BILE S M - prime.edu.pkprime.edu.pk/infoserver/Dr_Sara_Amjad/2nd Year MBBS/Bile Metabolism.pdfBILE...
55
Transcript of BILE S M - prime.edu.pkprime.edu.pk/infoserver/Dr_Sara_Amjad/2nd Year MBBS/Bile Metabolism.pdfBILE...

BILE SECRETION AND
METABOLISM
Dr Sara Amjad
FUNCTIONS OF LIVER
Synthetic functions
Metabolic functions
Bile secretion
Detoxification
Immunity
3
GALLBLADDER FUNCTION
• The gallbladder concentrates bile and stores much of
the bile salt pool during fasting
Isotonicity maintained as a result of micelles
having minimal osmotic activity
• Postprandially the gallbladder contracts in
response to CCK (cholecystokinin)
BILE
Is made up of bile salts, bile pigments and other
substances dissolved in alkaline electrolyte solution
Enter duodenum through bile duct
Storage in gall bladder( in between meals sphinctor of
oddi closed,when food enter duodenum sphinctor
releases and gall bladder evacuates)
PROPERTIES OF BILE
pH : 7.2
Daily secretion: 500 ml.
Colour: Yellow
Taste: Bitter
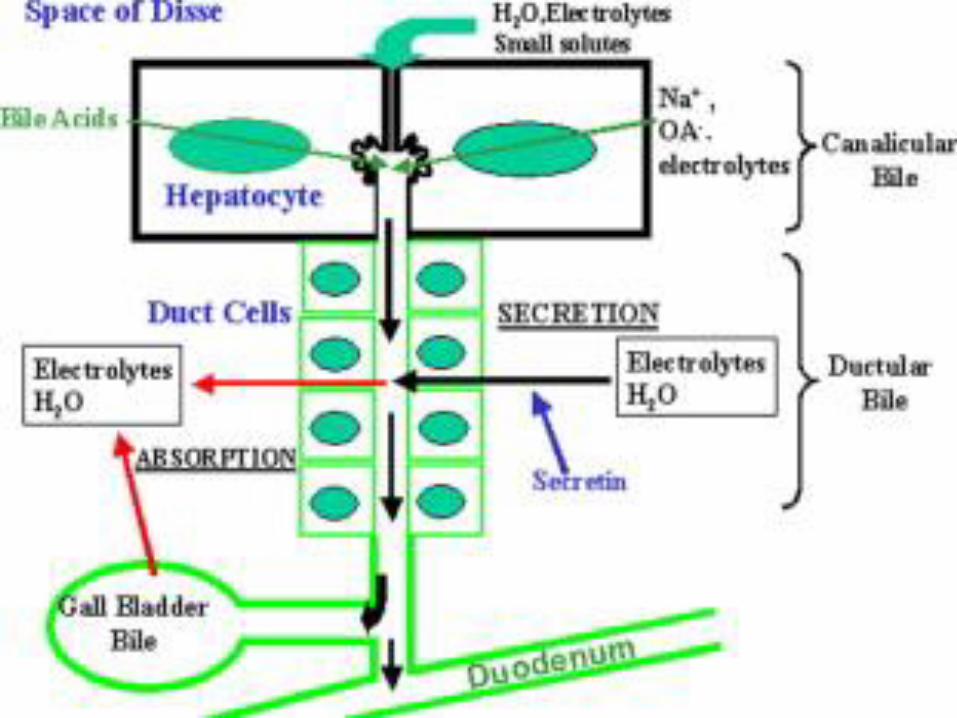
BILE SECRETION
Bile is secreted in two stages ;
Stage one;
Hepatocytes will secret an initial secretion that is rich
bile salts
cholesterol,
organic components,
initial secretion will drain through the many minute bile
