Early Versus Delayed Cholecystectomy for Acute Calculous Cholecystitis

PROTEINS ANDOTHERBIOCOLLOIDS OF URINE IN HEALTHAND IN CALCULOUSDISEASE. I. ELECTROPHORETIC
STUDIES AT PH 4.5 AND 8.6 OF THOSECOMPO-NENTSSOLUBLE IN MOLARSODIUM
CHLORIDE1
By WILLIAM H. BOYCE, FREDK. GARVEY, AND CHARLESM. NORFLEET, JR.
(From the Department of Urology, Division of Surgery, Bowman Gray School of Medicine ofWake Forest College, Winston-Salem, N. C.)
(Submitted for publication March 4, 1954; accepted June 16, 1954)
In approximately 92 per cent of all primary uri-nary calculi, more than 95 per cent of the totalcation content is composed of calcium (1-3).Concepts concerning the mechanism of biologiccalcification have undergone a marked revision inrecent years (4). Rubin and Howard (5) havepresented histochemical evidence that an acid mu-copolysaccharide of cartilage and bone matrix mayact as a "target substance" for the deposition ofcalcium and the eventual formation of bone salts.The structure of urinary concretions suggests thatthe initial matrix may be composed of ion-bindingmucopolysaccharides or other "substrates," whichnot only provide the architectonic framework butmay actually -"extract" specific inorganic compo-nents of urine from solution. The separation andidentification of the organic components of urineare essential prerequisites to an exploration of thispossibility.
A series of experiments, in which some subjectshave been repeatedly examined over a period oftwo years, has demonstrated that the biocolloidsof urine may be separated into three groups ofsubstances, on the basis of their solubilities in dif-ferent buffer systems. It is the purpose of thisreport to present the results of studies on one ofthese groups-those components which are solu-ble in molar sodium chloride and in two bufferswhich have been used in the electrophoretic studyof serum proteins (6-8).
METHODS
Three female and 10 adult male subjects from the staffof the North Carolina Baptist Hospital and the Bowman
1 This investigation was supported by research grantA-259 from the National Institute of Arthritis and Meta-bolic Diseases, of the National Institutes of Health, Pub-lic Health Service.
Gray School of Medicine were selected as a controlgroup; all were known to have normal renal function.The test group was made up of 17 patients (7 femalesand 10 males) selected over a period of 20 months be-cause they were demonstrated roentgenographically tohave progressively developing calculi. Later analysis ofthese stones showed them to contain pure calcium phos-phate or a mixture of calcium phosphate and calciumoxalate. These patients were studied prior to operation,and no individual with signs or symptoms of acute in-fection was included. In addition, two patients, ages 7and 11 years, with the nephrotic syndrome and two pa-tients, ages 16 and 18 years, with lupus erythematosuswere studied as examples of altered capillary permeability.Four additional patients with bilateral obstructive uri-nary tract disease and bacterial pyelonephritis were stud-ied before operation, but after the signs of pyelonephritishad subsided.
Clean voided specimens of urine were collected intochemically clean containers without preservatives, and im-mediately refrigerated at 0° C. Hospitalized subjectswere provided with bedside ice chests to insure promptrefrigeration. Each 24-hour specimen was centrifugedat 800 times gravity to remove formed elements, andthen dialyzed against distilled water at 3° C. until theelectrical conductivity approached 100 X 10' and the pHwas the same as the distilled water.
The dialyzed specimens were subj ected to ultrafiltra-tion in stainless steel filters through a modification of thecollodion membranes described by Gorbman (9). Vlari-ations in porosity of the membranes were minimized bypreparing 30 individual membranes from the same collo-clion mixture. These membranes, prepared on glass platesfloated on mercury with exact control of reagents, tem-perature and time, were of a reproducible porosity, asjudged by the filtration rates for distilled water and re-tention of Bence-Jones protein. The membranes werestored in distilled water to which a few thymol crystalswere added, and urine specimens from at least one normalsubject were examined with membranes from each batch.
Ultrafiltration was conducted in the cold room at 3 to50 C. Forty-eight hours was required for filtration of anormal 24-hour specimen through a single membrane un-der increasing pressures of 5 to 125 pounds per squareinch. The large quantity of colloidal material contained
1287

WILLIAM H. BOYCE, FRED K. GARVEY, AND CHARLES M. NORFLEET, JR.
in the urine of patients with calculi frequently requiredthree to six membranes for filtration of a 24-hour specimen.
The colloidal residues were removed from the mem-branes as a gel, immediately frozen, and stored until atotal of 72 to 240 hours of continuous urinary output persubj ect had been processed. To insure removal of allsoluble colloids from the membranes, each was shreddedand immersed in 30 ml. of Veronal buffer, ionic strength0.1, pH 8.6, and stored at 1.00 C. In a preliminary seriesof experiments the membranes were dissolved in 15 ml.of ethanol-ether at 0.50 C.; the precepitate was then ex-tracted three times with ethanol-ether, dried with ether,and added to the solid gel obtained above. This proceduredid not appear to have any advantage over.buffer extrac-tion of the membranes.
