035 Quick Queries Acute Rhinosinusitis
4
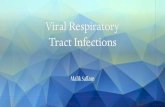
Copyright © Not for Sale or Commercial Distribution Unauthorised use prohibited. Authorised users can download, display, view and print a single copy for personal use S inusitis is more accurately termed rhinosi- nusitis and is defined as an inflammation of the nasal and sinus mucosa, which invariably coexist. Based on signs and symptoms, it is often impossible to distinguish the etiology of rhinosinusitis. Of all rhinosinusitis, only 0.5% to 2% have positive bacterial cultures. 1 The remainder are largely viral rhinosinusitis, other- wise known as the common cold. The diagnostic challenge therefore rests in detecting the small proportion of cases where a bacterial etiology is most likely. These cases may therefore be amenable to treatment with antibiotic therapy. What is the pathophysiology? The concept that the disease primarily involves the osteomeatal complex, which is the area where drainage of the maxillary, anterior ethmoid and frontal sinuses takes place (Figure 1). The pathophysiologic mechanism of sinus disease is related to disruption of one of three factors: • patency of the sinus osium (opening), • the highly regulated mucociliary function and • mucus production. What are the bacteria involved? The bacteria involved in the etiology of acute rhi- nosinusitis in Canada are illustrated in Figure 2. 2 The incidence of penicillin resistance is rising in The Canadian Journal of CME / June 2008 35 QUICK QUERIES Topical Questions, Sound Answers Acute Rhinosinusitis: A Diagnostic and Therapeutic Approach Talal Al-Khatib, MD; and Mark Samaha, MSc, MD, FRCSC Presented at McGill University’s CME Program to General Practitioners Evening Lecture Series, October 2007. Figure 1. CT scan view of osteomeatal complex. Figure 2. Bacterial incidence in acute rhinosinusitis. R hinosinusitis is defined as an inflammation of the nasal and sinus mucosa, which invariably coexist. Streptococcus pneumonia 35% Hemophilus influenza 35% Moraxella Catarrhalis 5% Staphylococcus aureus 2% Anaerobes 7%
-
Upload
rika-fitria -
Category
Documents
-
view
218 -
download
0
description
rhinosinusitis
Transcript of 035 Quick Queries Acute Rhinosinusitis
-
Copyright
Not for Sa
le orComm
ercial Dist
ribution
Unauthoris
ed use pro
hibited. Au
thorised us
ers can do
wnload,
display, vie
w andprint
a single cop
y forperso
nal use
Sinusitis is more accurately termed rhinosi-nusitis and is defined as an inflammation ofthe nasal and sinus mucosa, which invariablycoexist. Based on signs and symptoms, it isoften impossible to distinguish the etiology ofrhinosinusitis. Of all rhinosinusitis, only 0.5%to 2% have positive bacterial cultures.1 Theremainder are largely viral rhinosinusitis, other-wise known as the common cold. The diagnosticchallenge therefore rests in detecting the smallproportion of cases where a bacterial etiology ismost likely. These cases may therefore beamenable to treatment with antibiotic therapy.
What is the pathophysiology?
The concept that the disease primarily involvesthe osteomeatal complex, which is the area wheredrainage of the maxillary, anterior ethmoid andfrontal sinuses takes place (Figure 1).The pathophysiologic mechanism of sinus
disease is related to disruption of one of threefactors: patency of the sinus osium (opening),
the highly regulated mucociliary functionand
mucus production.
What are the bacteriainvolved?
The bacteria involved in the etiology of acute rhi-nosinusitis in Canada are illustrated in Figure 2.2
The incidence of penicillin resistance is rising in
The Canadian Journal of CME / June 2008 35
QUICK QUERIESTopical Questions, Sound Answers
Acute Rhinosinusitis:A Diagnostic and Therapeutic Approach
Talal Al-Khatib, MD; and Mark Samaha, MSc, MD, FRCSCPresented at McGill Universitys CME Program to General Practitioners Evening LectureSeries, October 2007.
Figure 1. CT scan view of osteomeatal complex.
Figure 2. Bacterial incidence in acute rhinosinusitis.
