. The falciform ligament dividing the liver into traditional
right and left lobes, does NOT equate with the right and left vascular
divisions. Each of the 4 sectors on each side are further divided
superiorly & inferiorly, hence forming 8 segments. However the left
paramedian sector is not formally divided, though known often as
segments 4A and 4B (or 9). The caudal lobe is its own segment (1).
Thus a right hepatectomy consists of removing segments (5,6,7,8) and
a left hepatectomy segments (2,3,4) whilst a left hepatic lobectomy
removes only segments (2+3).
Suggesting secondary carcinoma of the liver: a hard
nodular liver, evidence for a primary tumour. In carcinoma
of the stomach there may be a separate mass, dyspeptic
symptoms, or symptoms of pyloric obstruction.
Suggesting cholangiocarcinoma: deep jaundice, no bruit,
and a liver which is less big and irregular than with
hepatoma.
Suggesting carcinoma of the head of the pancreas:
deepening jaundice, little or no pain, the absence of bile
pigment in the stools, a gallbladder which is usually
palpable, no bruit.
Suggesting amoebic abscess: fever, a smooth, diffusely
enlarged, tender liver with no obvious lumps, no jaundice;
tenderness, especially intercostal tenderness.

302
302
Suggesting gallstones: severe colicky pain, biliary
dyspepsia, little or no weight loss.
Suggesting hydatid disease, with cholangitis: contact
with dogs, a tense, almost painless, long-standing (years),
smooth, rubbery mass, commonly in the right upper
quadrant; little weight loss, general condition good.
Suggesting a subphrenic abscess with downward
displacement of the liver: fever and an acute or subacute
illness, cough and chest signs on the right side, shoulder
tip pain on the right side.
Suggesting tuberculosis of the liver: a hard irregular
liver, often with no fever, no jaundice, pain is not marked,
especially in an immunocompromised patient. When there
is no jaundice, you cannot distinguish hepatoma and
secondary carcinoma from tuberculosis, except by needle
biopsy, which is one reason why it is so useful.
Suggesting intrahepatic stones: fever, right upper
quadrant pain, rarely jaundice in a patient in East Asia.
PROGNOSIS. Few patients survive >6 months.
MANAGEMENT. Cytokine inhibitors may palliate
usefully, but they are enormously expensive. There is little
you or anyone else can do for him, with the rare exception
of a single tumour confined to one lobe which can be
resected in specialist centres.
Try to promote hepatitis B vaccination in your area if
hepatoma is common.
15.12 Hydatid disease
The Echinococcus granulosus tapeworms in their larval
stages cause uni- or multi-locular or multiple hydatid
cysts; in their adult forms they inhabit the gut of dogs,
wolves, coyotes and foxes. Man is infested in the same
way as sheep, horses, oxen and cattle, by ingesting ova
from canine faeces (either by hand-to-mouth transfer or
from contaminated drinking water). Hydatid disease is
widespread in Turkey, Rio Grande do Sul in Brazil, as
well as Australia, North Africa & Southern Africa;
but also in Saudi Arabia, Siberia, Northern China, Japan
and the Philippines. Turkana, in north-west Kenya had the
highest prevalence, but now <4% of the population are
infected. Programmes to control hydatid infection have
been among the most successful measures of their kind.
If hydatid disease is endemic in your area, you may find
hydatid cysts in the liver (80%), spleen (7%) or the other
parts of the abdomen (14%), or occasionally in the lungs,
brain, bones, or indeed almost anywhere. If there is a
peripheral cyst, expect that there is at least one in the liver
too.
The presentation is typically of a tense, almost painless,
long-standing (years), smooth, rubbery, mobile cyst in the
upper right quadrant, with little fever or malaise,
it is probably a hydatid cyst: it may be enormous,
and there may be more than one.
A hydatid cyst usually contains several litres of clear
highly antigenic fluid under pressure. Around it there is a
thin, tough, fibrous ectocyst. Inside this, and separated
from it often by an easy plane of cleavage, is a thick,
yellowish, slimy, gelatinous endocyst, which the parasite
forms, and which tends to split and curl up on itself when
you cut it. Scolices, which are tiny, barely visible, white
granules, and daughter cysts, like grapes or soap bubbles,
float free in the fluid of the cyst.
Echinococcus vogeli, a parasite found in Central & South
America, produces multiple cysts in the liver. Likewise,
Echinococcus multilocularis, found in Central Asia,
produces multiple cysts, but also inflammatory infiltrations
that mimic tumour, and can spread to the lungs in 30%.
Fig. 15-9 HYDATID CYST OF THE LIVER.
A-F, some of the cysts you may find. C will need a thoraco-abdominal
incision. G, a patient with a single cyst. H, abdominal distension due
to multiple hydatid daughter cysts throughout the peritoneal cavity.
After Pelissier G, Goinard P, Peguilo J. Le kyste hydatique, Masson,
Niort 1960.
A cyst in the liver may rupture into:
(1) the bile ducts and cause cholangitis,
(2) a serous cavity, where it may cause a hypersensitivity
reaction, varying from urticaria to anaphylactic shock.
The diagnosis is difficult without ultrasound, and the
disease may be so rare that you forget it as a possibility.
There is hardly ever any hurry to operate, so investigate it
as fully as you can.

303
303
Surgery is likely to be difficult, so treat it medically before
you operate or aspirate. The method of puncture,
aspiration, injection (of scolicide) and re-aspiration (PAIR)
is safer than surgery in most cases. You may be able to do
this under ultrasound control if you have had some
experience.
If you intend to remove a hydatid cyst surgically, do so
in the plane between the tissues of host and parasite: leave
the ectocyst, and do not try to remove the entire cyst intact,
unless you can do this easily, as in the ovary or spleen.
Instead:
(1);Gain access to the cyst, and pack it off, so that if any
infective hydatid fluid does escape, it will not contaminate
the peritoneal cavity; 1mL can contain thousands of
scolices.
(2) Aspirate some of the fluid, and inject a scolicide.
(3);After 10mins, aspirate as much remaining fluid as you
can.
(4) Scoop out the endocyst and the daughter cysts.
(5);Close the cavity, so that it does not leave a sinus or a
fistula.
In a child, the cyst will probably be monolocular, so that
aspirating it will not be too difficult. But in an adult,
it is likely to be multilocular, so that:
(1);the fluid will be difficult to aspirate, because the
daughter cysts block the needle, and
(2);the scolices will be difficult to sterilize, because the
scolicide cannot penetrate in to them.
The great dangers are that you will spill the fluid which
may:
(1);allow daughter cysts to establish themselves in the
peritoneal cavity, &
(2);cause anaphylactic shock. The recurrence rate is
usually at least 25%.
PREVENTION. If yours is an endemic area, do all you
can to educate the local population, especially about
washing hands; eliminating stray dogs and regularly
deworming their domestic dogs, not feeding them
uncooked offal and burning refuse from slaughtered
animals.
