VENOUS THROMBOEMBOLISM( VTE ) DEEP VENOUS THROMBOSIS ( DVT ) PULMONARY THROMBOEMBOLISM( PTE )

9/23/19
1
Outpatient Management of Venous Thromboembolism (VTE)
Cari Batcheler, PharmD, BCPSClinical Pharmacy Specialist – Emergency Medicine
UnityPoint Health – St Luke’s HospitalCedar Rapids, Iowa
Disclosure
• No Conflicts of Interest
Objectives
EvaluateEvaluate primary literature to support outpatient management of VTE
DiscussDiscuss advantages and disadvantages of each direct oral anticoagulant
UtilizeUtilize prognostic models to determine disposition for patients with pulmonary embolism
Describe Describe outpatient treatment regimens for VTE
Topics Covered
Outpatient treatment regimens Disposition
Topics Not Covered
DiagnosisLaboratory tests
Imaging
Inpatient managementThrombolysis
Heparin infusions
Special populationsPregnancy
Cancer
Patient Case• 49 year old male presents with chest pain and shortness of breath
• No significant past medical history
• Family history of factor V Leiden mutation
• BP 132/80 mmHg
• Pulse 80 beats per minute
• Temp 36.4 OC
• RR 18
• SpO2 97% on room air
• CBC and within normal limits except serum creatinine = 1.18 mg/dL
• Troponin <0.02 ng/mL
• CTA of chest showed bilateral pulmonary emboli with no evidence of right ventricular dysfunction

9/23/19
2
Burden of VTE
• Venous thromboembolism (VTE) affects 900,000 people each year• Includes deep vein thrombosis (DVT) and pulmonary
embolism (PE)• 100,000 die of PE annually• Mortality rates of PE with shock exceed 30%
• 30-day morality rate of low-risk PE is less than 1%
Beckman MG, et al. Am J Prev Med. 2010;38(4 Suppl):S495-501.Kasper W, et al. J Am Coll Cardiol. 1997;30(5):1165-71.Beam DM, et al. Acad Emerg Med. 2015;22(7):788-95.
Phases of VTE Treatment
Initial Phase• First 7 days
Long Term Phase• 7 days to 3 months
Extended Phase• Beyond 3 months
Kearon C, et al. Chest. 2016;149(2):315-352.
Choice of Therapy
In patients with DVT of the leg or PE and no cancer, as long-term (first 3 months) anticoagulant
therapy, we suggest dabigatran, rivaroxaban, apixaban, or edoxaban over vitamin K antagonist (VKA) therapy.
Kearon C, et al. Chest. 2016;149(2):315-352.
Advantages of Direct Oral Anticoagulants (DOACs)
Predictable pharmacokinetics
and pharmacodynamics
Few drug and food interactions
No dietary restrictions
Rapid onset and offset
Short half-life Less laboratory monitoring
Wide therapeutic window
No need for parenteral
anticoagulation*
Mekaj YH, et al. Ther Clin Risk Manag. 2015;11:967-77.
Disadvantages of DOACs
No standardized test for monitoring
Rapid offset and short half-life
Antidotes costly and not widely available
High cost
More difficult to monitor compliance
Mekaj YH, et al. Ther Clin Risk Manag. 2015;11:967-77.
DOAC Dosing for VTE Treatment
Drug Dose Trial
Apixaban 10mg twice daily for 7 days, then 5mg twice daily AMPLIFYa
Dabigatran Parenteral anticoagulation for 5-10 days, then 150mg twice daily RE-COVERb,c
Edoxaban Parenteral anticoagulation for 5-10 days, then 60mg once daily Hokusai-VTEd
Rivaroxaban 15mg twice daily for 3 weeks (21 days), then 20mg once daily EINSTEINe,f
a. Agnelli G, et al. N Engl J Med. 2013;369:799-808; b. Schulman S, et al. N Engl J Med. 2009;361:2342-2352; c. Schulman S, et al. Circulation.2014;129:764-772; d. Hokusai-VTE Investigators. N Engl J Med. 2013;369:1406-1415; e. EINSTEIN Investigators. N Engl J Med. 2010;363:2499-510; f. EINSTEIN–PE Investigators. N Engl J Med. 2012;366:1287-1297.

