
토끼 망막에서 NMDA에 의한 아포프토시스의 발현 - KoreaMed · 2008-07-23 · 망막 조직 표본에서 tunel 염색을 시행하여 형광 빛을 보이는 아포프토시스로
Upload
truongquynhCategory
view
232download
11
대한내과학회지: 제 89 권 제 4 호 2015 http://dx.doi.org/10.3904/kjm.2015.89.4.452
- 452 -Copyrightⓒ 2015 The Korean Association of Internal MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 2015. 4. 30Revised: 2015. 6. 3Accepted: 2015. 6. 16
Correspondence to Jae Seuk Park, M.D., Ph.D.Department of Internal Medicine, Dankook University Hospital, Dankook University Medical College, 201 Manghyang-ro, Dongnam-gu, Cheonan 31116, KoreaTel: +82-41-550-3055, Fax: +82-41-556-3256, E-mail: [email protected]
궤양성 대장염으로 Infliximab 치료 중인 환자에서 발생한
Mycobacterium gordonae 폐질환 1예
단국대학교 의과대학 단국대학교병원 1내과, 2병리과
최지성1·배종욱1·이상원1·최규호1·신정은1·명나혜2·박재석1
A Case of Mycobacterium gordonae Pulmonary Disease in a Patient with Ulcerative Colitis Treated with Infliximab
Ji Sung Choi1, Jong Wook Bae1, Sang Won Lee1, Gyu Ho Choi1, Jeong Eun Shin1, Na-Hye Myung2, and Jae Seuk Park1
Departments of 1Internal Medicine and 2Pathology, Dankook University Hospital, Dankook University Medical College, Cheonan, Korea
Tumor necrosis factor-α (TNF-α) is a key component of the host defense against mycobacterial infection. Mycobacterium gordonae (M. gordonae) is one of the least virulent mycobacteria, and is generally considered non-pathogenic if detected from a
clinical specimen. Here, we report a rare case of pulmonary M. gordonae infection in a patient with ulcerative colitis who had been
treated with infliximab, a TNF-α antagonist. M. gordonae infection was treated successfully with clarithromycin, rifampin, and
ethambutol. We believe this to be the first report of M. gordonae pulmonary disease associated with TNF-α antagonist treatment.
(Korean J Med 2015;89:452-456)
Keywords: Mycobacterium gordonae; Ulcerative colitis; Infliximab; Tumor necrosis factor-alpha
서 론
종양괴사인자-알파(tumor necrosis factor-alpha, TNF-α) 길
항제들은 류마티스 관절염, 건선, 염증성 장질환과 같은 다
양한 염증성 질환의 치료제로 이용되고 있다[1]. TNF-α는 결
핵균뿐만 아니라 비결핵항산균(nontuberculous mycobacteria)에
대한 인체의 면역학적 방어기전에서 중요한 역할을 하므로
TNF-α 길항제 치료를 받고 있는 환자에서 비결핵항산균 폐
질환이 발생할 위험성이 증가한다[2,3] Mycobacterium gordonae (M. gordonae)는 독성이 낮아 객담에서 검출되면 비결핵항산
균 폐질환의 가능성이 낮고 대표적인 오염균으로 간주되고
있다[4]. 저자들은 TNF-α 길항제로 치료 중인 궤양성 대장염
환자에서 M. gordonae 폐질환으로 진단되어 적절한 약물 치
료 후 호전된 증례를 경험하였기에 문헌고찰과 함께 보고하
는 바이다.