SPECIAL TESTS. An absolute eosinophilia is present in
30% of patients. The Casoni test gives false -ve & +ve
results in c.20% of cases, and is no longer used.
Other antibody tests, such as the ELISA test, may also
give false negatives.
RADIOGRAPHS. Take a chest film: there may also be
cysts in the lungs. A cyst in the liver may raise the right
lobe of the diaphragm. An old aborted cyst may leave a
calcified shadow.
ULTRASOUND is the best way of detecting hydatid cysts
(38.2A). A lamellated membrane, detachment of the
membrane from the cyst wall, or the presence of daughter
cysts confirms the diagnosis. You should be able to
differentiate a hydatid from a simple liver cyst by its
having a double wall.
DIAGNOSTIC ASPIRATION. Do not try to do this,
because this may make the cyst leak, and may be fatal.
Aspiration is part of treatment. Do not try to tap a hydatid
cyst merely to make it smaller.
If you are aspirating what you think is an abscess, and
you aspirate clear fluid, it is highly likely to be a hydatid
cyst. Continue aspirating to dryness, before you remove
the needle. Then inject a scolicide, wait, re-aspirate and
then quickly withdraw the needle.
DIFFERENTIAL DIAGNOSIS.
Suggesting simple liver cyst: smooth hepatomegaly,
with single cyst wall on ultrasound.
Suggesting liver abscess: fever, tender smooth
hepatomegaly, with short history of illness.
Suggesting hepatoma: irregular huge liver with ascites
and weight loss; audible bruit.
Suggesting secondary carcinoma of the liver: hard knobbly enlarged liver with weight loss.
Fig. 15-10 OPERATION FOR HYDATID CYST OF THE LIVER.
A, high midline incision. B, expose the cyst. C, isolate the cyst with
scolicide-soaked packs, and suture a tubular sheath to the pericyst.
Work within this sheath to avoid spillage. Aspirate 50% of the fluid
into a bag of scolicide. Leave the needle in place and inject 50-100ml
scolicide till it becomes tense. Tie the purse string around the
puncture site and wait for 10mins. Re-aspirate the cyst till it is
flaccid. D, then incise the pericyst and suck out the rest of the fluid.
E, remove the daughter cysts with a spoon. F, remove the endocyst
completely with sponge forceps. G, swab out the cavity with scolicide.
Partly after Rob C, Smith R. Operative surgery: Part 1: Abdomen,
Rectum and Anus, Butterworth 2nd ed 1969 p.322 with kind permission.

304
304
TREATMENT
Treat with praziquantel 15-25mg/kg bd for 7-14days,
pre-operatively. This kills the proto-scolices. Small cysts
may disappear without surgical intervention. Albendazole
in high doses (10mg/kg od for 28days) damages the
germinal membrane and so is complementary to
praziquantel. You should therefore use both! Repeat the
dose 4 times after a rest interval of 15days. It is contra-
indicated in pregnancy. Mebendazole 600mg tid for 3wks
is an alternative, but only effective in c.40%.
Use cimetidine 400mg bd in addition.
PERCUTANEOUS ASPIRATION, INJECTION &
RE-ASPIRATION (PAIR)
Treat medically first for a minimum of 3wks.
If there is a single cyst <5cm diameter, withdraw as
much fluid as you can under ultrasound guidance through
a wide bore needle, and inject, preferably through a
T-connection piece, an equivalent volume (or slightly
more) of a scolicide (preferably chlorhexidine 0·04%,
which is safer and more effective than other scolicides
such as cetrimide, 70% alcohol, 1% povidone iodine, 0·5%
silver nitrate, hydrogen peroxide or hypochlorite.)
Start slowly by injecting a small volume; if there is any
pain, abandon the procedure. If not, continue, and
re-aspirate after 1hr.
CAUTION! Do not use formalin or hypertonic saline as
scolicides.
Do not use PAIR if the cyst communicates with the biliary
tree. Remember that the liver moves with respiration and
so even then a needle will not stay immobile.
LAPAROTOMY FOR HYDATID CYSTS OF THE LIVER
(GRADE 3.4)
INDICATIONS.
Large, symptomatic, subcapsular cysts in young patients;
large especially peripheral viable cysts, prone to traumatic
rupture.
Do not attempt operation if the cyst is high on the right,
under the diaphragm, or there are multiple, deep-seated
cysts, or if there is a communication with the bile ducts
because extensive mobilization of the liver will be
necessary.
PREPARATION. Kill the hydatids and make
dissemination less likely by using praziquantel or
albendazole as above.
Treat with hydrocortisone 100mg IM 12hrs before the
operation, so as to minimize the danger of anaphylaxis
when you open the cyst and reduce the risk of laryngeal
spasm.
Have ready: An aspirator, or a large-bore syringe with a
needle and 3-way tap; a long pair of sponge forceps,
and a sterile kitchen spoon to scoop out the cyst; coloured
packs which will let you to see the brood capsules and
scolices more easily (soak the packs in scolicide);
2 suckers, one for the trocar (if you use one), and another
ready for any spills; a sterilized 6x15cm tubular polythene
sheath; & a scolicide.
INCISION.
Make a midline incision unless the cyst is very peripheral.
If necessary, extend this laterally in a J-shape, so that you
have adequate exposure. Another way of getting better
access is to stuff packs, soaked with scolicide, into the
right subphrenic space, so as to push the liver down.
If you know exactly where the cyst is, a subcostal incision
may be even better.
The cysts present as smooth white swellings. Look and
feel carefully to find how many there are. The rest of the
liver is usually large, smooth, and distended.
Select a place where the cyst is close to the surface,
and isolate it with carefully placed scolicide-soaked packs.
Suture a tubular polythene sheath 6x15cm with 3/0 silk to
the pericyst without puncturing the cyst. Aspirate through
the polythene sheath at least half the fluid with a 1∙5mm
needle (15-10C).
If the needle blocks, clear it by injecting a little scolicide.
If needle aspiration does not work, use a trocar and
cannula. If necessary, try introducing a multi-holed
catheter through the cannula. This will however increase
the risk of spillage. If many daughter cysts block the
sucker, it is probably multilocular.
Collect the fluid in a bag containing an excess of scolicide.
Do not use an open dish as fluid may spill! Keep a record
of the volume you withdraw, as a guide to how much
scolicide you will need to inject. Leave the needle in place
and inject 50-100ml scolicide back into the cyst until it
becomes tense. Then tie a purse string suture snugly round
the puncture site, and remove the needle. Wait for 10mins
for the contents of the cyst to become sterile.
Re-aspirate the cyst till it becomes flaccid and open it
through the part which presents most easily. Insert the tip
of the sucker, and suck out the remaining fluid. Record-
sized cysts have had over 40L! Using a kitchen spoon,
remove all the daughter cysts, sediment and debris
(15-10E). Then, using finger dissection, find the natural
plane of cleavage between the ecto- and the endo-cyst.