9/23/19
3
Choice of AnticoagulantFactor Preferred Agent(s) Agent(s) to AvoidParenteral therapy to be avoided
Rivaroxaban, apixaban Dabigatran, edoxaban, VKA
Once daily oral therapy preferred
Rivaroxaban, edoxaban, VKA Apixaban, dabigatran
Liver disease and coagulopathy LMWH DOACs, VKA
Renal disease and creatinine clearance <30 mL/min
VKA, apixaban*Dabigatran, edoxaban, rivaroxaban
Coronary artery disease VKA, rivaroxaban, apixaban, edoxaban
Dabigatran
Dyspepsia or history of GI bleeding
VKA, apixaban Dabigatran
Poor compliance VKA Dabigatran
Kearon C, et al. Chest. 2016;149(2):315-352.
DOAC Elimination
Galgani A, et al. Front Neurol. 2018;9:1067.
DOAC Drug Interactions
Dalal J, et al. Indian Heart J. 2015;67 Suppl 2:S13-34.
Extended Treatment of VTE
Drug Dose TrialApixaban 2.5mg BID AMPLIFY-EXTa
Dabigatran 150mg BID RE-MEDY & RE-SONATEb
Edoxaban 60mg daily Hokausi-VTEc
Rivaroxaban 10mg daily EINSTEIN-EXTd
a. Agnelli G, et al. N Engl J Med. 2013;368:699-708.b. Schulman S, et al. N Engl J Med. 2013;368:709-718.c. Raskob G, et al. Lancet Haematol. 2016;3(5):e228-36.d. EINSTEIN Investigators, et al. N Engl J Med. 2010;363:2499-2510.
DOAC Monitoring
Baseline CMP, CBC, and coagulation
studies
Repeat at least annually
Routine coagulation testing not required
Disposition
In patients with low-risk PE and whose home
circumstances are adequate, we suggest treatment at home or early discharge over standard discharge
(e.g., after the first 5 days of treatment).
Kearon C, et al. Chest. 2016;149(2):315-352.

9/23/19
4
Rates of Discharge Home
• Outpatient treatment for DVT is the standard of care
• Prevalence of discharge home for PE patients is low• 1 to 8%
Vinson DR, et al. Ann Intern Med. 2018;169(12):855-865.
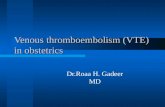
Home Treatment of
PE
983 emergency department patients with
pulmonary embolism
746 patients potentially eligible for outpatient
treatment
13 patients (1.7%) treated at home
733 patients (98.3%) admitted to the hospital
237 considered ineligible for
outpatient treatment
Stein PD, et al. Am J Med. 2016;129(9):974-7.
Benefits of Outpatient Treatment
Cost savings
Patient preference
Conservation of resources
Avoid risks associated with inpatient care
Vinson DR, et al. Ann Intern Med. 2018;169(12):855-865.
Risks of Hospitalization
Patients with low-risk PE who were admitted to the hospital were 8 times more likely to develop a hospital acquired condition• 13.3% vs 1.5% (95% CI: 3.77-19.94)
Bacterial pneumonias were also more common in hospitalized patients
• 11.7% vs 5.9% (95% CI: 1.24-3.23)
Among long LOS patients, hospital acquired conditions (52) exceeded adverse PE events (14 recurrent DVT, 5 bleeds)
Wang L, et al. PLoS ONE. 2017;12(10):e0185022.
Criteria for Outpatient Treatment of PE
Clinically stable with good
cardiopulmonary reserve
No contraindications
to anticoagulation
Recent bleeding
Severe renal or liver disease
Severe thrombocytopenia
(i.e. <70,000/mm3)
Expected to be compliant with treatment
Feels well enough to be treated at home
Kearon C, et al. Chest. 2016;149(2):315-352.