- Ji Sung Choi, et al. Mycobacterium gordonae pulmonary disease-
- 453 -
A B C
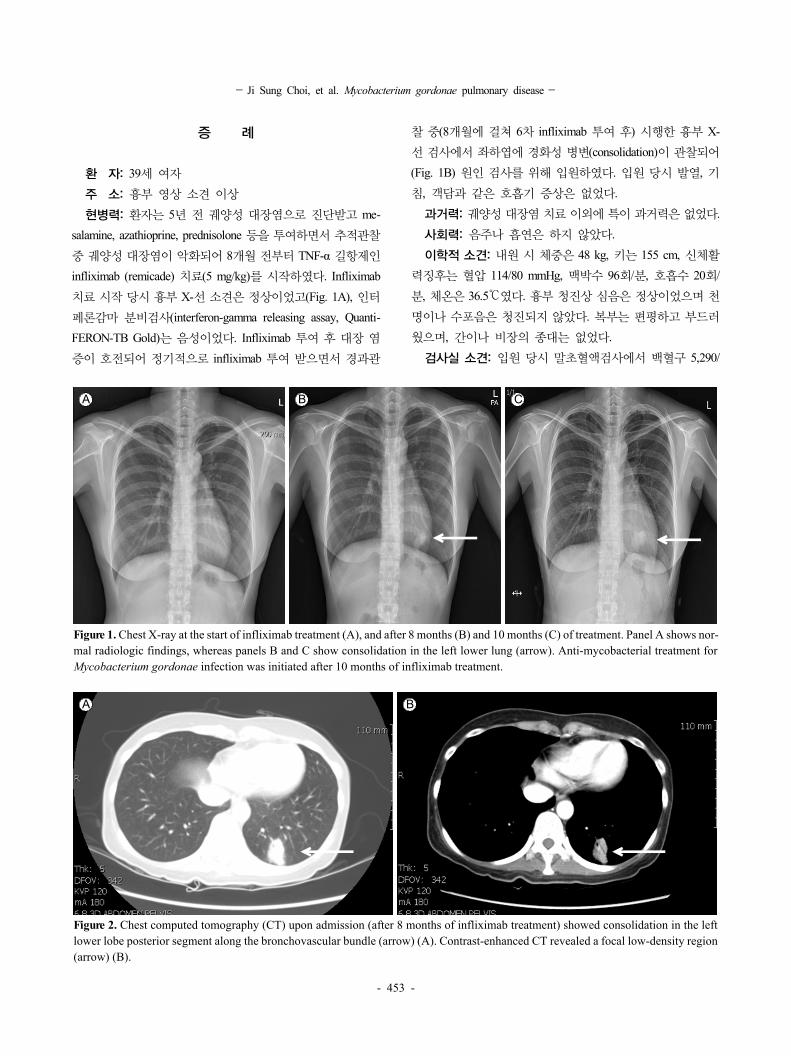
Figure 1. Chest X-ray at the start of infliximab treatment (A), and after 8 months (B) and 10 months (C) of treatment. Panel A shows nor-mal radiologic findings, whereas panels B and C show consolidation in the left lower lung (arrow). Anti-mycobacterial treatment for Mycobacterium gordonae infection was initiated after 10 months of infliximab treatment.
A B
Figure 2. Chest computed tomography (CT) upon admission (after 8 months of infliximab treatment) showed consolidation in the left lower lobe posterior segment along the bronchovascular bundle (arrow) (A). Contrast-enhanced CT revealed a focal low-density region (arrow) (B).
증 례
환 자: 39세 여자
주 소: 흉부 영상 소견 이상
현병력: 환자는 5년 전 궤양성 대장염으로 진단받고 me-
salamine, azathioprine, prednisolone 등을 투여하면서 추적관찰
중 궤양성 대장염이 악화되어 8개월 전부터 TNF-α 길항제인
infliximab (remicade) 치료(5 mg/kg)를 시작하였다. Infliximab
치료 시작 당시 흉부 X-선 소견은 정상이었고(Fig. 1A), 인터
페론감마 분비검사(interferon-gamma releasing assay, Quanti-
FERON-TB Gold)는 음성이었다. Infliximab 투여 후 대장 염
증이 호전되어 정기적으로 infliximab 투여 받으면서 경과관
찰 중(8개월에 걸쳐 6차 infliximab 투여 후) 시행한 흉부 X-
선 검사에서 좌하엽에 경화성 병변(consolidation)이 관찰되어
(Fig. 1B) 원인 검사를 위해 입원하였다. 입원 당시 발열, 기
침, 객담과 같은 호흡기 증상은 없었다.
과거력: 궤양성 대장염 치료 이외에 특이 과거력은 없었다.
사회력: 음주나 흡연은 하지 않았다.
이학적 소견: 내원 시 체중은 48 kg, 키는 155 cm, 신체활
력징후는 혈압 114/80 mmHg, 맥박수 96회/분, 호흡수 20회/
분, 체온은 36.5℃였다. 흉부 청진상 심음은 정상이었으며 천
명이나 수포음은 청진되지 않았다. 복부는 편평하고 부드러
웠으며, 간이나 비장의 종대는 없었다.