To get adequate exposure, you may have to incise the cyst
across the full width of its bulge, and deroof it.
Remove the yellow laminated membrane of the endocyst
completely, piece by piece, with sponge forceps (15-10F).
There will be little bleeding.
CAUTION!
(1);Try not to rupture the daughter cysts as you remove
them, because their contents are probably still infective.
(2) Do not try to remove the ectocyst; it is tightly stuck to
the liver, and will bleed.
Swab the inside of the cyst with packs soaked in scolicide,
and explore it for secondary cavities. If you find any,
repeat the process of aspiration and injection.
If the cavity is small, you may be able to bring its edges
together with mattress sutures.

305
305
If the cavity is large, you can:
(1).Suture any obvious small bile duct openings, and leave
it alone, which is probably the wisest method.
(2).Fill it with ordinary 0·9% saline, and suture it.
(3).Saucerize it by excising the protruding portion.
The difficulty with this is that the cut surfaces of the liver
will bleed.
(4).Fill it with a graft of omentum. Dissect a strip of
omentum on a vascular pedicle and stitch this into the
cavity. The omentum will swell to fill the space and absorb
the fluid from the cavity.
(5).Bring the walls of the cyst together with multiple
absorbable sutures, so that the cavity is obliterated.
Drain large cavities for about 10days, especially if you
have not been able to remove all the endocyst.
CAUTION!
(1);Do not let the untreated cyst fluid spill, or daughter
cysts will form in the peritoneal cavity.
(2) If the needle hole leaks, insert a purse string suture.
If the cyst is a simple non-hydatid cyst, you can simply
de-roof it and obliterate the cavity with omentum.
Make sure you control bleeding from the cut cyst edge
with a running suture or diathermy.
DIFFICULTIES WITH HYDATID CYSTS
If there are signs of peritonism with an anaphylactic
response, shock, and dyspnoea, the cyst has ruptured into
the peritoneal cavity. Use hydrocortisone 0·5-1g IV, and
adrenaline 1:1000 1ml SC.
If the blood pressure falls alarmingly and there is no
other reason for it, the cause is probably an anaphylactic
reaction. Treat as above. Alternatively the cyst may have
eroded into a major vessel such as the inferior vena cava or
portal vein: apply pressure with your fingers and get
suction, bulldog clamps etc as for a vascular injury.
If there is generalized abdominal swelling, consider the
possibility of HYDATIDOSIS OF THE PERITONEAL
CAVITY. At operation you may find the peritoneal cavity
distended with hydatid cysts, and remove bucketfuls of
them. Try to remove as many of them as you can.
Then flood it with liberal quantities of 0·04%
chlorhexidine solution as a scolicide. Aspirate this and
then irrigate it with saline to wash out the remaining
scolicide. The surface of the bowel may be seeded with
small white nodules. Make sure you start praziquantel and
albendazole unless already started.
If there is a cyst in the omentum, try to remove it entire,
with part of the omentum. If you cannot do this, aspirate
and inject scolicide, as for the liver.
If there is a cyst in the spleen, perform a splenectomy
(15.17).
If there is a cyst in the kidney, aspirate under ultrasound
guidance, and introduce scolicide as above.
If there is obstructive jaundice, perhaps with
cholangitis, aim to drain the common bile duct (15.7).
Remove all hydatid sludge, debris, and daughter
cysts from the duct, and irrigate it thoroughly.
Drain the common bile duct with a T-tube.
If a cyst is leaking into the peripheral bile ducts,
sterilize, evacuate, and drain the cyst. An external biliary
fistula may develop, which may improve cholangitis
which is likely to be present.
If a fever develops postoperatively, the cyst cavity is
probably infected. Treat with gentamicin or
chloramphenicol.
If there are features of a liver abscess: a swinging fever,
anorexia, and increasing pain, suspect that a hydatid cyst
has become infected. Open it, saucerize it, and drain it
(15.10). Infection will have destroyed the hydatids.
If there are recurrent cysts, they will probably take
about 3yrs to develop, be multiple, and be in the
abdominal cavity. Distinguish recurrent cysts from the
manifestation of an unsuspected second cyst. Start medical
treatment.
If there are cerebral cysts also, use praziquantel in
higher doses (60-90mg/kg bd for 30days), together with
dexamethasone 4mg qid)
If a cyst is calcified and asymptomatic, leave it alone.
15.13 Pancreatitis
Both acute and chronic pancreatitis are not uncommon;
rarely a pancreatic pseudocyst (15.14) or abscess (15.15)
develop as complications. If the patient does not recover
1wk after an acute episode, suspect such complications.
Pathologically, acute pancreatitis varies from oedema and
congestion of the pancreas to its complete autodigestion,
with necrosis, haemorrhage, and suppuration. Less severe
forms may go on to form a tender, ill-defined mass in the
epigastrium.
The main symptom is pain, which can vary from moderate
epigastric discomfort to an excruciating, penetrating
agony, which bores through to the back, and needs high
doses of opioids to relieve it. There is tenderness in the
epigastrium, perhaps with guarding. Vomiting, paralytic
ileus and the outpouring of fluid into the retroperitoneum
may result in severe fluid loss. If you see bruising around
the umbilicus or in the flanks, this indicates intra-
abdominal haemorrhage and means the pancreatitis is
severe.

306
306
The underlying cause is usually:
(1) alcohol abuse (especially spirits), or
(2) gallstones (or ‘sludge’), and occasionally,
(3) ascaris worms,
(4) liver flukes,
(5) leptospirosis,
(6) HIV disease (including treatment with ARV therapy),
(7) rarely typhoid.
(8) mumps or coxsackie virus,
(9) hypercalcaemia, hyperlipidaemia,
(10) systemic lupus or cystic fibrosis
(11) trauma (including endoscopic instrumentation)
(12) drugs such as sulphonamides, thiazides, œestrogens
(13) poisons such as organophosphates
(14) tityus scorpion envenomation (in Trinidad, Brazil &
Venezuela).
You may diagnose pancreatitis clinically, or from
laboratory tests, or only when (in error) you perform a
laparotomy for an acute abdomen. Estimating the serum
amylase is not difficult, and your laboratory should be able
to do it, because you should avoid a laparotomy for
pancreatitis at all costs!
Chronic relapsing or recurrent pancreatitis is one of the
causes of a severe chronic upper abdominal pain. It is quite
common in alcoholics anywhere, and there is a calcific
type found much in Kerala and Orissa in India, but also in
Japan and sub-Saharan Africa; the pancreas calcifies and
its endocrine function deteriorates. A longitudinal
pancreaticojejunostomy is helpful if the pain is
debilitating, but this is formidable surgery indeed.