canaliculi that penetrate the liver.
Stage Two ;
Initial secretion will flow towards the bile ducts ,
secondary secretion is added to the initial bile
which is a watery solution of sodium bicarbonate
ions.
The bile then will either empty into the
duodenum when the sphincter of Oddi is open
when the sphincter of Oddi is closed, it will be
prevented from draining into the intestine and
instead flows into the gallbladder, and
concentrated to up to five times its original
potency
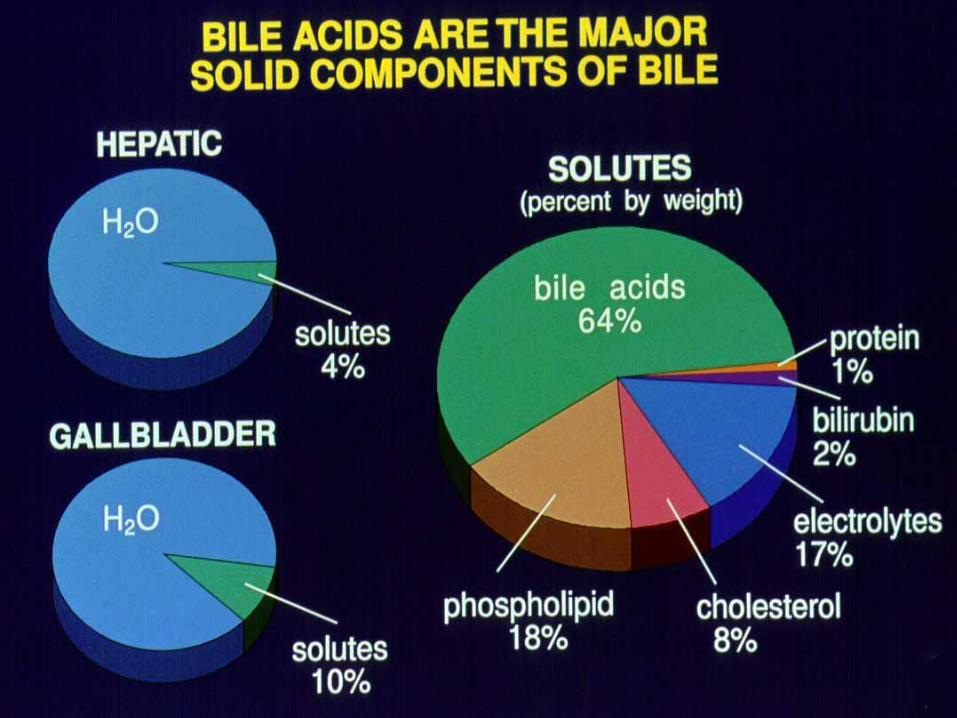
COMPOSITION OF BILE
Water : 97 percent
Solids : 3 percent
Solids
Organic
Inorganic
Inorganic mainly bicarbonates
Na, Cl and K and calcium palmitate
Organic
Bile salts
Bile pigments
Mucin
lipids
Alkaline phosphatase
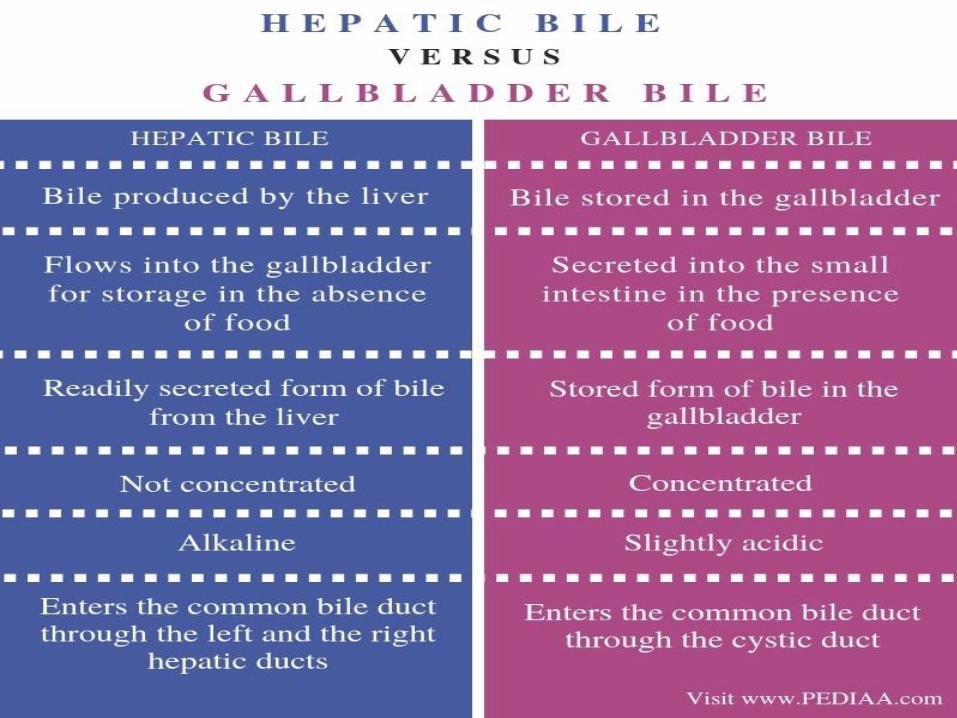
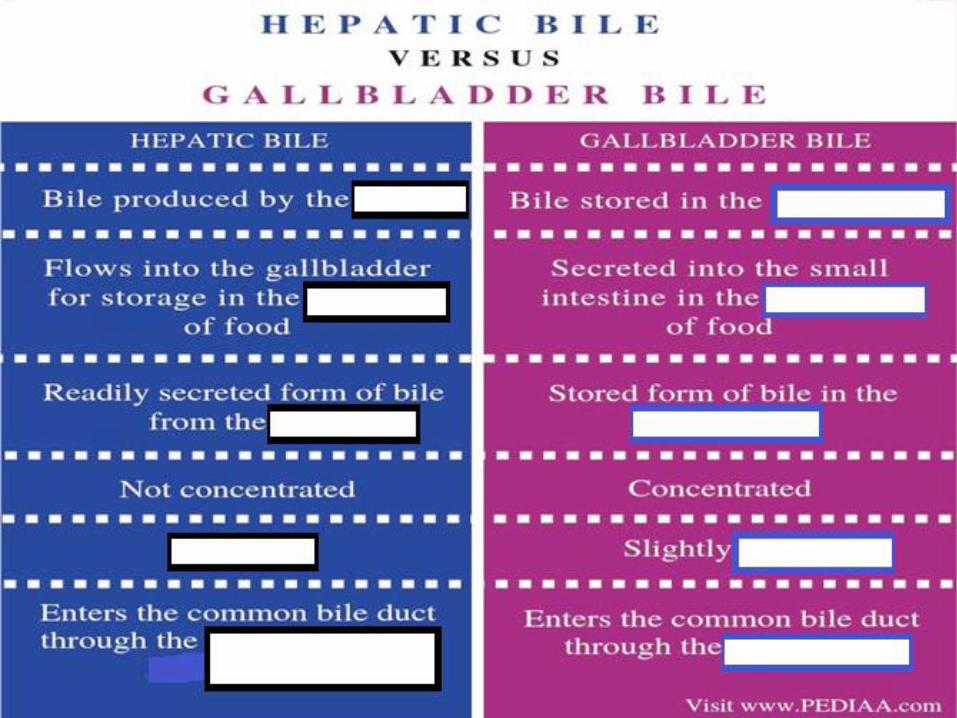
Gall bladder bile differs from Hepatic bile
1. Gall bladder capacity is 50ml
Inflammation of gall bladder
2. Exchange of H for Na
pH acidic
raised pH precipitates CaCO3
3. Mucin secretion
other subtances secreted are copper ,zinc and mercury
COMPOSITION OF BILE
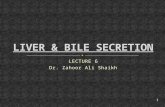
Bile acids
Bile acid :Primary bile acids are produced by
hepatocytes from cholesterol. They are cholic acid &
chenodeoxycholic acid.