검사실 소견: 입원 당시 말초혈액검사에서 백혈구 5,290/

-대한내과학회지: 제 89 권 제 4 호 통권 제 662 호 2015-
- 454 -
A B C
Figure 3. Fine needle aspiration cytology of the lung lesion showed relatively loose aggregates of epithelioid histiocytes admixed with scattered lymphocytes in a background of necrotic material (arrow) (A, B) (Papanicolaou stain, ×400). Immunohistochemical staining for CD68, a histiocytic marker, showed that cells were mostly composed of histiocytic inflammatory cells (C) (×200).
Table 1. Antibiotic susceptibility data for isolated Mycobacterium gordonae
Antibiotics Test concentrations
(mcg/mL) MIC
(mcg/mL)
Amikacin 1-128 32
Cefoxitin 2-256 > 256
Ciprofloxacin 0.125-16 > 16
Clarithromycin 0.5-64 1
Doxycycline 0.25-32 > 32
Imipenem 0.5-64 > 64
Moxifloxacin 0.125-16 4
Rifampicin 0.125-16 8
Sulfamethoxazole/trimethoprim 0.25/4.75-32/608 8/152
Tobramycin 0.25-32 8
Ethambutol 0.25-32 16
Linezolid 2-64 32
MIC, minimal inhibitory concentration.
mm3 (호중구 70.9%, 림프구 14.0%), 혈색소 9.4 g/dL, 혈소판
358,000/mm3, 혈청생화학 검사에서 혈청 총 단백 5.2 g/dL, 알
부민 2.9 g/dL, AST/ALT 21/10 U/L, 총 빌리루빈 0.26 mg/dL,
혈액요소질소 14.9 mg/dL, Cr 0.43 mg/dL, LDH 251 U/L,
C-reactive protein 1.56 mg/dL였다. 소변 검사상 특이 소견은
없었다. 인터페론감마 분비검사를 다시 시행했는데 음성이
었다. 객담 항산균 도말 및 배양검사는 음성이었다.
방사선 소견: 흉부 X-선 검사(Fig. 1B) 및 흉부 전산화단
층촬영(Fig. 2)에서 좌하엽에 폐경화(consolidation) 소견이 관
찰되었다.
기관지내시경 검사: 기관지 내 병변은 없었고 좌하엽 pos-
terior basal segment에서 기관지폐포세척(bronchoalveolar lavage)
을 시행하였다. 기관지폐포세척액 세포진 검사에서 암세포는
관찰되지 않았고, 항산균 도말검사는 음성이었고 결핵균 핵
산증폭검사에서 결핵균은 검출되지 않았다.
경피세침흡인검사(percutaneous fine needle aspiration):
좌측 폐 병변에 대해 경피세침흡인을 시행하여 시행한 병리
검사에서 괴사성 병변을 동반한 상피양 세포들과 림프구의
집합체가 관찰되었다(Fig. 3). 조직에 대한 항산균 도말검사
는 음성이었고, 핵산증폭검사에서 결핵균은 음성이었고 비결
핵항산균은 양성이었다.
치료 및 경과: 폐 세포 병리 소견상 비결핵항산균에 의한
폐 병변의 가능성이 크지만 호흡기 증상이 없고 균동정이 되
지 않았기 때문에 폐 병변에 대한 치료를 시행하지 않고 항
산균 배양 검사 결과를 기다렸다. 이후 기관지폐포세척액에
대한 액체배지와 고체배지에서 비결핵항산균이 배양되었다.
폐 조직에 대한 항산균 배양검사에서는 배양되지 않았다. 기
관지폐포세척액에서 배양된 비결핵항산균에 대해 균동정검
사를 시행하였는데 M. gordonae가 동정되었다. 결핵연구원에

-최지성 외 6인. M. gordonae 폐질환-
- 455 -
A B
Figure 4. Chest X-ray after 2 months (A) and 12 months (B) of anti-mycobacterial treatment for Mycobacterium gordonae pulmonary infection. Panel A shows partial resolution of the lesion observed in the left lower lung (arrow). Panel B shows complete resolution of the lesion.
