![Improvement of Hepatic and Extrahepatic Complications from ... · disease compared with patients without HCV [10], while substance abuse contributes to viral exposure due to usage](https://static.fdocuments.net/doc/165x107/5f0ab53a7e708231d42cf29a/improvement-of-hepatic-and-extrahepatic-complications-from-disease-compared.jpg)
HCV Extrahepatic manifestations.pdf
26
Extrahepatic Manifestations of Hepatitis C Virus Infection Anna Linda Zignego, MD, PhD a, * , Antonio Craxı`, MD b a Center for Systemic Manifestations of Hepatitis Viruses (MaSVE), Department of Internal Medicine, University of Florence, Viale GB Morgagni 85, 50134 Firenze, Italy b Gastroenterologia and Epatologia, Di.Bi.M.I.S., University of Palermo, Piazza Marina, 34–90133 Palermo, Italy Hepatitis C virus (HCV) is at the same time a hepatotropic and a lympho- tropic virus and may cause hepatic and extrahepatic diseases. Extrahepatic manifestations linked to HCV range from disorders for which a significant association with viral infection is supported by epidemiologic data and by biological plausibility, to anecdotal observations without clear proof of cau- sality. B cell lymphoproliferative disorders (ie, mixed cryoglobulinemia and non-Hodgkin’s lymphoma) are the extrahepatic conditions most closely linked to HCV, having been investigated extensively, and represent a model for both pathogenetic and clinico–therapeutic deductions. An association between HCV infection and other morbid conditions, including dermato- logic, nephrological, neurologic, endocrinologic, cardiocirculatory, and lung disorders also has been suggested. Overlap syndromes characterized by the presence in one patient of manifestations belonging to various path- ologic conditionsdtypically of autoimmune/lymphoproliferative natured would suggest that chronic HCV infection is a distinct systemic disease with a varying spectrum of clinical manifestations. Interferon-based antivi- ral therapy is considered, when feasible, the mainstay of treatment for most HCV-linked extrahepatic diseases. Although its efficacy in curtailing a non- hepatic manifestation after obtaining viral clearance often is seen as a confir- mation of the key pathogenetic role played by HCV, clinical symptoms and viral persistence also may be disjointed, the former persisting even beyond a sustained viral response to therapy. Because of this fact and the intrinsic potential inefficacy of interferon, which in some cases may even exacerbate * Corresponding author. E-mail address: [email protected] (A.L. Zignego). 1089-3261/08/$ - see front matter Ó 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.cld.2008.03.012 liver.theclinics.com Clin Liver Dis 12 (2008) 611–636
-
Upload
sharad-jha -
Category
Documents
-
view
234 -
download
0
Transcript of HCV Extrahepatic manifestations.pdf
Extrahepatic Manifestationsof Hepatitis C Virus Infection
Anna Linda Zignego, MD, PhDa,*,Antonio Craxı, MDb
aCenter for Systemic Manifestations of Hepatitis Viruses (MaSVE), Department
of Internal Medicine, University of Florence, Viale GB Morgagni 85, 50134 Firenze, ItalybGastroenterologia and Epatologia, Di.Bi.M.I.S., University of Palermo, Piazza Marina,
34–90133 Palermo, Italy
Hepatitis C virus (HCV) is at the same time a hepatotropic and a lympho-tropic virus and may cause hepatic and extrahepatic diseases. Extrahepaticmanifestations linked to HCV range from disorders for which a significantassociation with viral infection is supported by epidemiologic data and bybiological plausibility, to anecdotal observations without clear proof of cau-sality. B cell lymphoproliferative disorders (ie, mixed cryoglobulinemia andnon-Hodgkin’s lymphoma) are the extrahepatic conditions most closelylinked to HCV, having been investigated extensively, and represent a modelfor both pathogenetic and clinico–therapeutic deductions. An associationbetween HCV infection and other morbid conditions, including dermato-logic, nephrological, neurologic, endocrinologic, cardiocirculatory, andlung disorders also has been suggested. Overlap syndromes characterizedby the presence in one patient of manifestations belonging to various path-ologic conditionsdtypically of autoimmune/lymphoproliferative naturedwould suggest that chronic HCV infection is a distinct systemic diseasewith a varying spectrum of clinical manifestations. Interferon-based antivi-ral therapy is considered, when feasible, the mainstay of treatment for mostHCV-linked extrahepatic diseases. Although its efficacy in curtailing a non-hepatic manifestation after obtaining viral clearance often is seen as a confir-mation of the key pathogenetic role played by HCV, clinical symptoms andviral persistence also may be disjointed, the former persisting even beyonda sustained viral response to therapy. Because of this fact and the intrinsicpotential inefficacy of interferon, which in some cases may even exacerbate
Clin Liver Dis 12 (2008) 611–636
* Corresponding author.
E-mail address: [email protected] (A.L. Zignego).
1089-3261/08/$ - see front matter � 2008 Elsevier Inc. All rights reserved.
doi:10.1016/j.cld.2008.03.012 liver.theclinics.com

612 ZIGNEGO & CRAXI
extrahepatic conditions, an individualized tailoring of therapy is needed inthese patients.
Classification of extrahepatic manifestations of hepatitis C virus
Extrahepatic manifestations of HCV infection (EHMs-HCV) range fromdisorders for which a significant association with HCV infection is sup-ported clearly by multiple lines of evidence to anecdotal observations with-out clear proof of causality [1,2]. A tentative classification of EHMs-HCV issuggested in Box 1. According to such classification, extrahepatic manifesta-tions of HCV infection are distinguished, taking into account the robustnessof available scientific data. It is thus likely that the nosography of someEHMs-HCV may change over time.
Group A includes EHMs-HCV characterized by a strong associationproven by both epidemiologic and pathogenetic evidence. This category in-cludes B-cell lymphoproliferative disorders (LPDs). Group B includes disor-ders for which a significant association with HCV infection is supported bysubstantial epidemiologic data and groups C and D associations still requireconfirmation and/or a more detailed characterization as opposed to obser-vations that are of similar pathologic nature but of different etiology, or id-iopathic in nature, or only anecdotal (see Box 1).
Hepatitis C virus-related lymphoproliferative disorders
Mixed cryoglobulinemia
Mixed cryoglobulinemia (MC) is a systemic vasculitis caused by deposi-tion of circulating immune complexes in the small vessels and characterizedby multiple organ involvement, mainly skin, peripheral nerves, kidney, andsalivary glands, and less frequently associated with widespread vasculitisand malignant lymphoma [3–6]. The strong association between HCV andMC has been confirmed repeatedly by serologic and molecular investiga-tions [4,6,7]. Generally speaking, cryoglobulinemias are conditions charac-terized by the presence of serum immunoglobulins that become insolublebelow 37�C and can dissolve by warming serum (cryoglobulins, CGs). Ac-cording to Brouet and colleagues [8], CGs are classified on the basis of theirimmunoglobulin composition. In type I, they are composed of a pure mono-clonal component and usually associated with an indolent B-cell lymphoma,and in types II and III mixed CGs, they are composed of a mixture of poly-clonal IgG and monoclonal IgM or polyclonal IgG and polyclonal IgM, re-spectively. In MC, the IgM represents an autoantibody bearing rheumatoidfactor (RF) activity. In type II MC (MC II), the IgM RF molecules mostfrequently display the WA cross-reactive idiotype [9]. MC II accounts for50% to 60%, and type III (MC III) for the remaining 40% to 50% of MC.
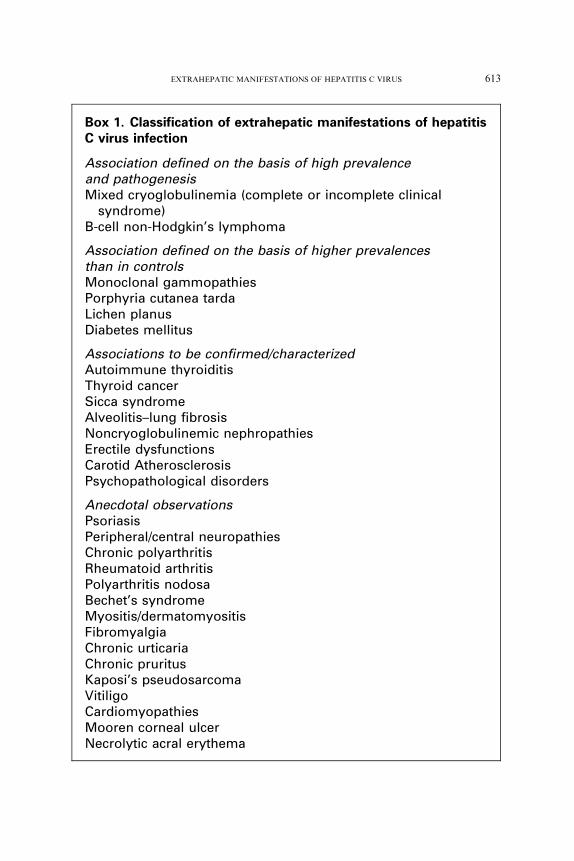
Box 1. Classification of extrahepatic manifestations of hepatitisC virus infection
Association defined on the basis of high prevalenceand pathogenesisMixed cryoglobulinemia (complete or incomplete clinical
syndrome)B-cell non-Hodgkin’s lymphoma
Association defined on the basis of higher prevalencesthan in controlsMonoclonal gammopathiesPorphyria cutanea tardaLichen planusDiabetes mellitus
Associations to be confirmed/characterizedAutoimmune thyroiditisThyroid cancerSicca syndromeAlveolitis–lung fibrosisNoncryoglobulinemic nephropathiesErectile dysfunctionsCarotid AtherosclerosisPsychopathological disorders
Anecdotal observationsPsoriasisPeripheral/central neuropathiesChronic polyarthritisRheumatoid arthritisPolyarthritis nodosaBechet’s syndromeMyositis/dermatomyositisFibromyalgiaChronic urticariaChronic pruritusKaposi’s pseudosarcomaVitiligoCardiomyopathiesMooren corneal ulcerNecrolytic acral erythema
613EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
614 ZIGNEGO & CRAXI
The prevalence of chronic HCV infection in patients who have CGs intheir serum ranges from 19% to more than 50% according to various stud-ies [10,11]. CGs, however, are generally present at low levels, and symptomsare generally absent or mild in chronically HCV-infected patients, whereasclinically overt MC syndrome (MCS) would be evident in 10% to 30% ofMC subjects [10–12].
Serum mixed CGs, high RF values, and reduced C4 values are the mostfrequent laboratory data. The most common symptoms of MCS are weak-ness, arthralgias, and purpura (Meltzer and Franklin triad). Raynaud’s phe-nomenondmicrocirculatory changes of the small vessels of the hands andfeet, identified as color changes in response to colddperipheral neuropathy,sicca syndrome, renal involvement, lung disorders, fever, and cytopeniasalso may be observed [3]. In a recent study involving 231 Italian MC pa-tients, peripheral neuropathy was observed in most cases, representing themost frequent clinical feature after the triad, followed by sicca syndrome,Raynaud phenomenon, and renal involvement [13].
