
06 Anatomy
63
Question 1 of 263 Next A 56 year old man is left impotent following an abdomino-perineal excision of the colon and rectum. What is the most likely explanation? A. Psychosexual issues related to an end colostomy B. Damage to the sacral venous plexus during total mesorectal excision C. Damage to the left ureter during sigmoid mobilisation D. Damage to the hypogastric plexus during mobilisation of the inferior mesenteric artery E. Damage to the internal iliac artery during total mesorectal excision Next question Autonomic nerve injury is the most common cause. Nerve lesions during surgery A variety of different procedures carry the risk of iatrogenic nerve injury. These are important not only from the patients perspective but also from a medicolegal standpoint. The following operations and their associated nerve lesions are listed here: • Posterior triangle lymph node biopsy and accessory nerve lesion. • Lloyd Davies stirrups and common peroneal nerve. • Thyroidectomy and laryngeal nerve. • Anterior resection of rectum and hypogastric autonomic nerves. • Axillary node clearance; long thoracic nerve, thoracodorsal nerve and intercostobrachial nerve. • Inguinal hernia surgery and ilioinguinal nerve. • Varicose vein surgery- sural and saphenous nerves. • Posterior approach to the hip and sciatic nerve. • Carotid endarterectomy and hypoglossal nerve. There are many more, with sound anatomical understanding of the commonly performed procedures the incidence of nerve lesions can be minimised. They commonly occur when surgeons operate in an unfamiliar tissue plane or by blind placement of haemostats (not recommended). Previous Question 2 of 263 Next A 73 year old man is due to undergo a radical prostatectomy for carcinoma of the prostate gland. To which of the following lymph nodes will the tumour drain primarily?
-
Upload
tahirthegreat2939 -
Category
Documents
-
view
11 -
download
2
description
mrcs
Transcript of 06 Anatomy

Question 1 of 263
Next
A 56 year old man is left impotent following an abdomino-perineal excision of the colon and rectum. What is the most likely
explanation?
A. Psychosexual issues related to an end colostomy
B. Damage to the sacral venous plexus during total mesorectal excision
C. Damage to the left ureter during sigmoid mobilisation
D. Damage to the hypogastric plexus during mobilisation of the inferior
mesenteric artery
E. Damage to the internal iliac artery during total mesorectal excision
Next question
Autonomic nerve injury is the most common cause.
Nerve lesions during surgery
A variety of different procedures carry the risk of iatrogenic nerve injury. These are important not only from the patients
perspective but also from a medicolegal standpoint.
The following operations and their associated nerve lesions are listed here:
• Posterior triangle lymph node biopsy and accessory nerve lesion.
• Lloyd Davies stirrups and common peroneal nerve.
• Thyroidectomy and laryngeal nerve.
• Anterior resection of rectum and hypogastric autonomic nerves.
• Axillary node clearance; long thoracic nerve, thoracodorsal nerve and intercostobrachial nerve.
• Inguinal hernia surgery and ilioinguinal nerve.
• Varicose vein surgery- sural and saphenous nerves.
• Posterior approach to the hip and sciatic nerve.
• Carotid endarterectomy and hypoglossal nerve.
There are many more, with sound anatomical understanding of the commonly performed procedures the incidence of nerve
lesions can be minimised. They commonly occur when surgeons operate in an unfamiliar tissue plane or by blind placement of
haemostats (not recommended).
Previous
Question 2 of 263
Next
A 73 year old man is due to undergo a radical prostatectomy for carcinoma of the prostate gland. To which of the following lymph nodes will the tumour drain primarily?
A. Para aortic
B. Internal iliac
C. Superficial inguinal
D. Meso rectal
E. None of the above
Next question The prostate lymphatic drainage is primarily to the internal iliac nodes and also the sacral nodes. Although internal iliac is the first site.
Prostate gland The prostate gland is approximately the shape and size of a walnut and is located inferior to the bladder. It is separated from the rectum by Denonvilliers fascia and its blood supply is derived from the internal iliac vessels. The internal sphincter lies at the apex of the gland and may be damaged during prostatic surgery, affected individuals may complain of retrograde ejaculation. Summary of prostate gland
Arterial supply Inferior vesical artery (from internal iliac)
Venous drainage Prostatic venous plexus (to paravertebral veins)
Lymphatic drainage Internal iliac nodes
Innervation Inferior hypogastric plexus
Dimensions • Transverse diameter (4cm) • AP diameter (2cm) • Height (3cm)
Lobes • Posterior lobe: posterior to urethra • Median lobe: posterior to urethra, in between ejaculatory ducts • Lateral lobes x 2 • Isthmus
Zones • Peripheral zone: subcapsular portion of posterior prostate. Most prostate cancers are here • Central zone • Transition zone • Stroma
Relations

Anterior Pubic symphysis Prostatic venous plexus
Posterior Denonvilliers fascia Rectum Ejaculatory ducts
Lateral Venous plexus (lies on prostate) Levator ani (immediately below the puboprostatic ligaments)
Previous
Question 3 of 263
Next
Which of the following statements relating to the vertebral column is false?
A. There are 7 cervical vertebrae
B. The cervical and lumbar lordosis are secondary curves developing after birth
due to change in shape of the intervertebral discs
C. The lumbar vertebrae do not have a transverse process foramina
D. The lumbar vertebrae receive blood directly from the aorta
E. The spinous process is formed by the junction of the pedicles posteriorly
Next question
The spinous process is formed by 2 laminae posteriorly.
Vertebral column

• There are 7 cervical, 12 thoracic, 5 lumbar, and 5 sacral vertebrae.
• The spinal cord segmental levels do not necessarily correspond to the vertebral segments. For example, while the C1
cord is located at the C1 vertebra, the C8 cord is situated at the C7 vertebra. While the T1 cord is situated at the T1
vertebra, the T12 cord is situated at the T8 vertebra. The lumbar cord is situated between T9 and T11 vertebrae. The
sacral cord is situated between the T12 to L2 vertebrae.
Cervical vertebrae
The interface between the first and second vertebra is called the atlanto-axis junction. The C3 cord contains the phrenic nucleus.
The cervical cord innervates the deltoids (C4), biceps (C4-5), wrist extensors (C6-8), triceps (C7), wrist flexors (C8-T1), and
hand muscles (C8-T1).
Thoracic vertebrae
The thoracic vertebral segments are defined by those that have a rib. The spinal roots form the intercostal nerves that run on the
bottom side of the ribs and these nerves control the intercostal muscles and associated dermatomes.
Lumbosacral vertebrae
Form the remainder of the segments below the vertebrae of the thorax. The lumbosacral spinal cord, however, starts at about T9
and continues only to L2. It contains most of the segments that innervate the hip and legs, as well as the buttocks and anal
regions.
Cauda Equina
The spinal cord ends at L2 vertebral level. The tip of the spinal cord is called the conus. Below the conus, there is a spray of
spinal roots that is called the cauda equina. Injuries below L2 represent injuries to spinal roots rather than the spinal cord proper.
Previous
Question 4 of 263
Next
The cephalic vein pierces the clavipectoral fascia to terminate in which of the veins listed below?
A. External jugular
B. Axillary
C. Internal jugular
D. Azygos
E. Brachial
Next question
Cephalic vein
Path

• Dorsal venous arch drains laterally into the cephalic vein
• Crosses the anatomical snuffbox and travels laterally up the arm
• At the antecubital fossa connected to the basilic vein by the median cubital vein
• Pierces deep fascia of deltopectoral groove to join axillary vein
Previous
Question 5 of 263
Next
A 78 year old lady falls over in her nursing home and sustains a displaced intracapsular fracture of the femoral neck. A decision
is made to perform a hemi arthroplasty through a lateral approach. Which of these vessels will be divided to facilitate access?
A. Saphenous vein
B. Superior gluteal artery
C. Superficial circumflex iliac artery
D. Profunda femoris artery
E. Transverse branch of the lateral circumflex artery
Next question
During the Hardinge style lateral approach the transverse branch of the lateral circumflex artery is divided to gain access. The
vessels and its branches are illustrated below:

Image sourced from Wikipedia
Hip joint
• Head of femur articulates with acetabulum of the pelvis
• Both covered by articular hyaline cartilage
• The acetabulum forms at the union of the ilium, pubis, and ischium
• The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones
• The acetabulum holds the femoral head by the acetabular labrum
• Normal angle between femoral head and femoral shaft is 130o
Ligaments
• Transverse ligament: joints anterior and posterior ends of the articular cartilage

• Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial supply to head of femur in
children.
Image sourced from Wikipedia
Image sourced from Wikipedia
Extracapsular ligaments
• Iliofemoral ligament: inverted Y shape. Anterior iliac spine to the trochanteric line
• Pubofemoral ligament: acetabulum to lesser trochanter
• Ischiofemoral ligament: posterior support. Ischium to greater trochanter.