They reach duodenum through bile duct and in the
small intestine and colon they are converted into
secondary bile acids deoxycholic acid and lithocholic
acid by bacterial action.
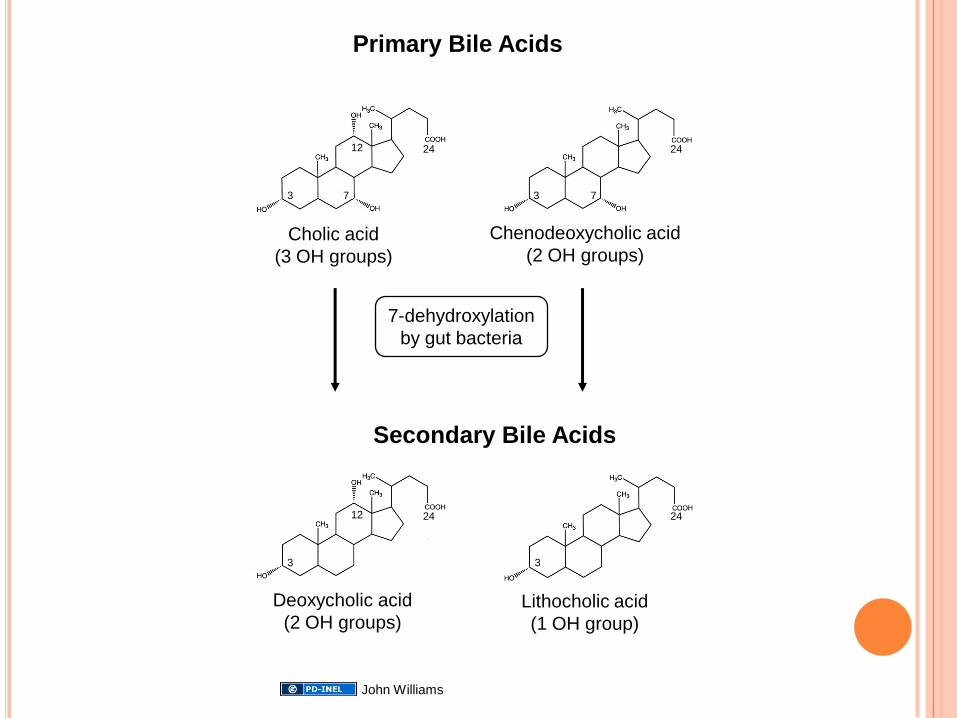
7-dehydroxylation
by gut bacteria
Cholic acid
(3 OH groups)
Chenodeoxycholic acid
(2 OH groups)
Secondary Bile Acids
Deoxycholic acid
(2 OH groups)Lithocholic acid
(1 OH group)
33
3 3
7 7
12
12 24
24
24
24
Primary Bile Acids
John Williams
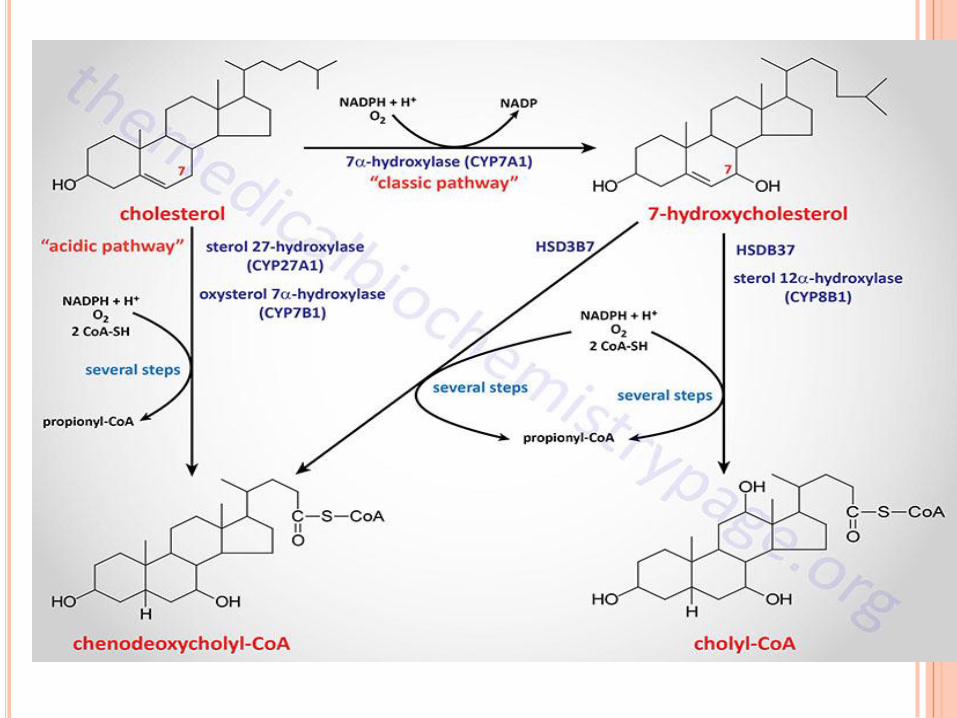
BILE ACID SYNTHESIS
Bile acids synthesized in the liver from cholesterol
In the “classical pathway” the first and most important regulated step is 7α hydroxylation by 7α hydroxylase
Next 12α hydroxylation is followed by several steps leading to cholic acid
The “alternative pathway” starts with initial formation of oxysterols and leads to chenodeoxycholic acid
BILE SALTS
Bile acids are first conjugated with taurine and glycine
to form bile salts in combination with Na or K
Sodium taurocholate & glycocholates
Potassium taurocholate & glycocholate.