MC-related peripheral neuropathy typically includes mixed neuropathies,which are more often sensitive and axonal. They can manifest themselves assymmetric distal neuropathies, multiple mononeuritis, or mononeuropa-thies. Involvement of the central nervous system is unusual and generallypresents as transient dysarthria and hemiplegia. Pathologic findings showaxonal damage with epineural vasculitic infiltrates and endoneuralmicroangiopathy.
A sicca syndrome (xerostomia and xerophthalmia) caused by involve-ment of salivary and lacrimal glands is recognized in a large proportionof MC patients [14–18]. This syndrome close resembles primary Sjogren’ssyndrome; however it typically lacks antinuclear autoantibodies and antiepi-thelial neutrophil-activating peptide (ENA, SSA/Ro, SSB/La) [13]. Thepathogenetic role of HCV infection in sicca syndrome and the characteris-tics distinguishing classic Sjogren’s syndrome from those associated withHCV remain at issue [19]. It has been proposed that HCV infection is a crite-rion to exclude diagnosis of primary Sjogren’s syndrome, especially if mixedcryoglobulins and hypocomplementemia are present, and anti-SSA/Roantibodies are absent [20].
Significant renal involvement is present in up to one third of patientswho have MC, being observed in about 20% of patients upon clinical pre-sentation of MC and in 35% to 60% of patients over long-term follow-up[13,21]. The most common features at diagnosis are one or more subclin-ical features of renal involvement including microscopic hematuria, pro-teinuria below the nephrotic range (!3 g/24 h), and with normal oronly fairly reduced renal function (creatinine !1.5 mg%). Arterial hyper-tension is observed in up to 80% of cases [22]. In about 20% of patients,proteinuria is in the nephrotic range, and in them a nephrotic syndromemay represent the principal manifestation of MC. About 20% to 30%of cases present with an acute nephritic syndrome as their first renal
615EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
manifestation [4,23]. Presence of a significant renal involvement is amongthe worst prognostic indices in patients who have MC, even when itscourse is variable [13,23]. In a study of 231 patients who had MC, glomer-ulonephritis with subsequent renal failure was the main complication(33%), leading to death during long-term follow-up [13]. The typical his-tologic pattern of renal damage observed in patients who have MC type Iis membranoproliferative glomerulonephritis (MPGN) [13]. The presenceof capillary thrombi, made up of precipitated cryoglobulins and depositsof IgM in capillary loops typically differentiates the cryoglobulinemicform from idiopathic MPGN. In a minority of cases (generally type IIIMC), different pathologic findings have been described (ie, focal and me-sangioproliferative glomerulonephritis and membranous glomerulonephri-tis) [24,25].
The association between MC and severe liver damage has been discussedwidely [1,2,9,26–29]. Several studies have shown an epidemiologic associa-tion between MC and severe liver damage [10,30]. An association betweenMC and liver steatosis also has been suggested [31]. Overall, it seems thatboth MC and the stage of liver damage are more related to a long durationof infection.
The occurrence of MC generally has an important impact on the qualityof life and survival of patients who have MC. Survival analysis according tothe Kaplan-Meier method shows a cumulative 10-year survival, calculatedfrom time of diagnosis, to be significantly lower in patients who have MCas compared with an age- and sex-matched general population. Lowest sur-vival rates were observed in males and in subjects who had renal involve-ment, the main causes of death being nephropathy (33%), malignancies(23%), liver failure (13%), and diffuse vasculitis (13%) [13].
Because of its variable presentation, no standardized criteria for the diag-nosis and staging of MCS are available, even if classifications have been pro-posed [32]. In the presence of purpura, mixed CGs, reduced C4 values, andorgan involvement, the diagnosis of MCS is relatively easy. Quite fre-quently, however, it is suggested by abnormal laboratory data (RF test ormixed CGs or reduced C4 values) with or without mild symptoms like ar-thralgias or asthenia. Moreover, some subjects who have HCV may showclinically evident MCS, though incomplete from a serologic point of view,mainly with the temporary absence of circulating CGs. This may be ex-plained by the difficulty in a proper determination of the presence ofCGs, because of their thermolability and the variability of the rate ofCGs responsible for vasculitic damage [13,33].
Because some mixed CGs are present in low concentrations, the differen-tiation between type II and type III CGs often requires a more sensitivemethod for immunochemical characterization such as electroimmunofixa-tion or Western blot, than conventional immunoelectrophoresis [34]. Severaldata, including the presence of a clonal expansion of B-lymphocytes (BL) inperipheral blood or liver infiltrates [35–38], and the histopathological
616 ZIGNEGO & CRAXI
features of the bone marrow and liver lymphoid infiltrates, confirm the lym-phoproliferative nature of MC. Some studies have shown that:
B-cell clonal expansion (in particular of RF B-cells) underlies MC.This condition is associated with Bcl2/JH rearrangement.MC II can evolve into a frank b-cell non-Hodgkin’s lymphoma (NHL) in
approximately 8% to 10% of cases after a long period of time [13].
From a histopathological point of view, the presence of monoclonal lym-phoproliferation of uncertain significance (MLDUS) in subjects who haveclinico–laboratory features of MC II is typical [33,39–41]. MLDUS repre-sents oligoclonal proliferations of small BL, preferentially located in thebone marrow and liver. In these organs, MLDUS is generally presentwith phenotypic and histologic aspects comparable to indolent B-cell lym-phoma. Further immune–morphologic analysis reveals two different varie-ties: the first and more frequent variety, with analogous features to B-cellchronic lymphatic leukemia (CLL)/small cell lymphoma and a second, lessfrequent, lymphoplasmacytic-like form. The prevalence of these histologicpatterns has varied in different reports [40,42–48].
Lymphoma
HCV-associated lymphoid malignancies can be observed during thecourse of MC or as non-MC related idiopathic forms. About 8% to 10%of MC II evolves into a frank lymphoma [43,49], generally after long-lastinginfection. According to recent data, MC patients had a 35 times higher riskof NHL than the general population [50].
An association between B-cell derived NHL and HCV infection initiallywas suggested by studies performed in populations from southern Europeand the southern United States, [46,51–55], whereas some northern Euro-pean and northern United States or Canadian surveys did not confirma higher prevalence of chronic HCV infection in patients with lymphomathan in the general population [56–61]. During the last decade, many studiesperformed at different latitudesdgenerally larger in size than initial onesdas well as meta-analysis, were able to confirm the existence of such associa-tion, even with a clear south/north gradient of prevalence. These differencesat least partly reflect how HCV is diffuse at different rates in the specificpopulations studied, but also suggest a likely contribution of environmentalor genetic factors [62] to lymphomagenesis.
Although virtually all types of lymphoid malignancy can be found in pa-tients with HCV infection, the strongest association is with B-cell derivedNHL [18,40,51,53,54,63–65]. The use of different classifications presentedin the various studies, however, may confound the evaluation of the actualincidences of each histotype [48,65–67]. Peripheral B-cell derived indolentNHL appears to be the most frequent HCV-associated lymphoma inmany studies. According to the Revised European-American Lymphoma
617EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
(REAL) classification/World Health Organization (WHO) Classification[68,69], the main HCV-related histotypes include B-cell chronic lymphocyticleukemia/small lymphocyte lymphoma, diffuse large B-cell lymphoma, fol-licular lymphoma, lymphoplasmacytic lymphoma, and marginal zone lym-phoma [40]. A recent European multicenter survey suggests a specific roleof HCV infection in the pathogenesis of diffuse large B-cell lymphoma[70]. Among marginal zone lymphomas, a special association with HCV in-fection was reported for the mucosa-associated lymphoid tissue (MALT)lymphoma [65,71,72] and the splenic forms. This is confirmed by reportsof regression of marginal splenic lymphoma after successful HCV clearancebecause of antiviral therapy, in spite of previous ineffective chemotherapy[73–75]. In general, the observations of a hematological regression ofsome HCV-associated NHL and expanded B-cell clones following effectiveantiviral therapy represent a consistent argument in favor of the pathoge-netic role played by HCV infection, even if a direct antineoplastic role of in-terferon cannot be excluded.
A serum monoclonal gammopathy, more frequently type IgM/K, hasbeen described among HCV-associated LPDs [76]. In most patients withHCV, however, MG was classified as MGUS (monoclonal gammopathiesof uncertain significance), whereas a few patients who have HCV withmonoclonal gammopathy can be considered as affected by myeloma accord-ing to their clinico–pathologic characteristics [69,77,78].
Pathogenesis of hepatitis C virus-related lymphoproliferative disorders
It now is accepted widely that the pathogenesis of LPDs is a complex,multistep process. Several studies investigating the pathogenetic mecha-nisms involved in the evolution of HCV infection to B-cell LPDs are avail-able, but in spite of interesting hypotheses, the exact mechanisms involvedare not known. Originally, the observation of HCV lymphotropism at thebeginning of the 1990s led to the hypothesis of a causal link between infec-tion of lymphatic cells and autoimmune–lymphoproliferative disorders [79].Earlier, it was observed that both HCV-positive strand (genomic) and -neg-ative strand (antigenomic ¼ replicative intermediates) could be detected inperipheral blood mononuclear cells (PBMC) taken from patients who hadchronic HCV infection [80]. During the past decade, ex vivo and in vitrostudies with techniques of increasing specificity and sensitivity have led tobetter characterization of HCV lymphotropism [81–87]. Nonetheless, noclear proof of a direct link between HCV lymphotropism and LPD patho-genesis has been obtained, despite the demonstration of a more extensive in-volvement of the lymphatic system by HCV infection in patients who haveB-cell LPDs than those who do not [5,88,89], and of an enhancing effect ofB-cell infection by HCV in promoting the proliferation of lymphoid cells[90]. By contrast, several studies have supported an indirect role of HCVthrough activation of the host’s immune response [37,91–94]. The
618 ZIGNEGO & CRAXI
importance of a sustained antigenic stimulation by viral epitopes and of thespecific binding between the HCV E2 protein and the CD81 molecule hasbeen stressed [95], supporting the key role played by the promotion ofa strong polyclonal B-cell response to chronic viral infection that progres-sively would favor lymphomagenesis until final malignant transformation.
Contrasting data, showing the possibility that HCV may favor mutationsof immunoglobulin genes and oncogenes by a ‘‘hit and run’’ mechanism, wereobtained in cell lines and in cultured cells taken from patients with HCV [96].This analysis originated from previous observations showing a significant as-sociation between Bcl-2 rearrangement (14;18 translocation) and chronicHCV infection, especially in those subjects who developed type 2 MC [97–102], and MALT lymphoma [103]. In patients who had type II MC, the anal-ysis of synchronous and metachronous blood samples showed the clonalexpansion of B-cells harboring this chromosomal rearrangement [99]. Inaddition, it was possible to demonstrate an overexpression of the antiapop-totic Bcl-2 protein with a higher bcl-2/bax ratio in t (14;18)-positive B-cellsamples [99], and a modification of t (14;18) B-cell clone detection followingantiviral treatment [104]. Only treatments leading to sustained clearance ofHCV RNA from serum led to the regression of clones, with consequentlack of t (14;18)-positive cells in PBMC at the end of treatment, whereasthis effect was not observed in nonresponder patients [104]. An extensive fol-low-up of HCV-positive MC patients after sustained virological response toIFN-based treatments has revealed the possibility of viral persistence in thelymphatic compartment in the absence of serumHCVRNAor liver infection.Interestingly, isolated lymphatic infection was associated strictly with the per-sistence of both MC-syndrome and t (14;18)-bearing B-cell clones.
