
門急診常見頭痛的治療及陷阱 Pitfalls of Headache and Treatment in Practice...
53
門門門門門門門門門門門門門 門門門門門門門門門門門門門 Pitfalls of Headache and Pitfalls of Headache and Treatment in Practice Treatment in Practice 門門門門門門 門門門門門 門門門門門 ER----Emergency Room
-
Upload
katrina-barton -
Category
Documents
-
view
400 -
download
7
Transcript of 門急診常見頭痛的治療及陷阱 Pitfalls of Headache and Treatment in Practice...

門急診常見頭痛的治療及陷阱門急診常見頭痛的治療及陷阱Pitfalls of Headache and Treatment Pitfalls of Headache and Treatment
in Practicein Practice
奇美醫學中心全人醫療科林高章主任
ER----Emergency Room

Functional headache ( 功能性頭痛 )
Migraine Tension type headache Cluster and other trigeminal
autonomic cephalalgia Other primary headache
(stabbing, cough, intercourse..)
Episodic <15d/mChronic >15d/m, >3m

Adults: 頻率≧ 5 times, 時間持續 4-72 hours
Migraine Diagnosis (IHS criteria)
At least two of the following features:Unilateral locationThrobbing characterWorsening pain with routine activityModerate to severe intensity
At least one of the following features:Nausea and/or vomitingPhotophobia and phonophobia
Medical History, Headache diary, Migraine triggersInvestigations (only to exclude secondary causes)
ex: EEG / CT Brain / MRI
2
1
Migraine Without Aura (ICHD, 2004)
1
Adolescents migraine:1-48 hours, bilateral, autonomic disturbance
Obvious postdrome symptoms

台灣經驗 (755 headache patients, 102 neurologists)
中重度頭痛、噁心、畏光敏感性 82%,特異性 73%陽性預測率 =91%(神經科門診 )
J Formos Med Assoc 2008;107:485–94
1. In past 3m, does your HA have nausea?2. Do you have more light sensitive during HA?3. Do you have more disability during HA?
2/3==91%3/3==98% (Lipton et al, Neurology, 2004)

Migraine headache ( 偏頭痛 )
Trigeminal nerve was stimuli extending from occipital to anterior, and substance-p (glutamate, CGRP) extra-vasation with evolving to central sensitization to hypothalamus resulting in nausea/vomiting, visual blurring, or fatigue symptoms.
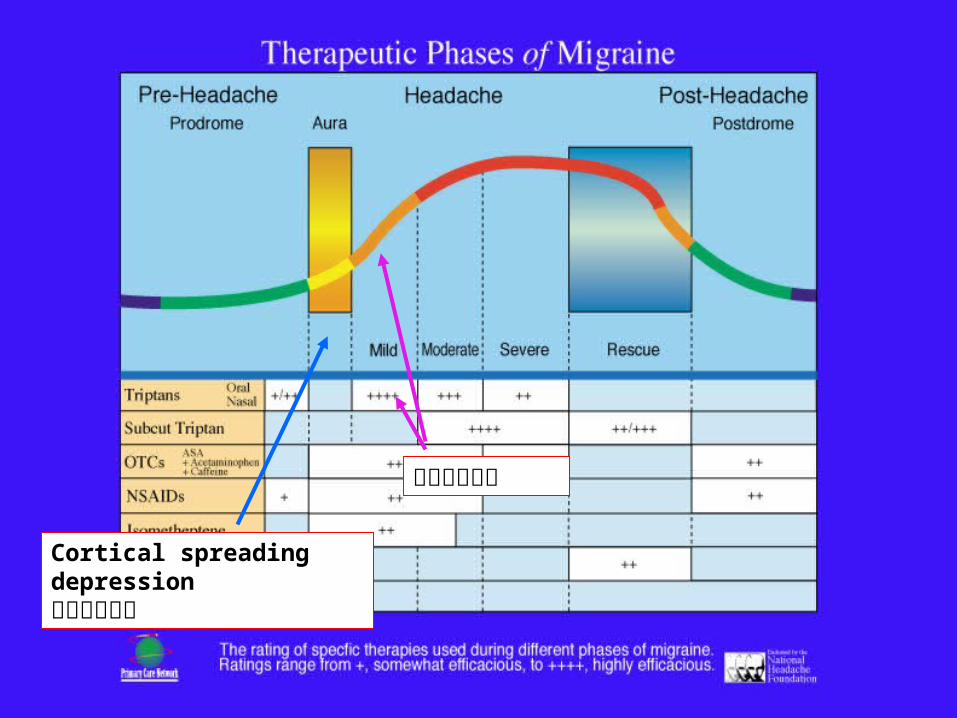
Cortical spreading depression皮質擴散抑制
藥物介入時機