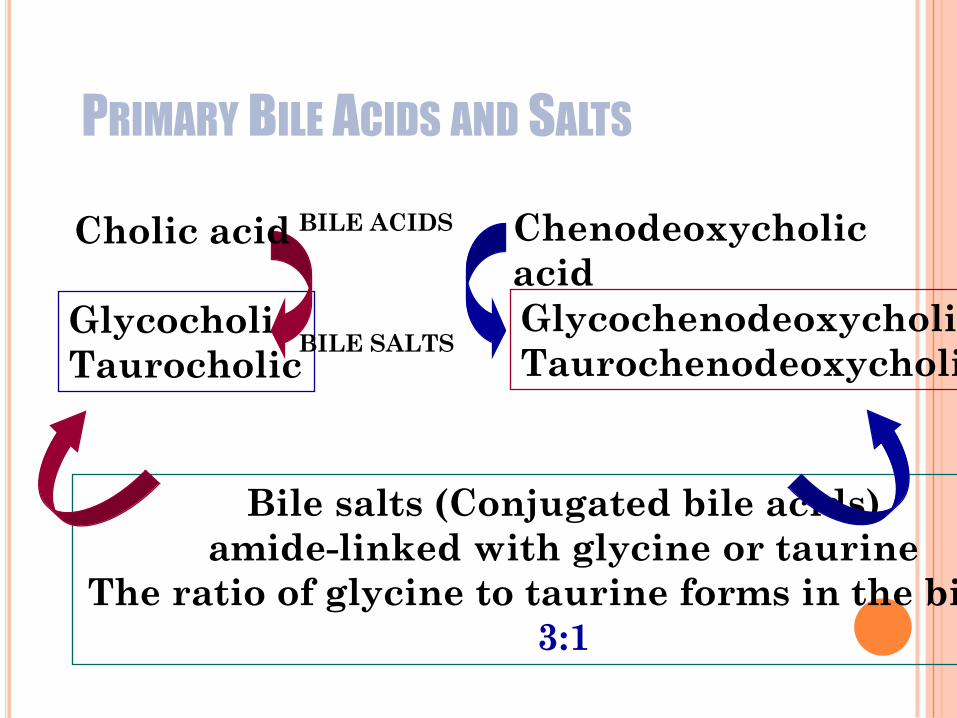
PRIMARY BILE ACIDS AND SALTS
Chenodeoxycholic
acid
Bile salts (Conjugated bile acids)
amide-linked with glycine or taurine
The ratio of glycine to taurine forms in the bile is
3:1
Glycocholic
Taurocholic
Glycochenodeoxycholic
Taurochenodeoxycholic
Cholic acid BILE ACIDS
BILE SALTS
BILE PIGMENTS
They are excretory products in the bile.
Formed by breakdown of Hb
15 to 20 % of the total solid of hepatic bile
Hemolytic disease
CHOLESTEROL
Every day 2gm of cholesterol is excreted in bile
Increased polyunsaturated fatty acids
Ratio of cholesterol to bile salt 1:20 and 1:30
If ratio falls1:13 , cholesterol precipitated
Immunoglobulins…IgA
Calcium palmitate…Formation of biliary calculi
Alkaline phosphatase…raised level of this
enzyme indicates obstruction to biliary flow
ROLE OF BILE
Emulsification of Fat
Breaking down of the large fat globules into smaller globules and make them water
soluble.
Bile …...Amphipathic
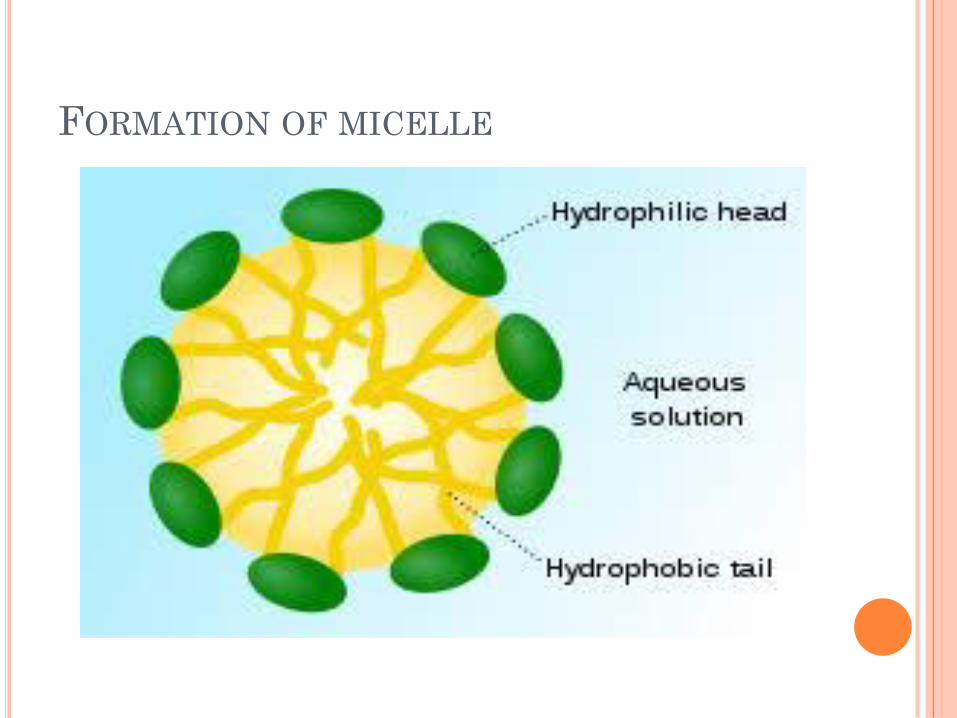
FORMATION OF MICELLE
After digestion, monoglycerides and fatty acids
associate with bile salts and phopholipids to form
micelles.