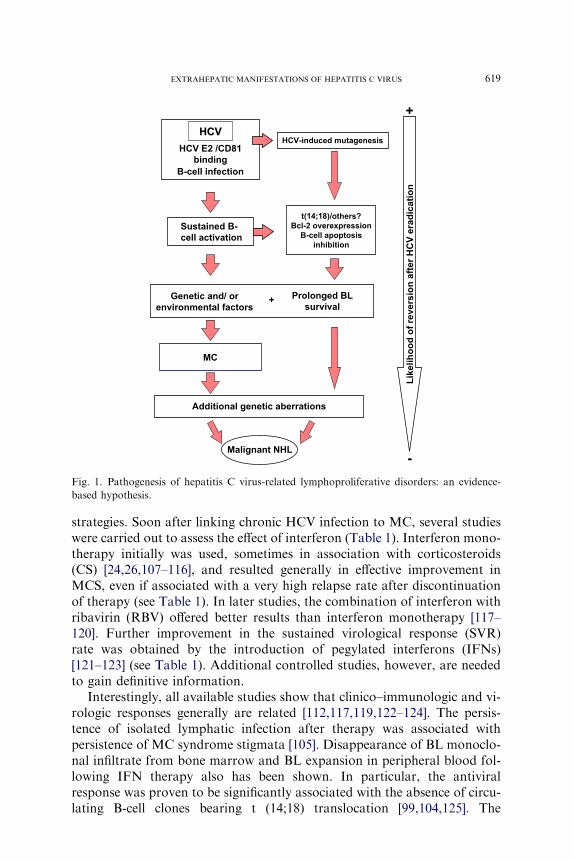
These observations reaffirm, after more than a decade since the originalsuggestions, the strong likelihood of a role played by HCV lymphotropismin lymphomagenesis, but the exact mechanisms involved remain unclear. Onthe other hand, they strongly suggest that the pathogenesis of MC is notnecessarily related to the intrahepatic challenge between HCV epitopesand lymphoid infiltrates. Considering the complexity of LPDs and the het-erogeneity of HCV-associated LPDs, it is conceivable that MC and otherHCV-related LPDs may have different pathogenetic pathways. An accurateunderstanding of these different pathways and the frequency of their in-volvement in the pathogenetic mechanisms would be essential for the correctappraisal of both therapeutic and preventive measures [105,106]. An attemptto summarize current knowledge of the interrelations between HCV andLPDs is presented in Fig. 1.
Treatment of hepatitis C virus-related mixed cryoglobulinemiaand lymphoproliferative disorders
Before the identification of its viral etiology, MC treatment includeda variable combination of anti-inflammatory and immunosuppressive
+
HCVHCV
HCV E2 /CD81
binding
B-cell infection
Sustained B-
cell activation
Genetic and/ or
environmental factors
Prolonged BL
survival
t(14;18)/others?
Bcl-2 overexpression
B-cell apoptosis
inhibition
MC
Additional genetic aberrations
Malignant NHL
HCV-induced mutagenesis
Likelih
oo
d o
f reversio
n after H
CV
erad
icatio
n
-
+
Fig. 1. Pathogenesis of hepatitis C virus-related lymphoproliferative disorders: an evidence-
based hypothesis.
619EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
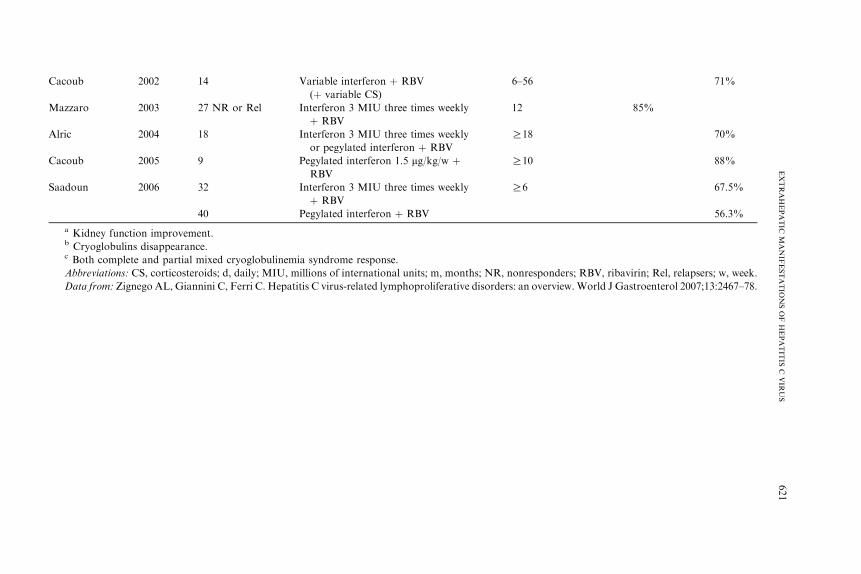
strategies. Soon after linking chronic HCV infection to MC, several studieswere carried out to assess the effect of interferon (Table 1). Interferon mono-therapy initially was used, sometimes in association with corticosteroids(CS) [24,26,107–116], and resulted generally in effective improvement inMCS, even if associated with a very high relapse rate after discontinuationof therapy (see Table 1). In later studies, the combination of interferon withribavirin (RBV) offered better results than interferon monotherapy [117–120]. Further improvement in the sustained virological response (SVR)rate was obtained by the introduction of pegylated interferons (IFNs)[121–123] (see Table 1). Additional controlled studies, however, are neededto gain definitive information.
Interestingly, all available studies show that clinico–immunologic and vi-rologic responses generally are related [112,117,119,122–124]. The persis-tence of isolated lymphatic infection after therapy was associated withpersistence of MC syndrome stigmata [105]. Disappearance of BL monoclo-nal infiltrate from bone marrow and BL expansion in peripheral blood fol-lowing IFN therapy also has been shown. In particular, the antiviralresponse was proven to be significantly associated with the absence of circu-lating B-cell clones bearing t (14;18) translocation [99,104,125]. The
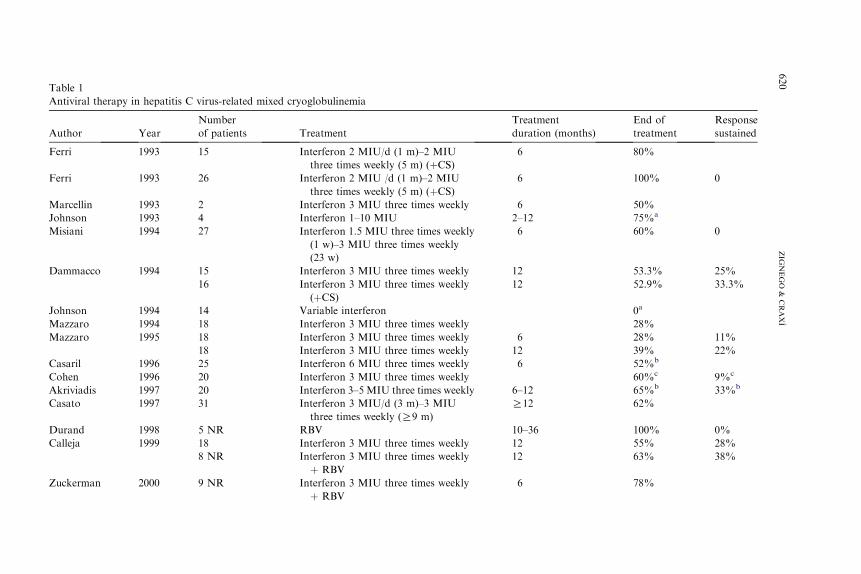
Table 1
Antiviral therapy in hepatitis C virus-related mixed cryoglobulinemia
Author Year
Number
of patients Treatment
Treatment
duration (months)
End of
treatment
Response
sustained
Ferri 1993 15 Interferon 2 MIU/d (1 m)–2 MIU
three times weekly (5 m) (þCS)6 80%
Ferri 1993 26 Interferon 2 MIU /d (1 m)–2 MIU
three times weekly (5 m) (þCS)6 100% 0
Marcellin 1993 2 Interferon 3 MIU three times weekly 6 50%
Johnson 1993 4 Interferon 1–10 MIU 2–12 75%a
Misiani 1994 27 Interferon 1.5 MIU three times weekly
(1 w)–3 MIU three times weekly
(23 w)
6 60% 0
Dammacco 1994 15 Interferon 3 MIU three times weekly 12 53.3% 25%
16 Interferon 3 MIU three times weekly
(þCS)12 52.9% 33.3%
Johnson 1994 14 Variable interferon 0a
Mazzaro 1994 18 Interferon 3 MIU three times weekly 28%
Mazzaro 1995 18 Interferon 3 MIU three times weekly 6 28% 11%
18 Interferon 3 MIU three times weekly 12 39% 22%
Casaril 1996 25 Interferon 6 MIU three times weekly 6 52%b
Cohen 1996 20 Interferon 3 MIU three times weekly 60%c 9%c
Akriviadis 1997 20 Interferon 3–5 MIU three times weekly 6–12 65%b 33%b
Casato 1997 31 Interferon 3 MIU/d (3 m)–3 MIU
three times weekly (R9 m)
R12 62%
Durand 1998 5 NR RBV 10–36 100% 0%
Calleja 1999 18 Interferon 3 MIU three times weekly 12 55% 28%
8 NR Interferon 3 MIU three times weekly
þ RBV
12 63% 38%
Zuckerman 2000 9 NR Interferon 3 MIU three times weekly
þ RBV
6 78%
620
ZIG
NEGO
&CRAXI
Cacoub 2002 14 Variable interferon þ RBV
(þ variable CS)
6–56 71%
Mazzaro 2003 27 NR or Rel Interferon 3 MIU three times weekly
þ RBV
12 85%
Alric 2004 18 Interferon 3 MIU three times weekly
or pegylated interferon þ RBV
R18 70%
Cacoub 2005 9 Pegylated interferon 1.5 mg/kg/w þRBV
R10 88%
Saadoun 2006 32 Interferon 3 MIU three times weekly
þ RBV
R6 67.5%
40 Pegylated interferon þ RBV 56.3%
a Kidney function improvement.b Cryoglobulins disappearance.c Both complete and partial mixed cryoglobulinemia syndrome response.
Abbreviations: CS, corticosteroids; d, daily; MIU, millions of international units; m, months; NR nonresponders; RBV, ribavirin; Rel, relapsers; w, week.
Data from: Zignego AL, Giannini C, Ferri C. Hepatitis C virus-related lymphoproliferative disord rs: an overview.World J Gastroenterol 2007;13:2467–78.
621
EXTRAHEPATIC
MANIF
ESTATIO
NSOFHEPATIT
ISC
VIR
US
,
e
622 ZIGNEGO & CRAXI
reappearance of circulating translocated BL clones after virological relapseat the end of treatment, and their persistent detection in subjects with un-modified viral load after antiviral therapy, strongly indicates that clonal ex-pansion of translocated cells depends on modifications of viral replicationinduced by antiviral treatment [104,125]. More recently, long-term analysisof patients with HCVand MCS showing SVR after therapy indicated thatoccult lymphatic infection and persistence of MCS stigmata also were asso-ciated with persistent determination of expanded t (14;18) carrying B-cellclones [105]. These data suggest the critical role played by a complete viraleradication and its possible role in preventing the evolution of LPD.