Chronic pancreatitis may also be due to tuberculosis (16.5)
ACUTE PANCREATITIS
DIFFERENTIAL DIAGNOSIS includes:
(1) gastritis,
(2) perforated peptic ulcer (13.3),
(3) acute cholecystitis (15.3),
(4) rupture of a liver abscess (15.10),
(5) strangulating upper small bowel obstruction (12.2).
SPECIAL TESTS. Serum amylase rises within hours of
the start of the pain, and remains high for about 2days.
A level of >1,000 Somogyi units is almost diagnostic.
A peritoneal tap in the right lower quadrant will confirm
the diagnosis: the aspirate may be straw-coloured, or
reddish-brown, but its amylase is always high.
In severe acute disease (Ranson’s criteria),
(1) the white count is >16000/mm³
(2) the glucose is >10mM; after 48hrs,
(3) the haematocrit drops >10%,
(4) the urea rises >10mM,
(5) the serum calcium drops <2mM,
(6) the pO2 drops <60 mm Hg with a metabolic acidosis.
Hyperglycaemia is common with chronic calcific
pancreatitis.
(The Balthazar score gives the severity of the pancreatitis in terms of the degree of inflammation and necrosis seen, but this needs contrast-
enhanced CT scanning.)
RADIOGRAPHS are not very helpful but may show
pancreatic calcification, if there have been previous
attacks; and a left pleural effusion, or distended loops of
bowel from ileus.
ULTRASOUND demonstrates oedema, and fluid
collections (or even necrosis) of the pancreas (38.2C).
You may see gallstones, and especially ‘sludge’ in the
common bile duct, or a completely different diagnosis!
TREATMENT.
If pancreatitis is mild, it will settle by a régime of
restricting oral intake, with nasogastric drainage, analgesia
and IV fluid replacement.
If pancreatitis is severe, replace fluid loss energetically
with large volumes of 0∙9% saline, Ringer's lactate, or a
plasma expander. Correct electrolyte losses. Monitor the
urinary output, the haematocrit, and if possible, the central
venous pressure. Monitor glucose; start an insulin sliding
scale. The pain may be overwhelming: treat with large
doses of opioids, supplemented by diazepam or
promethazine. Administer oxygen by mask; consider
mechanical ventilation. Prophylactic antibiotics, especially
against staph aureus are advisable. You may need blood
transfusion later.
If you are sure of the diagnosis, do not operate; but it is
better to operate unnecessarily, than not to operate on a
case of strangulated bowel, for example. The amylase
level may rise with necrotic bowel. Severe cases may
benefit from lavage with saline, via tubes which can be
inserted in the flanks under LA (13.3), but attacks tend to
recur. Formal open lavage is then better.
If you do open the peritoneum, you will know that there
is pancreatitis when you see areas of whitish-red fat
necrosis on the transverse mesocolon, or omentum, and the
exudate described above. The pancreas feels swollen and
oedematous, and may contain greenish-grey necrotic areas.
The fat necrosis may be confused with TB, so take a
biopsy. Drains by themselves do not help, but you may use
them for continuous peritoneal lavage.
If the abdomen is difficult to close, leave it open as a
laparostomy putting on a vacuum dressing (11.10, 11-20)
or make fasciotomies in the rectus sheath.
DIFFICULTIES WITH ACUTE PANCREATITIS
If you find that there are also gallstones, consider doing
a cholecystectomy (15-4) later. Do not be tempted to
remove the gallbladder in the acute phase.
If, during the course of 2-3wks, septicaemia develops,
suspect that a pancreatic abscess (15.15) is developing,
especially if there is haematemesis.
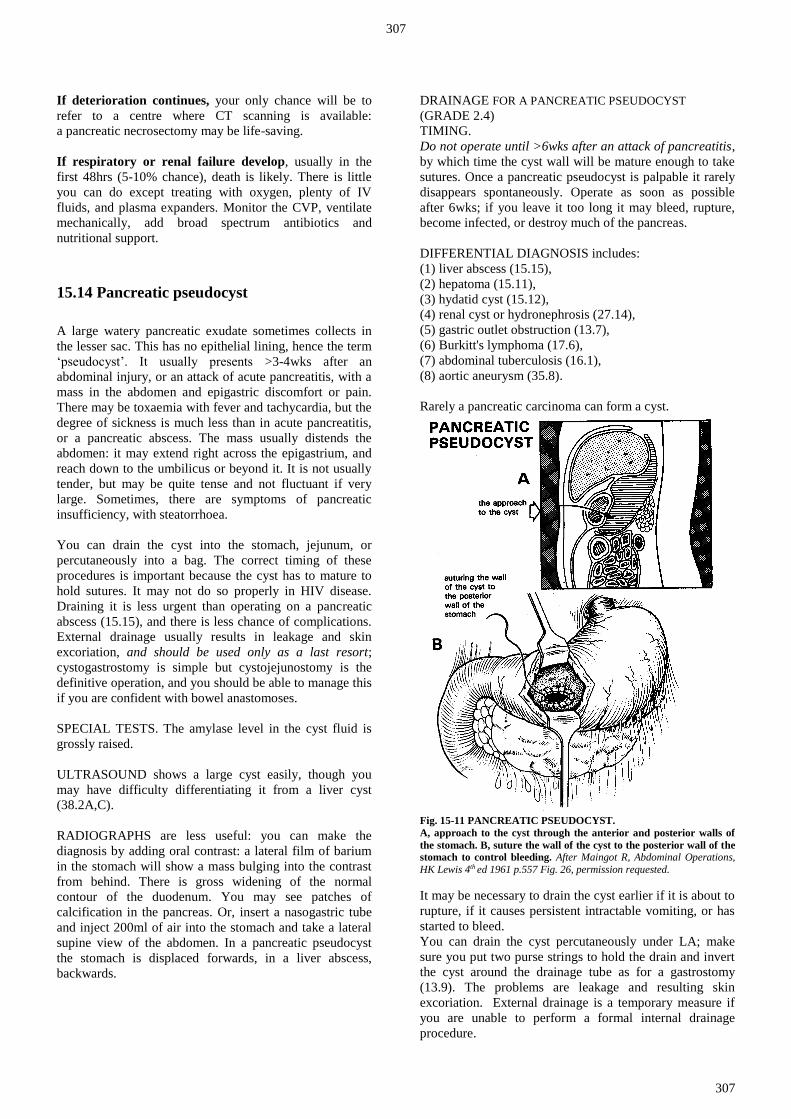
307
307
If deterioration continues, your only chance will be to
refer to a centre where CT scanning is available:
a pancreatic necrosectomy may be life-saving.
If respiratory or renal failure develop, usually in the
first 48hrs (5-10% chance), death is likely. There is little
you can do except treating with oxygen, plenty of IV
fluids, and plasma expanders. Monitor the CVP, ventilate
mechanically, add broad spectrum antibiotics and
nutritional support.