(C)
(AAN guideline-2000)
EBM for acute migraine (US)
1. Sumatriptan (po, iv, sc)2. Rizatriptan (po)3. Naprosin solium (po)4. Ibuprofen (po)5. Prochlorperazine (iv)
Group 1 recommend
1. Diclofenac K (po)2. Chlorpromazine (im, iv)3. Metochlopromide (iv)4. Ketorolac (im)
Group 2 recommend
1. Cafergot (po)2. Metochlopromide (im)
Group 3 recommend

Taiwan guideline for Acute Rx (2007)
(A) Imigran- 英明格 (po, nasl) , (Rizatan- 羅沙疼 )
(B) Ergots (cafergot) , DHE , Panadol , NSAIDs
(A) Aspirin , Ibuprofen (PO)- 輕度偏頭痛

(C) Magnesium, Valproate, Lidocaine, Opioids
(B) Primperan, Novamin, Droperidol (im/iv)
Tension type headache ( 緊縮性頭痛 )
Headaches lasting from 30 minutes to 7 daysAt least two of the following pain characteristics:
Pressing or tightening (nonpulsating) qualityMild to moderate intensityBilateral locationNo aggravation from walking stairs or similar routine
activities
Both of the following:No nausea or vomitingPhotophobia and phonophobia absent, or only one is
present

Tension-type Headache or Migraine
( 輕 / 中 ) 疼痛嚴重度 ( 中 / 重 )Tension-Type Migraine
Mild
Moderate
Severe
Unilateral
Bilateral
Photophobia
Nausea
Throbbing
Pressure
Aura
Vomiting
Aggravated by Activity
© 2002 Primary Care Network

Cluster headache ( 叢發性頭痛 )Unilateral – 100%Restlessness – 93%Retroorbital – 92%, (temporal – 70%)Lacrimation – 91%Conjuctival injections – 77%Nasal congestion/rhinorrhea – 75%Ptosis/eyelid swelling – 74%Phonophobia/phophobia – 50%
季節性因素,男 > 女,頭痛嚴重度 - 中,頭痛合併流淚 / 紅眼 / 眼窩痛 / 眼皮墜 ..

Treatment
• Acute– tryptans (Imigran/ Rizatan)
• 74% effective within 15 min• Nasal spray may be more effective
– Oxygen (100% O2, high flow volume, 7-12L)

References
• 陳韋達、陳錫銘、陳威宏、陳彥宇、傅中玲、謝蒼松、許立奇、莊凱迪、林高章、林日暉、劉崇祥、盧相如、蔡景仁、王博仁、王署君、吳進安 ( 台灣頭痛學會治療準則小組 ).偏頭痛急性發作藥物治療準則 .Acta Neurol Taiwan 2007;16:252-268.
• 林高章、陳錫銘、陳威宏、陳韋達、陳彥宇、傅中玲、謝蒼松、許立奇、莊凱迪、林日暉、劉崇祥、盧相如、蔡景仁、王博仁、王署君、吳進安 ( 台灣頭痛學會治療準則小組 ) 。偏頭痛預防性藥物治療準則。 Acta Neurol Taiwan 2008;17:132-148.
• 陳炳錕、陳錫銘、陳威宏、陳彥宇、傅中玲、李連輝、廖羽筑、林高章、曾弘斌、蔡景仁、王博仁、王署君、楊鈞百、姚俊興、吳進安 ( 台灣頭痛學會治療準則小組 ) 。叢發性頭痛治療準則。 Acta Neurol Taiwan 2011; 20: 213-217.