After completion of the collection period, each 24-hourcolloidal residue was extracted three times with 10 ml.of the buffer used to extract the collodion membrane, andfinally with 10 ml. of fresh buffer. Extraction with molarsodium chloride gave results which were quantitativelyand qualitatively similar to the buffer extracts from thesame individuals. All of the soluble proteins containedin the gel seemed to carry a high concentration of ad-sorbed or bound urinary pigments. These pigments servedas a convenient guide to the completeness of extraction.The pooled extracts of normal urine usually totaled 120to 200 ml. per 72 to 120 hours of urinary excretion.These were concentrated to a volume of 8 ml. by per-evaporation-that is, suspension of the solution in cello-phane bags 15/16 inch wide in a cold air stream at 50 C.Similar results have been obtained by pressure dialysisagainst 2 liters of Veronal buffer, and this technique hasbeen routinely used for subsequent experiments.
The total protein content of a small sample of thedialyzed extract was determined by the biuret method,and the solution was diluted with Veronal buffer to givea resulting protein content of 1 per cent. A final equili-bration dialysis against Veronal buffer of pH 8.6 was madeprior to electrophoretic studies with the Aminco electro-phoresis unit and calibrated cell of 8 ml. capacity. Theproteins were allowed to migrate for 7200 seconds undera potential gradient of 7.4 volts per cm. at 0.50 C. inVerqpal buffer of ionic strength 0.1 and pH 8.6 (10).Photographs were made with the slit diaphragm, cylin-drical lens system, using a red filter and high contrastpanchromatic film.
Samples of urinary proteins from the same patientswere also studied electrophoretically at pH 4.5, by themethod others (8, 11-14) have used for serum proteins.After the proteins had been collected and concentrated inVeronal buffer, they were dialyzed against an acetic acid,sodium acetate buffer of pH 4.5, ionic strength 0.1 (15)for 72 hours. Intermediate dialysis against phosphatebuffers to prevent precipitation was found to be unneces-sary. Electrophoretic migration was studied in the samecell for three to five hours under a potential gradient of6.0 volts per cm. at 0.50 C.
A very small precipitate which formed during the aciddialysis was removed by centrifugation. This precipitate
was much larger in the group of patients with calculousdisease than in the control group. It could not be com-pletely redissolved in Veronal buffer of pH 8.6, but thesoluble portions from five patients and from three normalsubjects were studied electrophoretically in Veronal buf-fer, pH 8.6, ionic strength 0.1, at a potential gradient of7.4 volts per cm. for two hours. The insoluble portiongave a positive Molisch test and was soluble in glycinebuffer of pH 10.
RESULTS
The colloidal gel obtained from normal 24-hourspecimens measured 0.90 to 1.25 ml. in volume.The dry weights of these lyophilized residues fromfive normal subjects averaged 0.0902 Gm. per 24hours, with a range of 0.0865 to 0.0975. In thepatients with calculous disease the lyophilized resi-due averaged 0.496 Gm. per 24 hours, with a rangeof 0.296 to 1.253.
Following extraction with Veronal buffer therewas a considerable residue of gel-like material,which occupied a volume almost as great as theoriginal material. After lyophilization, the dryweights of these residues from five normal sub-jects were in the range of 0.0439 to 0.0448 Gm. per24 hours. On the basis of dry weights it appearsthat approximately 42.6 to 52.7 mg. of the originalgel was extracted by Veronal buffer. The ratioof the insoluble residue to the total colloids wasmuch higher in the group of patients with calculi.Since no component of this gel was soluble inVeronal buffer of pH 8.6 or in acetate buffer of pH4.5, without procedures which modify its molecu-lar structure, further studies of this material willnot be considered in the present report. The larg-est single component of this residue is a conjugateof carbohydrate and protein, which has been sub-jected to electrophoretic, spectroscopic, and bio-chemical analysis. The resulting data are beingprepared for publication.
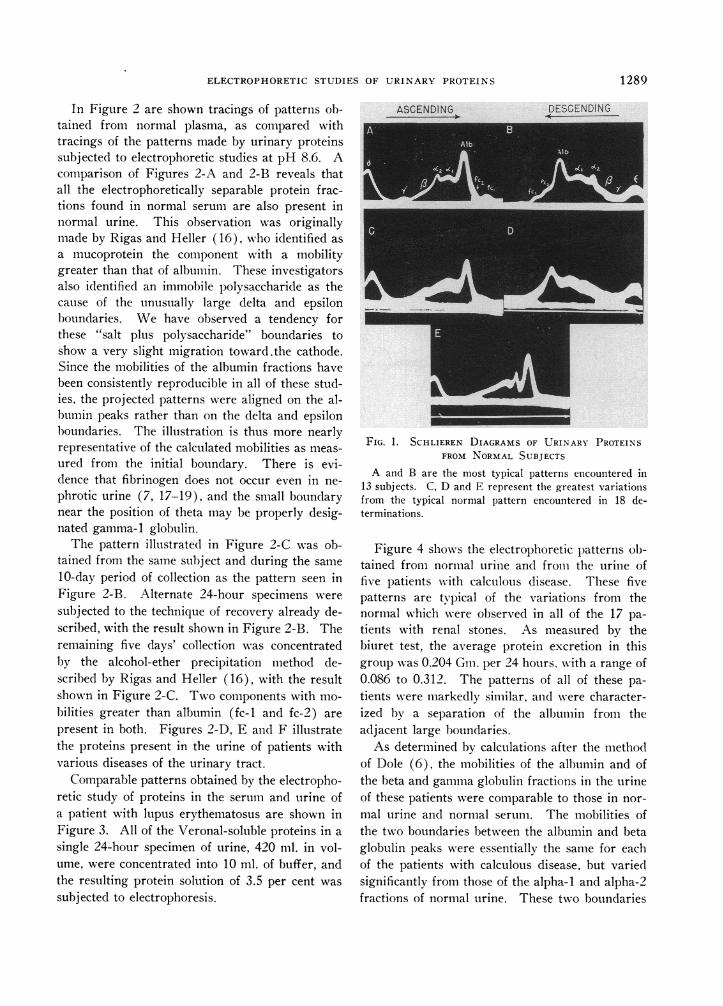
Electrophoretic studies at pH 8.6Figure 1 illustrates the most typical Schlieren
pattern obtained from normal urine, as comparedwith the maximal variations encountered in 18 de-terminations from 13 normal subjects. Thesevariations are in accord with the observations ofRigas and Heller (16), who noted minor varia-tions in the patterns obtained from different indi-viduals, whereas the pattern of a given individualtended to remain constant over several months.