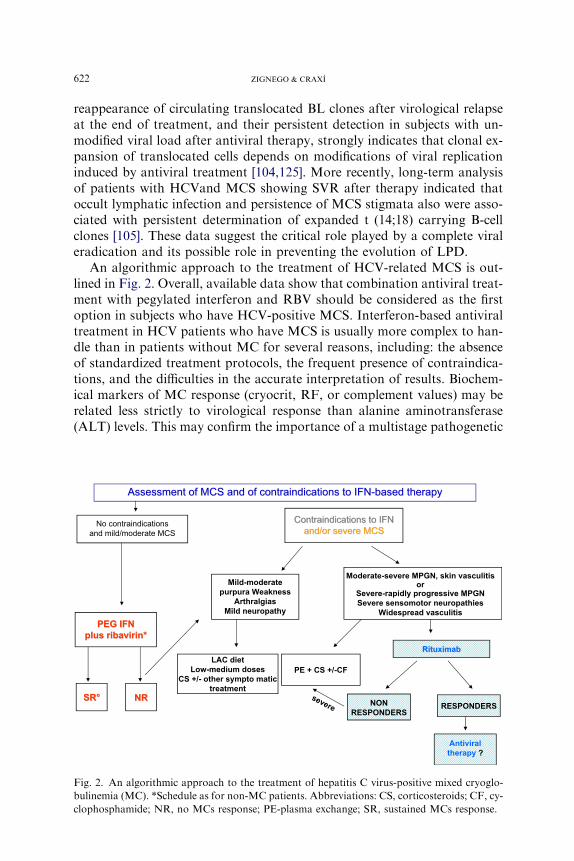
An algorithmic approach to the treatment of HCV-related MCS is out-lined in Fig. 2. Overall, available data show that combination antiviral treat-ment with pegylated interferon and RBV should be considered as the firstoption in subjects who have HCV-positive MCS. Interferon-based antiviraltreatment in HCV patients who have MCS is usually more complex to han-dle than in patients without MC for several reasons, including: the absenceof standardized treatment protocols, the frequent presence of contraindica-tions, and the difficulties in the accurate interpretation of results. Biochem-ical markers of MC response (cryocrit, RF, or complement values) may berelated less strictly to virological response than alanine aminotransferase(ALT) levels. This may confirm the importance of a multistage pathogenetic
Contraindications to IFNand/or severe MCS
Contraindications to IFNand/or severe MCS
Assessment of MCS and of contraindications to IFN-based therapyAssessment of MCS and of contraindications to IFN-based therapy
No contraindicationsand mild/moderate MCS
PEG IFN
plus ribavirin*
PEG IFN
plus ribavirin*
SR°SR° NRNR
LAC diet
Low-medium doses
CS +/- other sympto matic
treatment
NON
RESPONDERS
PE + CS +/-CF
RituximabRituximab
RESPONDERS
Antiviral
therapy ?
Moderate-severe MPGN, skin vasculitis
or
Severe-rapidly progressive MPGN
Severe sensomotor neuropathies
Widespread vasculitis
Mild-moderate
purpura Weakness
Arthralgias
Mild neuropathy
severe
Fig. 2. An algorithmic approach to the treatment of hepatitis C virus-positive mixed cryoglo-
bulinemia (MC). *Schedule as for non-MC patients. Abbreviations: CS, corticosteroids; CF, cy-
clophosphamide; NR, no MCs response; PE-plasma exchange; SR, sustained MCs response.
623EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
mechanism in MCS, suggesting the need for precise monitoring of this cat-egory of patients and the definition of predictive markers.
For patients in whom antiviral treatment is contraindicated or is nottolerated or in patients who are nonresponders, alternative therapeuticapproaches should be used, CS, immunosuppressive drugs, Non-SteroidalAnti-Inflammatory Drugs (NSAIDs), plasmapheresis (PE) and a hypoanti-genic diet (low antigen content [LAC] diet) administration [41,126]. Treat-ment should be tailored to the individual patient according to the severityof clinical symptoms, also considering the possible additional factors in-volved (age, renal failure, comorbidities), and the time (weeks or months)required for symptom remission. Corticosteroids represent the most com-monly used nonantiviral therapy for MCS and generally allow the controlof most MC symptoms even at low doses. They may favor HCV replica-tion, however, induce several adverse effects, and do not significantly mod-ify the natural history of the disease. Cytostatic–immunosuppressive drugs(ie, cyclophosphamide, chlorambucil, and azathioprine)may be used, espe-cially during the acute phases of MCS, but they may cause severe adverseeffects [127]. A special note must be made of new B-cell specific immuno-suppressive therapy based on the use of chimeric antibodies (rituximab)against the CD20, a B-cell specific surface antigen [128,129]. Rituximab iseffective in most patients who have MC, leading to marked improvementor resolution of the syndrome, especially of skin lesions, and to regressionof the expanded B-cell clones [128,129]. This therapeutic approach appearsto be very promising for managing patients who have MCS, but future con-trolled studies still are required to establish its ultimate role in treatingHCV-related MCS. It should be stressed that rituximab, as an immunosup-pressive agent, leads to an increase in HCV replication, but no significantreactivation of HCV-related liver disease has been reported. Its use in com-bination with direct antiviral molecules [41,128–131], when available, prob-ably will lead to further improvement in management.
Other therapeutic measures include plasma exchange (PE) and LAC diets.PE (ie, the apheretic removal of circulating immunocomplexes) specifically isindicated in the presence of clinically significant acute manifestations (cryo-globulinemic nephritis, severe sensorimotor neuropathies, cutaneous ulcers,and hyperviscosity syndrome). The LAC diets, generally prescribed at the ini-tial stage of MCS, essentially act by reducing the antigen load to the reticulo–endothelial system, thus allowing a more efficient removal of CGs.
Recent studies, performed in specific subgroups of patients with HCV-associated NHLs, such as marginal zone lymphomas [73,132], support therationale for the use of antiviral therapy also in the setting of malignantHCV-associated LPDs. In the study by Hermine and colleagues [73],a complete remission of Splenic Lymphoma with Villous Lymphocytes(SLVL) was observed in most HCV-positive patients but in none ofHCV-negative cases following treatment with IFN. In addition, regressionof clonal proliferation in response to antiviral treatment was shown to be
624 ZIGNEGO & CRAXI
associated clearly with virological response [99,104,125]. Seemingly onlya proportion of HCV-associated lymphomas are cured with antiviral ther-apy. Also in responsive patients who had SLVL, the rearrangement of themonoclonal immunoglobulin genes persistently was detected in the bloodeven after a complete hematological response [75]. Such data suggestthat the multistep lymphomagenetic cascade may have points of no-return,making the LPD progressively independent from HCV infection (seeFig. 1). Although antiviral therapy appears to be an attractive therapeutictool for low-grade HCV-positive NHL, in intermediate and high-gradeNHL, chemotherapy is most likely to be necessary while antiviral treat-ment possibly could represent a maintenance therapy [133]. Further studiesare needed to standardize antiviral therapy better in HCV-associatedNHL. The use of rituximab in HCV-associated NHL, in monotherapyor in combination with antiviral treatment and/or chemotherapy, appearsvery promising, particularly in the setting of low-grade NHL, where ritux-imab monotherapy has been proposed as first-line treatment [134–136]. Inspite of the limited number of described cases, rituximab may be consid-ered a safe and effective therapy for HCV-related indolent B-celllymphoma.
Other extrahepatic disorders and overlap syndromes
Many and different disorders have been linked to HCV infection. In mostcases, because of possible methodological bias, mainly in patient selection inthe various studies, it is difficult to verify whether the suggested associationis coincidental or whether a real pathogenetic link exists. Several conditionsare observed more frequently in the context of an MC and quite rarely asidiopathic forms. This is the case of skin, kidney, salivary glands, or lungdisorders. In addition, a clinicoserological overlap between differentEHMs-HCV often is observed [32,137,138]. In spite of the heterogeneityof the morbid conditions that have been linked to HCV, two issues are quiteconstant: the pathogenetic involvement of the host’s immune system and thesymptom severity with consequent worsening of quality of life [139]. In ad-dition, extrahepatic manifestations may be observed variably in the presenceor absence of hepatic damage. On the whole, these observations support theview of HCV infection as a distinct systemic disease with widely variableclinical expressions.
Dermatopathologic manifestations
In addition to MC-related purpura, HCV infection also has been associ-ated with several cutaneous disorders, including the sporadic variant of por-phyria cutanea tarda (PCT) [1,140–143], a metabolic disorder characterizedby reduced hepatic activity of uroporphyrinogen decarboxylase, and withoral lichen planus (OLP) [144–154]. A strong association between the
625EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
sporadic form of PCT and HCV was suggested by the high prevalence(greater than 50%) of HCV markers in these patients, mainly in studiesfrom southern Europe [1,140–143]. In HCV-positive patients withoutPCT, however, no significant alteration in porphyrin metabolism was shown[142,155,156]. Epidemiologic studies also proved the existence of a correla-tion between OLP and chronic HCV infection [144]. The prevalence of HCVinfection in a large population of patients who had OLP was about 27%[145]. Data supporting this correlation essentially stem from studies per-formed in Japan [144] and southern Europe [145–148], but these were notconfirmed in other populations [149–152]. It generally is agreed that in thesecutaneous disorders, HCV infection plays an indirect role, probably actingas a triggering factor in genetically predisposed individuals. As a matter offact, attempts to cure these disorders with antiviral therapy led to discor-dant, but generally negative results with the possible induction of a clinicalmanifestation in previously unaffected patients or worsening of the disease[33].
Nephrological disorders
A causative association between HCV and non-MC related forms of re-nal damage (membranoproliferative glomerulonephritis without simulta-neous presence of cryoglobulins, or membranous nephropathy) has beensuggested, but requires confirmation [33].
Neurologic disorders
Neurologic complications have been associated with HCV infectionmostly in the context of MC, but also in the absence of this condition[157,158]. Only cryoglobulinemic neuropathy, however, has been associatedclearly with HCV infection.
Disorders of the joints, bones and muscles
HCV-related chronic polyarthritis can be observed in HCV-positive pa-tients both with and without MC [13,159]. True rheumatoid arthritis(RA), in keeping with classic criteria, seems to be uncommon in subjectswho have HCV. In patients who have HCV, tests are usually negative forantibodies to cyclic citrullinated peptides (anti-CCP), which may help to dif-ferentiate the two conditions (true RA and HCV-related RA-like form). Bycontrast, intermittent oligoarthritis, generally not erosive and involving thebig and middle-sized joints, is observed frequently [13,32,159]. An associa-tion of HCV infection with osteosclerosis and a correlation between suchmanifestation and the imbalance in the osteoprotegerin/RANKL (ReceptorActivator of NF-kB Ligand) system with a predominance of osteoprotegerinalso were observed in some studies [160,161]. HCV infection also was sug-gested to be associated with myositis and dermatomyositis [162].