SinusSinus
TreatmentTreatment
TensionTension
MigraineMigraine
The Headache Dilemma…The Headache Dilemma…

Organic headache (pearl symptoms)
Midnight or early morning headacheAssociated with Sz, neck stiffness,
focal neurological signs, lapse..Headache with LOCHeadache pattern changeThunderclap headache (Shower HA)
Other (RCVS-Reversible cerebral vasoconstriction syndrome…)

Increased intracranial hypertensionIncreased intracranial hypertensionCPP= MAP-ICP = D+1/3(S-D)- ICP
(2006, BJA)

Symptoms and signs of IICPSymptoms and signs of IICP
Headache/vomiting/papilloedema Cushing triad VI palsy Thumb signs Sella erosion Sulci effacement

DVT
Empty sella
pseudo-tumor cerebri
VI palsy Thumb signMidline shift
IICPIICP
Idiopathic IICPIdiopathic IICP(pseudotumor cerebri)(pseudotumor cerebri)
1. Most frequently occurs in obese women of childbearing age.
2. F:M=3~8:1
3. May associate with endocrine (adrenal insuff, Cushing synd, hyper-, hypo-thyroidism..), drugs (cimetidine, steroids, minocycline, nalidixic acid, tamoxifen..), IDA, CKD, SLE, Lyme disease...
4. Headache, N/V, gradual visual loss,papilloedema..
5. Ddx by screening of CT/MRI/CSF/biochemistry/serology tests..
6. Rx: medical (prednisolone) and surgery (CSF diversion).
7. Underlying control (weight loss, stop causative meds..).

Red flags in IICPRed flags in IICP
CasesCases scenarioscenario
CC: 35-year-old had severe headache with vomiting
for 2 days.PI: Persistent headache for 4 weeks, from occipital
extended to frontal area. Non-pulsation character, position-related (upright
worsen, lying down better), whole days long.Severe pounding pain when head down (pain score 7-8)
Neurological exam.- NP

Brain CT (without contrast)Brain CT (without contrast)
1.IICP2.Sinus thrombosis

R/o SAH, aneurysm or AVM rupture

C-
C+

MRI (T2WI)MRI (T2WI) SDH? Subdural effusion?

MRIMRI

CSF studyCSF study
IP/TP= 60/30 mm H20
India ink- negative.
Gram stain- negative
TB-PCR-negative.
WBC=1
RBC=140
L:N=1:0
Protein= 54.3 (15-45mg)
Sugar 77 (40-70)
Diagnosis?

Intracranial hypotension syndrome:Intracranial hypotension syndrome:a comprehensive reviewa comprehensive review (Neurosurg Focus, 2003) (Neurosurg Focus, 2003)
1. It is characterized by orthostatic headache,
usually occur or worsen with upright posture.
2. May associate with chronic headache or even no
suffers.
3. Pain exacerbated by laughing, coughing, or
Valsalva maneuver.
4. Resistant to treatment of analgesic agents.

5. Nausea, vomiting, anorexia, neck pain, dizziness, horizontal diplopia, change in hearing, galactorrhea, facial numb and weakness can occur, related to orthostatic nature.
6. Usually benign course and resolve symptoms with conservative treatment.
7. Dx can be confirmed by CSF opening pressure (<60 mmH20), CSF usually be normal or mild increase protein, WBC, or RBC.
8. Occur from a persistent CSF leakage, dural puncture, myelography or spinal anesthesia; may be violated as craniotomy, spinal surgery, craniospinal trauma, or VP shunting.

CT and MRI diagnosisCT and MRI diagnosis
CT demonstrate obliteration of basal cisterns due to sagging of brain (misdiagnosed of SAH).
MRI (Gd+) with diffused thickening of pachymeninges, engorge venous sinus, subdural fluid collection, enlargement of pituitary gland, and downward displacement of the brain.
MR images resolution parallels to clinical improvement.
Compensatory hypothetical mechanism to CSF loss with above findings.