15.14 Pancreatic pseudocyst
A large watery pancreatic exudate sometimes collects in
the lesser sac. This has no epithelial lining, hence the term
‘pseudocyst’. It usually presents >3-4wks after an
abdominal injury, or an attack of acute pancreatitis, with a
mass in the abdomen and epigastric discomfort or pain.
There may be toxaemia with fever and tachycardia, but the
degree of sickness is much less than in acute pancreatitis,
or a pancreatic abscess. The mass usually distends the
abdomen: it may extend right across the epigastrium, and
reach down to the umbilicus or beyond it. It is not usually
tender, but may be quite tense and not fluctuant if very
large. Sometimes, there are symptoms of pancreatic
insufficiency, with steatorrhoea.
You can drain the cyst into the stomach, jejunum, or
percutaneously into a bag. The correct timing of these
procedures is important because the cyst has to mature to
hold sutures. It may not do so properly in HIV disease.
Draining it is less urgent than operating on a pancreatic
abscess (15.15), and there is less chance of complications.
External drainage usually results in leakage and skin
excoriation, and should be used only as a last resort;
cystogastrostomy is simple but cystojejunostomy is the
definitive operation, and you should be able to manage this
if you are confident with bowel anastomoses.
SPECIAL TESTS. The amylase level in the cyst fluid is
grossly raised.
ULTRASOUND shows a large cyst easily, though you
may have difficulty differentiating it from a liver cyst
(38.2A,C).
RADIOGRAPHS are less useful: you can make the
diagnosis by adding oral contrast: a lateral film of barium
in the stomach will show a mass bulging into the contrast
from behind. There is gross widening of the normal
contour of the duodenum. You may see patches of
calcification in the pancreas. Or, insert a nasogastric tube
and inject 200ml of air into the stomach and take a lateral
supine view of the abdomen. In a pancreatic pseudocyst
the stomach is displaced forwards, in a liver abscess,
backwards.
DRAINAGE FOR A PANCREATIC PSEUDOCYST
(GRADE 2.4)
TIMING.
Do not operate until >6wks after an attack of pancreatitis,
by which time the cyst wall will be mature enough to take
sutures. Once a pancreatic pseudocyst is palpable it rarely
disappears spontaneously. Operate as soon as possible
after 6wks; if you leave it too long it may bleed, rupture,
become infected, or destroy much of the pancreas.
DIFFERENTIAL DIAGNOSIS includes:
(1) liver abscess (15.15),
(2) hepatoma (15.11),
(3) hydatid cyst (15.12),
(4) renal cyst or hydronephrosis (27.14),
(5) gastric outlet obstruction (13.7),
(6) Burkitt's lymphoma (17.6),
(7) abdominal tuberculosis (16.1),
(8) aortic aneurysm (35.8).
Rarely a pancreatic carcinoma can form a cyst.
Fig. 15-11 PANCREATIC PSEUDOCYST.
A, approach to the cyst through the anterior and posterior walls of
the stomach. B, suture the wall of the cyst to the posterior wall of the
stomach to control bleeding. After Maingot R, Abdominal Operations,
HK Lewis 4th ed 1961 p.557 Fig. 26, permission requested.
It may be necessary to drain the cyst earlier if it is about to
rupture, if it causes persistent intractable vomiting, or has
started to bleed.
You can drain the cyst percutaneously under LA; make
sure you put two purse strings to hold the drain and invert
the cyst around the drainage tube as for a gastrostomy
(13.9). The problems are leakage and resulting skin
excoriation. External drainage is a temporary measure if
you are unable to perform a formal internal drainage
procedure.

308
308
CYSTOGASTROSTOMY FOR PANCREATIC PSEUDOCYST
(GRADE 3.2)
PREPARATION
In dehydration, anorexia, or toxaemia, administer IV fluids
and high calorie high protein enteral feeding for a few
days pre-operatively. Insert a nasogastric tube the evening
before operation, and wash out the stomach thoroughly.
INCISION.
Make a midline incision.
Choose an area on the anterior wall of the stomach that is
overlying the cyst. Use a knife or diathermy to start a 4cm
incision in the long axis of the stomach between
2 Babcock forceps. Enlarge it with scissors. Clamp any
briskly bleeding vessels, and retract the edges of the
incision, so that you can inspect the posterior wall of the
stomach. Suck it empty.
After opening the stomach, aspirate through its posterior
wall into the cyst. Expect to find a mildly opaque
straw-coloured, or murky brownish fluid. If so, insert a
small haemostat through the hole in the stomach into the
cyst, and open it so as to enlarge the opening to 3cm.
Suck out the fluid: expect to aspirate up to 4l.
CAUTION! Do not incise the cyst widely; it may bleed
severely.
N.B. If you aspirate fresh blood, the ‘cyst’ may be an
aortic aneurysm: stop! Get an ultrasound scan (38.2D).
If you have waited the 6wks for adhesions to form and the
cyst wall to mature, there will be no need to suture the
stomach wall to the cyst, as they will already be tightly
stuck together. But control brisk bleeding from the
stomach edge; so quickly oversew the opening all round
with a continuous interlocking haemostatic suture of 2/0
non-absorbable. Do not use absorbable suture, because
pancreatic juice digests it. When you are sure the posterior
opening in the stomach is no longer bleeding, close the
anterior opening in two layers, the first a full-thickness
haemostatic continuous layer of 3/0 absorbable sutures,
and the second a seromuscular Lembert layer of
continuous non-absorbable suture. Close the abdominal
wall in the usual way.
CYSTOJEJUNOSTOMY-EN-Y FOR PANCREATIC
PSEUDOCYST (GRADE 3.5)
INCISION. This is the definitive operation. Proceed as
above; after opening the cyst, lift up the proximal jejunum
and look at its blood supply; select a point 30cm from the
ligament of Treitz where to divide the bowel so that the
distal loop easily reaches the pseudocyst. Divide the bowel
between non-crushing clamps. You will need to divide
some of the vascular arcades in the mesentery to mobilize
the distal bowel (the Roux loop) adequately. When you are
satisfied there is no tension, make an end-to-side
anastomosis of the loop to the opening in the pseudocyst.
Then anastomose the proximal cut end of jejunum to the
right side of the Roux loop some 20cm along its length
with an end-to-side anastomosis, making sure the bowel
lies comfortably. Close any mesenteric defects carefully
avoiding damage to the fine mesenteric vessels.
Fig. 15-12 THE ORIGINAL ROUX LOOP.
A, the distal afferent (Roux) loop, which you can use to drain the
gallbladder, bile duct, pancreatic cyst, or stomach. B, the proximal
efferent loop. The small bowel has been divided at c, and the
proximal part anastomosed end-to-side at c'. Here the plan is to
anastomose the Roux loop to the gallbladder.