626 ZIGNEGO & CRAXI
Endocrinologic disorders
Practically all known manifestations of a thyroid disorder have been de-scribed in patients who have HCV infection, but frequently with discordantdata [163–167]. Geographic, genetic, or environmental cofactors [168–171]and different methodological approaches partially explain discordant obser-vations. The most frequently observed HCV-associated thyroid disorder in-volves circulating antithyroid peroxidase antibodies in female subjects [166].Subclinical hypothyroidism was observed in 2% to 9% of patients who hadchronic HCV infection and particularly in those who had MC [2,165,172].Finally, a higher prevalence of papillary thyroid carcinoma in patientswho had HCV was observed [173–175]. Interferon alfa therapy may exacer-bate or induce underlying latent thyroid disorders, and the relative contribu-tion of the role played by HCV or by antiviral therapy in leading to suchassociations has been discussed [166,176–178]. Recently, it was suggestedthat molecular mimicry between viral and self-antigens might be involvedin the pathogenesis of HCV-associated autoimmune thyroid diseases [179].A high prevalence of diabetes mellitus type 2 was observed in patientswho had chronic HCV infection in several studies [180–187], and it hasbeen suggested that HCV acts as a risk factor independently of liver disease[188]. In patients who had HCV infection, the appearance of diabetes type 2was associated with insulin resistance and was considered part of a complexvirus-induced metabolic syndrome including both hepatic (steatosis) and ex-trahepatic manifestations. In agreement with this, an association betweencarotid atherosclerosis and HCV infection recently has been suggested[189,190].
Lung and cardiocirculatory disorders
A pathogenetic link between HCV infection and idiopathic pulmonary fi-brosis has been reported [191,192]. The fact that MC can be complicated byan involvement of pulmonary interstitium suggests that such association insome cases can be related to a pre-existing MC [193]. An association be-tween HCV and hypertrophic cardiomyopathy was suggested by the obser-vation of significantly higher prevalence of anti-HCV in Japanese patientswith such condition compared with controls [194]. Studies performed inItaly and in Greece by other authors, however, did not confirm this associ-ation. Regardless, the recent determination of a significantly higher preva-lence of carotid atherosclerosis in patients with HCV infection [189] isnoteworthy; this association was mostly evident in case of active viral repli-cation [190]. In a very recent study, the association between HCV chronicinfection and carotid atherosclerotic lesions was confirmed also in a largeItalian population. Further, HCV RNA sequence was determined in carotidplaques, strongly suggesting a local proatherogenetic action of the virus in-side the plaque [195].

627EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
Psychopathological disorders
Patients who have HCV infection have a low quality of life and may ex-perience excessive fatigue, decreased cognitive ability, and low mood tone[196–198]. These symptoms are not related directly to liver damage, and ithas been proposed that the virus may cause direct cerebral dysfunction byan unknown mechanism [197]. Recently, plasma tryptophan and kynureninecontent in blood, together with indoleamine 2,3-dioxygenase activity inmacrophages, was evaluated in a cohort of patients who had mild HCV-re-lated chronic liver disease. Patients also underwent psychopathological eval-uation. Serum tryptophan concentrations were lower than those of healthysubjects or patients who had chronic HBV infection, and were associatedwith high levels of anxiety and depression, strongly suggesting that thesemodifications may be causally related. In addition, mechanisms involvedin the pathogenesis of HCV-associated reduced tryptophan levels appeareddifferent from those observed in other chronic infections, thus possibly rep-resenting a new model for viral-induced alterations of tryptophan metabo-lism [199–201].
References
[1] Zignego AL, Brechot C. Extrahepatic manifestations of HCV infection: facts and contro-
versies. J Hepatol 1999;31:369–76.
[2] Cacoub P, Poynard T, Ghillani P, et al. Extrahepatic manifestations of chronic hepatitis C.
MULTIVIRC group. Multidepartment virus C. Arthritis Rheum 1999;42:2204–12.
[3] Ferri C, ZignegoAL, Pileri S. Cryoglobulins. In: YoungNS, Gerson SL, HighKA, editors.
Clinical hematology, vol. Mosby (MO): Elsevier; 2005. 625–36, Chapter 24.
[4] Misiani R, Bellavita P, Fenili D, et al. Hepatitis C virus infection in patients with essential
mixed cryoglobulinemia. Ann Intern Med 1992;117:573–7.
[5] Ferri C, Monti M, La Civita L, et al. Infection of peripheral blood mononuclear cells by
hepatitis C virus in mixed cryoglobulinemia. Blood 1993;82:3701–4.
[6] Zignego AL, Ferri C, Giannini C, et al. Hepatitis C virus infection in mixed cryoglobuline-
mia and B-cell non-Hodgkin’s lymphoma: evidence for a pathogenetic role. Arch Virol
1997;142:545–55.
[7] Agnello V, ChungRT, Kaplan LM.A role for hepatitis C virus infection in type II cryoglo-
bulinemia [see comments]. N Engl J Med 1992;327:1490–5.
[8] Brouet JC, Clauvel JP, DanonF, et al. Biologic and clinical significance of cryoglobulins. A
report of 86 cases. Am J Med 1974;57:775–88.
[9] Agnello V.Hepatitis C virus infection and type II cryoglobulinemia: an immunological per-
spective [published erratum appears in Hepatology 1998Mar;27(3):889]. Hepatology 1997;
26:1375–9.
[10] Lunel F,Musset L, Cacoub P, et al. Cryoglobulinemia in chronic liver diseases: role of hep-
atitis C virus and liver damage. Gastroenterology 1994;106:1291–300.
[11] Wong VS, EgnerW, Elsey T, et al. Incidence, character and clinical relevance of mixed cry-
oglobulinaemia in patients with chronic hepatitis C virus infection. Clin Exp Immunol
1996;104:25–31.
[12] Pawlotsky JM, Roudot-Thoraval F, Simmonds P, et al. Extrahepatic immunologic mani-
festations in chronic hepatitis C and hepatitis C virus serotypes. Ann InternMed 1995;122:
169–73.

628 ZIGNEGO & CRAXI
[13] Ferri C, Sebastiani M, Giuggioli D, et al. Mixed cryoglobulinemia: demographic, clinical,
and serologic features and survival in 231 patients. Semin Arthritis Rheum 2004;33:355–74.
[14] Meltzer M, Franklin EC. Cryoglobulinemiada study of twenty-nine patients. I. IgG and
IgM cryoglobulins and factors affecting cryoprecipitability. Am J Med 1966;40:828–36.
[15] MeltzerM, Franklin EC, EliasK, et al. Cryoglobulinemiada clinical and laboratory study.
II. Cryoglobulins with rheumatoid factor activity. Am J Med 1966;40:837–56.
[16] Haddad J, Deny P,Munz-Gotheil C, et al. Lymphocytic sialadenitis of Sjogren’s syndrome
associated with chronic hepatitis C virus liver disease. Lancet 1992;339:321–3.
[17] Koike K,MoriyaK, Ishibashi K, et al. Sialadenitis histologically resembling Sjogren’s syn-
drome in mice transgenic for hepatitis C virus envelope genes. Proc Natl Acad Sci U S A
1997;94:233–6.
[18] De Vita S, Sacco C, Sansonno D, et al. Characterization of overt B-cell lymphomas in pa-
tients with hepatitis C virus infection. Blood 1997;90:776–82.
[19] Scott CA, Avellini C, Desinan L, et al. Chronic lymphocytic sialoadenitis in HCV-related
chronic liver disease: comparison of Sjogren’s syndrome. Histopathology 1997;30:41–8.
[20] Ferri C, Longombardo G, La Civita L, et al. Hepatitis C virus chronic infection as a com-
mon cause of mixed cryoglobulinaemia and autoimmune liver disease. J Intern Med 1994;
236:31–6.
[21] Daghestani L, Pomeroy C. Renal manifestations of hepatitis C infection. Am J Med 1999;
106:347–54.
[22] D’Amico G. Renal involvement in hepatitis C infection: cryoglobulinemic glomerulone-
phritis. Kidney Int 1998;54:650–71.
[23] TarantinoA, CampiseM, BanfiG, et al. Long-termpredictors of survival in essentialmixed
cryoglobulinemic glomerulonephritis. Kidney Int 1995;47:618–23.
[24] Johnson RJ, Gretch DR, Yamabe H, et al. Membranoproliferative glomerulonephritis as-
sociated with hepatitis C virus infection [see comments]. N Engl J Med 1993;328:465–70.
[25] Beddhu S, Bastacky S, Johnson JP. The clinical and morphologic spectrum of renal cryo-
globulinemia. Medicine (Baltimore) 2002;81:398–409.
[26] Ferri C, Marzo E, Longombardo G, et al. Interferon-alfa in mixed cryoglobulinemia pa-
tients: a randomized, crossover-controlled trial. Blood 1993;81:1132–6.
[27] Bartenschlager R, Ahlborn-Laake L,Mous J, et al. Nonstructural protein 3 of the hepatitis
C virus encodes a serine-type proteinase required for cleavage at theNS3/4 andNS4/5 junc-
tions. J Virol 1993;67:3835–44.
[28] CacoubP, Fabiani FL,Musset L, et al.Mixed cryoglobulinemia and hepatitis C virus. Am J
Med 1994;96:124–32.
[29] Borowski P, Heiland M, Oehlmann K, et al. Nonstructural protein 3 of hepatitis C virus
inhibits phosphorylation mediated by cAMP-dependent protein kinase. Eur J Biochem
1996;237:611–8.
[30] Kayali Z, BuckwoldVE, ZimmermanB, et al. Hepatitis C, cryoglobulinemia, and cirrhosis:
a meta-analysis. Hepatology 2002;36:978–85.
[31] Saadoun D, Asselah T, Resche-Rigon M, et al. Cryoglobulinemia is associated with stea-
tosis and fibrosis in chronic hepatitis C. Hepatology 2006;43:1337–45.
[32] Ferri C, Zignego AL, Pileri SA. Cryoglobulins. J Clin Pathol 2002;55:4–13.
[33] Zignego AL, Giannini C, Ferri C. Hepatitis C virus-related lymphoproliferative disorders:
an overview. World J Gastroenterol 2007;13:2467–78.
[34] Musset L, Diemert MC, Taibi F, et al. Characterization of cryoglobulins by immunoblot-
ting. Clin Chem 1992;38:798–802.
[35] Sansonno D, De Vita S, Iacobelli AR, et al. Clonal analysis of intrahepatic B cells from
HCV-infected patients with and without mixed cryoglobulinemia. J Immunol 1998;160:
3594–601.
[36] MagaliniAR, Facchetti F, Salvi L, et al. Clonality of B-cells in portal lymphoid infiltrates of
HCV-infected livers. J Pathol 1998;185:86–90.

629EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
[37] Racanelli V, SansonnoD, Piccoli C, et al.Molecular characterization of B cell clonal expan-
sions in the liver of chronically hepatitis C virus-infected patients. J Immunol 2001;167:
21–9.
[38] Vallat L, Benhamou Y, Gutierrez M, et al. Clonal B cell populations in the blood and liver
of patients with chronic hepatitis C virus infection. Arthritis Rheum 2004;50:3668–78.
[39] Monteverde A, Pileri S. Lymphoproliferative diseases of uncertain classification. Ann Ital
Med Int 1991;6:162–70.
[40] Ferri C, Pileri S, Zignego AL. Hepatitis C virus infection and non-Hodgkin’s lymphoma.