TreatmentTreatment
1. Conservative treatment and bed rest.
2. Increase fluid restoration, eliminating CSF leakage.
3. Increase salty intake.
4. Epidural blood patch to be a safe and effective treatment (85~98%).
5. Epidural fibrin glue shows a promising result.
6. Surgical correction when all procedures are failed.
Pearl symptom: Orthostatic headache

What kind of headache appearance is pathogenic?
All might be.

無緣無故怎麼會出血 ?如果高血壓 , 也不是常見位置 !怎麼會頭痛 ????
Sinus thrombosis with ICH
1. 37 yrs, young F, had pulsatile tinnitus and bilateral throbbing headache for 1 month.
2. S/s off and on after medications but frequent recurrence.
3. Neck rigid followed persistent headache and MFP told by physician.
4. Lapse with seizure once, and was sent to ER.
5. PE/NE with Lt side weakness.

高血壓常見出血位置
• Putamen (40%)
• Thalamus (30%)
• Brain stem-Pons(10%)
• Cerebellum (10%)
• Subcortical area (10%)

Management of sinus thrombosis
1. ICU care with IICP control
2. Heparinization
CPP= MAP- ICP
V
P
Pearl symptom:Headache with lapse, neck rigid
or focal NE signs
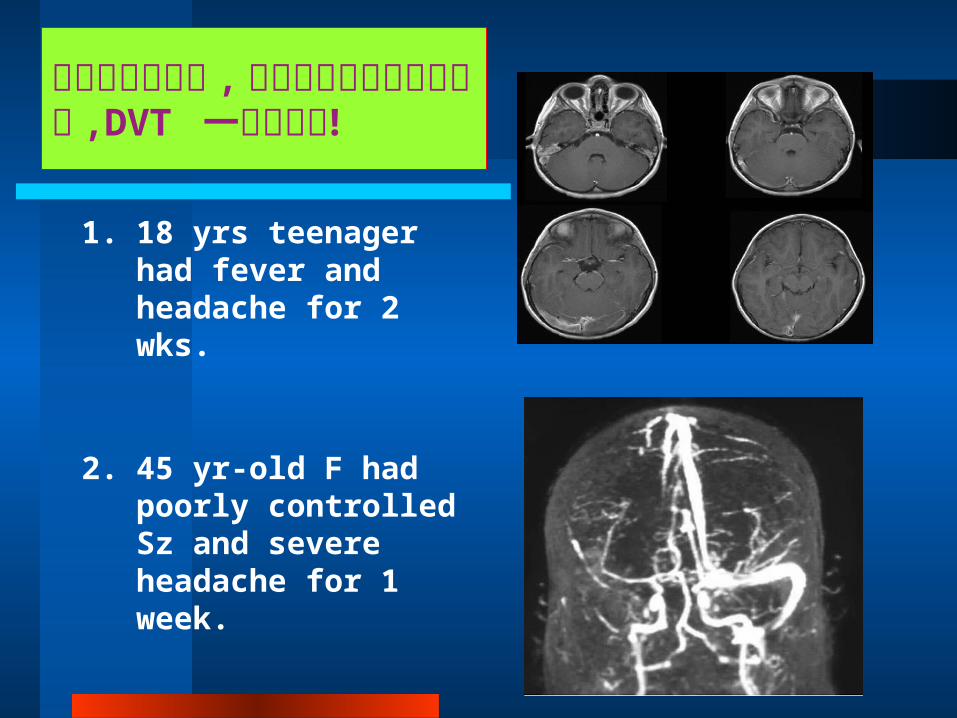
其他例子對於奇怪的頭痛 , 不論有否合併神經學異常 ,DVT 一定要考慮 !
1. 18 yrs teenager had fever and headache for 2 wks.
2. 45 yr-old F had poorly controlled Sz and severe headache for 1 week.
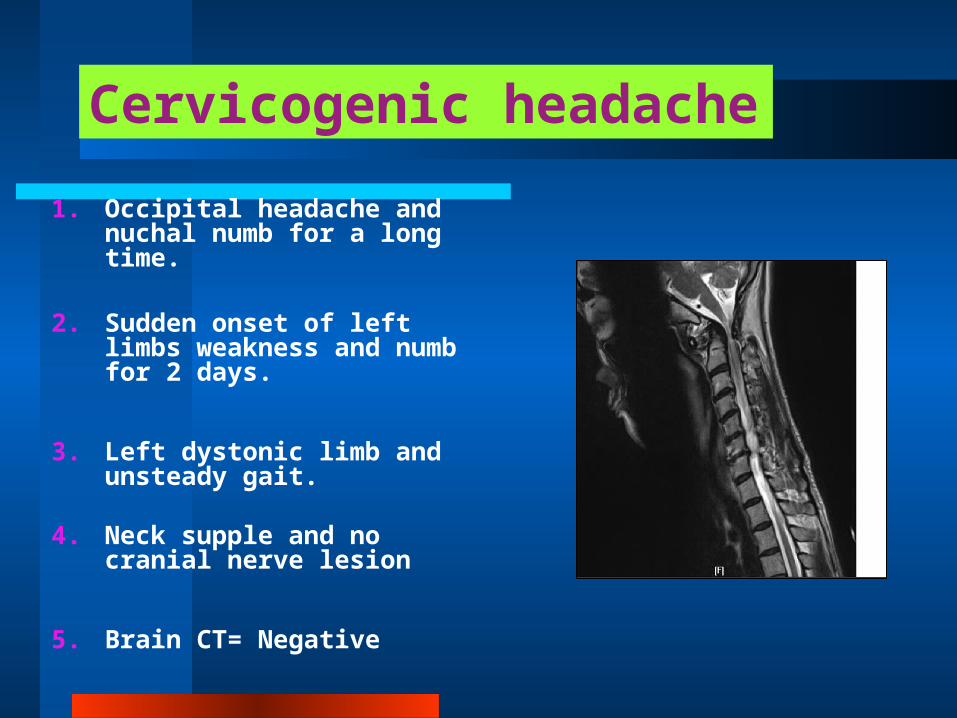
1. Occipital headache and nuchal numb for a long time.
2. Sudden onset of left limbs weakness and numb for 2 days.
3. Left dystonic limb and unsteady gait.
4. Neck supple and no cranial nerve lesion
5. Brain CT= Negative
Cervicogenic headache