의뢰하여 동정된 M. gordonae의 약제 감수성 검사를 시행하
였다(Table 1). 폐병변이 처음 관찰된 지 2개월 후에 시행한
흉부 X-선에서 좌하엽 경화성 병변이 지속적으로 관찰되어
(Fig. 1C) M. gordonae 폐질환으로 진단하고 약제감수성 검사
에서 감수성을 보인 clarithromycin, rifampin, ethambutol로 치
료를 시작하였다. 치료 시작 후 병변이 지속적으로 감소하였
고(Fig. 4) 치료 시작 1개월과 3개월 후에 2차례 추구 객담
항산균 도말 및 배양검사를 시행하였는데 모두 음성이었다.
1년간 약물치료 후 M. gordonae 폐질환 치료를 종결하였다.
치료 종결 6개월에 시행한 흉부 X-선 소견에서 재발의 증거
가 없었으며 infliximab 5 mg/kg로 6주 간격으로 투약하면서
증상 및 내시경적 관해를 유지하고 있다.
고 찰
궤양성 대장염은 호전과 악화를 반복하는 만성 염증성 장
질환으로 그 원인은 정확히 알려져 있지 않다. TNF-α가 장관
염증의 중요한 매개체이며 TNF-α 길항제들이 스테로이드나
면역억제제에 비해 우수한 증상 호전과 점막 치유 효과를 보
이는 것이 밝혀짐에 따라 스테로이드나 azathioprine과 같은
면역억제제 사용으로 관해나 호전을 보이지 않는 중등도 이
상의 궤양성 대장염 환자에서 TNF-α 길항제들의 사용이 증
가하고 있다[5].
TNF-α는 육아종의 형성 등 결핵균에 대한 인체의 면역학
적 방어기전에서 중요한 역할을 하는데 TNF-α 길항제가 이
과정을 억제하므로 결핵균에 감염된 사람에서 TNF-α 길항제
치료를 받을 경우 결핵이 발생할 위험성이 증가한다[2]. 그러
므로 TNF-α 길항제 사용 전에 활동성 결핵 여부를 확인하고
결핵이 없을 경우 결핵감염 검사를 시행하고 잠복결핵감염
으로 진단되면 잠복결핵감염치료를 시행하도록 권고하고 있
다[5]. 본 증례의 환자도 TNF-α 길항제를 사용하기 전에 흉부
X-선 검사와 인터페론감마 분비검사를 시행하여 폐결핵이 없
고 잠복결핵감염 상태가 아님을 확인하였다.
TNF-α 길항제는 결핵균뿐만 아니라 비결핵항산균에 대한
방어기전도 억제하므로 TNF-α 길항제 치료를 받는 환자에서
비결핵항산균 폐질환이 발생 또한 증가하는 것으로 알려져
있다[6].
비결핵항산균은 균종에 따라 독성(virulence)이 다른데,
mycobacterium avium complex (MAC), M. kansasii, M. abscessus 등은 상대적으로 독성이 높아 객담에서 검출되면 비결핵항
산균 폐질환의 가능성이 크지만, M. gordonae는 독성이 낮아
폐 병변을 일으키는 경우가 거의 없으며 객담에서 M. gordonae가 검출되면 대표적인 오염균으로 간주되어 왔다[4,7]. 그러
나 기관지폐포세척액 또는 폐 조직 생검에서 M. gordonae가

-The Korean Journal of Medicine: Vol. 89, No. 4, 2015-
- 456 -
검출되거나 객담의 경우 M. gordonae가 반복해서 검출되고
폐 병변을 일으킬 수 있는 다른 원인이 없을 때 M. gordonae 폐질환(true infection)을 의심해 볼 수 있으며[7], 사람면역결
핍바이러스(human immunodeficiency virus) 감염, 스테로이드
치료, 장기이식환자와 같은 면역억제 환자들뿐만 아니라 정
상 면역인에서도 M. gordonae가 병을 일으킬 수 있다는 보고
들이 있다[8,9].
TNF-α 길항제로 치료 중인 환자들에서 발생한 비결핵항
산균 폐질환의 원인균을 분석한 국내외의 연구들에서도 대
부분 MAC이 원인균이었으며 M. gordonae가 원인균인 경우
는 없었다[3,10]. 그러나 본 증례는 TNF-α 길항제를 사용 중
인 환자에서도 M. gordonae가 폐질환을 일으킬 수 있음을 보
여주고 있다.