Contraindications to Outpatient Treatment
Right ventricular dysfunction
Elevated troponin Hemodynamically unstable
Oxygen requirement
Kearon C, et al. Chest. 2016;149(2):315-352.

9/23/19
5
Timeline
PESI Score developed
2005
Hestia Criteria developed
2011
PESI Score validated for outpatient use
2011
Rivaroxaban approved for treatment of VTE
2012
Apixaban and dabigatran approved for treatment of VTE
2014
Edoxaban approved for treatment of VTE
2015
Beam, et al.
2015
Roy, et al.
2017
Mercury PE and eSPEED
2018
HoT-PE
2019
Hestia Study
• First published by Zondag and colleagues in 2011• Objective: to evaluate the efficacy and safety of
outpatient treatment of selected patients with acute pulmonary embolism• Prospective cohort study included 297 patients with PE• Enrolled subjects from May 2008 to April 2010• Treated with LMWH and VKA• Discharged immediately from the ED or admitted for less
than 24 hours (23%)
Zondag W, et al. J Thromb Haemost. 2011;9(8):1500-7.
Adapted Hestia Criteria
• Hemodynamically unstable by clinician judgement• Thrombolysis or embolectomy needed• Active bleeding or high risk for
bleeding• GI bleeding or surgery ≤2 weeks ago• Stroke ≤1 month ago• Bleeding disorder or platelet count
<75,000/mm3
• Uncontrolled hypertension (SBP >180 or DBP >110)
• Oxygen needed to maintain SaO2 >90%• PE diagnosed while on anticoagulation• Requiring IV pain medication• Medical or social reason for admission• Creatinine clearance <30 mL/min• Severe liver impairment• Known history of heparin induced
thrombocytopenia• Pregnant
Zondag W, et al. J Thromb Haemost. 2011;9(8):1500-7.
Hestia Study Results
• 2% of patients had recurrent VTE during the 3
month follow-up period
• 95% CI: 0.8 – 4.3%
• No fatal VTE events
• 0.7% of patients had a major bleeding episodes
• 95% CI: 0.08 – 2.4%
• One fatal intracranial bleed
• 5.1% of patients had clinically relevant non-
major bleeding
• 95% CI: 2.9 – 8.2%
Zondag W, et al. J Thromb Haemost. 2011;9(8):1500-7.
Hestia Study Conclusion
Patients with PE selected for outpatient treatment with predefined criteria can be treated with anticoagulants on an outpatient basis
Subsequently validated by multiple studies
Zondag W, et al. J Thromb Haemost. 2011;9(8):1500-7.
Patient Case• 49 year old male presents with chest pain and shortness of breath
• No significant past medical history
• Family history of factor V Leiden mutation
• BP 132/80 mmHg
• Pulse 80 beats per minute
• Temp 36.4 OC
• RR 18
• SpO2 97% on room air
• CBC and CMP within normal limits except serum creatinine = 1.18 mg/dL
• Troponin <0.02 ng/mL
• CTA of chest showed bilateral pulmonary emboli with no evidence of right ventricular dysfunction

9/23/19
6
Patient Case
Is this patient a candidate for outpatient treatment?
Yes 0% mortality in 90 days
2% incidence of VTE recurrence
Is this patient considered low risk based on the Hestia Criteria?
Yes
Pulmonary Embolism Severity Index (PESI)• Originally published by Aujesky and colleagues in 2005 • Retrospective cohort study from 2000 to 2002• Inpatients >18 years old • Primary or secondary diagnosis of PE
• 15,531 patients from 186 hospitals were identified• 10,354 (67%) randomly selected for derivation• 5,177 (33%) for internal validation
• Logistic regression analysis used to identify 11 criteria that were associated with 30-day mortality
Aujesky D, et al. Am J Respir Crit Care Med. 2005;172(8):1041-6.