In: Geodert JJ, editor. Infectious causes of cancer. Targets for intervention. Totowa
(NJ): The Human Press inc.; 2000. p. 349–68.
[41] Ferri C, Zignego AL, Pileri SA. Cryoglobulinemia. Philadelphia: Elsevier; 2006.
[42] Santini GF, Crovatto M, Modolo ML, et al. Waldenstrom macroglobulinemia: a role of
HCV infection? Blood 1993;82:2932.
[43] Pozzato G, Mazzaro C, Crovatto M, et al. Low-grade malignant lymphoma, hepatitis C
virus infection, and mixed cryoglobulinemia. Blood 1994;84:3047–53.
[44] Mussini C, Ghini M, Mascia MT, et al. Monoclonal gammopathies and hepatitis C virus
infection. Blood 1995;85:1144–5.
[45] Mangia A, Clemente R, Musto P, et al. Hepatitis C virus infection and monoclonal gam-
mopathies not associated with cryoglobulinemia. Leukemia 1996;10:1209–13.
[46] Mazzaro C, Zagonel V, Monfardini S, et al. Hepatitis C virus and non-Hodgkin’s lympho-
mas [see comments]. Br J Haematol 1996;94:544–50.
[47] Musto P, Dell’Olio M, Carotenuto M, et al. Hepatitis C virus infection: a new bridge be-
tween hematologists and gastroenterologists? Blood 1996;88:752–4.
[48] Silvestri F, Barillari G, Fanin R, et al. Impact of hepatitis C virus infection on clinical fea-
tures, quality of life and survival of patients with lymphoplasmacytoid lymphoma/immu-
nocytoma. Ann Oncol 1998;9:499–504.
[49] Ferri C, Monti M, La Civita L, et al. Hepatitis C virus infection in non-Hodgkin’s B-cell
lymphoma complicating mixed cryoglobulinaemia. Eur J Clin Invest 1994;24:781–4.
[50] Monti G, Pioltelli P, Saccardo F, et al. Incidence and characteristics of non-Hodgkin’s lym-
phomas in a multicenter case file of patients with hepatitis C virus-related symptomatic
mixed cryoglobulinemias. Arch Intern Med 2005;165:101–5.
[51] Ferri C, Caracciolo F, La Civita L, et al. Hepatitis C virus infection and B-cell lymphomas
[letter]. Eur J Cancer 1994;10:1591–2.
[52] Ferri C, La Civita L, Caracciolo F, et al. Non-Hodgkin’s lymphoma: possible role of hep-
atitis C virus [letter]. JAMA 1994;272:355–6.
[53] Luppi M, Grazia Ferrari M, Bonaccorsi G, et al. Hepatitis C virus infection in subsets of
neoplastic lymphoproliferations not associated with cryoglobulinemia. Leukemia 1996;
10:351–5.
[54] Pioltelli P, Zehender G, Monti G, et al. HCV and non-Hodgkin’s lymphoma. Lancet 1996;
347:624–5.
[55] Silvestri F, Pipan C, Barillari G, et al. Prevalence of hepatitis C virus infection in patients
with lymphoproliferative disorders. Blood 1996;87:4296–301.
[56] Brind AM, Watson JP, Burt A, et al. Non-Hodgkin’s lymphoma and hepatitis C virus in-
fection. Leuk Lymphoma 1996;21:127–30.
[57] Hanley J, Jarvis L, Simmonds P, et al. HCV and non-Hodgkin’s lymphoma. Lancet 1996;
347:1339.
[58] McCollMD, Singer IO, Tait RC, et al. The role of hepatitis C virus in the aetiology of non-
Hodgkin’s lymphomada regional association? Leuk Lymphoma 1997;26:127–30.
[59] Ellenrieder V,WeidenbachH, FrickhofenN, et al. HCV andHGV in B-cell non-Hodgkin’s
lymphoma. J Hepatol 1998;28:34–9.
[60] Collier JD, Zanke B, Moore M, et al. No association between hepatitis C and B-cell lym-
phoma [see comments]. Hepatology 1999;29:1259–61.

630 ZIGNEGO & CRAXI
[61] Hausfater P, Cacoub P, Rosenthal E, et al. Hepatitis C virus infection and lymphoprolifer-
ative diseases in France: a national study. The Germivic group. Am J Hematol 2000;64:
107–11.
[62] Matsuo K, Kusano A, Sugumar A, et al. Effect of hepatitis C virus infection on the risk of
non-Hodgkin’s lymphoma: a meta-analysis of epidemiological studies. Cancer Sci 2004;95:
745–52.
[63] Silvestri F, Baccarani M. Hepatitis C virus-related lymphomas. Br J Haematol 1997;99:
475–80.
[64] Ascoli V, Lo Coco F, Artini M, et al. Extranodal lymphomas associated with hepatitis C
virus infection. Am J Clin Pathol 1998;109:600–9.
[65] LuppiM, LongoG, FerrariMG, et al. Clinico–pathological characterization of hepatitis C
virus-related B- cell non-Hodgkin’s lymphomas without symptomatic cryoglobulinemia
[see comments]. Ann Oncol 1998;9:495–8.
[66] TrepoC, Berthillon P,Vitvitski L.HCVand lymphoproliferative diseases.AnnOncol 1998;
9:469–70.
[67] Talamini R,MontellaM, CrovattoM, et al. Non-Hodgkin’s lymphoma and hepatitis C vi-
rus: a case–control study from northern and southern Italy. Int J Cancer 2004;110:380–5.
[68] Harris NL, Jaffe ES, Stein H, et al. A revised European-American classification of lym-
phoid neoplasms: a proposal from the International Lymphoma Study Group [see com-
ments]. Blood 1994;84:1361–92.
[69] Jaffe Es HN, Stein H, Vardiman JW. Tumours of haematopoietic and lymphoid tissues.
World Health Organization classification of tumours. Lyon (France): IARC Press; 2001.
[70] Nieters A,Kallinowski B, Brennan P, et al. Hepatitis C and risk of lymphoma: results of the
European multicenter case–control study Epilymph. Gastroenterology 2006;131:1879–86.
[71] De Vita S, Sansonno D, Dolcetti R, et al. Hepatitis C virus within a malignant lymphoma
lesion in the course of type II mixed cryoglobulinemia. Blood 1995;86:1887–92.
[72] Luppi M, Longo G, Ferrari MG, et al. Additional neoplasms and HCV infection in low-
grade lymphoma of MALT type. Br J Haematol 1996;94:373–5.
[73] Hermine O, Lefrere F, Bronowicki JP, et al. Regression of splenic lymphoma with villous
lymphocytes after treatment of hepatitis C virus infection. N Engl J Med 2002;347:89–94.
[74] Lefrere F, Troussard X, Hermine O. Regression of splenic lymphoma with villous lympho-
cytes after treatment of hepatitis C virus infection.NEngl JMed 2002;347:2168–70, (author
reply).
[75] Saadoun D, Suarez F, Lefrere F, et al. Splenic lymphoma with villous lymphocytes, asso-
ciated with type II cryoglobulinemia and HCV infection: a new entity? Blood 2005;105:
74–6.
[76] Andreone P, ZignegoAL, Cursaro C, et al. Prevalence of monoclonal gammopathies in pa-
tients with hepatitis C virus infection. Ann Intern Med 1998;129:294–8.
[77] Bartl R, Frisch B, Fateh-Moghadam A, et al. Histologic classification and staging of mul-
tiple myeloma. A retrospective and prospective study of 674 cases. Am J Clin Pathol 1987;
87:342–55.
[78] Pileri S, Poggi S, Baglioni P, et al. Histology and immunohistology of bone marrow biopsy
in multiple myeloma. Eur J Haematol Suppl 1989;51:52–9.
[79] Zignego AL, Ferri C, Monti M, et al. Hepatitis C virus as a lymphotropic agent: evidence
and pathogenetic implications. Clin Exp Rheumatol 1995;13(Suppl 13):S33–7.
[80] Zignego AL, Macchia D, Monti M, et al. Infection of peripheral mononuclear blood cells
by hepatitis C virus [see comments]. J Hepatol 1992;15:382–6.
[81] Zignego AL, De Carli M, Monti M, et al. Hepatitis C virus infection of mononuclear cells
fromperipheral blood and liver infiltrates in chronically infected patients. JMedVirol 1995;
47:58–64.
[82] Shimizu YK, Igarashi H, Kanematu T, et al. Sequence analysis of the hepatitis C virus ge-
nome recovered from serum, liver, and peripheral blood mononuclear cells of infected
chimpanzees. J Virol 1997;71:5769–73.
631EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
[83] Bronowicki JP, Loriot MA, Thiers V, et al. Hepatitis C virus persistence in human hema-
topoietic cells injected into SCID mice [see comments]. Hepatology 1998;28:211–8.
[84] Lerat H, Rumin S, Habersetzer F, et al. In vivo tropism of hepatitis C virus genomic se-
quences in hematopoietic cells: influence of viral load, viral genotype, and cell phenotype.
Blood 1998;91:3841–9.
[85] Roque-Afonso AM, Jiang J, Penin F, et al. Nonrandom distribution of hepatitis C virus
quasispecies in plasma and peripheral blood mononuclear cell subsets. J Virol 1999;73:
9213–21.
[86] Sansonno D, Lotesoriere C, Cornacchiulo V, et al. Hepatitis C virus infection involves
CD34(þ) hematopoietic progenitor cells in hepatitis C virus chronic carriers. Blood
1998;92:3328–37.
[87] Roque-Afonso AM, Ducoulombier D, Di Liberto G, et al. Compartmentalization of hep-
atitis C virus genotypes between plasma and peripheral blood mononuclear cells. J Virol
2005;79:6349–57.
[88] GalliM, ZehenderG,MontiG, et al. Hepatitis C virusRNA in the bonemarrowof patients
with mixed cryoglobulinemia and in subjects with noncryoglobulinemic chronic hepatitis
type C. J Infect Dis 1995;171:672–5.
[89] Sansonno D, Lauletta G, Montrone M, et al. Virological analysis and phenotypic charac-
terization of peripheral blood lymphocytes of hepatitis C virus-infected patients with and
without mixed cryoglobulinaemia. Clin Exp Immunol 2006;143:288–96.
[90] Pal S, Sullivan DG, Kim S, et al. Productive replication of hepatitis C virus in perihepatic
lymph nodes in vivo: implications of HCV lymphotropism. Gastroenterology 2006;130:
1107–16.
[91] Ivanovski M, Silvestri F, Pozzato G, et al. Somatic hypermutation, clonal diversity, and
preferential expression of the VH 51p1/VL kv325 immunoglobulin gene combination in
hepatitis C virus-associated immunocytomas. Blood 1998;91:2433–42.
[92] De Re V, De Vita S, Marzotto A, et al. Sequence analysis of the immunoglobulin antigen
receptor of hepatitis C virus-associated non-Hodgkin’s lymphomas suggests that themalig-
nant cells are derived from the rheumatoid factor-producing cells that occur mainly in type
II cryoglobulinemia. Blood 2000;96:3578–84.
[93] Sansonno D, Lauletta G, De Re V, et al. Intrahepatic B cell clonal expansions and extra-
hepatic manifestations of chronic HCV infection. Eur J Immunol 2004;34:126–36.