Micelles are necessary because they transport
the poorly soluble monoglycerides and fatty acids
to the surface of the enterocyte where they can be
absorbed
Activate pancreatic lipase
Role in fat digestion and absorption
BACTERIOSTATIC ACTION
Inhibits multiplication of pathogenic intestinal
bacteria
ROUTE FOR LOSS OF CHOLESTEROL
Major route for loss of cholesterol from body
Bile salts keeps cholesterol in soluble form, thus
prevents stone formation
Lubrication
Lubricating function due to mucus
Laxative action
Bile salts
Neutralization of HCl
High content of bicarbonate
Neutralize any HCl escape to intestine
Excretion
Drugs
Toxins
Bile pigments
Fat soluble vitamins
Steriods
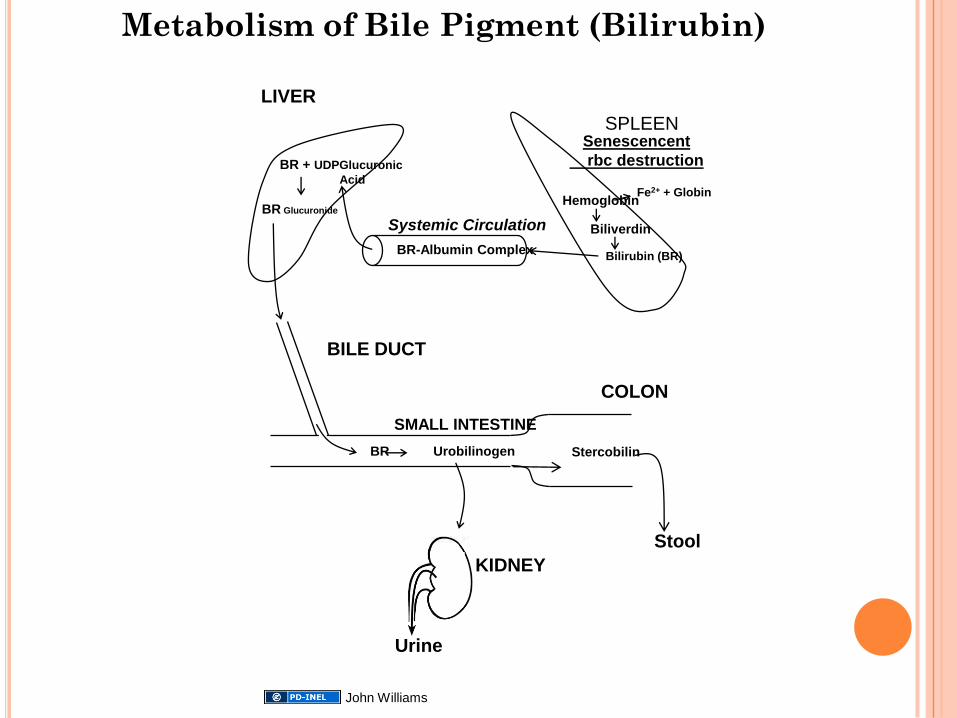
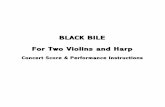
Metabolism of Bile Pigment (Bilirubin)
Systemic Circulation
BR-Albumin Complex
SMALL INTESTINE
BR Urobilinogen
BILE DUCT
LIVER
SPLEEN
Stercobilin
KIDNEY
Urine
COLON
BR + UDPGlucuronic
Acid
BR Glucuronide
Senescencent
rbc destruction
Hemoglobin
Biliverdin
Bilirubin (BR)
Fe2+ + Globin
Stool
John Williams
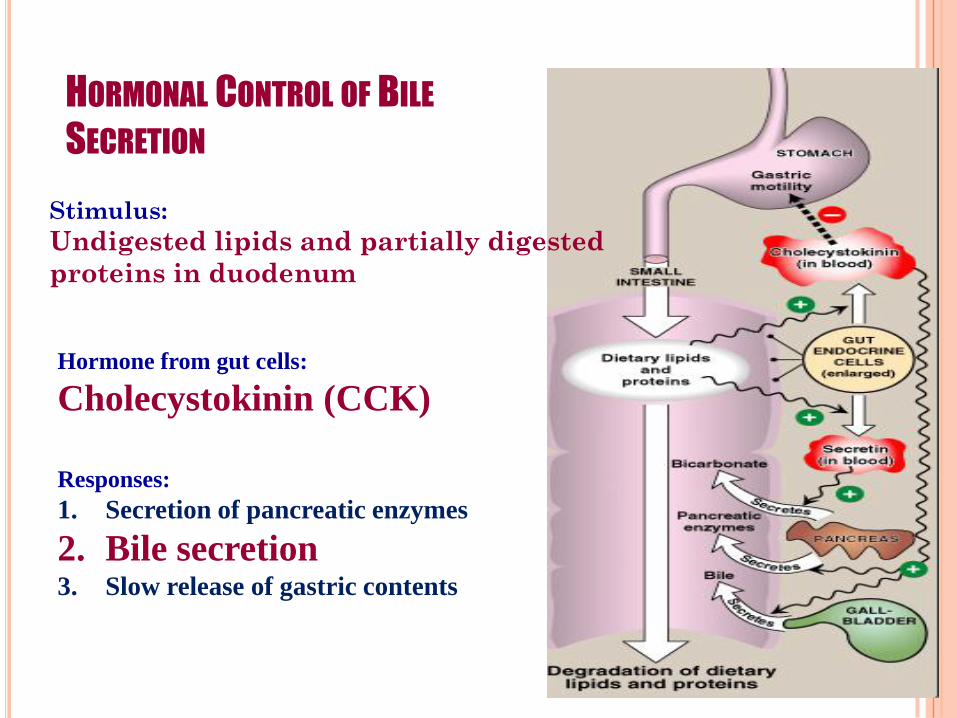