Blood supply
Medial circumflex femoral and lateral circumflex femoral arteries (Branches of profunda femoris)
2 anastomoses: Cruciate and the trochanteric anastomoses (provides most of the blood to the head of the femur) Hence the need
for hemiarthroplasty when there is a displaced femoral head fracture. These anastomoses exist between the femoral artery or
profunda femoris and the gluteal vessels.
Previous
Question 6 of 263
Next
A 73 year old man undergoes a sub total oesophagectomy with anastomosis of the stomach to the cervical oesophagus. Which
vessel will be primarily responsible for the arterial supply to the oesophageal portion of the anastomosis?
A. Superior thyroid artery
B. Internal carotid artery
C. Direct branches from the thoracic aorta
D. Inferior thyroid artery
E. Subclavian artery
Next question
The cervical oesophagus is supplied by the inferior thyroid artery. The thoracic oesophagus (removed in this case) is supplied
by direct branches from the thoracic aorta.
Oesophagus
• 25cm long
• Starts at C6 vertebra, pierces diaphragm at T10 and ends at T11
• Squamous epithelium
Constrictions of the oesophagus
Structure Distance from incisors
Cricoid cartilage 15cm
Arch of the Aorta 22.5cm
Left principal bronchus 27cm

Diaphragmatic hiatus 40cm
Relations
Anteriorly • Trachea to T4 • Recurrent laryngeal nerve • Left bronchus, Left atrium • Diaphragm
Posteriorly • Thoracic duct to left at T5 • Hemiazygos to the left T8 • Descending aorta • First 2 intercostal branches of aorta
Left • Thoracic duct • Left subclavian artery
Right • Azygos vein
Arterial, venous and lymphatic drainage of the oesophagus
Artery Vein Lymphatics Muscularis externa
Upper third Inferior thyroid Inferior thyroid Deep cervical Striated muscle
Mid third Aortic branches Azygos branches Mediastinal Smooth & striated muscle
Lower third Left gastric Posterior mediastinal and coeliac Gastric Smooth muscle
Nerve supply
• Upper half is supplied by recurrent laryngeal nerve
• Lower half by oesophageal plexus (vagus)
Histology
• Mucosa :Nonkeratinized stratified squamous epithelium
• Submucosa: glandular tissue
• Muscularis externa (muscularis): composition varies. See table
• Adventitia

• Previous
Question 7 of 263
Next
Which of the following structures is not closely related to the brachial artery?
A. Ulnar nerve
B. Median nerve
C. Cephalic vein
D. Long head of triceps
E. Median cubital vein
Next question
The cephalic vein lies superficially and on the contralateral side of the arm to the brachial artery. The relation of the ulnar
nerves and others are demonstrated in the image below:
Image sourced from Wikipedia
Brachial artery
The brachial artery begins at the lower border of teres major as a continuation of the axillary artery. It terminates in the cubital
fossa at the level of the neck of the radius by dividing into the radial and ulnar arteries.
Relations
Posterior relations include the long head of triceps with the radial nerve and profunda vessels intervening. Anteriorly it is
overlapped by the medial border of biceps.
It is crossed by the median nerve in the middle of the arm.
In the cubital fossa it is separated from the median cubital vein by the bicipital aponeurosis.
The basilic vein is in contact at the most proximal aspect of the cubital fossa and lies medially.
Previous
Question 8 of 263
Next
The following statements relating to the musculocutaneous nerve are true except?
A. It arises from the lateral cord of the brachial plexus
B. It provides cutaneous innervation to the lateral side of the forearm
C. If damaged then extension of the elbow joint will be impaired
D. It supplies the biceps muscle
E. It runs beneath biceps
Next question
It supplies biceps, brachialis and coracobrachialis so if damaged then elbow flexion will be impaired.
Musculocutaneous nerve
• Branch of lateral cord of brachial plexus
Path
• It penetrates the Coracobrachialis muscle
• Passes obliquely between the Biceps brachii and the Brachialis to the lateral side of the arm
• Above the elbow it pierces the deep fascia lateral to the tendon of the Biceps brachii
• Continues into the forearm as the lateral cutaneous nerve of the forearm
Innervates
• Coracobrachialis
• Biceps brachii
• Brachialis
Previous
Question 9 of 263
Next
Which ligament keeps the head of the radius connected to the radial notch of the ulna?
A. Annular (orbicular) ligament
B. Quadrate ligament
C. Radial collateral ligament of the elbow
D. Ulnar collateral ligament

E. Radial collateral ligament
Next question
The annular ligament connects the radial head to the radial notch of the ulna. This is illustrated below:
Image sourced from Wikipedia
Radius
• Bone of the forearm extending from the lateral side of the elbow to the thumb side of the wrist
Upper end
• Articular cartilage- covers medial > lateral side
• Articulates with radial notch of the ulna by the annular ligament
• Muscle attachment- biceps brachii at the tuberosity
Shaft
• Muscle attachment-
Upper third of the body Supinator, Flexor digitorum superficialis, Flexor pollicis longus

Middle third of the body Pronator teres
Lower quarter of the body Pronator quadratus , tendon of supinator longus
Lower end
• Quadrilateral
• Anterior surface- capsule of wrist joint
• Medial surface- head of ulna
• Lateral surface- ends in the styloid process
• Posterior surface: 3 grooves containing:
1. Tendons of extensor carpi radialis longus and brevis
2. Tendon of extensor pollicis longus
3. Tendon of extensor indicis

Image sourced from Wikipedia
Previous
Question 10 of 263
Next
A 38 year old man presents to the clinic with shoulder weakness. On examination he has an inability to initiate shoulder
abduction. Which of the nerves listed below is least likely to be functioning normally?
A. Suprascapular nerve
B. Medial pectoral nerve
C. Axillary nerve
D. Median nerve
E. Radial nerve
Next question
Theme from April 2012 Exam
Suprascapular nerve
The suprascapular nerve arises from the upper trunk of the brachial plexus. It lies superior to the trunks of the brachial plexus
and passes inferolaterally parallel to them. It passes through the scapular notch, deep to trapezius. It innervates both
supraspinatus and infraspinatus and initiates abduction of the shoulder. If damaged, patients may be able to abduct the shoulder
by leaning over the affected side and deltoid can then continue to abduct the shoulder.

I
Previous
Question 11 of 263
Next
Which of the following statements relating to the Cavernous Sinus is false?
A. The pituitary gland lies medially
B. The internal carotid artery passes through it
C. The temporal lobe of the brain is a lateral relation
D. The mandibular branch of the trigeminal and optic nerve lie on the lateral wall
E. The ophthalmic veins drain into the anterior aspect of the sinus
Next question

The veins that drain into the sinus are important as sepsis can cause cavernous sinus thrombosis. The maxillary branch of the
trigeminal and not the mandibular branches pass through the sinus
Cavernous sinus
The cavernous sinuses are paired and are situated on the body of the sphenoid bone. It runs from the superior orbital fissure to
the petrous temporal bone.
Relations
Medial Lateral
Pituitary fossa Sphenoid sinus
Temporal lobe
Contents
Lateral wall components (from top to bottom:) Oculomotor nerve Trochlear nerve Ophthalmic nerve Maxillary nerve
Contents of the sinus (from medial to lateral:) Internal carotid artery (and sympathetic plexus) Abducens nerve
Blood supply
Ophthalmic vein, superficial cortical veins, basilar plexus of veins posteriorly.
Drains into the internal jugular vein via: the superior and inferior petrosal sinuses
Image sourced from Wikipedia
Previous
Question 12 of 263
Next

Which of the following is not a branch of the subclavian artery?
A. Superior thyroid artery
B. Vertebral artery
C. Thyrocervical trunk
D. Internal thoracic artery
E. Dorsal scapular artery
Next question
Mnemonic for the branches of the subclavian artery: VIT C & D
V ertebral artery
I nternal thoracic
T hyrocervical trunk
C ostalcervical trunk
D orsal scapular
Superior thyroid artery is a branch of the external carotid artery.
Subclavian artery
Path
• The left subclavian comes directly off the arch of aorta
• The right subclavian arises from the brachiocephalic artery (trunk) when it bifurcates into the subclavian and the right
common carotid artery.
• From its origin, the subclavian artery travels laterally, passing between anterior and middle scalene muscles, deep to
scalenus anterior and anterior to scalenus medius. As the subclavian artery crosses the lateral border of the first rib, it
becomes the axillary artery. At this point it is superficial and within the subclavian triangle.