PESI CriteriaPredictors Points AssignedAge 1 point per yearMale sex 10Cancer 30Heart failure 10Chronic lung disease 10Pulse ≥ 100 beats/min 20Systolic blood pressure <100 mmHg 30Respiratory rate >30/min 20Temperature <36 C 20Altered mental status 60Arterial oxygen saturation <90% 20
Aujesky D, et al. Am J Respir Crit Care Med. 2005;172(8):1041-6.
PESI Score Interpretation
PESI Score Class 30 day Mortality Risk0-65 I (very low risk) 0.0-1.6%
76-85 II (low risk) 1.7-3.5%
86-105 III (intermediate risk) 3.2-7.1%
106-125 IV (high risk) 4.0-11.4%
≥125 V (very high risk) 10-24.5%
Aujesky D, et al. Am J Respir Crit Care Med. 2005;172(8):1041-6.
Patient Case
• 59 • 1 point per year (49) + 10 points for male sex
What is the patient’s PESI score?
• Very low risk (Class I)• 0 – 1.6% risk of 30-day mortality
To which class does this score correspond?
PESI Outpatient Validation
Study
• Open-label non-inferiority trial in 19 EDs in Switzerland, France, Belgium, and USA
• Included patients between 2007 and 2010 who • Had been diagnosed with symptomatic PE• Low risk PESI scores (Class I or II)
• Excluded those in shock, hypoxia, or bleeding risk• 334 patients randomized in 1:1 ratio to inpatient or
outpatient treatment• 171 were treated as outpatients• 168 were treated as inpatients
• Everyone got subcutaneous LMWH followed by oral anticoagulation
Aujesky D, et al. Lancet. 2011;378(9785):41-8.

9/23/19
7
PESI Outpatient Validation Study
Demonstrated non-inferiority of outpatient management for recurrent PE and death• 1 patient (0.6%) in each group died within 90 days• 1 (0.6%) outpatient and 0 inpatients had a recurrent PE
Outpatient management also non-inferior to inpatient management for major bleeding up to 14 days
Narrowly missed non-inferiority margin for outpatient management for bleeding to 90 days• 3 (1.8%) outpatients and 0 inpatients had major
bleeding events in 90 days
Aujesky D, et al. Lancet. 2011;378(9785):41-8.
Beam, et al.
Prospective observational study
Two academic emergency departments
Utilized modified Hestia criteria to identify
low risk PE patients
106 patients with VTE
discharged on
rivaroxaban
71 (67%) with DVT
30 (28%) with PE
5 (5%) with DVT and PE
Beam DM, et al. Acad Emerg Med. 2015;22(7):788-95.
Beam, et al.
Patients were followed for a mean of 389 days
No patient developed a recurrent or new VTE
while on therapy
3 patients had VTE recurrence after
completing their prescribed courses of
anticoagulation
No patients had a major bleeding event
Beam DM, et al. Acad Emerg Med. 2015;22(7):788-95.
Beam, et al. Limitations
Observational study Small sample size
No control group Duration of anticoagulation not
disclosed
Beam DM, et al. Acad Emerg Med. 2015;22(7):788-95.
Beam, et al. Conclusions
Low-risk ED patients with deep vein thrombosis and pulmonary
embolism can be treated at home with a low rate of venous thromboembolism recurrence
and low rate of bleeding.
Beam DM, et al. Acad Emerg Med. 2015;22(7):788-95.
Roy, et al.
• Retrospective propensity-score matched cohort study• Patients diagnosed with a symptomatic
acute PE between January 2007 and December 2012• Exclusion criteria:
• Age ≤ 18 years• PE diagnosed during hospitalization• Chronic PE• Cardiogenic shock at admission• Thrombolysis, surgery, radiovascular
intervention, or IVC filter placement• No anticoagulation treatment • Follow-up for PE outside the Ottawa Hospital
Roy PM, et al. J Thromb Haemost. 2017;15(4):685-694.

9/23/19
8
Roy, et al.
