Stress Management Allan Sanders, MN, ARNP [email protected].
Upload
jessie-rickardsCategory
view
214download
1
1
Multi-Disciplinary Heart Failure Management
Connie Keibler, MSN, ARNP
Western Washington Medical Group, Cardiology
2
3
Heart Failure Outlook
• 5 million Americans have Heart Failure
• 1/2 million new diagnosis of HF annually
• $27 Billion annual health care burden
• 250,000 deaths from HF annually
• Leading cause of hospitalization for those over 65 years old
4
Heart Failure Hospitalization• $14 Billion spent annually for those admitted to the
hospital in Acute Decompensated Heart Failure• 3.5 million hospitalizations annually• 1/3 of those admitted for ADHF are re-admitted
within 90 days• A hospital visit for ADHF results in 60 day
mortality rates between 8 and 20%• Increased mortality risk persists for 6 mos.

5
Heart Failure Future

6
Heart Failure Mortality
• 250, 000 deaths annually
• 1/2 of those diagnosed with Heart Failure die within 5 years
Leading Causes of Death CDC 2005
Heart Disease
Cancer
Stroke
Accidents
Chronic Lung Disease
Diabetes
Nephritis
Alzheimers
Influenza/Pneumonia
Septicemia
7
8
Heart Failure Risk
Common Causes– Ischemic heart Disease
– Diabetes
– Hypertension
– Valvular Heart Disease
– ETOH Abuse
– Obesity
– Cigarette Smoking
– Hyperlipidemia
– Physical Inactivity
– Sleep Apnea
Less Common Causes– Familial Hypertrophic CM
– Postpartum CM
– Thyroid Abnormality
– Connective Tissue Disorders
– Toxin Exposure
– Myocarditis
– Sarcoidosis
– Hemochromatosis
– Medication Exposure
9
Heart Failure-A Syndrome
Heart failure is a constellation of symptoms and signs produced by a complex circulatory and neuro-hormonal response to cardiac dysfunction
Heart failure is a complex clinical syndrome that can results from any structural or functional cardiac disorder that impairs the ability of the ventricle to fill with or eject blood.
10
Clinical Classifications
• Backward– Inability of the ventricle to eject its contents,
resulting in elevated filling pressures
• Forward– decreased cardiac output and inadequate tissue
perfusion
11
Clinical Classifications
• Left-Sided– Left Ventricle is weakened or overloaded
• Results in pulmonary congestion
• Right-Sided– Right Ventricle is impaired
• Results in systemic venous overload
• May occur independently from conditions affecting the right ventricle only
• Left-Sided failure usually is the cause of right-sided failure

12
Clinical Classifications• Systolic:
– Impaired ability of the heart to contract– Weakened muscle, enlarged heart size– Inability of heart to empty– Left ventricular ejection fraction (LVEF) < 40–45%
• Diastolic: – inability of the heart to relax is impaired– Stiff, thickened myocardial wall but normal size– Inability of heart to fill– LVEF 45%
13
Clinical Classifications
• Acute– sudden onset with associated signs and
symptoms
• Chronic– secondary to slow structural changes occurring
in the stressed myocardium
• Acute Decompensated– sudden exacerbation or onset of symptoms in
chronic heart failure
14
Clinical ClassificationsHeart Failure is a Symptomatic Disorder
New York Heart Association-Functional Classification
Class I: No abnormal symptoms with activity
Class II: Symptoms with normal activity
Class III: Marked limitation due to symptoms with less than ordinary activity
Class IV: Symptoms at rest and severe limitations in functional activity
15
Clinical ClassificationsHeart Failure is a Progressive Disorder
ACC/AHA Stages of HFStage A--Presence of risk factors for heart failure
Stage B--Presence of structural heart disease but no Symptoms
Stage C--Presence of structural heart disease along with signs and symptoms
Stage D--Presence of structural heart diseases and advanced signs and symptoms