頸因性頭痛(ICHD-II, 2004)
A. 源自頸而表現在頭及 / 或臉一處或多處的疼痛,符合基準 C 及 D
B. B. 經臨床、實驗室及 / 或影像證明,有一已知是或普遍認定為頭痛確切致因的頸椎或頸部軟組織疾患或病變
C. C. 依據至少下列一項,證實該疼痛可歸因於頸疾患或病變:1. 臨床徵候顯示,疼痛來自頸部 2. 在安慰劑或其他合適的控制型試驗
下,對頸部結構或其支配神經施行診斷性神經阻斷後,可解除頭痛
D. D. 疼痛在致病疾患或病變有效治療後三個月內緩解

Cervical artery dissection
1. 29 yrs male patient suffered from headache and right neck pain after message.
2. Throbbing HA pattern without Nausea/Vomiting.
3. Transient fall and dizzy after morning awakened on the next day.
4. NE-NP, PE-Neck bruits?
5. HA subsided with NSAID, but dizzy persistent….. Diagnosis?

自發性或外傷性頸動脈撕裂傷
1. 頭痛及頸部疼痛為主要主訴2. 神經學檢查 ( 必須聽一聽頸部
有否雜音 )3. CT/MRI不一定會有發現 , 必
須靠血管檢查 (CTA,MRA)4. 頸動脈超音波可以協助了解是
否狹窄或撕裂5. 治療可以置放頸部支架或血管
修補術
Pearl symptom:Headache and neck bruit
(post-massage)

Space-occupied lesion (primary brain tumor or meta?)
1. 56 yrs old, F, had sudden headache with pounding character over vertex (VAS-10).
2. Previous migraine Hx(+), and breast ca 5 yrs ago, with CT/RT therapy.
3. PE/NE showed no focal limbs weakness, visual filed (VF) defect was defined by confrontation test. Diagnosis?
Pearl symptom:Headache and VF defect