Rhinosinusitis isdefined as aninflammation of the nasaland sinus mucosa, whichinvariably coexist.
INDOMINO
COMFI
DO
Streptococcuspneumonia 35%
Hemophilus influenza35%
Moraxella Catarrhalis 5%
Staphylococcus aureus2%
Anaerobes 7%
-
The Canadian Journal of CME / June 2008 37
QUESTIONS & ANSWERS
ACUTE RHINOSINUSITISTopical Questions, Sound Answers
Canada. Fourteen and a half per cent ofStreptococcus pneumoniae, 33% of Haemophilusinfluenzae and > 95% of Moraxella catarrhalisare -lactamase producing organisms.3
How can it be diagnosed?
The signs and symptoms suggestive of rhinosi-nusitis are listed in Table 1. Diagnosis of acutebacterial rhinosinusitis may be made if signs andsymptoms persist after 10 days or worsen afterfive days. Facial pain or headache alone, evenwhen present in an area of a sinus, is neither sen-sitive nor specific for sinus disease. Contrary topopular belief, change in colour of secretions isnot a specific sign of bacterial infection.Neutrophil and macrophage influx beginning inthe third to fourth day of a viral rhinosinusitis con-tributes to the formation of coloured secretions.4
Sinus films are not recommended in the rou-tine evaluation of an uncomplicated community-acquired rhinosinusitis. Indications are listed inTable 2. A meta-analysis of six studies demon-strated that positive plain film radiographs have
Dr. Al-Khatib is an OtolaryngologyResident, McGill University, Montreal,Quebec.
Dr. Samaha is an Assistant Professor,Department of Otolaryngology, McGillUniversity Health Centre, RoyalVictoria Hospital, Montreal, Quebec.
Table 1
Signs and symptoms of rhinosinusitis
Major
Facial pain/pressure/fullness Nasal obstruction/blockage Nasal or postnasal discharge/purulence
(by history or physical exam) Hyposmia/anosmia Fever (in acute rhinosinusitis)
Minor
Headaches Halitosis Fatigue Dental pain Cough Otalgia
Table 2
Indications for a sinus film
Equivocal diagnosis
Severe symptomatology
Hospitalized patients
Comorbid conditions
Resistant organisms
Significant frontal symptoms (suspectedfrontal sinusitis, which carries a higher risk ofintracranial complications)
Figure 3b. Right maxillary opacification.
Figure 3a. Right maxillary sinus air-fluid level.
-
38 The Canadian Journal of CME / June 2008
moderate sensitivity (76%) and specificity(79%) compared with maxillary sinus puncture.5
An air fluid level (Figure 3a) or a completeopacification of a sinus detected on plain films(Figure 3b) is diagnostic of acute rhinosinusitis.Mucosal thickening is not sufficiently reliable.CT scanning is the gold standard radiologic testto evaluate the sinuses. However, because ofinaccessibility and cost, it does not play a signifi-cant role in the diagnosis of non-complicatedacute rhinosinusitis.Rhinosinusitis can be classified according to the:
duration of symptoms (i.e., acute [less thanfour weeks], subacute [four to 12 weeks]and chronic [ 12 weeks]),
etiology (i.e., viral, bacterial, or fungal), or site (i.e., frontal, ethmoidal, maxillary,sphenoidal, or pansinusitis where all sinusesare involved).
How can it be treated?
The goal of treatment is to provide symptomaticrelief and prevent complications. Treatmentincludes: nasal saline irrigation, topical nasal steroids, antihistamines in the case of allergicpatients,
Table 3
Treatment of rhinosinusitis
Antibiotics
Topical corticosteroids
Decongestants
Antihistamines
Nasal saline irrigation
Mucolytics
Table 4
Indications for using second-lineantibiotics
No clinical response to treatment withfirst-line antibiotics within 72-96 hours
Allergy to -lactam antibiotics
The use of antibiotics in the preceeding3 months
Underlying chronic illness orimmunosuppression
Prolonged duration of symptoms
Figure 4. Treatment algorithm for acute rhinosinusitis.