Patients selected for outpatient treatment were
discharged home from the ED and seen within 24 hours
of the diagnosis at a dedicated thrombosis clinic
Follow up at 7–14 days and 90 days
Outpatients defined as those discharged directly from
the emergency room and patients discharged within 48
hours of admission
Outpatients matched to inpatients using propensity
scores
Primary outcome: combination of major bleeding,
recurrent VTE, or all-cause death within 14 days of the
diagnosis of PE
Roy PM, et al. J Thromb Haemost. 2017;15(4):685-694.
Roy, et al. Results
• 583 (51.7%) required hospitalization• 544 (48.3%) were managed as
outpatients• 485 discharged from the emergency
department and 59 discharged within 48 hours
1127 patients included
• Confusion (n = 6)• Nosocomial infection (n = 6)• Falls (n = 2)• Several events (n = 5) • Miscellaneous (n = 9)
During hospitalization,
28 patients (2.5%) had a
serious iatrogenic
event
Roy PM, et al. J Thromb Haemost. 2017;15(4):685-694.
Roy, et al. Results
Inpatients Outpatients P valueCombined events (14 days) 13.0% 3.3% 0.011
Recurrent VTE 1.7% 0.6% 0.135Recurrent VTE + PE related death 9.2% 2.0% 0.026Major bleeding 3.8% 0.0 <0.001All cause mortality 8.2% 2.8% 0.104
Combined events (3 months) 21.7% 6.9% 0.001Recurrent VTE 4.7% 3.6% 0.586Recurrent VTE + PE related death 15.7% 4.8% 0.004Major bleeding 5.9% 0.7% <0.001All cause mortality 16.3% 3.2% 0.005
Roy PM, et al. J Thromb Haemost. 2017;15(4):685-694.
Roy, et al. Conclusions
Hospitalized normotensive patients with acute PE
have a higher risk of recurrent VTE, major bleeding,
or death than patients managed as outpatients
None of the outpatients with a low PESI risk (PESI
class I/II) had recurrence of VTE, major bleeding, or
death during the first 2 weeks after the diagnosis
• 5.1% for hospitalized patients and 0% for outpatients
• P = 0.005
Low-risk patients can be safely managed as
outpatients
Roy PM, et al. J Thromb Haemost. 2017;15(4):685-694.
Mercury PE Study
Randomized, open-label, parallel group, multicenter study
Adult patients presenting to the emergency department with objectively confirmed low risk PE
Low risk PE defined by the absence of any Hestia criteria
Exclusion criteria:Elevated troponinContraindications to anticoagulationBarriers to follow-up
Mercury PE
114 patients randomized in 1:1 ratio to ED discharge on rivaroxaban or standard care
Principal investigators and outcome adjudicators were masked to group assignment
Primary efficacy outcome: time spent in the hospital in the 30 day period after randomization
Primary safety outcome: major bleeding within 90 days
Peacock FW, et al. Acad Emerg Med. 2018;25(9):995-1003.

9/23/19
9
Mercury PE Results
• Mean duration of initial and subsequent hospitalizations for bleeding and/or VTE events within 30 days of randomization was shorter in the rivaroxaban group versus standard of care• 4.8 hours vs 33.6 hours (p<0.0001)• Mean difference in length of stay was 28.8 hours
(95% CI: -41.5 to -16.2)
• No recurrence of VTE or VTE related death within 90 days of randomization for either group
• No differences in bleeding-related hospitalizations or physician visits within 90 days of randomization for rivaroxaban vs standard of care• 3.9% vs 6.3%
Peacock FW, et al. Acad Emerg Med. 2018;25(9):995-1003.
Mercury PE Conclusions
and Limitations
Early discharge on rivaroxaban was associated with a
significant cost savings (~$2,500) compared to standard
care
Standard of care migrated to early discharge on
rivaroxaban throughout the study period
Underpowered to detect differences in safety outcomes
ED admission for a limited period of intravenous
anticoagulation provides little benefit over immediate
ED discharge
Peacock FW, et al. Acad Emerg Med. 2018;25(9):995-1003.