16
ACC/AHA 2005 Guidelines

17

18
HF Hospitalization
• 1/3 of those admitted for ADHF are re-admitted within 90 days
• 1/2 of all HF Hospital Re-Admissions are Avoidable
• A hospital visit for ADHF results in 60 day mortality rates between 8 and 20%
19
Clinical Predictors
• A Multivariate Analysis using the ADHERE Data Identified the Following Most Significant Predictors of Mortality:– Bun– Systolic BP– HR– Age
20
Seattle Heart Failure Model
• Age
• Gender
• Ischemic Etiology
• NYHA
• Ejection Fraction
• Systolic BP
• Cholesterol
• Hemoglobin
• % Lymphocyte Count
• Uric Acid
• Sodium
• Use of
– K-Sparing Diuretic
– Statin
– Allupurinol
– Diuretic
Multivariate risk model using the following Predictors of Survival at Baseline and after Interventions
21
Reasons for Re-Admission
• Compliance with Medication
• Compliance with Diet, Specifically Sodium
• Delays in Seeking Medical Attention
22
JACHO Quality of Care Indicators
• DC Instructions
• Assessment of LV Function
• ACEI or ARB at Discharge
• Smoking Cessation Advice/Counseling
23
JACHO Quality of Care Indicators
• Education better absorbed when the patient is stable and adapted to living with HF
• OPTIMIZE-HF found that DC Instructions did not have an effect on Mortality or Re-hospitalization @ 60-90 days.
• Missing continuity of Care in the Community• Home Care• Heart Failure Clinics• Primary Care
24
Barrier to HF Management
• Cognitive Impairment• Complex Self Care
Management• Lack of Motivation
– Poor Physical Capacity
– Depression
– Anxiety
• Multiple Co-Morbidities• Psychosocial/Financial
Concerns• Physical Limitations• Multiple Heath Care
Providers and Lack of Shared Communication

25
26
Heart Failure Management
• Improve Access to Appropriate Cost-Effective Health Care
• Prevent Hospitalization
• Improve QOL
• Improved Survival
• Control Health Care Costs
Goals

27
Multi-Disciplinary HF MGMT
• Fluid Management• Education
• Intensity of Care• Access
Characteristics
Strategy must outline and follow clinical rationalebased on practice guidelines that define target care patterns for patients.

28
Systematic Review
• Literature Review• 74 Trials and 30 Meta-
Analysis• Shared Key Elements
– One to One Patient Education
– Symptom Monitoring and Strategies for Self-Management
0% 5% 10% 15% 20% 25% 30%
All CauseHospitalization
All CauseMortality
HFHospitalization
Multi-Disciplinary Interventions for Heart Failure

29
Self-Management of HF• Compliance with evidence based medications• Adopt a low-sodium diet• Reduce fat and cholesterol in diet• Restrict fluid intake if indicated• Stop smoking• Eliminate alcohol consumption• Increase activity/exercise• Monitor daily weight

30
Self-Management of HFAND Notify health care provider of signs and symptoms of
worsening heart failure – pain in jaw, neck, or chest– increased SOB– increased fatigue– dizziness of syncope– swelling in feet, ankles, legs, or abdomen– palpitations– tachycardia– weight gain– decreased exercise capacity

31
Deventer-Alkmaar HF Study• Physician and Nurse Directed HF Clinic vs. Usual Care
– 1 year intervention– 9 scheduled visits
• 3 telephone• 6 office• 1 week after discharge• Verbal and written education• Optimized Rx• Easy Access• Advice for self-care
32
Deventer-Alkmaar HF Study
• 51% risk reduction in Primary End-Point
– Hospitalization for worsened HF and/or All Cause Mortality
– NNT - 5
• Improved EF at 1 Year
• Improved NYHA Class
• Significant Improvement in QOL Scores
33
Multi-Disciplinary Management
• Quick and sustained improvements
• 6 wk intervention
• Cost savings of $67,804
Comprehensive inpatient education, discharge planning,and outpatient support vs. usual care*
•Multi-Disciplinary TeamPhysician ChampionAdvanced Practice Nurse or PANurse EducatorHome Health NurseDieticianPhysical TherapySocial ServicesPharmacist

34

35
Nursing
Nursing is a profession focused on assisting individuals, families,
and communities in attaining, maintaining, and recovering
optimal health and functioning. Modern definitions of nursing
define it as a science and an art that focuses on promoting quality
of life as defined by persons and families, throughout their life
experiences from birth to care at the end of life.
36
Collaborative practice is intended to combine the knowledge and skills
of several health professionals to maximize the efficiency of both the clinicians
and the health care system.
Collaborative practice brings together health care professionals with different
and complimentary knowledge and skills to increase the scope of and
access to patient services.
Collaborative Practice
Shared responsibility and outcomes
37
Collaborative Practice
• Correct and accurate transfer of vital patient information
• Effective team collaboration that produces positive patient care outcomes
• Behaviors that aid and encourage respect, trust and credibility among team members
Expected Outcomes