< 7 daysViral URTI
ResolvingViral URTI
Tx Complete
OORRLL RReeffeerrrraall
Tx Complete
Dx Equivocal
NO. Switch to2nd line Abx
Dx clinically suggestive
Sinus FilmsNegative
PositiveDecongest/Mucolytics
> 7 days
YesAmoxil
No ResponseSINUSITIS
Response in 72-96 hours
ResponseYes
No
No
Dx: diagnosis URTI: upper respiratory tract infection Abx: antibiotics Tx: treatment ORL: otolaryngology
-
QUESTIONS & ANSWERS
ACUTE RHINOSINUSITISTopical Questions, Sound Answers
mucolytics (provided the patients waterintake is sufficient),
antibiotics and oral or topical nasal decongestant (Table 3). Topical decongestants are not recommended formore than three to five days, as prolonged usemay lead to dependence and a rebound rhinitisoften referred to as rhinitis medicamentosa.Duration of antibiotic treatment recommended isusually seven to 10 days. Despite quoted resis-tance rates, amoxicillin is still recommended asthe first-line treatment, as it is clinically effectivein > 95% of cases. In instances where a second-line antibiotic is indicated (Table 4), amoxicillin-clavulanate, macrolides, cephalosporins (secondgeneration) and fluoroquinolones can be used.
Conclusion
Acute rhinosinusitis is among the most diag-nosed conditions in Canada. The large majorityof these cases are evaluated and treated by pri-mary care physicians. In an era of increasingantibiotic resistance, judicious and selective useof antibiotic therapy is pertinent. This articleattempts to aid practitioners in distinguishingthe minority of patients in whom a bacterial eti-ology may benefit from antibiotic therapy, asopposed to the majority of viral rhinosinusitiscases who require only supportive symptomatictreatment.
References1. Berg O, Carenfelt C, Rystedt G, et al: Occurrence of Asymptomatic
Sinusitis in Common Cold and Other Acute ENT-Infections. Rhinology1986; 24(3):223-5.
2. Desrosiers M, Frenkiel S, Hamid QA, et al: Acute Bacterial Sinusitis inAdults: Management in the Primary Care Setting. J Otolaryngol2002; 31(Suppl 2);2S2-14.
3. R. Davidson, PhD, February 2002 Canadian Bacterial SurveillanceNetwork, Jan 2002. http://microbiology.mtsinai.on.ca.
4. Winther B: Effects on the Nasal Mucosa of Upper Respiratory Viruses(Common Cold). Dan Med Bull 1994; 41(2);193-204.
5. AHCPR. Diagnosis and Treatment of Acute Bacterial Rhinosinusitis.Rockville (MD): Agency for Health Care Policy and Research; No. 99-E016, March 1999.
Resources1. Bailey BJ, Calhoun KH, Derkay CS, et al: Head and Neck Surgery-
Otolaryngology. Third Edition. Lippincott Williams & Wilkins,Philadelphia, 2001. p.345-57.
2. Rosenfeld RM, Andes D, Bhattacharyya N, et al: Clinical PracticeGuideline: Adult Sinusitis. Otolaryngol Head Neck Surg 2007; 137(3Suppl):S1-31.
3. Osguthorpe JD: Adult Rhinosinusitis: Diagnosis and Management.Am Fam Physician 2001; 63(1);69-76.
Acute rhinosinusitis isamong the most diagnosed conditions inCanada.
Product Monograph available upon requestWyeth Consumer Healthcare Inc. Mississauga, ON, Canada L4Z 3M6
AD #: CAL78009ECLIENT: WYETH CONSUMERPRODUCT: CALTRATESIZE: 2.875 x 2.875COLOUR: 4C PROCESSSCREEN: 150DATE: SPRING 2008PUBLICATION: CANADIAN JOURNAL OF DIAGNOSIS
JOURNAL OF CME
CYAN MAGENTA YELLOW BLACK**78009_E CAL Ad.indd 1 1/28/08 11:43:29 AM
For prescribing information see page XXX
Ad_Rx_English Master:Layout 1 2/1/08 2:02 PM Page 3