1288
ELECTROPHORETICSTUDIES OF URINARY PROTEINS
In Figure 2 are shown tracings of patterns ob-tained from normal plasma, as compared withtracings of the patterns made by urinary proteinssubjected to electrophoretic studies at pH 8.6. Acomparison of Figures 2-A and 2-B reveals thatall the electrophoretically separable protein frac-tions found in normal serum are also present innormal urine. This observation was originallymade by Rigas and Heller (16), who identified as
a mucoprotein the component with a mobilitygreater than that of albumin. These investigatorsalso identified an immobile polysaccharide as thecause of the unusually large delta and epsilonboundaries. We have observed a tendency forthese "salt plus polysaccharide" boundaries toshow a very slight migration toward.the cathode.Since the mobilities of the albumin fractions havebeen consistently reproducible in all of these stud-ies, the projected patterns were aligned on the al-bumin peaks rather than on the delta and epsilonboundaries. The illustration is thus more nearlyrepresentative of the calculated mobilities as meas-
ured from the initial boundary. There is evi-dence that fibrinogen does not occur even in ne-
phrotic urine (7, 17-19), and the small boundarynear the position of theta may be properly desig-nated gamma-i globulin.
The pattern illustrated in Figure 2-C was ob-tained from the same subject and during the same
10-day period of collection as the pattern seen inFigure 2-B. Alternate 24-hour specimens were
subjected to the technique of recovery already de-scribed, with the result shown in Figure 2-B. Theremaining five days' collection was concentratedby the alcohol-ether precipitation method de-scribed by Rigas and Heller (16), with the resultshown in Figure 2-C. Two components with mo-
bilities greater than albumin (fc-i and fc-2) are
present in both. Figures 2-D, E and F illustratethe proteins present in the urine of patients withvarious diseases of the urinary tract.
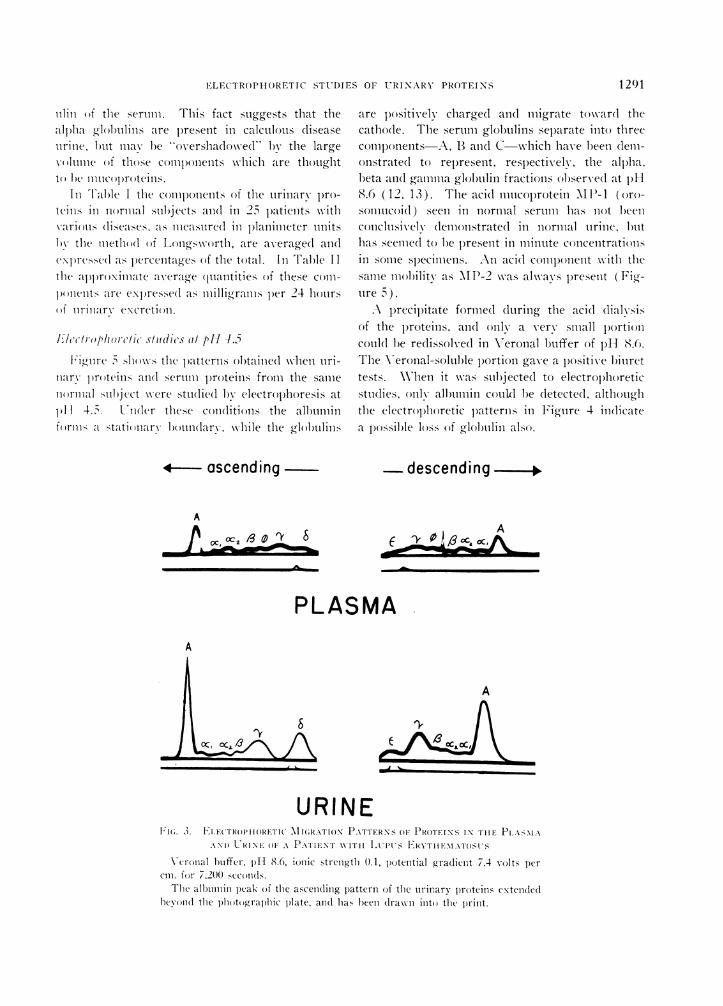
Comparable patterns obtained by the electropho-retic study of proteins in the serum and urine ofa patient with lupus erythematosus are shown inFigure 3. All of the Veronal-soluble proteins in a
single 24-hour specimen of urine, 420 ml. in vol-ume, were concentrated into 10 ml. of buffer, andthe resulting protein solution of 3.5 per cent was
subjected to electrophoresis.