Image sourced from Wikipedia
Branches
• Vertebral artery
• Internal thoracic artery
• Thyrocervical trunk
• Costocervical trunk
• Dorsal scapular artery
Previous
Question 13 of 263
Next
During the repair of an atrial septal defect the surgeons note that blood starts to leak from the coronary sinus. Which structure
forms the largest tributary of the coronary sinus?
A. Thesbian veins
B. Great cardiac vein
C. Oblique vein
D. Small cardiac veins
E. None of the above
Next question
The great cardiac vein runs in the anterior interventricular groove, and is the largest tributary of the coronary sinus. The
Thesbian veins drain into the heart directly.
Heart anatomy

The walls of each cardiac chamber comprise:
• Epicardium
• Myocardium
• Endocardium
Cardiac muscle is attached to the cardiac fibrous skeleton.
Relations
The heart and roots of the great vessels within the pericardial sac are related anteriorly to the sternum, medial ends of the 3rd to
5th ribs on the left and their associated costal cartilages. The heart and pericardial sac are situated obliquely two thirds to the left
and one third to the right of the median plane.
The pulmonary valve lies at the level of the left third costal cartilage.
The mitral valve lies at the level of the fourth costal cartilage.
Coronary sinus
This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The great cardiac vein lies at its
left and the middle and small cardiac veins lie on its right. The smallest cardiac veins drain into the atria directly.
Aortic sinus
Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus and no vessel emerges from
the posterior sinus.
Right and left ventricles
Structure Left Ventricle
A-V Valve Mitral (double leaflet)
Walls Twice as thick as right
Trabeculae carnae Much thicker and more numerous
Right coronary artery
The RCA supplies:
• Right atrium
• Diaphragmatic part of the left ventricle
• Usually the posterior third of the interventricular septum
• The sino atrial node (60% cases)
• The atrio ventricular node (80% cases)

Left coronary artery
The LCA supplies:
• Left atrium
• Most of left ventricle
• Part of the right ventricle
• Anterior two thirds of the inter ventricular septum
• The sino atrial node (remaining 40% cases)
Innervation of the heart
Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the bifurcation of the trachea,
posterior to the ascending aorta and superior to the bifurcation of the pulmonary trunk. The parasympathetic supply to the heart
is from presynaptic fibres of the vagus nerves.
Valves of the heart
Mitral valve Aortic valve Pulmonary valve Tricuspid valve
2 cusps 3 cusps 3 cusps 3 cusps
First heart sound Second heart sound Second heart sound First heart sound
1 anterior cusp 1 anterior cusp 2 anterior cusps 2 anterior cusps
Attached to chordae tendinae No chordae No chordae Attached to chordae tendinae
Previous
Question 14 of 263
Next
Which of the following vessels provides the greatest contribution to the arterial supply of the breast?
A. External mammary artery
B. Thoracoacromial artery
C. Internal mammary artery
D. Lateral thoracic artery
E. Subclavian artery
Next question
60% of the arterial supply to the breast is derived from the internal mammary artery. The external mammary and lateral thoracic

arteries also make a significant (but lesser) contribution. This is of importance clinically in performing reduction mammoplasty
procedures.
Breast
The breast itself lies on a layer of pectoral fascia and the following muscles:
1. Pectoralis major
2. Serratus anterior
3. External oblique
Image showing the topography of the female breast
Image sourced from Wikipedia
Breast anatomy
Nerve supply Branches of intercostal nerves from T4-T6.
Arterial supply • Internal mammary (thoracic) artery • External mammary artery (laterally) • Anterior intercostal arteries • Thoraco-acromial artery
Venous drainage Superficial venous plexus to sub clavian, axillary and intercostal veins.
Lymphatic drainage • 70% Axillary nodes • Internal mammary chain • Other lymphatic sites such as deep cervical and supraclavicular fossa (later in disease)
Previous
Question 15 of 263
Next
Which of the following muscles is supplied by the external laryngeal nerve?
A. Transverse arytenoid
B. Cricothyroid
C. Thyro-arytenoid
D. Posterior crico-arytenoid
E. Oblique arytenoid
Next question

The others are all supplied by the recurrent laryngeal nerve.
Larynx
The larynx lies in the anterior part of the neck at the levels of C3 to C6 vertebral bodies. The laryngeal skeleton consists of a
number of cartilagenous segments. Three of these are paired; arytenoid, corniculate and cuneiform. Three are single; thyroid,
cricoid and epiglottic. The cricoid cartilage forms a complete ring (the only one to do so).
The laryngeal cavity extends from the laryngeal inlet to the level of the inferior border of the cricoid cartilage.
Divisions of the laryngeal cavity
Laryngeal vestibule Superior to the vestibular folds
Laryngeal ventricle Lies between vestibular folds and superior to the vocal cords
Infraglottic cavity Extends from vocal cords to inferior border of the cricoid cartilage
The vocal folds (true vocal cords) control sound production. The apex of each fold projects medially into the laryngeal cavity.
Each vocal fold includes:
• Vocal ligament
• Vocalis muscle (most medial part of thyroarytenoid muscle)
The glottis is composed of the vocal folds, processes and rima glottidis. The rima glottidis is the narrowest potential site within
the larynx, as the vocal cords may be completely opposed, forming a complete barrier.
Muscles of the larynx
Muscle Origin Insertion Innervation Action
Posterior cricoarytenoid
Posterior aspect of lamina of cricoid
Muscular process of arytenoid
Recurrent Laryngeal
Abducts vocal fold
Lateral cricoarytenoid
Arch of cricoid Muscular process of arytenoid
Recurrent laryngeal
Adducts vocal fold
Thyroarytenoid Posterior aspect of thyroid cartilage
Muscular process of arytenoid
Recurrent laryngeal
Relaxes vocal fold
Transverse and oblique arytenoids
Arytenoid cartilage Contralateral arytenoid Recurrent laryngeal
Closure of intercartilagenous part of the rima glottidis
Vocalis Depression between lamina of thyroid cartilage
Vocal ligament and vocal process of arytenoid cartilage
Recurrent laryngeal
Relaxes posterior vocal ligament, tenses anterior part

Cricothyroid Anterolateral part of cricoid
Inferior margin and horn of thyroid cartilage
External laryngeal
Tenses vocal fold
Blood supply
Arterial supply is via the laryngeal arteries, branches of the superior and inferior thyroid arteries. The superior laryngeal artery
is closely related to the internal laryngeal nerve. The inferior laryngeal artery is related to the inferior laryngeal nerve. Venous
drainage is via superior and inferior laryngeal veins, the former draining into the superior thyroid vein and the latter draining
into the middle thyroid vein, or thyroid venous plexus.
Lymphatic drainage
The vocal cords have no lymphatic drainage and this site acts as a lymphatic watershed.
Supraglottic part Upper deep cervical nodes
Subglottic part Prelaryngeal and pretracheal nodes and inferior deep cervical nodes
The aryepiglottic fold and vestibular folds have a dense plexus of lymphatics associated with them and malignancies at these
sites have a greater propensity for nodal metastasis.
Topography of the larynx
Image sourced from Wikipedia
Question 1 of 248
Next
A 28 year old man has sustained a non salvageable testicular injury to his left testicle. The surgeon decides to perform an
orchidectomy and divides the left testicular artery. From which of the following does this vessel originate?
A. Abdominal aorta

B. Internal iliac artery
C. Inferior epigastric artery
D. Inferior vesical artery
E. External iliac artery
Next question
The testicular artery is a branch of the abdominal aorta.
Scrotal and testicular anatomy
Spermatic cord
Formed by the vas deferens and is covered by the following structures:
Layer Origin
Internal spermatic fascia Transversalis fascia
Cremasteric fascia From the fascial coverings of internal oblique
External spermatic fascia External oblique aponeurosis
Contents of the cord
Vas deferens Transmits sperm and accessory gland secretions
Testicular artery Branch of abdominal aorta supplies testis and epididymis
Artery of vas deferens Arises from inferior vesical artery
Cremasteric artery Arises from inferior epigastric artery
Pampiniform plexus Venous plexus, drains into right or left testicular vein
Sympathetic nerve fibres Lie on arteries, the parasympathetic fibres lie on the vas
Genital branch of the genitofemoral nerve Supplies cremaster
Lymphatic vessels Drain to lumbar and para-aortic nodes
Scrotum
• Composed of skin and closely attached dartos fascia.