HORMONAL CONTROL OF BILE
SECRETION
Hormone from gut cells:
Cholecystokinin (CCK)
Responses:
1. Secretion of pancreatic enzymes
2. Bile secretion3. Slow release of gastric contents
Stimulus:
Undigested lipids and partially digested
proteins in duodenum
FACTORS AFFECTING BILIARY SECRETION
Choleretic action
Bile salts
Ingestion of food
Heptocrinin , Secretin , CCK
CHOLAGOGUE ACTION
Bile salts, magnesium sulphate
CCK
stimulate contraction and evacuation of gall bladder
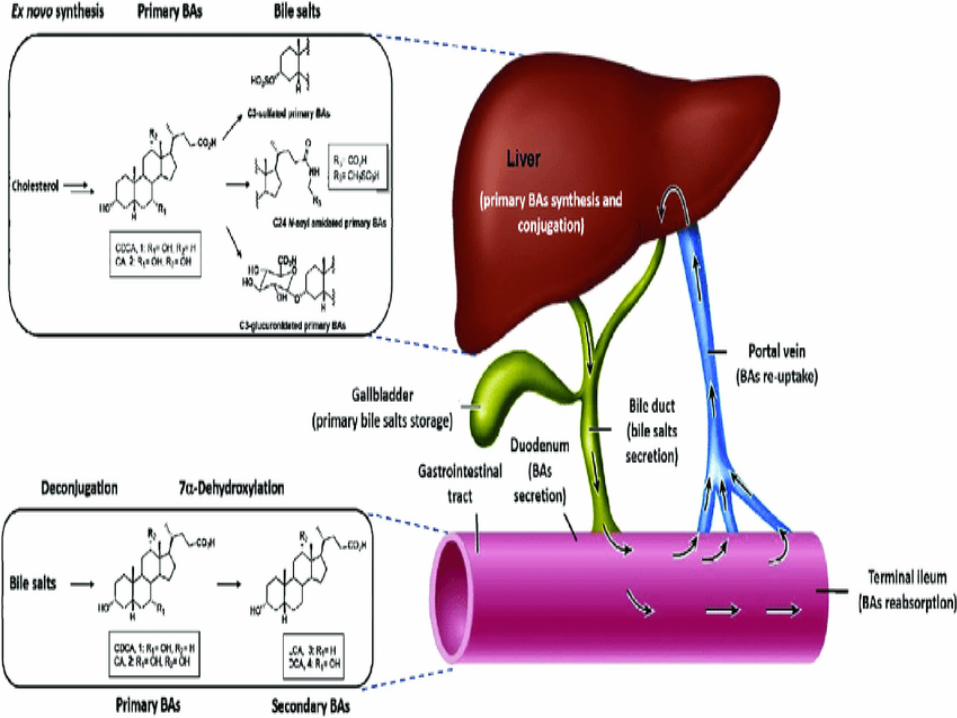
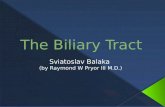
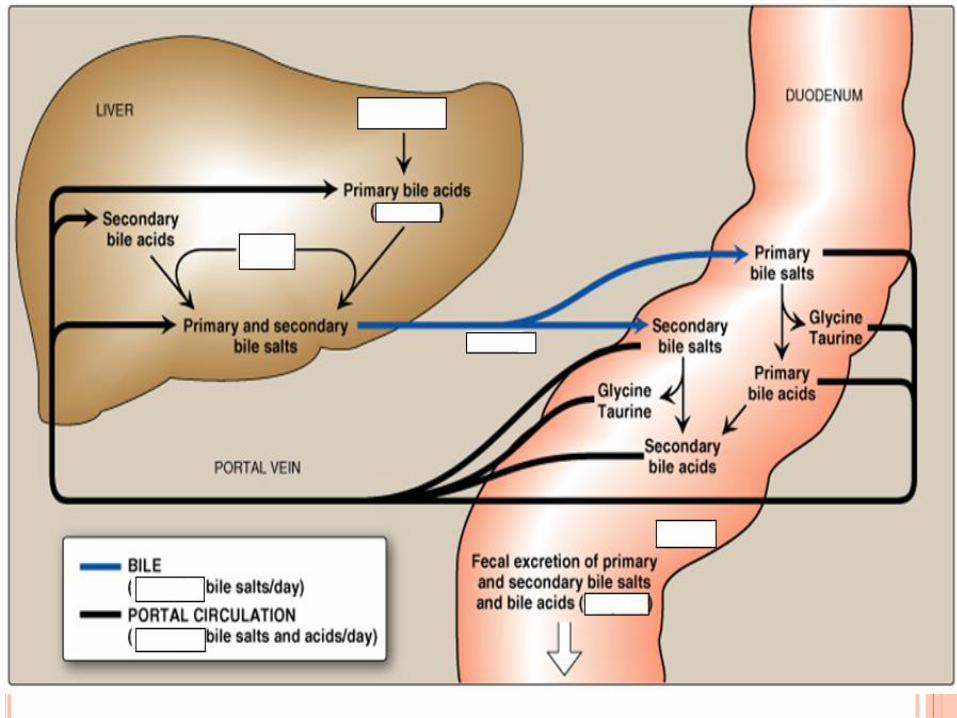
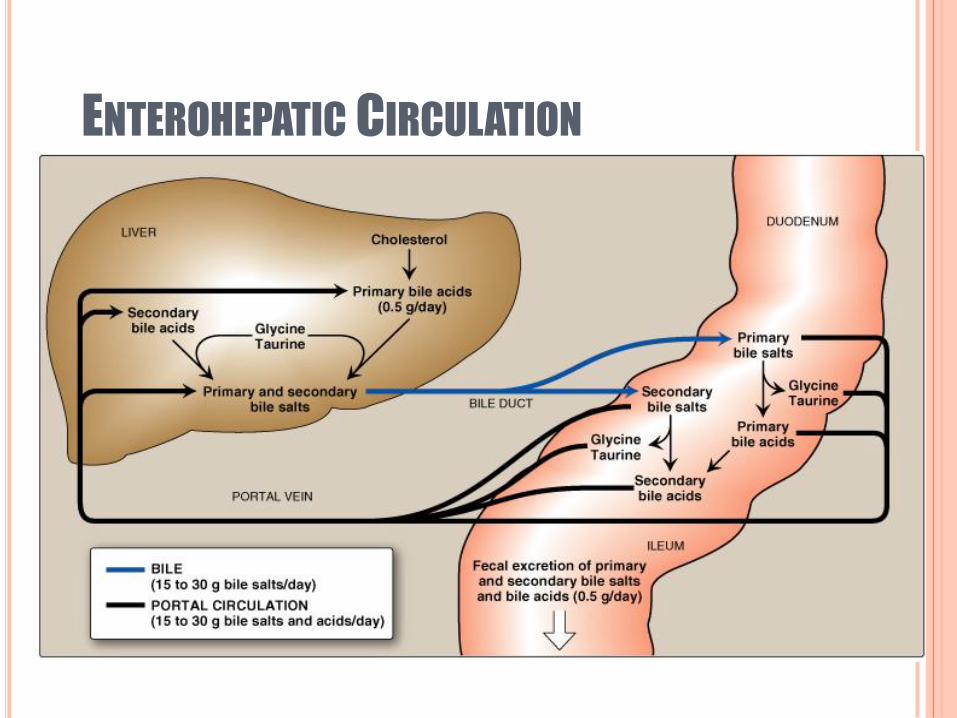
ENTEROHEPATIC CIRCULATION
94% of bile salts are reabsorbed from the small
intestine( by diffusion in early part of intestine &
by active transport from distal ileum).
portal blood
liver
bile salts are absorbed back into the hepatic cells
reexcreted into the bile.
94% bile salts re circulated into bile,
Salts make the entire circuit some 17 times before
being carried out in the feces.
Small quantities of bile salts lost in to the feces are