ASCENDING DESCENDING
FIG. 1. SCHLIEREN DIAGRAMS OF URINARY PROTEINSFROM NORMALSUBJECTS
A and B are the most typical patterns encountered in13 subjects. C, D and E represent the greatest variationsfrom the typical normal pattern encountered in 18 de-terminations.
Figure 4 showvs the electrophoretic patterns ob-tained from normal urine and from the urine offive patients with calculous disease. These fivepatterns are typical of the variations from thenormal which were observed in all of the 17 pa-tients with renal stones. As measured by thebiuret test, the average protein excretion in thisgroup was 0.204 Gm. per 24 hours, with a range of0.086 to 0.312. The patterns of all of these pa-tients were markedly similar, and were character-ized bv a separation of the albumin from theadjacent large boundaries.
As determined by calculations after the methodof Dole (6), the mobilities of the albumin and ofthe beta and gammaglobulin fractions in the urineof these patients were comparable to those in nor-mal urine and normal serum. The mobilities ofthe two boundaries between the albumin and betaglobulin peaks were essentially the same for eachof the patients with calculous disease, but variedsignificantly from those of the alpha-1 and alpha-2fractions of normal urine. These two boundaries
1 289

WILLIAM H. BOYCE, FRED K. GARVEY, AND CHARLES M. NORFLEET. JR.
ISS, fasceOI9-.4---'eeire --.
A.
S.
C.
E.
F.
FIG. 2. TRACINGS OF ELECTROPHORETICMIGRATION PATTERNSOF NORMALHUMANPLASMA AND OF URINARY PROTEINS IN HEALTH AND IN THREEDISEASE STATES ACCOMPANIEDBY INCREASED PROTEINURIA
Veronal buffer, pH 8.6, ionic strength 0.1, potential gradient 7.4 volts percm. for 7,200 seconds.
Tracings of the projected patterns are utilized to eliminate inequalities ofexposure which the presence of urinary pigments introduces into the originalphotographs. These inequalities do not impair the usefulness of any singlepattern, but preclude the simultaneous copying of the large number of pat-terns used in this illustration.
together comprised 46.7 per cent of the totalamount of protein in the urine of patients withcalculous disease (Table I). The larger peak hadan average mobility of - 4.81 (± 0.11) x 10-cm.,/volt sec., and the smaller an average of - 3.99(± 0.02) X 10-5 cm.2/volt sec. Dole (6) gives amobility of - 5.07 x 10- cm.2/volt sec. for alpha-1
globulin and - 4.08 x 10-- cm.2/volt sec. foralpha-2 globulin.
In Figures 4-B, 4-C and 6-B a small peak canbe seen between those representing albumin andthe large components of calculous disease urinejust discussed. These small peaks have a cal-culated mobility of the same value as alpha-1 glob-
1290
ELECTROPHORETICSTUDIES OF U'RI NARY PROTEINS
liun of the sertum. This fact suggests that thealjha g'lol)uhnlis are p)resent in calculous diseaseurine, l)ut mav l)e overshadowe(l by the large\ mlinIIe of tIRose components which are thoughtto lbe lnucojprotellns.
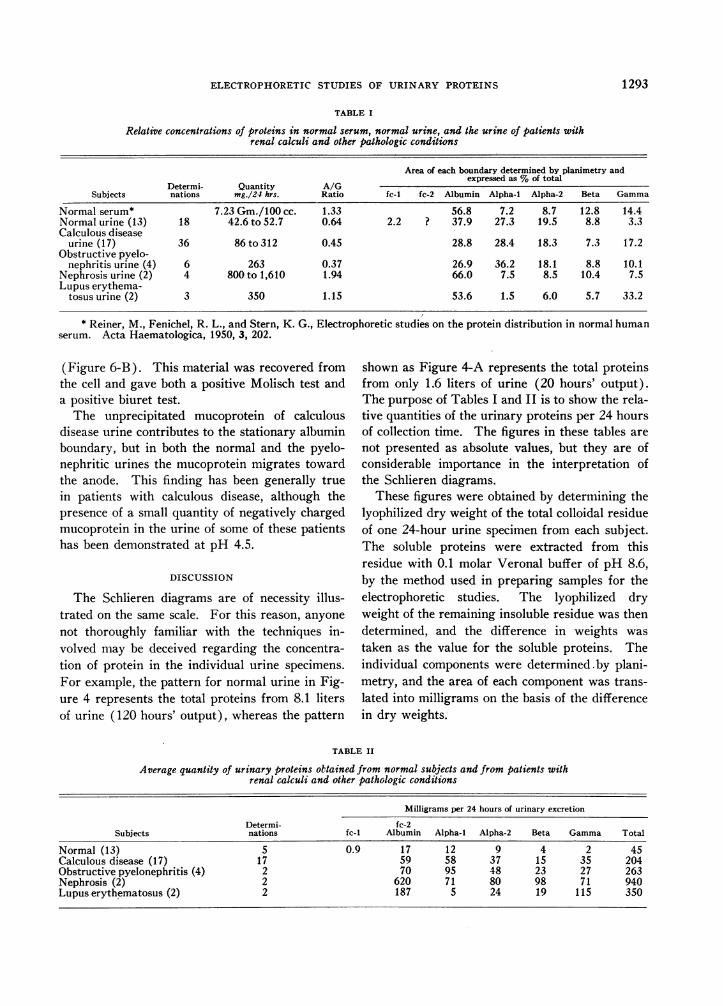
In Table I the components of the urinary pro-teills in normal sub'ject ( in 25 patients withvarimi1 (liSeasIeXS. as mleaIsire(l in l)lanilmeter unitsl)! the metho(d of Loigsworth, are average(l an(l
eNl)rcsse(l as )ercenta(ges of the total. In Table 11the appnroximate average qiantities Of these comn-pmeldts are exl)resse(l as milligramis per 24 hoursof urinary excretion.