• Arterial supply from the anterior and posterior scrotal arteries
• Lymphatic drainage to the inguinal lymph nodes
• Parietal layer of the tunica vaginalis is the innermost layer
Testes
• The testes are surrounded by the tunica vaginalis (closed peritoneal sac). The parietal layer of the tunica vaginalis
adjacent to the internal spermatic fascia.
• The testicular arteries arise from the aorta immediately inferiorly to the renal arteries.
• The pampiniform plexus drains into the testicular veins, the left drains into the left renal vein and the right into the
inferior vena cava.
• Lymphatic drainage is to the para-aortic nodes.
Previous
Question 2 of 248
Next
During a carotid endarterectomy the internal carotid artery is cross clamped. Assuming that no shunt is inserted, which of the
following vessels will not have diminished or absent flow as a result?
A. Anterior cerebral artery
B. Ophthalmic artery
C. Middle cerebral artery
D. Maxillary artery
E. None of the above
Next question
Mnemonic for branches of the cerebral portion of the internal carotid artery 'Only Press Carotid Arteries Momentarily'
Only = Opthalmic
Press = Posterior communicating
Carotid = Choroidal
Arteries = Anterior cerebral
Momentarily = Middle cerebral
The maxillary artery is a branch of the external carotid artery.
Internal carotid artery
The internal carotid artery is formed from the common carotid opposite the upper border of the thyroid cartilage. It extends

superiorly to enter the skull via the carotid canal. From the carotid canal it then passes through the cavernous sinus, above
which it divides into the anterior and middle cerebral arteries.
Relations in the neck
Posterior • Longus capitis • Pre-vertebral fascia • Sympathetic chain • Superior laryngeal nerve
Medially • External carotid (near origin) • Wall of pharynx • Ascending pharyngeal artery
Laterally • Internal jugular vein (moves posteriorly at entrance to skull) • Vagus nerve (most posterolaterally)
Anteriorly • Sternocleidomastoid • Lingual and facial veins • Hypoglossal nerve
Relations in the carotid canal
• Internal carotid plexus
• Cochlea and middle ear cavity
• Trigeminal ganglion (superiorly)
• Leaves canal lies above the foramen lacerum
Path and relations in the cranial cavity
The artery bends sharply forwards in the cavernous sinus, the aducens nerve lies close to its inferolateral aspect. The
oculomotor, trochlear, opthalmic and, usually, the maxillary nerves lie in the lateral wall of the sinus. Near the superior orbital
fissure it turns posteriorly and passes postero-medially to pierce the roof of the cavernous sinus inferior to the optic nerve. It
then passes between the optic and oculomotor nerves to terminate below the anterior perforated substance by dividing into the
anterior and middle cerebral arteries.
Branches
• Anterior and middle cerebral artery
• Ophthalmic artery
• Posterior communicating artery
• Anterior choroid artery
• Meningeal arteries

• Hypophyseal arteries
Image demonstrating the internal carotid artery and its relationship to the external carotid artery
Image sourced from Wikipedia
Previous
Question 3 of 248
Next
A 72 year old lady with osteoporosis falls and sustains an intracapsular femoral neck fracture. The fracture is completely
displaced. Which of the following vessels is the main contributor to the arterial supply of the femoral head?
A. Deep external pudendal artery
B. Superficial femoral artery
C. External iliac artery
D. Circumflex femoral arteries
E. Superficial external pudendal artery
Next question
Theme from 2010 Exam

The vessels which form the anastomoses around the femoral head are derived from the medial and lateral circumflex femoral
arteries. These are usually derived from the profunda femoris artery.
Hip joint
• Head of femur articulates with acetabulum of the pelvis
• Both covered by articular hyaline cartilage
• The acetabulum forms at the union of the ilium, pubis, and ischium
• The triradiate cartilage (Y-shaped growth plate) separates the pelvic bones
• The acetabulum holds the femoral head by the acetabular labrum
• Normal angle between femoral head and femoral shaft is 130o
Ligaments
• Transverse ligament: joints anterior and posterior ends of the articular cartilage
• Head of femur ligament (ligamentum teres): acetabular notch to the fovea. Contains arterial supply to head of femur in
children.
Image sourced from Wikipedia

Image sourced from Wikipedia
Extracapsular ligaments
• Iliofemoral ligament: inverted Y shape. Anterior iliac spine to the trochanteric line
• Pubofemoral ligament: acetabulum to lesser trochanter
• Ischiofemoral ligament: posterior support. Ischium to greater trochanter.
Blood supply
Medial circumflex femoral and lateral circumflex femoral arteries (Branches of profunda femoris)
2 anastomoses: Cruciate and the trochanteric anastomoses (provides most of the blood to the head of the femur) Hence the need
for hemiarthroplasty when there is a displaced femoral head fracture. These anastomoses exist between the femoral artery or
profunda femoris and the gluteal vessels.
Previous
Question 4 of 248
Next
A 21 year old man is hit with a hammer and sustains a depressed skull fracture at the vertex. Which of the following sinuses is
at risk in this injury?
A. Superior sagittal sinus
B. Inferior petrosal sinus
C. Transverse sinus

D. Inferior sagittal sinus
E. Straight sinus
Next question
Theme in September 2011 Exam
The superior sagittal sinus is at greatest risk in this pattern of injury. This sinus begins at the front of the crista galli and courses
backwards along the falx cerebri. It becomes continuous with the right transverse sinus near the internal occipital protuberance.
Cranial venous sinuses
The cranial venous sinuses are located within the dura mater. They have no valves which is important in the potential for
spreading sepsis. They eventually drain into the internal jugular vein.
They are:
Superior sagittal sinus
Inferior sagittal sinus
Straight sinus
Transverse sinus
Sigmoid sinus
Confluence of sinuses
Occipital sinus
Cavernous sinus
Topography of cranial venous sinuses
Image s

Previous
Question 5 of 248
Next
A 44 year old man is stabbed in the back and the left kidney is injured. A haematoma forms, which of the following fascial
structures will contain the haematoma?
A. Waldeyers fascia
B. Sibsons fascia
C. Bucks fascia
D. Gerotas fascia
E. Denonvilliers fascia
Next question
Waldeyers fascia- Posterior ano-rectum
Sibsons fascia- Lung apex
Bucks fascia- Base of penis
Gerotas fascia- Surrounding kidney
Denonvilliers fascia- Between rectum and prostate
Renal anatomy
Each kidney is about 11cm long, 5cm wide and 3cm thick. They are located in a deep gutter alongside the projecting verterbral
bodies, on the anterior surface of psoas major. In most cases the left kidney lies approximately 1.5cm higher than the right. The
upper pole of both kidneys approximates with the 11th rib (beware pneumothorax during nephrectomy). On the left hand side
the hilum is located at the L1 vertebral level and the right kidney at level L1-2. The lower border of the kidneys is usually
alongside L3.
The table below shows the anatomical relations of the kidneys:
Relations
Relations Right Kidney Left Kidney
Posterior Quadratus lumborum, diaphragm, psoas major, transversus abdominis
Quadratus lumborum, diaphragm, psoas major, transversus abdominis
Anterior Hepatic flexure of colon Stomach, Pancreatic tail
Superior Liver, adrenal gland Spleen, adrenal gland
Fascial covering
Each kidney and suprarenal gland is enclosed within a common and layer of investing fascia that is derived from the
transversalis fascia into anterior and posterior layers (Gerotas fascia).
Renal structure
Kidneys are surrounded by an outer cortex and an inner medulla which usually contains between 6 and 10 pyramidal structures.
The papilla marks the innermost apex of these. They terminate at the renal pelvis, into the ureter.
Lying in a hollow within the kidney is the renal sinus. This contains:
1. Branches of the renal artery
2. Tributaries of the renal vein
3. Major and minor calyces's
4. Fat
Structures at the renal hilum
The renal vein lies most anteriorly, then renal artery (it is an end artery) and the ureter lies most posterior.
Previous
Question 6 of 248
Next
A baby is found to have a Klumpke's palsy post delivery. Which of the following is most likely to be present?
A. Loss of flexors of the wrist
B. Weak elbow flexion
C. Pronation of the forearm
D. Adducted shoulder
E. Shoulder medially rotated
Next question
Features of Klumpkes Paralysis
• Claw hand (MCP joints extended and IP joints flexed)
• Loss of sensation over medial aspect of forearm and hand
• Horner's syndrome
• Loss of flexors of the wrist
A C8, T1 root lesion is called Klumpke's paralysis and is caused by delivery with the arm extended.
Brachial plexus
Origin Anterior rami of C5 to T1
Sections of the plexus • Roots, trunks, divisions, cords, branches

• Mnemonic:Real Teenagers Drink Cold Beer
Roots • Located in the posterior triangle • Pass between scalenus anterior and medius
Trunks • Located posterior to middle third of clavicle • Upper and middle trunks related superiorly to the subclavian artery • Lower trunk passes over 1st rib posterior to the subclavian artery
Divisions Apex of axilla
Cords Related to axillary artery
Diagram illustrating the branches of the brachial plexus
Image sourced from Wikipedia
Previous
Question 7 of 248
Next
A 22 year old man undergoes a superficial parotidectomy for a pleomorphic adenoma. The operation does not proceed well and
a diathermy malfunction results in division of the buccal branch of the facial nerve. Which of the following muscles will not
demonstrate impaired function as a result?
A. Zygomaticus minor

B. Mentalis
C. Buccinator
D. Levator anguli oris
E. Risorius
Next question
Buccal branch supplies
Zygomaticus minor Elevates upper lip
Risorius Aids smile
Buccinator
Pulls corner of mouth backward and compresses cheek
Levator anguli oris Pulls angles of mouth upward and toward midline
Orbicularis Closes and tightens lips together
Nasalis Flares nostrils and compresses nostrils
Facial nerve
The facial nerve is the main nerve supplying the structures of the second embryonic branchial arch. It is predominantly an
efferent nerve to the muscles of facial expression, digastric muscle and also to many glandular structures. It contains a few
afferent fibres which originate in the cells of its genicular ganglion and are concerned with taste.
Supply - 'face, ear, taste, tear'
• Face: muscles of facial expression
• Ear: nerve to stapedius
• Taste: supplies anterior two-thirds of tongue
• Tear: parasympathetic fibres to lacrimal glands, also salivary glands
Path
Subarachnoid path
• Origin: motor- pons, sensory- nervus intermedius
• Pass through the petrous temporal bone into the internal auditory meatus with the vestibulocochlear nerve. Here they
combine to become the facial nerve.