[94] Mariette X. Lymphomas complicating Sjogren’s syndrome and hepatitis C virus infection
may share a common pathogenesis: chronic stimulation of rheumatoid factor B cells. Ann
Rheum Dis 2001;60:1007–10.
[95] Pileri P, Uematsu Y, Campagnoli S, et al. Binding of hepatitis C virus to CD81. Science
1998;282:938–41.
[96] Machida K, Cheng KT, Sung VM, et al. Hepatitis C virus induces a mutator phenotype:
enhanced mutations of immunoglobulin and protooncogenes. Proc Natl Acad Sci U S A
2004;101:4262–7.
[97] Zignego AL, Giannelli F, Marrocchi ME, et al. Frequency of bcl-2 rearrangement in pa-
tients with mixed cryoglobulinemia and HCV-positive liver diseases. Clin Exp Rheumatol.
1997;15:711–2.
[98] Zignego AL, Giannelli F, Marrocchi ME, et al. T (14;18) translocation in chronic hepatitis
C virus infection. Hepatology 2000;31:474–9.
[99] Zignego AL, Ferri C, Giannelli F, et al. Prevalence of bcl-2 rearrangement in patients with
hepatitis C virus-related mixed cryoglobulinemia with or without B-cell lymphomas. Ann
Intern Med 2002;137:571–80.
[100] Kitay-Cohen Y, Amiel A, Hilzenrat N, et al. Bcl-2 rearrangement in patients with chronic
hepatitis C associated with essential mixed cryoglobulinemia type II. Blood 2000;96:
2910–2.
[101] Zuckerman E, Zuckerman T, Sahar D, et al. bcl-2 and immunoglobulin gene rearrange-
ment in patients with hepatitis C virus infection. Br J Haematol 2001;112:364–9.
632 ZIGNEGO & CRAXI
[102] SassoEH,MartinezM,Yarfitz SL, et al. Frequent joining of Bcl-2 to a JH6 gene in hepatitis
C virus-associated t (14;18). J Immunol 2004;173:3549–56.
[103] LibraM,Gloghini A,Navolanic PM, et al. JH6 gene usage amongHCV-associatedMALT
lymphomas harboring t (14;18) translocation. J Immunol 2005;174:3839, author reply
3839.
[104] Giannelli F, Moscarella S, Giannini C, et al. Effect of antiviral treatment in patients with
chronic HCV infection and t (14;18) translocation. Blood 2003;102:1196–201.
[105] Giannini C, Giannelli F, Linda Zignego A. Association between mixed cryoglobulinemia,
translocation (14;18), and persistence of occult HCV lymphoid infection after treatment.
Hepatology 2006;43:1166–7.
[106] Giannini C, Petrarca A,MontiM, et al. Association between persistent lymphatic infection
by hepatitis C virus after antiviral treatment and mixed cryoglobulinemia. Blood 2008;111:
2943–5.
[107] Ferri C, Zignego AL, Longombardo G, et al. Effect of alpha interferon on hepatitis C virus
chronic infection in mixed cryoglobulinemia patients. Infection 1993;21:93–7.
[108] Marcellin P, Descamps V, Martinot-Peignoux M, et al. Cryoglobulinemia with vasculitis
associated with hepatitis C virus infection. Gastroenterology 1993;104:272–7.
[109] Misiani R, Bellavita P, Fenili D, et al. Interferon alfa-2a therapy in cryoglobulinemia asso-
ciated with hepatitis C virus [see comments]. N Engl J Med 1994;330:751–6.
[110] Dammacco F, Sansonno D, Han JH, et al. Natural interferon-alfa versus its combination
with 6-methyl- prednisolone in the therapy of type II mixed cryoglobulinemia: a long- term,
randomized, controlled study. Blood 1994;84:3336–43.
[111] Johnson RJ, Gretch DR, Couser WG, et al. Hepatitis C virus-associated glomerulonephri-
tis. Effect of alpha-interferon therapy. Kidney Int 1994;46:1700–4.
[112] Mazzaro C, Pozzato G,Moretti M, et al. Long-term effects of alpha-interferon therapy for
type II mixed cryoglobulinemia [published erratum appears in Haematologica 1994 Sep–
Oct;79(5):486]. Haematologica 1994;79:342–9.
[113] Casaril M, Capra F, Gabrielli GB, et al. Cryoglobulinemia in hepatitis C virus chronic
active hepatitis: effects of interferon-alfa therapy. J Interferon Cytokine Res 1996;16:
585–8.
[114] Cohen P, Nguyen QT, Deny P, et al. Treatment of mixed cryoglobulinemia with recombi-
nant interferon-alfa and adjuvant therapies. A prospective study on 20 patients. Ann Med
Interne (Paris) 1996;147:81–6.
[115] Akriviadis EA, Xanthakis I, Navrozidou C, et al. Prevalence of cryoglobulinemia in
chronic hepatitis C virus infection and response to treatment with interferon-alfa. J Clin
Gastroenterol 1997;25:612–8.
[116] Casato M, Agnello V, Pucillo LP, et al. Predictors of long-term response to high-dose in-
terferon therapy in type II cryoglobulinemia associated with hepatitis C virus infection.
Blood 1997;90:3865–73.
[117] Calleja JL, Albillos A, Moreno-Otero R, et al. Sustained response to interferon-alfa or to
interferon-alfa plus ribavirin in hepatitis C virus-associated symptomatic mixed cryoglobu-
linaemia. Aliment Pharmacol Ther 1999;13:1179–86.
[118] Zuckerman E, KerenD, Slobodin G, et al. Treatment of refractory, symptomatic, hepatitis
C virus related mixed cryoglobulinemia with ribavirin and interferon-alfa. J Rheumatol
2000;27:2172–8.
[119] Cacoub P, LidoveO,Maisonobe T, et al. Interferon-alfa and ribavirin treatment in patients
with hepatitis C virus-related systemic vasculitis. Arthritis Rheum 2002;46:3317–26.
[120] Mazzaro C, Zorat F, Comar C, et al. Interferon plus ribavirin in patients with hepatitis C
virus positive mixed cryoglobulinemia resistant to interferon. J Rheumatol 2003;30:
1775–81.
[121] Alric L, Plaisier E, Thebault S, et al. Influence of antiviral therapy in hepatitis C virus-as-
sociated cryoglobulinemic MPGN. Am J Kidney Dis 2004;43:617–23.
633EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
[122] CacoubP, SaadounD, LimalN, et al. PEGylated interferon alfa-2b and ribavirin treatment
in patients with hepatitis C virus-related systemic vasculitis. Arthritis Rheum 2005;52:
911–5.
[123] Mazzaro C, Zorat F, CaizziM, et al. Treatment with peg-interferon alfa-2b and ribavirin of
hepatitis C virus-associated mixed cryoglobulinemia: a pilot study. J Hepatol 2005;42:
632–8.
[124] Levine JW, Gota C, Fessler BJ, et al. Persistent cryoglobulinemic vasculitis following suc-
cessful treatment of hepatitis C virus. J Rheumatol 2005;32:1164–7.
[125] Zuckerman E, Zuckerman T, Sahar D, et al. The effect of antiviral therapy on t (14;18)
translocation and immunoglobulin gene rearrangement in patients with chronic hepatitis
C virus infection. Blood 2001;97:1555–9.
[126] Ferri C, Giuggioli, Cazzato M, et al. HCV-related cryoglobulinemic vasculitis: update of
etiopathogenesis and therapeutic strategies. Clin Exp Rheumatol 2003;21:578–84.
[127] BallareM,Bobbio F, Poggi S, et al. A pilot study on the effectiveness of cyclosporine in type
II mixed cryoglobulinemia. Clin Exp Rheumatol 1995;13(Suppl 13):S201–3.
[128] Zaja F, De Vita S, Mazzaro C, et al. Efficacy and safety of rituximab in type II mixed cry-
oglobulinemia. Blood 2003;101:3827–34.
[129] SansonnoD,DeReV, Lauletta G, et al.Monoclonal antibody treatment of mixed cryoglo-
bulinemia resistant to interferon alpha with an anti-CD20. Blood 2003;101:3818–26.
[130] Zaja F, Russo D, Fuga G, et al. Rituximab for the treatment of type II mixed cryoglobu-
linemia. Haematologica 1999;84:1157–8.
[131] Zaja F, De Vita S, Russo D, et al. Rituximab for the treatment of type II mixed cryoglobu-
linemia. Arthritis Rheum 2002;46:2252–4, author reply 2254–55.
[132] Kelaidi C, Rollot F, Park S, et al. Response to antiviral treatment in hepatitis C virus-as-
sociated marginal zone lymphomas. Leukemia 2004;18:1711–6.
[133] Gisbert JP, Garcia-Buey L, Pajares JM, et al. Systematic review: regression of lymphopro-
liferative disorders after treatment for hepatitis C infection. Aliment Pharmacol Ther 2005;
21:653–62.
[134] Hainsworth JD, Litchy S, Burris HA III, et al. Rituximab as first-line and maintenance
therapy for patients with indolent non-Hodgkin’s lymphoma. J ClinOncol 2002;20:4261–7.
[135] SomerBG,TsaiDE,DownsL, et al. Improvement in Sjogren’s syndrome following therapy
with rituximab for marginal zone lymphoma. Arthritis Rheum 2003;49:394–8.
[136] Ramos-CasalsM, Lopez-GuillermoA, Brito-Zeron P, et al. Treatment of B-cell lymphoma
with rituximab in two patients with Sjogren’s syndrome associated with hepatitis C virus
infection. Lupus 2004;13:969–71.
[137] Ferri C, La Civita L, Longombardo G, et al. Mixed cryoglobulinaemia: a crossroad be-
tween autoimmune and lymphoproliferative disorders. Lupus 1998;7:275–9.
[138] Ferri C, Zignego AL. Relation between infection and autoimmunity in mixed cryoglobuli-
nemia. Curr Opin Rheumatol 2000;12:53–60.
[139] Silberbogen AK, Janke EA, Hebenstreit C. A closer look at pain and hepatitis C: prelimi-
nary data from a veteran population. J Rehabil Res Dev 2007;44:231–44.
[140] Piperno A, D’Alba R, Roffi L, et al. Hepatitis C virus infection in patients with idiopathic
hemochromatosis (IH) and porphyria cutanea tarda (PCT). Arch Virol Suppl 1992;4:
215–6.
[141] Fargion S, PipernoA, CappelliniMD, et al. Hepatitis C virus and porphyria cutanea tarda:
evidence of a strong association. Hepatology 1992;16:1322–6.
[142] Ferri C, Baicchi U, la Civita L, et al. Hepatitis C virus-related autoimmunity in patients
with porphyria cutanea tarda. Eur J Clin Invest 1993;23:851–5.
[143] Navas S, Bosch O, Castillo I, et al. Porphyria cutanea tarda and hepatitis C and B viruses
infection: a retrospective study. Hepatology 1995;21:279–84.
[144] Nagao Y, Sata M, Tanikawa K, et al. Lichen planus and hepatitis C virus in the northern
Kyushu region of Japan. Eur J Clin Invest 1995;25:910–4.
634 ZIGNEGO & CRAXI
[145] Carrozzo M, Gandolfo S, Carbone M, et al. Hepatitis C virus infection in Italian patients
with oral lichen planus: a prospective case–control study. J Oral Pathol Med 1996;25:
527–33.