U"cchroplihorc/wsic fdl(dM8 (It p11 4.3Rli'o-nre 5 shlows the p)atterns ol)taine(l wxhen uri-
nary proteins and( serunm l)roteins from the samenormial subiect were stutdie(l 1b electrol)horesis at
1)1 1 4. 5. lUnder these conditiOisn the albumillforous a statio nary hootun(larv. while the globuilills
*- ascending
A
Oc, °c2 3 0 86
are positively charged an(l migrate towar(l thecathodle. The seruim globuilins separate into threec0:1ml)on1ents A, B andi C which have heen dem-onstratedl to represent, reslectivelv, the alpha.beta and gammaglobumlin fractions ohserved at p)H8.6 (12, 13). The acid mucoprotein \MP-i (oro-somiucoitd) seen in ncormal seruim hlas not beenconclusively (lemonstratedl in normal tirine, buthas seemed to be l)resent in minuite concentratiOnlsin some sl)ecilmlens. An acidl component with thesame mll()b)ilit- as wIP-was alwas present ( Fi--tire 1i5).
A precipitate formed during the acidl dialvsisof the l)roteins, an(l only a very small l)ortioncould be re(lissolvedl in Veronal buffer of p)H 8.6.The Veronal-soluble p)ortion gave a positive bitirettests. \When it was suhjected to electrophoreticstudies, only allbmin couilkl be dletecte(l. althoughthe electrophoretic l)atterns in Figure 4 indicatea psossible loss of glo)bulin als(o).
descending X
A
PLASMAA
_jLA ~~~~~~~~~cxz, 13j
URINEFI;. 3. LILECTROPHIIRETIC MIGRATION PATTERNS() PROTEINS IN TIHE Pl.AsM.xAS
.\NIO URINE oF.O PATIENT WITH ILtoPs FRYt-IEM;EN ATI\T(St s
Veronal buffer, plH 8.6, iOnlic strenlgt-th 0.1, p)otential g-radient 7.4 volts percm. fIor ,200 seconds.
The alnnlnn 1)eak Of the ascending p)attern of the nriliary proteins extendedbeolod the photographic plate, and has been dlrawn into the print.
1291

12WILLIA'M H. BOYCE, FRED K. (GARVEY, AND CHARLES M.\T. NORFLEET, JR.
*-oscendingq . - descending
E-P
1i1(;. 4. TRACINGS OF ELECTROPOIIDRETIC MIGRATION PATTERNS OF LRIN ARY
PROTEINS IN HEA.\TlI AND IN CALcU.0os DISEASE
Veronal buffer. pH 8.6. ilonic strength 0.1, l)otential gradient 7.4 volts per
cm. fOr 7/200 SCCoI1(lS.
In a p)reop)erative study of the l)atient with a functioning adeilomila of the
larathyroid glan(l (4-C), a 24-hour specimen of urine contained 180 mg. ofproteilns.
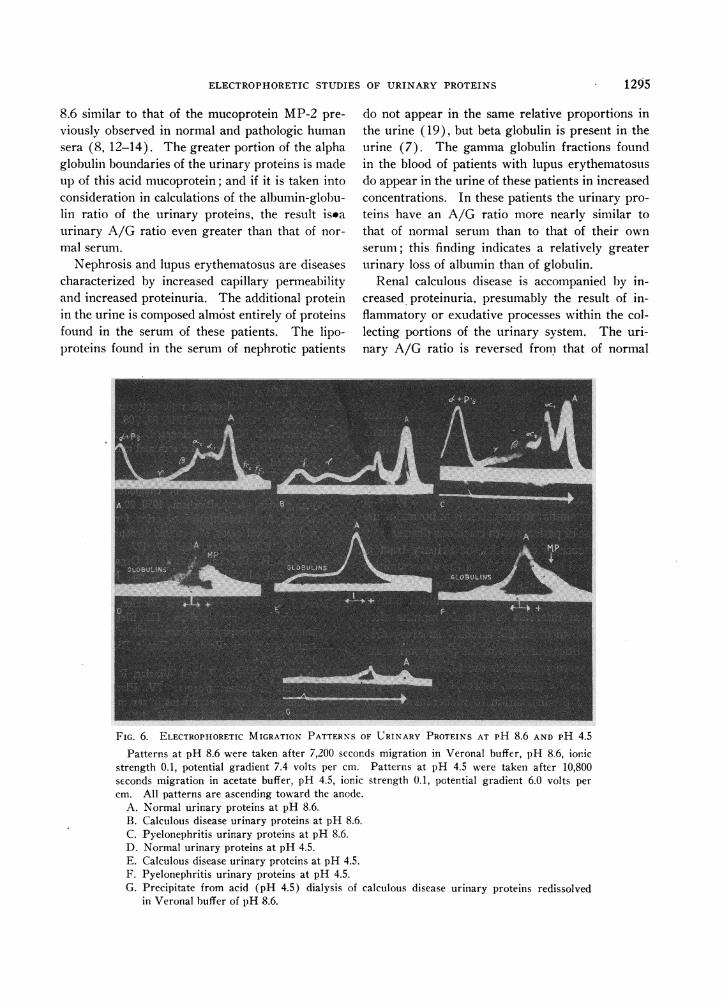
In Figure 6 the electroplhoretic lpatterns froninormal tirine and from the tirine of patients withcalculous dlisease ali(l chironiic pyelonepliritis are
compl)aredl at pH 8.6 and 4.5. For the purlpC)ose ofthis illustration the proteins were recovered fromthe cell followingy studies at pH 8.6, concentrated
to the original volume, an(l dlialyze(l to a p-H of 4.5.The l)recip)itate which occurred in every case wvas
coml)ose(l primarily of a polysaccharide ( Alolischtest ) which was immllobile at pH 8.6. In the nor-
ial anld peloneelIiritic urines the only other (le-tectable comIponent of the precipitate was a very
small anmount of all)umin. In the urine of l)atients
with calculous disease the precipitate coutaimei a
relatively greater concentration of the muco-
l)rotein thau of albumin ( Figure 6-G) -Note that.although the precipitated albl umin retains the nor-
Dial mobility for all)bumin at pH 8.6. the miobl)ilitvof the precil)itatecl mucoprotein is even less thanit was in the original tleteriiiinatioii at p1H- 8.6
,1 0 r 6.Ps
1 292
ELECTROPHORETICSTUDIES OF URINARY PROTEINS
TABLE I
Relative concentrations of proteins in normal serum, normal urine, and the urine of patients withrenal calculi and other pathologic conditions