Electronic Support for Pulmonary Embolism Emergency Disposition(eSPEED) Trial
Controlled pragmatic trial from January 2014 to
April 2015
21 emergency departments in Kaiser Permanente system in
Northern California
Included patients 18 years or older with acute
PE
Utilized a clinical decision support system (CDSS) to
assist with disposition decision making
PESI score utilized to guide clinicians
Vinson DR, et al. Ann Intern Med. 2018;169(12):855-865.
eSPEED
1703 patients were included
• 46.9% directly from the ED• 53.1% after a brief observation period (<24 hours)
324 patients were discharged home
• 31.8% versus 21.1% (p = 0.016)
Activation of the CDSS was associated with increased home discharge
• 27.7% to 41.1%
Home discharge increased from pre- to postintervention for low-risk PE
• 12% to 6.2%
Rates of PE-related return visits within 5 days decreased from pre- to postintervention
Vinson DR, et al. Ann Intern Med. 2018;169(12):855-865.
eSPEED Conclusions
Implementation and promotion of an EHR-integrated CDSS safely reduced hospitalization
of ED patients with acute PE
For every 100 ED patients with acute PE, 11 hospitalizations were avoided
Estimated cost reduction of $80,000 per 100 patients
Vinson DR, et al. Ann Intern Med. 2018;169(12):855-865.
HoT-PE
• Prospective multicenter single-arm trial
• Patients with acute low-risk PE without
• Hemodynamic instability
• Right ventricular dysfunction or intracardiac thrombi
• Serious comorbidities
• Utilized adapted Hestia Criteria to exclude patients
• Patients could be admitted for up to 48 hours
• Primary outcome: symptomatic recurrent VTE or PE-
related death within 3 months of enrolment
Barco S, et al. Eur Heart J. 2019;

9/23/19
10
HoT-PE Results
• Study terminated for efficacy after the predefined interim
analysis
• 525 patients included in the pre-planned interim analysis
• Primary efficacy outcome occurred in three patients (0.6%)
• One-sided upper 99.6% CI 2.1%
• One-sided P-value <0.0001
• All three recurrent events presented as non-fatal PE
• 6 of 519 patients (1.2%) in the safety population had a
major bleeding episode
• Two-sided 95% CI 0.4–2.5%
Barco S, et al. Eur Heart J. 2019;
Evidence Summaries• 13 Meta-analysis by Zondag, et al.a
• Included observational studies• 13 studies (1657 patients) with outpatients (discharged <24 hours)• 3 studies (256 patients) with early discharge patients (discharged
within 72 hours) • 5 studies (383 patients) with inpatients
• Incidences of recurrent VTE, major bleeding, and mortality were comparable between the three groups
• Home treatment or early discharge of selected low-risk patients with pulmonary embolism is as safe as inpatient treatment
• 2018 Cochrane Reviewb
• Included 2 randomized control trials (Aujesky 2011 and Mercury PE)
• No evidence of any clear difference between the interventions in overall mortality, bleeding, and recurrence of PE
a. Zondag W, et al. Eur Respir J. 2013;42(1):134-44. b. Yoo HH, et al. Cochrane Database Syst Rev. 2019;3:CD010019.
Cost Savings
If all eligible patients with PE seen in U.S. emergency
departments were treated at home rather than in the
hospital, health care costs would decrease by $1 billion
per year.
Dalen JE, et al. Am J Med. 2016;129:899-900.
Patient Case
• Yes• No contraindications to outpatient
management per Hestia Criteria• Very low risk according to PESI score
Can this patient be safely managed as an
outpatient?
• Apixaban 10mg BID for 7 days, then 5mg BID
• Rivaroxaban 15mg BID for 21 days, then 20mg daily
If the patient prefers not to be treated with parenteral
anticoagulants, which regimens would be
acceptable?
Patient Education
Risks of outpatient treatment
Close return precautions
Signs and symptoms of recurrent VTE
Signs and symptoms of bleeding
Importance of adherence
Avoid NSAIDs
Fall precautions
Alcohol in moderation
Summary
DOACs have revolutionized the management of VTE
Utilize validated prognostic models to risk-stratify patients with PE
Low-risk patients with PE can be safely treated at home