Facial canal path
• The canal passes superior to the vestibule of the inner ear
• At the medial aspect of the middle ear, it becomes wider and contains the geniculate ganglion.
- 3 branches:
1. greater petrosal nerve
2. nerve to stapedius
3. chorda tympani
Stylomastoid foramen
• Passes through the stylomastoid foramen (tympanic cavity anterior and mastoid antrum posteriorly)
• Posterior auricular nerve and branch to Posterior belly of Digastric and Stylohyoid muscle
Face
Enters parotid gland and divides into 5 branches:
• Temporal branch
• Zygomatic branch
• Buccal branch
• Marginal mandibular branch
• Cervical branch
Previous
Question 8 of 248
Next
At which of the following vertebral body levels does the common carotid artery typically bifurcate into the external and internal
carotid arteries?
A. C4
B. C2
C. C1
D. C6
E. C7
Next question
It terminates at the upper border of the thyroid cartilege, Which is usually located at C4.
Common carotid artery

The right common carotid artery arises at the bifurcation of the brachiocephalic trunk, the left common carotid arises from the
arch of the aorta. Both terminate at the level of the upper border of the thyroid cartilage (the lower border of the third cervical
vertebra) by dividing into the internal and external carotid arteries.
Left common carotid artery
This vessel arises immediately to the left and slightly behind the origin of the brachiocephalic trunk. Its thoracic portion is 2.5-
3.5 cm in length and runs superolaterally to the sternoclavicular joint.
In the thorax
The vessel is in contact, from below upwards, with the trachea, left recurrent laryngeal nerve, left margin of the oesophagus.
Anteriorly the left brachiocephalic vein runs across the artery, and the cardiac branches from the left vagus descend in front of
it. These structures together with the thymus and the anterior margins of the left lung and pleura separate the artery from the
manubrium.
In the neck
The artery runs superiorly deep to sternocleidomastoid and then enters the anterior triangle. At this point it lies within the
carotid sheath with the vagus nerve and the internal jugular vein. Posteriorly the sympathetic trunk lies between the vessel and
the prevertebral fascia. At the level of C7 the vertebral artery and thoracic duct lie behind it. The anterior tubercle of C6
transverse process is prominent and the artery can be compressed against this structure (it corresponds to the level of the
cricoid).
Anteriorly at C6 the omohyoid muscle passes superficial to the artery.
Within the carotid sheath the jugular vein lies lateral to the artery.
Right common carotid artery
The right common carotid arises from the brachiocephalic artery. The right common carotid artery corresponds with the cervical
portion of the left common carotid, except that there is no thoracic duct on the right. The oesophagus is less closely related to
the right carotid than the left.
Summary points about the carotid anatomy
Path
Passes behind the sternoclavicular joint (12% patients above this level) to the upper border of the thyroid cartilage, to divide
into the external (ECA) and internal carotid arteries (ICA).
Relations
• Level of 6th cervical vertebra crossed by omohyoid
• Then passes deep to the thyrohyoid, sternohyoid, sternomastoid muscles.
• Passes anterior to the carotid tubercle (transverse process 6th cervical vertebra)-NB compression here stops
haemorrhage.
• The inferior thyroid artery passes posterior to the common carotid artery.
• Then : Left common carotid artery crossed by thoracic duct, Right common carotid artery crossed by recurrent
laryngeal nerve

Previous
Question 9 of 248
Next
A man is stabbed in the chest to the right of the manubriosternal angle. Which structure is least likely to be injured in this case?
A. Aortic arch
B. The trachea
C. Right phrenic nerve
D. Right recurrent laryngeal nerve
E. Brachiocephalic vein
Next question
The right recurrent laryngeal nerve branches off the right vagus more proximally and arches posteriorly round the subclavian
artery. So of the structures given it is the least likely to be injured.
Mediastinum
Region between the pulmonary cavities.
It is covered by the mediastinal pleura. It does not contain the lungs.
It extends from the thoracic inlet superiorly to the diaphragm inferiorly.
Mediastinal regions
• Superior mediastinum
• Inferior mediastinum
• Posterior mediastinum
• Anterior mediastinum
Region Contents
Superior mediastinum • Superior vena cava • Brachiocephalic veins • Arch of aorta • Thoracic duct • Trachea • Oesophagus • Thymus • Vagus nerve • Left recurrent laryngeal nerve • Phrenic nerve

Anterior mediastinum • Thymic remnants • Lymph nodes • Fat
Middle mediastinum • Pericardium • Heart • Aortic root • Arch of azygos vein • Main bronchi
Posterior mediastinum • Oesophagus • Thoracic aorta • Azygos vein • Thoracic duct • Vagus nerve • Sympathetic nerve trunks • Splanchnic nerves
Previous
Question 10 of 248
Next
An 18 year old man is stabbed in the neck and has to undergo repair of a laceration to the internal carotid artery. Post
operatively he is noted to have a Horners syndrome. Which of the following will not be present?
A. Apparent enopthalmos
B. Loss of sweating on the entire ipsilateral side of the face
C. Constricted pupil
D. Mild ptosis
E. Normal sympathetic activity in the torso
Next question
The anhidrosis will be mild as this is a distal lesion and at worst only a very limited area of the ipsilateral face will be
anhidrotic.
Horners syndrome
Horners syndrome, clinical features:
• Ptosis
• Miosis
• Enopthalmos
• Anhydrosis

Primarily a disorder of the sympathetic nervous system. Extent of symptoms depends upon the anatomical site of the lesion.
Proximal lesions occur along the hypothalamospinal tract
Distal lesions are usually post ganglionic e.g. at level of internal carotid artery or beyond.
In contrast to a 3rd nerve palsy the ptosis is more mild and the pupil constricted rather than dilated.
Previous
Question 11 of 248
Next
Which of the following types of epithelium lines the lumenal surface of the normal oesophagus?
A. Non keratinised stratified squamous epithelium
B. Ciliated columnar epithelium
C. Keratinised stratified squamous epithelium
D. Non ciliated columnar epithelium
E. None of the above
Next question
The oesphagus is lined by non keratinised stratified squamous epithelium. Changes to glandular type epithelium occur as part of
metaplastic processes in reflux.
Oesophagus
• 25cm long
• Starts at C6 vertebra, pierces diaphragm at T10 and ends at T11
• Squamous epithelium
Constrictions of the oesophagus
Structure Distance from incisors
Cricoid cartilage 15cm
Arch of the Aorta 22.5cm
Left principal bronchus 27cm
Diaphragmatic hiatus 40cm

Relations
Anteriorly • Trachea to T4 • Recurrent laryngeal nerve • Left bronchus, Left atrium • Diaphragm
Posteriorly • Thoracic duct to left at T5 • Hemiazygos to the left T8 • Descending aorta • First 2 intercostal branches of aorta
Left • Thoracic duct • Left subclavian artery
Right • Azygos vein
Arterial, venous and lymphatic drainage of the oesophagus
Artery Vein Lymphatics Muscularis externa
Upper third Inferior thyroid Inferior thyroid Deep cervical Striated muscle
Mid third Aortic branches Azygos branches Mediastinal Smooth & striated muscle
Lower third Left gastric Posterior mediastinal and coeliac Gastric Smooth muscle
Nerve supply
• Upper half is supplied by recurrent laryngeal nerve
• Lower half by oesophageal plexus (vagus)
Histology
• Mucosa :Nonkeratinized stratified squamous epithelium
• Submucosa: glandular tissue
• Muscularis externa (muscularis): composition varies. See table
• Adventitia
Previous
Question 12 of 248
Next