Area of each boundary determined by planimetry andexpressed as %of total
Determi- Quantity A/GSubjects nations mg./24 hrs. Ratio fc-l fc-2 Albumin Alpha-1 Alpha-2 Beta Gamma
Normal serum* 7.23 Gm./100 cc. 1.33 56.8 7.2 8.7 12.8 14.4Normal urine (13) 18 42.6 to 52.7 0.64 2.2 ? 37.9 27.3 19.5 8.8 3.3Calculous disease
urine (17) 36 86to312 0.45 28.8 28.4 18.3 7.3 17.2Obstructive pyelo-
nephritis urine (4) 6 263 0.37 26.9 36.2 18.1 8.8 10.1Nephrosis urine (2) 4 800 to 1,610 1.94 66.0 7.5 8.5 10.4 7.5Lupus erythema-
tosus urine (2) 3 350 1.15 53.6 1.5 6.0 5.7 33.2
* Reiner, M., Fenichel, R. L., and Stern, K. G., Electrophoretic studies on the protein distribution in normal humanserum. Acta Haematologica, 1950, 3, 202.
(Figure 6-B). This material was recovered fromthe cell and gave both a positive Molisch test anda positive biuret test.
The unprecipitated mucoprotein of calculousdisease urine contributes to the stationary albuminboundary, but in both the normal and the pyelo-nephritic urines the mucoprotein migrates towardthe anode. This finding has been generally truein patients with calculous disease, although thepresence of a small quantity of negatively chargedmucoprotein in the urine of some of these patientshas been demonstrated at pH 4.5.
DISCUSSION
The Schlieren diagrams are of necessity illus-trated on the same scale. For this reason, anyone
not thoroughly familiar with the techniques in-volved may be deceived regarding the concentra-tion of protein in the individual urine specimens.
For example, the pattern for normal urine in Fig-ure 4 represents the total proteins from 8.1 litersof urine (120 hours' output), whereas the pattern
shown as Figure 4-A represents the total proteinsfrom only 1.6 liters of urine (20 hours' output).The purpose of Tables I and II is to show the rela-tive quantities of the urinary proteins per 24 hoursof collection time. The figures in these tables are
not presented as absolute values, but they are ofconsiderable importance in the interpretation ofthe Schlieren diagrams.
These figures were obtained by determining thelyophilized dry weight of the total colloidal residueof one 24-hour urine specimen from each subject.The soluble proteins were extracted from thisresidue with 0.1 molar Veronal buffer of pH 8.6,by the method used in preparing samples for theelectrophoretic studies. The lyophilized dryweight of the remaining insoluble residue was thendetermined, and the difference in weights was
taken as the value for the soluble proteins. Theindividual components were determined-by plani-metry, and the area of each component was trans-lated into milligrams on the basis of the differencein dry weights.
3LE II
Average quantity of urinary proteins obtained from normal subjects and from patients withrenal calculi and other pathologic conditions
Milligrams per 24 hours of urinary excretion
Determi- fc-2Subjects nations fc-1 Albumin Alpha-i Alpha-2 Beta Gamma Total
Normal (13) 5 0.9 17 12 9 4 2 45Calculous disease (17) 17 59 58 37 15 35 204Obstructive pyelonephritis (4) 2 70 95 48 23 27 263Nephrosis (2) 2 620 71 80 98 71 940Lupuserythematosus (2) 2 187 5 24 19 115 350
1293

WILLIAM H. BOYCE, FRED K. GARVEY, AND CHARLES M. NORFLEET, JR.
FIG. 5. ELECTROPHORETICMIGRATION PATTERNSOF NORMALSERUMAND OF NORMALURINARYPROTEINS AT PH 4.5
Slit diaphragm, cylindrical lens patterns of boundaries ascending toward the anode. Acetatebuffer, pH 4.5, ionic strength 0.1, potential gradient 6.2 volts per cm.