38

39
Just One DayEL
89 y/o female
CAD, S/P MI
Ischemic CM/EF 20/NYHA Class III
DM Type II
Chronic Renal Insufficiency/GFR 38
Parox Afib on Amiodarone
Dyslipidemia
ICD/DDD
SB
70 y/o Male
SSS
Chronic Afib
Idiopathic CM/EF 30/NYHA Class I
HTN
DS
76 y/o Male
CAD w/ recent MI/Stent
Ischemic CM/EF 45/NYHA Class II
Diabetes/Poorly controlled/HgA1C 10
HTN
Dyslipidemia
Chronic renal insufficiency
LO
87 y/o Male
CM/EF 24/NYHA Class III
HTN
Dyslipidemia
Chronic Alcoholism
Chronic Afib
Chronic renal insufficiency/GFR 37
40
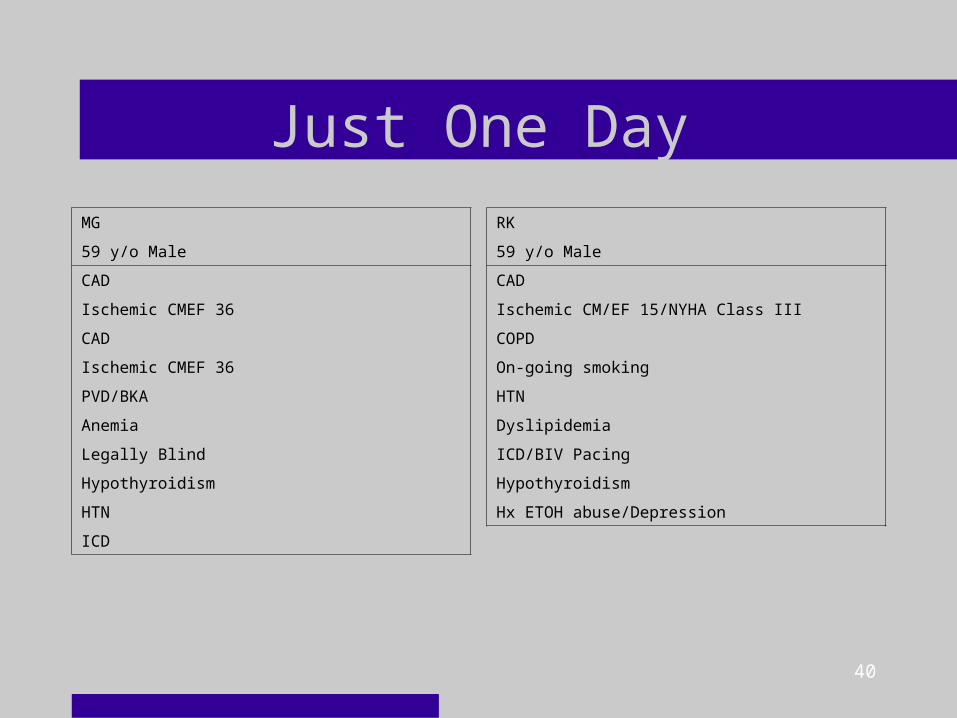
Just One Day
MG
59 y/o Male
CAD
Ischemic CMEF 36
CAD
Ischemic CMEF 36
PVD/BKA
Anemia
Legally Blind
Hypothyroidism
HTN
ICD
RK
59 y/o Male
CAD
Ischemic CM/EF 15/NYHA Class III
COPD
On-going smoking
HTN
Dyslipidemia
ICD/BIV Pacing
Hypothyroidism
Hx ETOH abuse/Depression
41
Cardiac Rhythm Management
•Small improvements in hemodynamics =significant improvements in HF symptoms symptoms.•Optimizing hemodynamics has long been a target of therapy in HF.
42
Cardiac Rhythm Management
•Risk Reduction•CRT•Diagnostics
•HR Trends•HR Variability•Patient Activity•Intrathoracic Impedance
•Arrhythmias•Remote Monitoring
43
Cardiac Rhythm Management
• Identify and recognize cardiac device patients who are eligible for monitoring
• Download device data• Analyze/interpret the data• Use the data to guide therapy• Establish a collaborative model and cooperative
environment between the EP team and HF
Goals for Heart Failure Management

44
Quality of Life Issues
End of Life Issues
And

45
Challenges are what make life interesting;
overcoming them is what makes life meaningful. -Joshua J. Marine
I am only one,But still I am one.I cannot do everything,But still I can do something;And because I cannot do everythingI will not refuse to do the something that I can do.- Edward Everett Hale
46
References
47
References
48
References