replaced by new amount formed continuously by liver
cells.
Necessary because of limited pool of bile salts
BILE ACID POOL
Fecal loss of bile acids 0.3 to 0.6g/day.
compensated by an equal daily synthesis of bile
acids by liver and bile acid pool is maintained.
Normal bile acid pool 2 to 4g.
Bile acids returning to the liver suppress hepatic
synthesis of bile acids by inhibiting the rate
limiting enzyme
Maximum rate of synthesis is approximately
0.5g/day
ENTEROHEPATIC CIRCULATION
Cholestyramine:
Bile acid sequestrants
It binds to bile acids in the gut
Prevents reabsorption
Promoting their excretion
It is used for treatment of
hypercholesterolemia
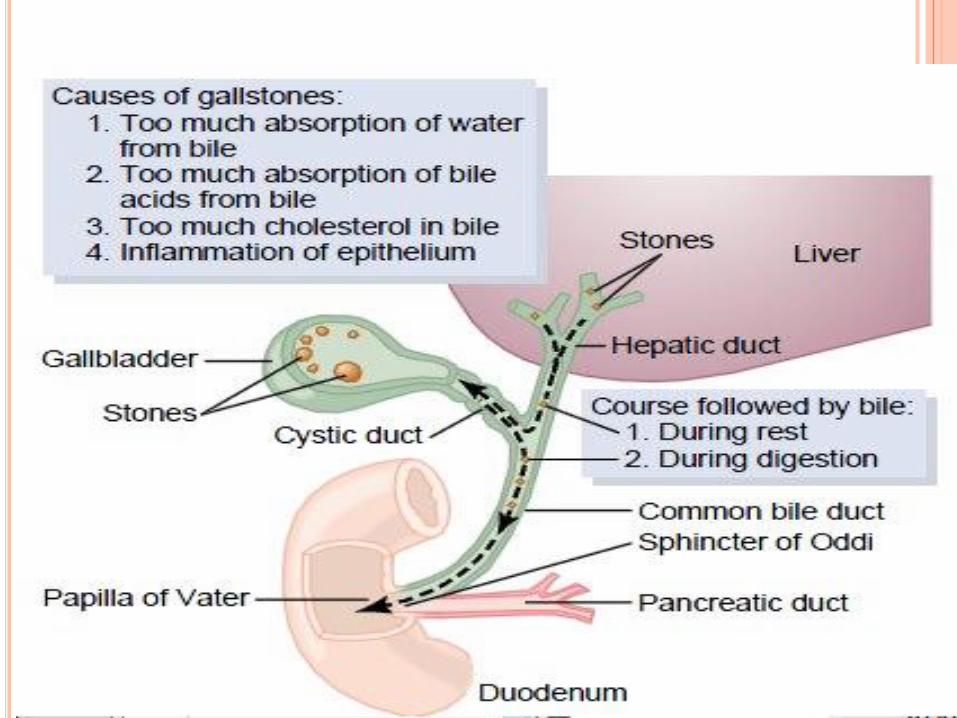
GALLSTONES
Cholesterol, ordinarily insoluble in water, comes
into solution by forming vesicles with
phospholipids
If ratio of cholesterol, phospholipids, and bile
salts altered, cholesterol crystals may form
Gallstone formation involves a variety of factors:
Cholesterol supersaturation
Mucin hypersecretion by the gallbladder mucosa
creates a viscoelastic gel that fosters nucleation.