SIMPLE CYSTOJEJUNOSTOMY FOR PANCREATIC
PSEUDOCYST (GRADE 3.4)
INCISION. This is a simpler, but less satisfactory,
procedure. Make a midline incision. Open the lesser sac to
get access to the pancreatic pseudocyst; check that its wall
is thick enough to hold sutures. Then pack off the
abdominal contents with large swabs, open the cyst by
2cm only and drain its contents. Bring a loop of proximal
jejunum up to the cyst and make a side-to-side
anastomosis (as for a gastrojejunostomy (13-16).
POSTOPERATIVELY, restrict oral intake with
nasogastric suction for 3-4days, until flatus is passed;
then start oral fluids, followed by a soft diet.
15.15 Pancreatic abscess
This is a dangerous complication of acute pancreatitis
(15.13) or perforated duodenal ulcer. Occasionally it
results from severe pancreatic injury. A collection of pus,
necrotic tissue, and clot fills the lesser sac; it enlarges
behind the peritoneum, it expands anteriorly to obliterate
the lesser sac, and it pushes the stomach and transverse
colon forwards. It may present with a catastrophic
haematemesis.

309
309
If the abscess develops during the course of an attack of
pancreatitis, the diagnosis is usually obvious, but it may be
difficult otherwise. So if ever a severely sick patient has an
ill-defined deep-seated epigastric mass, remember that
there might perhaps be a pancreatic abscess.
SPECIAL TESTS. The urinary and serum amylase are
usually high. Check the glucose.
ULTRASOUND. A fluid-filled cavity is seen adjacent to
the pancreas, as a pancreatic pseudocyst (38.2C).
Aspiration is difficult and hazardous, so is not
recommended.
LAPAROTOMY FOR PANCREATIC ABSCESS (GRADE 3.4)
PREPARATION. Resuscitate with adequate IV saline or
Ringers lactate. Correct hyperglycaemia with insulin.
Administer oxygen, bicarbonate and calcium in seriously
ill patients. Catheterize the bladder. Treat with gentamicin,
ampicillin and metronidazole. Cross-match blood.
Decompress the stomach with a nasogastric tube.
EXPLORATION. Make an upper midline incision from
the xiphisternum to beyond the umbilicus. Open the
abdominal cavity with care, because the mass, or the
stomach or colon, may have stuck to the abdominal wall.
You may find it difficult to know what you are seeing.
Dissection is difficult and dangerous, because the tissues
are so vascular and oedematous. Lift and free the
abdominal wall from the organs under it, and insert a
self-retaining retractor. Feel for the upper border of the
abdominal mass. Try to find a place where you can incise
it without injuring anything. This will usually be through
the lesser omentum, or better, the transverse mesocolon to
the left of the ligament of Treitz. When you have decided
where to drain, seal the area from the rest of the
peritoneum with large moist packs. Using a syringe and a
large needle, aspirate the place where there seems to be the
thinnest layer of tissue between the abscess and your
finger. Take pus for culture. If you find pus under
pressure, decompress the abscess with suction. Enlarge the
abscess so that you can insert two fingers, but don't try to
dissect further. Wash out any floating solid matter.
CAUTION! Don't disturb the necrotic pancreatic tissue
at the bottom of the abscess - it will bleed!
Place 2 catheters in the abscess cavity, and bring them out
through stab wounds. Bring one out anteriorly, and the
other as far back as possible, in the most 'dependent'
position. Use these to irrigate the abscess cavity
continuously (about 2l in 24hrs). Make a feeding
jejunostomy (11.7), because oral feeding will not be
possible for 3wks, and you will probably be unable to feed
parenterally. Feeding through a jejunostomy results in less
secretion of gastric juice than feeding through a
gastrostomy.
POSTOPERATIVELY.
Continue nasogastric suction, fluids, and antibiotics until
the temperature is normal. Chart the daily drainage output.
Don't be in a hurry to remove the drains, even if leaving
them in does seem to increase the risk of a fistula.
Allowing pus to collect again is a greater risk.
If the wound is looking fairly clean, close it by secondary
suture in 7-10days.
CAUTION! This is heroic surgery! A pancreatic
abscess carries a 30-50% mortality, and often reforms,
even with adequate drainage. If so, be prepared to
re-operate 3 or 4 times if necessary. However, if you do
not operate, death is inevitable!
DIFFICULTIES WITH PANCREATIC ABSCESS
If pancreatic juice is still discharging after 2wks, leave
the catheters in situ for a month and then withdraw them
slowly 5cm per day.
If a pancreatic fistula develops, collect the juice in a stoma
bag with the orifice carefully cut to size to prevent skin
excoriation. This can be mixed with jejunostomy feeds if
malabsorption is a problem.
If bleeding becomes severe, try pinching the vessels in
the free edge of the lesser omentum between your fingers
and pack the pancreatic area. Leave the packs for 48hrs
and remove them at a second laparotomy, when bleeding
should be much less.
15.16 Pancreatic carcinoma
If the carcinoma is in the head of the pancreas (70%),
it may obstruct the common bile duct, so that presentation
is with painless progressive obstructive jaundice (15.9).
If it is in the body of the pancreas (30%), presentation is
with upper abdominal and back pain and general
symptoms of malignancy. Spread to the lymphatics and
surrounding structures is early, and 10% of patients
develop ascites.
Thrombophlebitis migrans (thrombophlebitis in any
superficial vein appearing, resolving, and then appearing
again elsewhere) may occur with any malignant tumour,
but is particularly common with this one.
Radiotherapy, chemotherapy, and surgery are of little
value, but differentiation with tuberculosis is important.
Taking a biopsy of the pancreas itself may cause
pancreatitis and worsen the condition, so try to get a piece
of tissue from an adjacent node or piece of omentum.
Sometimes carcinoma of the pancreas cannot be easily
distinguished from chronic pancreatitis (15.13)
or tuberculosis.

310
310
15.17 Surgery of the spleen
If you operate on the spleen, you often end up removing it.
The indications for doing so (apart from trauma) must be
good, because the spleen of a tropical patient is commonly
large, and may be so firmly stuck to the diaphragm that:
(1) exposing it is difficult.
(2) bleeding is likely from the vascular adhesions that join
it to the diaphragm.
If there is portal hypertension, the vena cava carries high
pressure venous blood which escapes into the systemic
circulation. Remember the spleen protects against
subsequent infection, especially pneumococcal
pneumonia, malaria and dog & cat bites with
Capnocytophaga canimorsus (a common commensal)
which may rapidly be fatal. Infection is even more
common if HIV is present.
INDICATIONS (OTHER THAN FOR TRAUMA) FOR
SPLENECTOMY
(1) Spontaneous rupture. This is rare, but may occur typically in massive malarial
(not bilharzial) splenomegaly; though it may be truly
spontaneous, e.g. in mononucleosis, the patient may not
remember any trauma because it was slight. It may occur
after colonoscopy. Signs are of shock, left upper
abdominal pain and abdominal distension, although
initially there may be felt a reduction in abdominal girth as
a large spleen bleeds.