A 23 year old man is stabbed in the neck, in the region between the omohyoid and digastric muscles, the injury is explored
surgically. At operation a nerve injury is identified immediately superior to the lingual artery as is branches off the external
carotid artery. Which of the following is the most likely result of this injury?
A. Paralysis of the ipsilateral side of the tongue
B. Abduction of the ipsilateral vocal cord
C. Winging of the scapula
D. Paralysis of the ipsilateral hemi diaphragm
E. Inability to abduct the shoulder
Next question
The hypoglossal nerve runs anterior to the external carotid, above the lingual arterial branch. If damaged then ipsilateral
paralysis of the genioglossus, hyoglossus and styloglossus muscles will occur. If the patient is asked to protrude their tongue
then it will tend to point to the affected side.
Anterior triangle of the neck
Boundaries
Anterior border of the Sternocleidomastoid Lower border of mandible Anterior midline
Sub triangles (divided by Digastric above and Omohyoid)
• Muscular triangle: Neck strap muscles
• Carotid triangle: Carotid sheath
• Submandibular Triangle (digastric)
Contents of the anterior triangle
Digastric triangle Submandibular gland Submandibular nodes Facial vessels Hypoglossal nerve
Muscular triangle Strap muscles External jugular vein
Carotid triangle Carotid sheath (Common carotid, vagus and internal jugular vein)

Ansa cervicalis
Nerve supply to digastric muscle
• Anterior: Mylohyoid nerve
• Posterior: Facial nerve
Image sourced from Wikipedia
Previous
Question 13 of 248
Next
Which of the following structures is not directly related to the right adrenal gland?
A. Diaphragm posteriorly
B. Bare area of the liver anteriorly
C. Right renal vein
D. Inferior vena cava
E. Hepato-renal pouch
Next question
The right renal vein is very short and lies more inferiorly.
Adrenal gland anatomy
Anatomy
Location Superomedially to the upper pole of each kidney

Relationships of the right adrenal
Diaphragm-Posteriorly, Kidney-Inferiorly, Vena Cava-Medially, Hepato-renal pouch and bare area of the liver-Anteriorly
Relationships of the left adrenal
Crus of the diaphragm-Postero- medially, Pancreas and splenic vessels-Inferiorly, Lesser sac and stomach-Anteriorly
Arterial supply
Superior adrenal arteries- from inferior phrenic artery, Middle adrenal arteries - from aorta, Inferior adrenal arteries -from renal arteries
Venous drainage of the right adrenal
Via one central vein directly into the IVC
Venous drainage of the left adrenal
Via one central vein into the left renal vein
Previous
Question 14 of 248
Next
With respect to the basilic vein, which statement is false?
A. Its deep anatomical location makes it unsuitable for use as an arteriovenous
access site in fistula surgery
B. It originates from the dorsal venous network on the hand
C. It travels up the medial aspect of the forearm
D. Halfway between the shoulder and the elbow it lies deep to muscle
E. It joins the brachial vein to form the axillary vein
Next question
It is used in arteriovenous fistula surgery during a procedure known as a basilic vein transposition.
Basilic vein
The basilic and cephalic veins both provide the main pathways of venous drainage for the arm and hand. It is continuous with
the palmar venous arch distally and the axillary vein proximally.
Path
• Originates on the medial side of the dorsal venous network of the hand, and passes up the forearm and arm.
• Most of its course is superficial.
• Near the region anterior to the cubital fossa the vein joins the cephalic vein.
• Midway up the humerus the basilic vein passes deep under the muscles.
• At the lower border of the teres major muscle, the anterior and posterior circumflex humeral veins feed into it.
• Joins the brachial veins to form the axillary vein.

Previous
Question 15 of 248
Next
Mobilisation of the left lobe of the liver will facilitate surgical access to which of the following?
A. Abdominal oesophagus
B. Duodenum
C. Right colic flexure
D. Right kidney
E. Pylorus of stomach
Next question
The fundus of the stomach is a posterior relation. The pylorus lies more inferolaterally. During a total gastrectomy division of
the ligaments holding the left lobe of the liver will facilitate access to the proximal stomach and abdominal oesophagus. This
manoeuvre is seldom beneficial during a distal gastrectomy.
Liver
Structure of the liver
Right lobe • Supplied by right hepatic artery • Contains Couinard segments V to VIII (-/+Sg I)
Left lobe • Supplied by the left hepatic artery • Contains Couinard segments II to IV (+/- Sg1)
Quadrate lobe • Part of the right lobe anatomically, functionally is part of the left • Couinard segment IV • Porta hepatis lies behind • On the right lies the gallbladder fossa • On the left lies the fossa for the umbilical vein
Caudate lobe • Supplied by both right and left hepatic arteries • Couinard segment I • Lies behind the plane of the porta hepatis • Anterior and lateral to the inferior vena cava • Bile from the caudate lobe drains into both right and left hepatic ducts
Detailed knowledge of Couinard segments is not required for MRCS Part A

• Between the liver lobules are portal canals which contain the portal triad: Hepatic Artery, Portal Vein, tributary of Bile
Duct.
Relations of the liver
Anterior Postero inferiorly
Diaphragm Oesophagus
Xiphoid process Stomach
Duodenum
Hepatic flexure of colon
Right kidney
Gallbladder
Inferior vena cava
Porta hepatis
Location Postero inferior surface, it joins nearly at right angles with the left sagittal fossa, and separates the caudate lobe behind from the quadrate lobe in front
Transmits • Common hepatic duct • Hepatic artery • Portal vein • Sympathetic and parasympathetic nerve fibres • Lymphatic drainage of the liver (and nodes)
Ligaments
Falciform ligament • 2 layer fold peritoneum from the umbilicus to anterior liver surface • Contains ligamentum teres (remnant umbilical vein) • On superior liver surface it splits into the coronary and left triangular ligaments
Ligamentum teres Joins the left branch of the portal vein in the porta hepatis
Ligamentum venosum Remnant of ductus venosus

Arterial supply
• Hepatic artery
Venous
• Hepatic veins
• Portal vein
Nervous supply
• Sympathetic and parasympathetic trunks of coeliac plexus
Previous
Question 16 of 248
Next
The following statements relating to the ankle joint are true except?
A. Three groups of ligaments provide mechanical stability
B. The sural nerve lies medial to the Achilles tendon at its point of insertion
C. Eversion of the foot occurs at the sub talar joint
D. The flexor hallucis longus tendon is the most posterior structure at the medial malleolus
E. The saphenous nerve crosses the ankle joint.
Next question
The sural nerve lies behind the distal fibula. Inversion and eversion are sub talar movements. The structures passing behind the
medial malleolus from anterior to posterior include: tibialis posterior, flexor digitorum longus, posterior tibia vein, posterior
tibial artery, nerve, flexor hallucis longus.
Ankle joint
The ankle joint is a synovial joint composed of the tibia and fibula superiorly and the talus inferiorly.
Ligaments of the ankle joint
• Deltoid ligament (medially)
• Lateral collateral ligament
• Talofibular ligaments (both anteriorly and posteriorly)

The calcaneofibular ligament is separate from the fibrous capsule of the joint. The two talofibular ligaments are fused with it.
The components of the syndesmosis are
• Antero-inferior talofibular ligament
• Postero-inferior talofibular ligament
• Inferior transverse talofibular ligament
• Interosseous ligament
Movements at the ankle joint
• Plantar flexion (55 degrees)
• Dorsiflexion (35 degrees)
• Inversion and eversion movements occur at the level of the sub talar joint
Nerve supply
Branches of deep peroneal and tibial nerves.
Previous
Question 17 of 248
Next
A 78 year old man is lifting a heavy object when a feels a pain in his forearm and is unable to continue. He has a swelling over
his upper forearm. An MRI scan shows a small cuff of tendon still attached to the radial tuberosity consistent with a recent tear.
Which of the following muscles has been injured?
A. Pronator teres
B. Supinator
C. Aconeus
D. Brachioradialis
E. Biceps brachii
Next question
Biceps inserts into the radial tuberosity. Distal injuries of this muscle are rare but are reported and are clinically more important
than more proximal ruptures.
Radius
• Bone of the forearm extending from the lateral side of the elbow to the thumb side of the wrist

Upper end
• Articular cartilage- covers medial > lateral side
• Articulates with radial notch of the ulna by the annular ligament
• Muscle attachment- biceps brachii at the tuberosity
Shaft
• Muscle attachment-
Upper third of the body Supinator, Flexor digitorum superficialis, Flexor pollicis longus
Middle third of the body Pronator teres
Lower quarter of the body Pronator quadratus , tendon of supinator longus
Lower end
• Quadrilateral
• Anterior surface- capsule of wrist joint
• Medial surface- head of ulna
• Lateral surface- ends in the styloid process
• Posterior surface: 3 grooves containing:
1. Tendons of extensor carpi radialis longus and brevis
2. Tendon of extensor pollicis longus
3. Tendon of extensor indicis