M. gordonae 폐질환의 흉부 방사선 소견은 폐결절, 공동,
폐침윤(infiltration), 기관지확장, 폐경화(consolidation) 등 다양
한 소견을 보일 수 있다고 알려져 있으며[9], 본 증례에서는
폐경화 소견을 보였다(Fig. 2).
M. gordonae 감염의 치료 약제와 치료 기간은 아직 정립되
지 않는데 시험관에서 항균력이 있는 clarithromycin, rifampin,
ethambutol, fluoroquinolone 등이 경험적으로 사용되고 있다[7].
본 증례에서도 배양된 M. gordonae에 대한 약제 감수성 검사
에서 감수성을 보이는 clarithromycin, rifampin, ethambutol로
치료하였고 치료에 좋은 반응을 보였다. 치료 기간 또한 문
헌마다 9개월에서 22개월까지 다양한데 본 증례에서는 12개
월간 약물 치료로 적절히 치료되었다[8].
본 증례는 TNF-α 길항제를 사용 중인 환자에서 발생한
M. gordonae 폐질환으로 적절한 약물치료로 완치된 첫 번째
증례 보고이다. 그러므로 임상 검체에서 M. gordonae가 검
출되더라도 오염균으로 보고 감별진단에서 배제하지 말고
M. gordonae 감염병의 가능성을 고려하여야 할 것으로 사료
된다.
요 약
TNF-α는 항산균에 대한 인체의 면역학적 방어기전에서
중요한 역할을 한다. Mycobacterium gordonae는 독성이 낮아
임상 검체에서 검출되면 대부분 오염균으로 간주되고 있다.
저자들은 TNF-α 길항제로 치료 중인 궤양성 대장염 환자에
서 M. gordonae 폐질환으로 진단되어 적절한 약물 치료 후
호전된 증례를 경험하였기에 문헌고찰과 함께 보고하는 바
이다.
중심 단어: Mycobacterium gordonae; 궤양성 대장염; In-
fliximab; 종양괴사인자-알파
REFERENCES
1. Gisbert JP, González-Lama Y, MatéJ. Systematic review:
Infliximab therapy in ulcerative colitis. Aliment Pharmacol
Ther 2007;25:19-37.
2. Keane J, Gershon S, Wise RP, et al. Tuberculosis associated
with infliximab, a tumor necrosis factor alpha-neutralizing
agent. N Engl J Med 2001;345:1098-1104.
3. Yoo JW, Jo KW, Kang BH, et al. Mycobacterial diseases de-
veloped during anti-tumour necrosis factor-α therapy. Eur
Respir J 2014;44:1289-1295.
4. Koh WJ, Kwon OJ, Jeon K, et al. Clinical significance of
nontuberculous mycobacteria isolated from respiratory speci-
mens in Korea. Chest 2006;129:341-348.
5. Hyams J, Damaraju L, Blank M, et al. Induction and main-
tenance therapy with infliximab for children with moderate
to severe ulcerative colitis. Clin Gastroenterol Hepatol 2012;
10:391-399.e1.
6. Winthrop KL, Yamashita S, Beekmann SE, Polgreen PM;
Infectious Diseases Society of America Emerging Infections
Network. Mycobacterial and other serious infections in pa-
tients receiving anti-tumor necrosis factor and other newly
approved biologic therapies: case finding through the Emerg-
ing Infections Network. Clin Infect Dis 2008;46:1738-1740.
7. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official
ATS/IDSA statement: diagnosis, treatment, and prevention
of nontuberculous mycobacterial diseases. Am J Respir Crit
Care Med 2007;175:367-416.
8. Weinberger M, Berg SL, Feuerstein IM, Pizzo PA, Witebsky
FG. Disseminated infection with Mycobacterium gordonae:
report of a case and critical review of the literature. Clin
Infect Dis 1992;14:1229-1239.
9. Mazumder SA, Hicks A, Norwood J. Mycobacterium gor-
donae pulmonary infection in an immunocompetent adult. N
Am J Med Sci 2010;2:205-207.
10. Mori S, Tokuda H, Sakai F, et al. Radiological features and
therapeutic responses of pulmonary nontuberculous myco-
bacterialdisease in rheumatoid arthritis patients receiving
biological agents: a retrospective multicenter study in Japan.
Mod Rheumatol 2012;22:727-737.