(2) Hypersplenism. A big spleen may be responsible for removing all the
blood cell lines, resulting in anaemia, leucopenia and
thrombocytopenia of varying severity, though the
thrombocytopenia is commonest. The problem is that the
same picture can be shown by HIV disease, which itself
can give rise to splenomegaly. Thrombocytopenia is a
serious hazard in surgery and so you need to have some
experience before attempting a splenectomy without
platelets available for transfusion. However, your hand
may be forced if a patient continues to bleed elsewhere
because of the thrombocytopenia, particularly if there is
portal hypertension.
If the underlying cause is HIV disease, blood counts will
improve with ARV therapy (5.8) without splenectomy.
You should anyway be wary of removing a spleen when
there is HIV disease because of the risks of infection;
you may be able to make the distinction between
hypersplenism and HIV-pancytopenia by looking at a bone
marrow film: this is normal or hyperplastic in
hypersplenism, but hypoplastic in HIV disease.
(3) Chronic idiopathic thrombocytopenia. Here the low platelet count is not associated with an
enlarged spleen but through destruction of platelets by
antibodies. There are often ‘megathrombocytes’ in the
peripheral blood film and raised numbers of
megakaryocytes in the bone marrow.
It occurs more often in females than males (4:1);
there is usually quite a good response to prednisolone,
but eventually this option becomes undesirable in the
chronic case.
However splenectomy may not benefit 20% of cases.
Do not do it if systemic lupus erythematosus or rheumatoid
arthritis is the cause of the chronic thrombocytopenia.
Never do it for the acute thrombocytopenia, and especially
not where thrombocytopenia is due to drug sensitivity
(especially quinine). If you have access to radiotherapy
this may be the safer option.
(4) Haemolytic anaemias.
There are several haemoglobinopathies, including sickle
cell trait (never sickle cell disease) thalassaemia, and
spherocytosis for which splenectomy may be beneficial,
but their selection needs the advice of an expert.
(5) Splenic torsion or wandering spleen.
These are both very rare and arise when the spleen has an
abnormally long pedicle and no adhesive attachments.
You are unlikely to make the diagnosis before you operate.
Torsion of the spleen tends to occur during pregnancy
when it is confused with an ovarian tumour!
(6) Hydatid cyst (15.12).
(7) Malignancy. HIV-ve lymphoma, Schistosomiasis related giant follicular
lymphoma, chronic myeloid or lymphatic leukaemia,
or fibrosarcoma affecting only the spleen, but you should
get advice from an expert.
KASHY (20yrs) complained of a swelling in the right iliac fossa.
Ordinarily, it was painless but during attacks of 'fever' it became painful and tender. At laparotomy, the whole spleen was found to be in the right
iliac fossa, but the splenic vessels crossed the abdomen to their normal
position. The 'wandering spleen' was removed easily. LESSON Some rare conditions have easy solutions.
CONTRA-INDICATIONS TO SPLENECTOMY
(1) Splenic abscess (15.18) occurs occasionally. It starts
acutely, it may become chronic, and it shows up
radiologically as a fluid level in an irregular space.
Ultrasound shows the spleen to be filled with dense fluid.
The pus is sterile usually, but may be secondary to
amoebiasis, brucellosis, salmonellosis, leptospirosis or
candidiasis. There may be sickle cell disease, acute
myeloid leukaemia or pancreatitis. Carefully pack away
other abdominal viscera, and drain the abscess: do not try
to remove the spleen.
(2) Tropical splenomegaly syndrome
This is an immune response to recurrent attacks of malaria,
and is responsible for nearly all large spleens in malarious
areas. It responds to long courses of antimalarials.
Do not remove such spleens unless hypersplenism is a
complication.

311
311
(3) Splenic tuberculosis (16.5).
Anti-TB therapy should make splenectomy superfluous;
fibrosis during healing will shrink the spleen. HIV disease
is particularly likely.
(4) Leishmaniasis (34.7). Medication should likewise
make splenectomy unnecessary.
(5) Acute diseases, viz. leptospirosis, acute thrombo-
cytopenia.
(6) HIV disease (5.6).
Whilst not an absolute rule, the risk of infection increases,
and so the indication must be really good. Institute ARV
treatment first.
CAUTION!
(1);Do not operate lightly; your only absolute indications
for doing so are the first three.
(2);If the spleen is huge, think seriously about operating
because it may need a thoraco-abdominal approach.
SPLENECTOMY (GRADE 3.4)
PREPARATION.
Make sure you have a wide bore cannula in place for fluid
replacement; have blood cross-matched (but do not be in a
hurry to raise the haemoglobin if this has been chronically
low), and a nasogastric tube to decompress the stomach.
Provided there is no allergy, always give prophylactic
penicillin perioperatively. Place a sandbag or pillow
behind the left thorax to rotate it to the right.
INCISION. Make a midline or left subcostal incision:
this will give better direct access to the spleen, and you
can extend this as a chevron with a right subcostal
incision. Alternatively for a very big malarial spleen,
you can make a left thoraco-abdominal incision, because
this allows you to see vascular diaphragmatic adhesions
directly. (11.1)
Doing an elective splenectomy is different from an
emergency splenectomy in that you can approach the
spleen in a relaxed manner. Explore the abdomen,
noting the condition of the liver and presence of any
lymph nodes, as well as the mobility of the spleen.
If it is adherent, and large, it is wisest to tie the splenic
vessels first.
You can improve access by placing a pack behind the
spleen if there are insignificant adhesions. Otherwise
divide the peritoneal attachments. If bleeding is a problem
at this stage, deliver the spleen, rotate it forwards to the
right and tie a thick ligature right round the entire splenic
pedicle. This is safer than trying to grasp it with a large
clamp. As you do so, try not to damage the stomach,
and try to cause the least possible damage to the pancreas.
When you have controlled bleeding, proceed to tie the
vessels individually.
Enter the lesser sac by opening a window in the greater
omentum, and lift up the stomach off the pancreas by
dividing the adhesions between them a short distance.
Then feel for the splenic artery along the upper border of
the pancreas. Incise the peritoneum over it, pass an angled
haemostat underneath it and pass ligatures round it.
Carefully expose the splenic vein by dissecting away the
fatty tissue in the pedicle and tie it off. You can then tie off
the splenic artery and divide the splenic pedicle.
For extra security apply a second set of ligatures at the
same point before the vessels divide.
CAUTION! Make sure you pass the ligatures and tie
them before dividing the vessels. If you use haemostats
and the cut vessel drops off and is lost in a pool of blood,
you may never find it again.
If you haven’t been able to draw the spleen forwards,
do so now, if necessary by dividing adhesions to the
parietal peritoneum. Then divide the peritoneum lateral to
the spleen (the lienorenal ligament); put your finger into
the opening and gently free the spleen. You can now bring
it well outside the abdomen. Free the splenic flexure of the
colon from the spleen and separate the tail of the pancreas
from the splenic vessels. Free the spleen from its
attachments to the greater curvature of the stomach by
dividing the short gastric vessels individually in the
gastrosplenic ligament.