A. Urinary proteins at 3,600 seconds.B. Serum proteins at 3,600 seconds.C. Urinary proteins at 10,800 seconds.D. Serum proteins at 10,800 seconds. MP-1 has migrated beyond the photographic range.
Certain errors are obviously inherent in thistechnique. The polysaccharide, which contributedto the total weight of the soluble material, is im-mobile at pH 8.6 and is not included in the plani-metric studies, since a variable portion of this re-fractive gradient (E + Ps in Figure 4) is also dueto the epsilon "salt" boundary. Inspection of thepatterns will demonstrate that planimetric separa-tion of the individual gradients is much more ar-bitrary in studies of these urinary proteins than incomparable studies of serum proteins. Further-more, the overlap of fc-2 and albumin gradientsmade it desirable to express these values as a singlesum (Tables I and II).
There are two components of normal urinewhose electrophoretic mobilities at pH 8.6 aregreater than that of albumin. The urinary muco-protein recovered by Tammand Horsfall (20) iselectrophoretically homogeneous at pH 6.8 and
8.6 (21), and has a mobility slightly greater thanthat of human serum albumin (22). This muco-protein is insoluble in molar sodium chloride., butit is possible that it may have a limited solubilityin the 0.1 molar Veronal buffer used for extractionin our experiments. The refractive gradient fc-2may therefore represent the mucoprotein of Tammand Horsfall. Since these authors obtained a yieldof 0.025 Gm. of mucoprotein per liter of urine, itis obvious that fc-2 (Figures 1, 2, 6) is only a por-tion of the total quantity of this mucoprotein pres-ent in the 72- to 120-hour urine specimens repre-sented by these Schlieren patterns. This findingwould be in accord with the limited solubility ofthis material in 0.1 and 0.025 molar buffers (20).
The large alpha globulin boundaries in normalurine at pH 8.6 are composed not only of thealpha globulins of serum but also of an acid pro-tein. This protein has a mobility at pH 4.5 and
1294
ELECTROPHORETICSTUDIES OF URINARY PROTEINS
8.6 similar to that of the mucoprotein MP-2 pre-viously observed in normal and pathologic humansera (8, 12-14). The greater portion of the alphaglobulin boundaries of the urinary proteins is madeup of this acid mucoprotein; and if it is taken intoconsideration in calculations of the albumin-globu-lin ratio of the urinary proteins, the result iseaurinary A/G ratio even greater than that of nor-mal serum.
Nephrosis and lupus erythematosus are diseasescharacterized by increased capillary permeabilityand increased proteinuria. The additional proteinin the urine is composed almost entirely of proteinsfound in the serum of these patients. The lipo-proteins found in the serum of nephrotic patients
do not appear in the same relative proportions inthe urine (19), but beta globulin is present in theurine (7). The gamma globulin fractions foundin the blood of patients with lupus erythematosuisdo appear in the urine of these patients in increasedconcentrations. In these patients the urinary pro-teins have an A/G ratio more nearly similar tothat of normal serum than to that of their ownserum; this finding indicates a relatively greaterurinary loss of albumin than of globulin.
Renal calculous disease is accompanied by in-creased proteinuria, presumably the result of in-flammatory or exudative processes within the col-lecting portions of the urinary system. The uri-nary A/G ratio is reversed from that of normal
FIG. 6. ELECTROPHORETICMIGRATION PATTERNSOF URINARY PROTEINS AT PH 8.6 AND PH 4.5
Patterns at pH 8.6 were taken after 7,200 seconds migration in Veronal buffer, pH 8.6, ionicstrength 0.1, potential gradient 7.4 volts per cm. Patterns at pH 4.5 were taken after 10,800seconds migration in acetate buffer, pH 4.5, ionic strength 0.1, potential gradient 6.0 volts percm. All patterns are ascending toward the anode.
A. Normal urinary proteins at pH 8.6.B. Calculous disease urinary proteins at pH 8.6.C. Pyelonephritis urinary proteins at pH 8.6.D. Normal urinary proteins at pH 4.5.E. Calculous disease urinary proteins at pH 4.5.F. Pyelonephritis urinary proteins at pH 4.5.G. Precipitate from acid (pH 4.5) dialysis of calculous disease urinary proteins redissolved
in Veronal buffer of pH 8.6.
1295

WILLIAM H. BOYCE, FRED K. GARVEY, AND CHARLES M. NORFLEET, JR.
serum, because the urine contains two componentswhich have mobilities slightly less than the alphaglobulins. These two components are isoelectric atpH 4.5, where they tend to precipitate spontane-ously and to contribute to the stationary albuminboundary. Whether these are structural modifica-tions of the alpha fractions of normal urine or are
entirely different substances peculiar to the urinein calculous disease remains at present unknown.The observed alteration in the mobility of thesealpha boundaries (Figures 2 and 4) may be dueto the fact that, in patients with calculous disease,the relative concentrations of these and othercomponents of urine differ from those found innormal subjects (Table II). Studies are now inprogress to isolate and identify further these com-
ponents from both normal urine and the urine ofpatients with calculous disease.
Obstruction of the urinary tract, with resultantbacterial infection, may persist in some individualsfor prolonged periods of time without the formationof calculi. The electrophoretic patterns of theurinary proteins from such patients contain thenegatively charged component (MP-2) at pH 4.5,and are more similar to the patterns of normal urinethan to those of patients with calculous disease.