Image sourced from Wikipedia
Previous
Question 18 of 248
Next
The oesophagus is constricted at the following levels apart from:
A. Cricoid cartilage
B. Arch of the aorta
C. Lower oesophageal sphincter
D. Left main stem bronchus
E. Diaphragmatic hiatus

Next question
The oesophagus is not constricted at the level of the lower oesophageal sphincter.
Previous
Question 19 of 248
Next
A 19 year old man is playing rugby when he suddenly notices a severe pain at the posterolateral aspect of his right thigh. Which of the following muscle groups is most likely to have been injured?
A. Semimembranosus
B. Semitendinosus
C. Long head of biceps femoris
D. Gastrocnemius
E. Soleus
Next question Theme from April 2012 Exam The biceps femoris is the laterally located hamstring muscle. The semitendinosus and semimembranosus are located medially. Rupture of gastrocnemius and soleus may occur but is less common.
Biceps femoris The biceps femoris is one of the hamstring group of muscles located in the posterior upper thigh. It has two heads. Long head
Origin Ischial tuberosity
Insertion Fibular head
Action Knee flexion, lateral rotation tibia, extension hip
Innervation Tibial nerve (L5, S1, S2)
Arterial supply Profunda femoris artery, inferior gluteal artery, and the superior muscular branches of popliteal artery
Image demonstrating the biceps femoris muscle, with the long head outlined

Image sourced from Wikipedia
Short head
Origin Lateral lip of linea aspera, lateral supracondylar ridge of femur
Insertion Fibular head
Action Knee flexion, lateral rotation tibia
Innervation Common peroneal nerve (L5, S1, S2)
Arterial supply Profunda femoris artery, inferior gluteal artery, and the superior muscular branches of popliteal artery
Previous
Question 20 of 248
Next
Which of the following is a branch of the third part of the axillary artery?
A. Superior thoracic
B. Lateral thoracic
C. Dorsal scapular
D. Thoracoacromial
E. Posterior circumflex humeral
Next question
The other branches include:
• Subscapular
• Anterior circumflex humeral
Axilla
Boundaries of the axilla
Medially Chest wall and Serratus anterior
Laterally Humeral head
Floor Subscapularis
Anterior aspect Lateral border of Pectoralis major
Fascia Clavipectoral fascia
Content:
Long thoracic nerve (of Bell)
Derived from C5-C7 and passes behind the brachial plexus to enter the axilla. It lies on the medial chest wall and supplies serratus anterior. Its location puts it at risk during axillary surgery and damage will lead to winging of the scapula.
Thoracodorsal nerve and thoracodorsal trunk
Innervate and vascularise latissimus dorsi.
Axillary vein Lies at the apex of the axilla, it is the continuation of the basilic vein. Becomes the subclavian vein at the outer border of the first rib.
Intercostobrachial nerves Traverse the axillary lymph nodes and are often divided during axillary surgery. They provide cutaneous sensation to the axillary skin.
Lymph nodes The axilla is the main site of lymphatic drainage for the breast.
Previous
Question 21 of 248
Next
Which of the following structures separates the intervertebral disks from the spinal cord?
A. Anterior longitudinal ligament
B. Posterior longitudinal ligament
C. Supraspinous ligament

D. Interspinous ligament
E. Ligamentum flavum
Next question
The posterior longitudinal ligament overlies the posterior aspect of the vertebral bodies. It also overlies the posterior aspect of
the intervertebral disks.
Intervertebral discs
• Consist of an outer annulus fibrosus and an inner nucleus pulposus.
• The anulus fibrosus consists of several layers of fibrocartilage.
• The nucleus pulposus contains loose fibres suspended in a mucoprotein gel with the consistency of jelly. The nucleus
of the disc acts as a shock absorber.
• Pressure on the disc causes posterior protrusion of the nucleus pulposus. Most commonly in the lumbrosacral and lower
cervical areas.
• The discs are separated by hyaline cartilage.
• There is one disc between each pair of vertebrae, except for C1/2 and the sacrococcygeal vertebrae.
Previous
Question 22 of 248
Next
At what level does the aorta bifurcate into the left and right common iliac arteries?
A. L1
B. L2
C. L3
D. L4
E. L5
Next question
The aorta typically bifurcates at L4. This level is usually fairly constant and is often tested in the exam.
Levels
Transpyloric plane
Level of the body of L1
• Pylorus stomach
• Left kidney hilum (L1- left one!)
• Right hilum of the kidney (1.5cm lower than the left)

• Fundus of the gallbladder
• Neck of pancreas
• Duodenojejunal flexure
• Superior mesenteric artery
• Portal vein
• Left and right colic flexure
• Root of the transverse mesocolon
• 2nd part of the duodenum
• Upper part of conus medullaris
• Spleen
Can be identified by asking the supine patient to sit up without using their arms. The plane is located where the lateral border of
the rectus muscle crosses the costal margin.
Anatomical planes
Subcostal plane Lowest margin of 10th costal cartilage
Intercristal plane Level of body L4 (highest point of iliac crest)
Intertubercular plane Level of body L5
Common level landmarks
Inferior mesenteric artery L3
Bifurcation of aorta into common iliac arteries L4
Formation of IVC L5 (union of common iliac veins)
Diaphragm apertures • Vena cava T8 • Oesophagus T10 • Aortic hiatus T12
Previous
Question 23 of 248
Next
A 23 year old man is due to undergo a mitral valve repair for mitral regurgitation. Which of the following is a feature of the
mitral valve?
A. Its closure is marked by the first heart sound
B. It has two anterior cusps
C. The chordae tendinae attach to the anterior cusps only

D. The chordae tendinae anchor the valve directly to the wall of the left ventricle
E. It is best auscultated in the left third interspace
Next question
The mitral valve is best auscultated over the cardiac apex, where its closure marks the first heart sound. It has only two cusps.
These are attached to chordae tendinae which themselves are linked to the wall of the ventricle by the papillary muscles.
Heart anatomy
The walls of each cardiac chamber comprise:
• Epicardium
• Myocardium
• Endocardium
Cardiac muscle is attached to the cardiac fibrous skeleton.
Relations
The heart and roots of the great vessels within the pericardial sac are related anteriorly to the sternum, medial ends of the 3rd to
5th ribs on the left and their associated costal cartilages. The heart and pericardial sac are situated obliquely two thirds to the left
and one third to the right of the median plane.
The pulmonary valve lies at the level of the left third costal cartilage.
The mitral valve lies at the level of the fourth costal cartilage.
Coronary sinus
This lies in the posterior part of the coronary groove and receives blood from the cardiac veins. The great cardiac vein lies at its
left and the middle and small cardiac veins lie on its right. The smallest cardiac veins drain into the atria directly.
Aortic sinus
Right coronary artery arises from the right aortic sinus, the left is derived from the left aortic sinus and no vessel emerges from
the posterior sinus.
Right and left ventricles
Structure Left Ventricle
A-V Valve Mitral (double leaflet)
Walls Twice as thick as right
Trabeculae carnae Much thicker and more numerous

Right coronary artery
The RCA supplies:
• Right atrium
• Diaphragmatic part of the left ventricle
• Usually the posterior third of the interventricular septum
• The sino atrial node (60% cases)
• The atrio ventricular node (80% cases)
Left coronary artery
The LCA supplies:
• Left atrium
• Most of left ventricle
• Part of the right ventricle
• Anterior two thirds of the inter ventricular septum
• The sino atrial node (remaining 40% cases)
Innervation of the heart
Autonomic nerve fibres from the superficial and deep cardiac plexus. These lie anterior to the bifurcation of the trachea,
posterior to the ascending aorta and superior to the bifurcation of the pulmonary trunk. The parasympathetic supply to the heart
is from presynaptic fibres of the vagus nerves.
Valves of the heart
Mitral valve Aortic valve Pulmonary valve Tricuspid valve
2 cusps 3 cusps 3 cusps 3 cusps
First heart sound Second heart sound Second heart sound First heart sound
1 anterior cusp 1 anterior cusp 2 anterior cusps 2 anterior cusps
Attached to chordae tendinae No chordae No chordae Attached to chordae tendinae
Previous 2 / 3 Question 24-26 of 248
Next
Theme: Nerve lesions
A. Intercostobrachial
B. Median
C. Axillary
D. Radial