CAUTION! Do not include an area of stomach wall
with your ligatures, especially at the upper margin of the
spleen.
Remove the spleen, keeping it in saline for possible
autotransplantation (see below), and put a big dry pack in
the splenic bed. Leave it there for 5mins; then remove it
and look for any bleeding vessels and tie them off.
If the operative site is not absolutely dry and you are
uncertain about an injury to the tail of the pancreas, place a
large drain in the splenic bed.
SPLENIC IMPLANTATION. This is controversial and
may not work. Keep some slices of spleen, say 5x3x0·5cm,
and implant them under the peritoneum in the side wall of
the abdomen, or in the anterior abdominal wall. Or, place
some 1cm cubes of spleen within a sandwich of omentum.
They will usually take, and may reduce the severity of
attacks of malaria and perhaps the danger of septicaemia,
but will not fully protect against pneumococci.
The risk of adhesions is much less than the risk of
life-threatening infections. You can check if the splenic
slices are functional after 4wks if there are no Howell-Jolly
bodies and no target cells in the peripheral blood film,
and the platelet count is normal.
Do not do this with splenectomy indications 4,5,6 or if
there is already an accessory spleen.
SEGMENTAL SPLENECTOMY (GRADE 3.5)
Preserving a functional remnant of c. 20-30% of the spleen
avoids septic and immunological problems also; it can also
be used in hypersplenism. You need to devascularize
anatomical segments (especially middle and lower
portions) of the spleen, by ligating branches of the splenic
artery at the hilum.
Wait for 5mins to observe a line of demarcation, and cut it
along this line in a V-shape whilst squeezing the proximal
portion manually. A vascular clamp across the pedicle will
reduce bleeding. Then sew over the remnant an omental
patch, bringing the edges of the ‘V’ together. This is not
easy surgery.

312
312
DIFFICULTIES WITH SPLENECTOMY
If you have damaged the stomach or the colon, close the
perforation in two layers with long-acting absorbable
suture, make sure nasogastric suction is in place.
Start gentamicin and metronidazole.
If you have damaged the pancreas, suture a piece of
omentum over the damaged segment of pancreas and leave
a drain. Try to monitor the amylase levels of fluid draining
If bleeding from the diaphragm persists, insert one or
two dry packs for 10mins by the clock; then come back
and remove them to see if you can identify the bleeding
vessels to tie them. If you still fail to control bleeding,
leave packs tightly in situ, close the abdomen, and return
after 48hrs to remove them by which time the bleeding
will almost certainly have stopped.
If shock suddenly develops postoperatively, a ligature
has probably come off. Reopen the abdomen immediately,
with good suction available to try to find the bleeding
vessel, and tie it off.
If the wound sloughs and there is a fluid discharge,
the tail of the pancreas or stomach may have been injured.
Reopen the wound, and suture a piece of omentum over
the damaged viscus; do not try to ligate the pancreas or
suture the gastric perforation as sutures will probably cut
out and cause more damage.
If there is fever with no obvious cause, and you have
given penicillin, check for a subphrenic abscess (10.2).
If there is rapidly developing haemolytic anaemia and
fever, suspect malaria or babesiosis, a tick-borne illness
usually affecting domestic or wild animals, and get both
thick and thin blood films. Use quinine 650mg orally tid
and clindamycin 600mg orally tid for 5-10days.
If there is respiratory distress postoperatively, think of
a pneumothorax.
POSTOPERATIVE CARE AFTER SPLENECTOMY
Treat with penicillin prophylactically for 2wks, and longer
in children <2yrs. If you can get it, pneumococcus,
haemophilus and meningococcus vaccine is very
beneficial. Insist on malaria prophylaxis in endemic areas,
including the perioperative period.
15.18 Splenic abscess
This starts acutely, though it may become chronic.
It occurs in sickle cell disease, acute myeloid leukaemia,
HIV+ve patients with candidiasis, and secondary to
amoebiasis, brucellosis, salmonellosis, leptospirosis and
occasionally as a result of acute pancreatitis or perforation
from a gastric ulcer. The danger is rupture into the
peritoneal or pleural cavity and may be accompanied by
disastrous bleeding.
There is left upper abdominal pain, a dragging sensation in
the abdomen, discomfort after meals, anorexia, and a
palpable tender mass extending down from the left upper
quadrant towards the right lower quadrant. This might be
huge. There is usually anaemia and a low-grade fever.
The mass may be tympanic because it usually is filled with
gas, arising from oxygen liberated by red cells in the
spleen, and carbon dioxide from tissue metabolism rather
than gas-forming organisms.
SPECIAL TESTS. Leucocytosis and anaemia are usual,
but the white count may not be raised with HIV disease.
CHEST RADIOGRAPH. An erect film will show a gas
bubble and fluid level below the left hemidiaphragm,
pushing it upwards.
ULTRASOUND. Look for a fluid-filled cavity in the area
of the spleen (38.2F). Much of the splenic tissue may be
destroyed. Aspiration will confirm the diagnosis, but
beware of causing severe haemorrhage or rupturing the
colon. You may be able to aspirate a splenic abscess
completely, and avoid surgery. Treat with antibiotics 48hrs
beforehand and then follow a procedure as for a liver
abscess (15.10).
LAPAROTOMY FOR SPLENIC ABSCESS (GRADE 3.1)
INDICATIONS. Essentially all splenic abscesses need
surgery.
PREPARATION. Cross-match blood and start
pre-operative penicillin and metronidazole.
EXPLORATION. Make a left subcostal incision or
Chevron (inverted-V double subcostal) for very big
abscesses. Pack away the rest of the abdominal contents.
Drain the abscess and leave a large tube or catheter in the
space, passed through a separate stab incision in the lateral
abdominal wall. Lavage the abdomen with warm saline or
water.
DIFFICULTIES WITH SPLENIC ABSCESS
If access is difficult and you have made a midline incision
not expecting a splenic abscess, extend it as an inverted-L
laterally with a left subcostal arm, as a left-sided Kocher
incision (11-1).
If serious bleeding from the spleen ensues, pack the area
and press firmly. Get assistance. Place a further pack
(or two) above and behind the spleen to lift it forward,
and perform a splenectomy (15.17). If you are
experienced, this is the definitive operation rather than
simple drainage.
If you find a gastric perforation, the tissues will be very
friable. Don’t attempt to close the perforation with sutures,
but stuff a segment of omentum into the hole, and fix it
there with absorbable sutures. Make sure you drain the
stomach with a nasogastric tube. You are unlikely to be
able to save the spleen because unravelling the inflamed
tissues will damage it and result in considerable bleeding.
Grasp the hilum of the spleen, place a pack or two behind
it, and perform a splenectomy (15.17)