The presence of calculi in the urinary tract isnot considered to be the cause of the abnormalitiesobserved in the urinary proteins. Four of the pa-
tients in this series have been examined one tothree times at intervals of 3 to 14 months aftersurgical removal of all the calculi. In every case
the abnormalities observed in the preoperative ex-
aminations were present in the follow-up exami-nations. It is recognized, however, that such pa-
tients have a predisposition to recurrent calculusformation, and the presence of developing or un-
recognized stones cannot be excluded at the pres-
ent time.
SUMMARY
The total quantity of proteins and other particlesof colloidal size in the urine of patients with calcu-lous disease is 3 to 13 times greater than that innormal urine. Electrophoretic studies of thosecomponents soluble in buffers of pH 4.5 and 8.6have demonstrated consistent variations in theproteins from the urine of patients with calculous
disease as compared with normal urine. Thesevariations have been most apparent in the "alpha"fractions.
REFERENCES
1. Boyce, W. H., Chemical analysis of four hundredurinary calculi. Unpublished data.
2E Colby, F. L., Essential Urology, 2nd ed., Baltimore,Williams & Wilkins, 1953, pp. 195.
3. Wardlaw, H. S. H., Observations on the incidenceand composition of urinary calculi. M. J. Australia,1952, 1, 180.
4. Howard, J. E., Some current concepts on the mecha-nism of calcification. J. Bone & Joint Surg., 1951,33-A, 801.
5. Rubin, P. S., and Howard, J. E., Histochemical stud-ies on the role of acid mucopolysaccharides in cal-cifiability and calcification. Trans. Second Con-ference on Metabolic Interrelations, Reifenstein,E. C., ed., New York, Josiah Macy, Jr. Founda-tion, 1950, p. 155.
6. Dole, V. P., The electrophoretic patterns of normalplasma. J. Clin. Invest., 1944, 23, 708.
7. Longsworth, L. G., and MacInnes, D. A., An electro-phoretic study of nephrotic sera and urine. J. Ex-per. Med., 1940, 71, 77.
8. Miller, G. L., Miller, E. E., and Eitelman, E. S., ThepH-mobility relationships of components of hu-man plasma. Arch. Biochem., 1950, 29, 413.
9. Gorbman, A., Ultrafiltration of urine for collectionand biological assay of excreted hypophyseal hor-mones. Endocrinolgy, 1945, 37, 177.
10. Moore, D. H., Physical Methods of Organic Chem-istry, 2nd ed., Weissberger, A., ed., New York,Interscience Publishers, 1949, vol. I, p. 1703.
11. Mehl, J. W., Humphrey, J., and Winzler, R. J., Mu-coproteins of human plasma. III. Electrophoreticstudies of mucoproteins from perchloric acid fil-trates of plasma. Proc. Soc. Exper. Biol. & Med.,1949, 72, 106.
12. Mehl, J. W., Golden, F., and Winzler, R. J., Muco-proteins of human plasma. IV. Electrophoreticdemonstration of mucoproteins in serum at pH 4.5.Proc. Soc. Exper. Biol. & Med., 1949, 72, 110.
13. Mehl, J. W., and Golden, F., Electrophoretic stud-ies of human serum at pH 4.5. J. Clin. Invest.,1950, 29, 1214.
14. Petermann, M. L., and Hogness, K. R., Electro-phoretic studies on the plasma proteins of pa-tients with neoplastic disease. II. An acid proteinpresent in the plasma. Cancer, 1948, 1, 104.
15. Miller, G. L., and Golder, R. H., Buffers of pH 2 to12 for use in electrophoresis. Arch. Biochem.,1950, 29, 420.
16. Rigas, D. A., and Heller, C. G., The amount andnature of urinary proteins in normal human sub-jects. J. Clin. Invest., 1951, 30, 853.
1296
ELECTROPHORETICSTUDIES OF URINARY PROTEINS
17. Blackman, S. S., and Davis, B. D., Electrophoreticand chemical analysis of protein in nephrotic urine.J. Clin. Invest., 1943, 22, 545.
18. Farnsworth, E. B., and Ruppenthal, N. C., Electro-phoretic studies on serum and urine proteins innephrosis treated with ACTH. J. Lab. & Clin.Med., 1951, 38, 407.
19. Slater, R. J., and Kunkel, H. G., Filter paper electro-phoresis with special reference to urinary proteins.J. Lab. & Clin. Med., 1953, 41, 619.
20. Tamm, I., and Horsfall, F. L., Jr., A mucoprotein de-rived from human urine which reacts with influ-enza, mumps, and Newcastle disease viruses. J.Exper. Med., 1952, 95, 71.
21. Perlmann, G. E., Tamm, I., and Horsfall, F. L., Jr.,An electrophoretic examination of a urinary mu-coprotein which reacts with various viruses. J.Exper. Med., 1952, 95, 99.
22. Perlmann, G. E., Personal communication.
ERRATUM
A Possible Fourth Plasma Thromboplastin Component, by TheodoreH. Spaet, Paul M. Aggeler, and Beverly G. Kinsell, J. Clin. Invest.,1954, 33, 1095. Table V.
The item, "5%7 normal plasma + PTA-deficient blood" shouldread "5% normal -plasma + PTC-deficient blood."
SPECIAL NOTICE TO SUBSCRIBERS
Post Offices will no longer forward the Journal when you move.
Please notify The Journal of Clinical Investigation, BusinessOffice, 622 West 168th Street, New York 32, N. Y. at once whenyou have a change of address, and do not omit the zone number ifthere is one.
1297