SAH, aneurysm rupture
1. 68 yrs old male pt, HTN+, DM+, Sudden severe headache and LOC.
2. Vomiting during HA, and four limbs weakness defined.
3. Neck stiffness was noted (4fb band width) and OCHA on arriving at ER.
4. pupil dilated on both eyes

SAH
1. 自發性必需深究原因 ( 年輕人 -AVM; 中老年 -Aneurysm)
2. 外傷性可以症狀治療處理3. 血壓高必須區別是否腦壓升高 .4. 注意有否 IICP(如前 -Cushing, severe
vomiting, VI palsy..)5. 外傷性但輕微神經學症狀 , 不一定要住 ICU.6. 使用 Nimotop (CCB) 避免血管收縮造成腦缺血7. TCD可以了解腦血流狀況 ( 流量高低 , 阻力高低… )
Pearl symptom:Unusual headache and neck stiffness
Thunderclap headache
( 雷擊性頭痛 )

(Copyright 2004 American Academy of Neurology)
Summary of findings Increased Intracranial Summary of findings Increased Intracranial Pressure (ICP) and Cerebral Circulatory Pressure (ICP) and Cerebral Circulatory ArrestArrest
INDICATION SENSITIVITY (%)
SPECIFICITY (%)
REFERENCE STANDARD
Cerebral Circulatory Arrest and Brain Death
91-100 97-100Conventional angiography, EEG, clinical outcome
Recommendation: TCD is a useful adjunct test for the evaluation of
cerebral circulatory arrest associated with brain death (Type A, Class
II evidence).

E1VEM1FLACCID RESPONSEALL REFLEX(-)
Small systolic sharpReverse flow patternMCA + BA (較準確 )

SDHwithIICP
High Peak,Low
diastolic

Meningo-encephalitis
1. 28 yrs, F, URI for 1 wk.
2. Fever and non-specific headache off and on, but persistent for 10 more days.
3. Seizure once and was sent to ER.
4. PE/NE; neck stiff (2fb), and post-ictal confusion.
Diagnosis?

腦膜腦炎1. 可以單獨影響腦膜或腦炎 ( 意識較易影響 )2. 區別病因 ( 病毒 , 細菌 , 其他 )3. CSF+MRI檢查4. 確定病毒性 , 急診就需使用 acyclovir
( 愈早使用愈好 )5. 預後依其影響範圍而定6. 抽搐必須藥物控制避免缺氧或重積癲癇7. 使用 EEG評估功能影響 ( 不必一直 MRI追蹤 )
Pearl symptom:Headache, fever and conscious change

Acute glaucoma
1. 46 yrs, F, Rt frontal headache for 5 days, with hallow vision( 中空 , 光蘊 , 散射光 ..)
2. PE- right reddish eye, tender over eyeball (+)
3. IOP 30(od), 18(os)
4. NE- NP
Diagnosis?
Pearl symptom:Headache, eyeball pain

CCF (Carotid cavernous fistula)
1. 70 yrs, M, had MCA, on right frontal and eye injury.
2. Chemosis, exopthalmosis, and throbbing headache.
3. Carotid and right eye bruit.
4. Confirmed by angiography or imaging study.
5. Rx with balloon tamponade or surgical repair.
Diagnosis?
Pearl symptom:Headache, exo-OPH, eye bruits

Take home message
1. 區別 Functional 或 Organic HA
2. Organic HA 必須影像區別 (SAH, SIH, tumor, dissection, meningitis, meningo-encephalitis, CCF, glaucoma, sinusitis, sinus thrombosis, etc)
3. Babinski’s sign should be performed if possible (可以區別 pyramidal tract 是否 involved)
4. NSAIDs/ acetaminophen/Aspirin are preferred firstly, and opioids followed if pain not subsided or pain score> 7-8
5. Education is useful to prevent the re-visiting ED.

Thank you for your attention


