[146] Bagan JV, Ramon C, Gonzalez L, et al. Preliminary investigation of the association of oral
lichen planus and hepatitis C. Oral Surg OralMedOral Pathol Oral Radiol Endod 1998;85:
532–6.
[147] MignognaMD,LoMuzioL,FaviaG, et al.Oral lichenplanus andHCV infection: a clinical
evaluation of 263 cases. Int J Dermatol 1998;37:575–8.
[148] del Olmo JA, Pascual I, Bagan JV, et al. Prevalence of hepatitis C virus in patients with li-
chen planus of the oral cavity and chronic liver disease. Eur J Oral Sci 2000;108:378–82.
[149] Cribier B, Garnier C, Laustriat D, et al. Lichen planus and hepatitis C virus infection: an
epidemiologic study. J Am Acad Dermatol 1994;31:1070–2.
[150] GroteM, Reichart PA, Berg T, et al. Hepatitis C virus (HCV) infection and oral lichen pla-
nus. J Hepatol 1998;29:1034–5.
[151] IngafouM, Porter SR, Scully C, et al. No evidence of HCV infection or liver disease in Brit-
ish patients with oral lichen planus. Int J Oral Maxillofac Surg 1998;27:65–6.
[152] van derMeij EH, van derWaal I. Hepatitis C virus infection and oral lichen planus: a report
from The Netherlands. J Oral Pathol Med 2000;29:255–8.
[153] NagaoY, Kameyama T, SataM. Hepatitis C virus RNA detection in oral lichen planus tis-
sue. Am J Gastroenterol 1998;93:850.
[154] Arrieta JJ, Rodriguez-InigoE, CasqueiroM, et al. Detection of hepatitis C virus replication
by In situ hybridization in epithelial cells of antihepatitis C virus-positive patients with and
without oral lichen planus. Hepatology 2000;32:97–103.
[155] Hussain I, Hepburn NC, Jones A, et al. The association of hepatitis C viral infection with
porphyria cutanea tarda in the Lothian region of Scotland. Clin Exp Dermatol 1996;21:
283–5.
[156] O’Reilly FM, Darby C, Fogarty J, et al. Porphyrin metabolism in hepatitis C infection.
Photodermatol Photoimmunol Photomed 1996;12:31–3.
[157] Tembl JI, Ferrer JM, Sevilla MT, et al. Neurologic complications associated with hepatitis
C virus infection. Neurology 1999;53:861–4.
[158] Lidove O, Cacoub P, Maisonobe T, et al. Hepatitis C virus infection with peripheral neu-
ropathy is not always associated with cryoglobulinaemia. Ann Rheum Dis 2001;60:290–2.
[159] Rosner I, RozenbaumM, Toubi E, et al. The case for hepatitis C arthritis. Semin Arthritis
Rheum 2004;33:375–87.
[160] Fiore CE, Riccobene S, Mangiafico R, et al. Report of a new case with involvement of the
OPG/RANKL system. Osteoporos Int 2005;16:2180–4.
[161] Manganelli P, Giuliani N, Fietta P, et al. OPG/RANKL system imbalance in a case of hep-
atitis C-associated osteosclerosis: the pathogenetic key? Clin Rheumatol 2005;24:296–300.
[162] Muzio AD, Bonetti B, Capasso M, et al. Hepatitis C virus infection and myositis: a virus
localization study. Neuromuscul Disord 2002;13:68–71.
[163] Pateron D, Hartmann DJ, Duclos-Vallee JC, et al. Latent autoimmune thyroid disease in
patients with chronic HCV hepatitis. J Hepatol 1992;16:244–5.
[164] HuangMJ,WuSS, LiawYF. Thyroid abnormalities in patientswith chronic viral hepatitis.
Hepatology 1994;20:1651–2.
[165] Preziati D, LaRosa L, Covini G, et al. Autoimmunity and thyroid function in patients with
chronic active hepatitis treatedwith recombinant interferon alfa-2a. Eur J Endocrinol 1995;
132:587–93.
[166] Fernandez-Soto L, Gonzalez A, Escobar-Jimenez F, et al. Increased risk of autoimmune
thyroid disease in hepatitis C vs hepatitis B before, during, and after discontinuing inter-
feron therapy. Arch Intern Med 1998;158:1445–8.
[167] HuangMJ, Tsai SL,HuangBY, et al. Prevalence and significance of thyroid autoantibodies
in patients with chronic hepatitis C virus infection: a prospective controlled study. Clin En-
docrinol (Oxf) 1999;50:503–9.

635EXTRAHEPATIC MANIFESTATIONS OF HEPATITIS C VIRUS
[168] Prentice LM, Phillips DI, SarseroD, et al. Geographical distribution of subclinical autoim-
mune thyroid disease in Britain: a study using highly sensitive direct assays for autoanti-
bodies to thyroglobulin and thyroid peroxidase. Acta Endocrinol (Copenh) 1990;123:
493–8.
[169] Lenzi M, Johnson PJ, McFarlane IG, et al. Antibodies to hepatitis C virus in autoimmune
liver disease: evidence for geographical heterogeneity. Lancet 1991;338:277–80.
[170] McFarlane IG. Autoimmunity and hepatotropic viruses. Semin Liver Dis 1991;11:
223–33.
[171] Minelli R, Braverman LE, Giuberti T, et al. Effects of excess iodine administration on thy-
roid function in euthyroid patients with a previous episode of thyroid dysfunction induced
by interferon-alfa treatment. Clin Endocrinol (Oxf) 1997;47:357–61.
[172] Marazuela M, Garcia-Buey L, Gonzalez-Fernandez B, et al. Thyroid autoimmune disor-
ders in patients with chronic hepatitis C before and during interferon-alfa therapy. Clin En-
docrinol (Oxf) 1996;44:635–42.
[173] Antonelli A, Ferri C, Fallahi P. Thyroid cancer in patients with hepatitis C infection.
JAMA 1999;281:1588.
[174] Montella M, Crispo A, Pezzullo L, et al. Is hepatitis C virus infection associated with thy-
roid cancer? A case–control study. Int J Cancer 2000;87:611–2.
[175] Antonelli A, Ferri C, Fallahi P, et al. Thyroid cancer in HCV-related mixed cryoglobuline-
mia patients. Clin Exp Rheumatol 2002;20:693–6.
[176] Zignego AL, Ferri C, Pileri SA, et al. Extrahepatic manifestations of hepatitis C virus in-
fection: a general overview and guidelines for a clinical approach. Dig Liver Dis 2007;39:
2–17.
[177] Hsieh MC, YuML, ChuangWL, et al. Virologic factors related to interferon-alfa induced
thyroid dysfunction in patients with chronic hepatitis C. Eur J Endocrinol 2000;142:431–7.
[178] PrummelMF, Laurberg P. Interferon-alfa and autoimmune thyroid disease. Thyroid 2003;
13:547–51.
[179] Muratori L, BogdanosDP,Muratori P, et al. Susceptibility to thyroid disorders in hepatitis
C. Clin Gastroenterol Hepatol 2005;3:595–603.
[180] Simo R, Hernandez C, Genesca J, et al. High prevalence of hepatitis C virus infection in
diabetic patients. Diabetes Care 1996;19:998–1000.
[181] Caronia S, Taylor K, Pagliaro L, et al. Further evidence for an association between nonin-
sulin-dependent diabetesmellitus and chronic hepatitis C virus infection. Hepatology 1999;
30:1059–63.
[182] KnoblerH, SchihmanterR, ZifroniA, et al. Increased risk of type 2 diabetes in noncirrhotic
patients with chronic hepatitis C virus infection. Mayo Clin Proc 2000;75:355–9.
[183] Mehta SH, Brancati FL, SulkowskiMS, et al. Prevalence of type 2 diabetes mellitus among
persons with hepatitis C virus infection in the United States. Ann Intern Med 2000;133:
592–9.
[184] MasonA.Viral induction of type 2 diabetes and autoimmune liver disease. JNutr 2001;131:
2805S–8S.
[185] Ryu JK, Lee SB, Hong SJ, et al. Association of chronic hepatitis C virus infection and di-
abetes mellitus in Korean patients. Korean J Intern Med 2001;16:18–23.
[186] Antonelli A, Ferri C, Fallahi P, et al. Hepatitis C virus infection: evidence for an association
with type 2 diabetes. Diabetes Care 2005;28:2548–50.
[187] Noto H, Raskin P. Hepatitis C infection and diabetes. J Diabetes Complications 2006;20:
113–20.
[188] Mason AL, Lau JY, Hoang N, et al. Association of diabetes mellitus and chronic hepatitis
C virus infection. Hepatology 1999;29:328–33.
[189] Ishizaka N, Ishizaka Y, Takahashi E, et al. Association between hepatitis C virus seropos-
itivity, carotid artery plaque, and intima–media thickening. Lancet 2002;359:133–5.
[190] Ishizaka N, Ishizaka Y, Takahashi E, et al. Increased prevalence of carotid atherosclerosis
in hepatitis B virus carriers. Circulation 2002;105:1028–30.
636 ZIGNEGO & CRAXI
[191] Ueda T, Ohta K, Suzuki N, et al. Idiopathic pulmonary fibrosis and high prevalence of se-
rum antibodies to hepatitis C virus. Am Rev Respir Dis 1992;146:266–8.
[192] OhtaK, Ueda T, Nagai S, et al. Pathogenesis of idiopathic pulmonary fibrosisdis hepatitis
C virus involved? Nihon Kyobu Shikkan Gakkai Zasshi 1993;315:32–5.
[193] Ferri C, La Civita L, Fazzi P, et al. Interstitial lung fibrosis and rheumatic disorders in pa-
tients with hepatitis C virus infection. Br J Rheumatol 1997;36:360–5.
[194] Matsumori A, Ohashi N, HasegawaK, et al. Hepatitis C virus infection and heart diseases:
a multicenter study in Japan. Jpn Circ J 1998;62:389–91.
[195] Boddi M, Abbate R, Chellini B, et al. HCV infection facilitates asimptomatic carotid ath-
erosclerosis: preliminary report of HCV RNA localization in human carotid plaques. Dig
Liver Dis 2007;39:54–9.
[196] Dwight MM, Kowdley KV, Russo JE, et al. Depression, fatigue, and functional disability
in patients with chronic hepatitis C. J Psychosom Res 2000;49:311–7.
[197] FortonDM, ThomasHC,MurphyCA, et al. Hepatitis C and cognitive impairment in a co-
hort of patients with mild liver disease. Hepatology 2002;35:433–9.
[198] Hilsabeck RC, Perry W, Hassanein TI. Neuropsychological impairment in patients with
chronic hepatitis C. Hepatology 2002;35:440–6.
[199] Cozzi A, Zignego AL, Carpendo R, et al. Low serum tryptophan levels, reduced macro-
phage IDO activity and high frequency of psychopathology in HCV patients. J Viral Hepat
2006;13:402–8.
[200] Korsmeyer SJ. BCL-2 gene family and the regulation of programmed cell death. Cancer
Res 1999;59:1693s–700s.
[201] TigheH,WarnatzK, BrinsonD, et al. Peripheral deletion of rheumatoid factor B cells after
abortive activation by IgG. Proc Natl Acad Sci U S A 1997;94:646–51.