E. Ulnar
F. Musculocutaneous
G. Brachial plexus upper cord
H. Brachial plexus lower cord
Please select the most likely nerve injury for the scenarios given. Each option may be used once, more than once or not at all.
24. A 23 year old rugby player sustains a Smiths Fracture. On examination opposition of the thumb is markedly weakened.
Median This high velocity injury can often produce significant angulation and displacement. Both of these may impair the function of the median nerve with loss of function of the muscles of the thenar eminence
25. A 45 year old lady recovering from a mastectomy and axillary node clearance notices that sensation in her armpit is impaired.
Intercostobrachial The intercostobrachial nerves are frequently injured during axillary dissection. These nerves traverse the axilla and supply cutaneous sensation.
26. An 8 year old boy falls onto an outstretched hand and sustains a supracondylar fracture. In addition to a weak radial pulse the child is noted to have loss of pronation of the affected hand.
You answered Ulnar The correct answer is Median This is a common injury in children. In this case the angulation and displacement have resulted in median nerve injury.
Previous
Question 27 of 248
Next
A 23 year old lady with sialolithiasis of the submandibular gland is undergoing excision of the gland. Which of the following
nerves is at risk as the duct is mobilised?
A. Lingual nerve
B. Buccal nerve
C. Facial nerve

D. Glossopharyngeal
E. Vagus
Next question
The lingual nerve wraps around Whartons duct. The lingual nerve provides sensory supply to the anterior 2/3 of the tongue.
Submandibular gland
Relations of the submandibular gland
Superficial Platysma, deep fascia and mandible Submandibular lymph nodes Facial vein (facial artery near mandible) Marginal mandibular nerve Cervical branch of the facial nerve
Deep Facial artery (inferior to the mandible) Mylohoid muscle Sub mandibular duct Hyoglossus muscle Lingual nerve Submandibular ganglion Hypoglossal nerve
Submandibular duct (Wharton's duct)
• Opens lateral to the lingual frenulum on the anterior floor of mouth.
• 5 cm length
• Lingual nerve wraps around Wharton's duct. As the duct passes forwards it crosses medial to the nerve to lie above it
and then crosses back, lateral to it, to reach a position below the nerve.
Innervation
• Sympathetic innervation- Superior Cervical ganglion via the Lingual nerve
• Parasympathetic innervation- Submandibular ganglion
Arterial supply
Branch of the Facial artery. The facial artery passes through the gland to groove its deep surface. It then emerges onto the face
by passing between the gland and the mandible.
Venous drainage
Anterior Facial vein (lies deep to the Marginal Mandibular nerve)

Lymphatic drainage
Deep cervical and jugular chains of nodes
Previous
Question 28 of 248
Next
Which of the following is true in connection with the phrenic nerves?
A. They both lie anterior to the hilum of the lungs
B. They are derived from spinal roots C 2,3,4
C. They pierce the diaphragm at the level of T7
D. They consist of motor fibres only
E. None of the above
Next question
C3,4,5
Keeps the diaphragm alive!
They both lie anterior to the hilum of the lung. The phrenic nerves have both motor and sensory functions. For this reason sub
diaphragmatic pathology may cause referred pain to the shoulder.
Phrenic nerve
Origin
• C3,4,5
Supplies
• Diaphragm, sensation central diaphragm and pericardium
Path
• The phrenic nerve passes with the internal jugular vein across scalenus anterior. It passes deep to prevertebral fascia of
deep cervical fascia.
• Left: crosses anterior to the 1st part of the subclavian artery.
• Right: Anterior to scalenus anterior and crosses anterior to the 2nd part of the subclavian artery.
• On both sides, the phrenic nerve runs posterior to the subclavian vein and posterior to the internal thoracic artery as it
enters the thorax.

Right phrenic nerve
• In the superior mediastinum: anterior to right vagus and laterally to superior vena cava
• Middle mediastinum: right of pericardium
• It passes over the right atrium to exit the diaphragm at T8
Left phrenic nerve
• Passes lateral to the left subclavian artery, aortic arch and left ventricle
• Passes anterior to the root of the lung
• Pierces the diaphragm alone
Image showing the passage of the phrenic nerve in the neck
Image sourced from Wikipedia
Previous
Question 29 of 248
Next
A 32 year old man presents with an inguinal hernia and undergoes an open surgical repair. The surgeons decide to place a mesh
on the posterior wall of the inguinal canal to complete the repair, which of the following structures will lie posterior to the
mesh?
A. Transversalis fascia
B. External oblique
C. Rectus abdominis

D. Obturator nerve
E. None of the above
Next question
Inguinal canal walls: 'MALT: 2M, 2A, 2L, 2T':
Starting from superior, moving around in order to posterior:
Superior wall (roof): 2 Muscles:Internal oblique, transversus abdominis
Anterior wall: 2 Aponeuroses: Aponeurosis of external oblique, Aponeurosis of internal oblique
Lower wall (floor): 2 Ligaments: Inguinal Ligament, Lacunar Ligament Posterior wall: 2Ts: Transversalis fascia, Conjoint
Tendon
This is actually quite a straightforward question. It is simply asking for the structure that forms the posterior wall of the inguinal
canal. This is composed of the transversalis fascia, the conjoint tendon and more laterally the deep inguinal ring.
Inguinal canal
Location
• Above the inguinal ligament
• The inguinal canal is 4cm long
Boundaries of the inguinal canal
Floor • External oblique aponeurosis • Inguinal ligament • Lacunar ligament
Roof • Internal oblique • Transversus abdominis
Anterior wall External oblique aponeurosis
Posterior wall • Transversalis fascia • Conjoint tendon
Laterally • Internal ring • Fibres of internal oblique

Medially • External ring • Conjoint tendon
Contents
Males Spermatic cord and ilioinguinal nerve As it passes through the canal the spermatic cord has 3 coverings:
• External spermatic fascia from external oblique aponeurosis
• Cremasteric fascia • Internal spermatic fascia
Females Round ligament of uterus and ilioinguinal nerve
Related anatomy of the inguinal region
The boundaries of Hesselbachs triangle are commonly tested and illustrated below:
Image sourced from Wikipedia
The image below demonstrates the close relationship of the vessels to the lower limb with the inguinal canal. A fact to be borne
in mind when repairing hernial defects in this region.
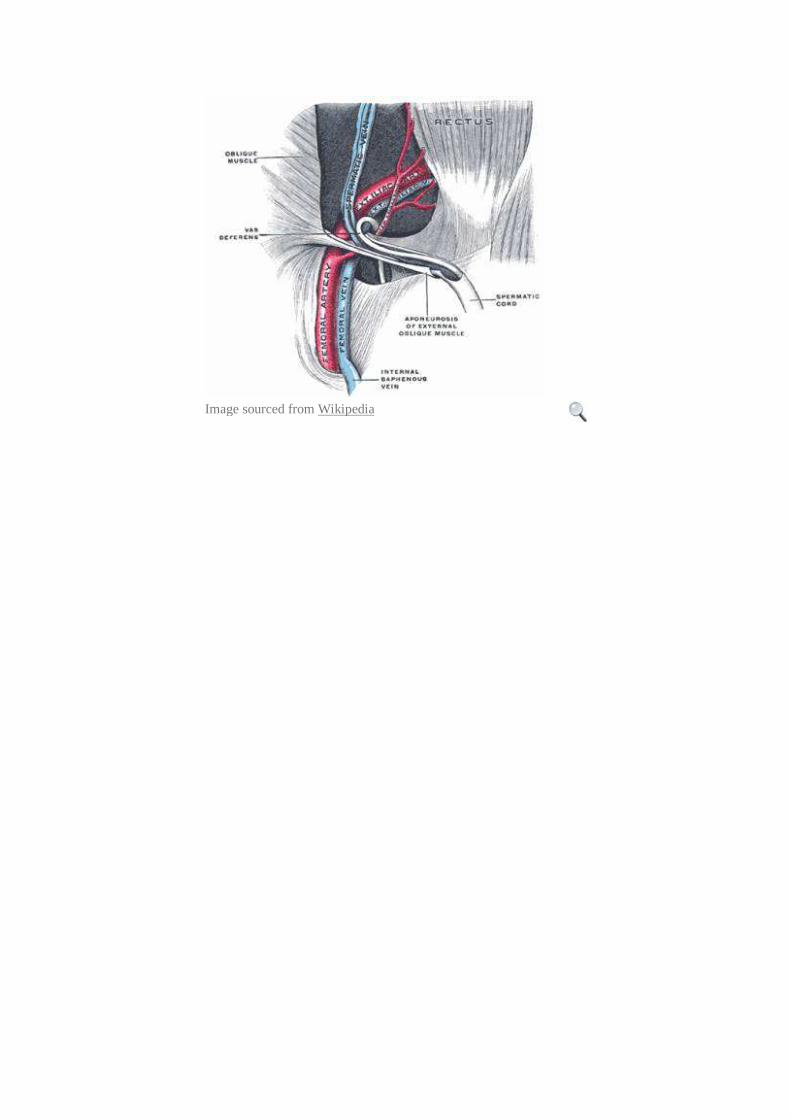
Image sourced from Wikipedia


