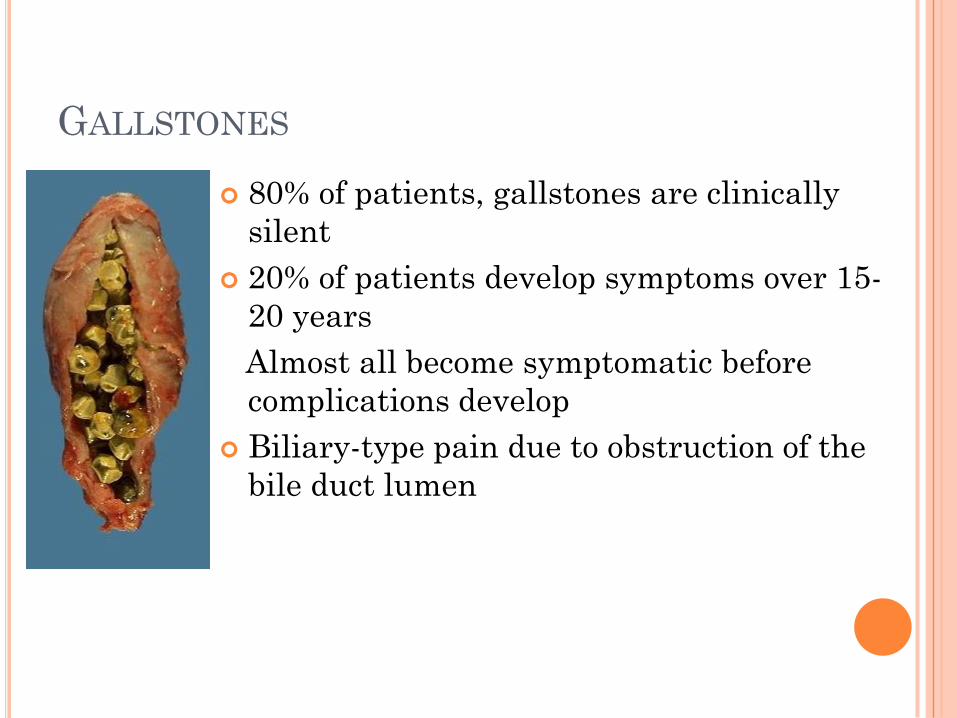
GALLSTONES
80% of patients, gallstones are clinically
silent
20% of patients develop symptoms over 15-
20 years
Almost all become symptomatic before
complications develop
Biliary-type pain due to obstruction of the
bile duct lumen
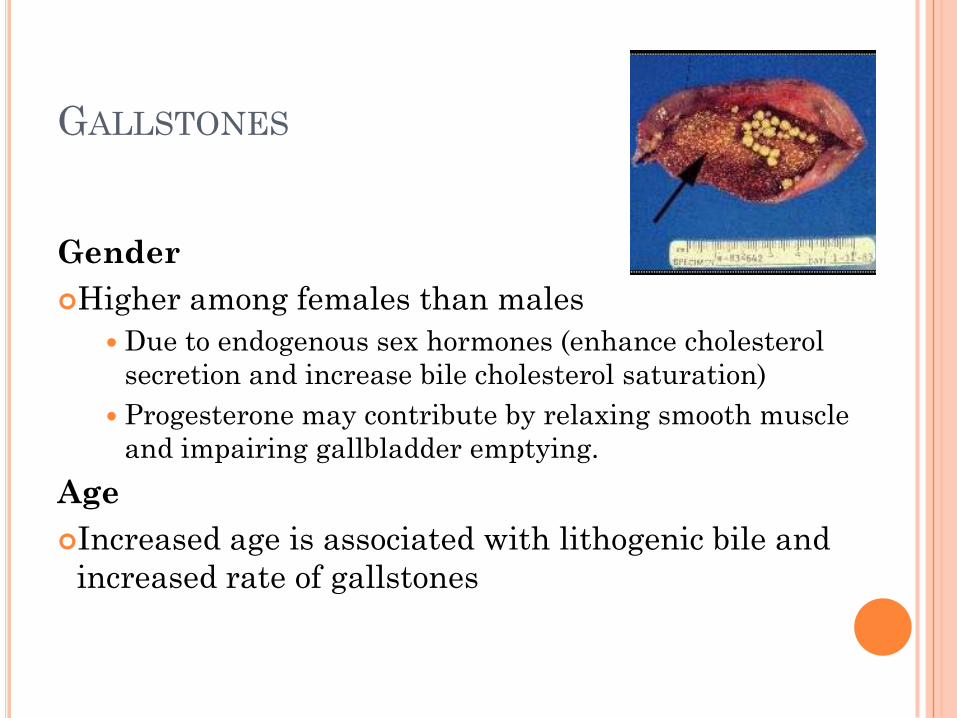
GALLSTONES
Gender
Higher among females than males
Due to endogenous sex hormones (enhance cholesterol
secretion and increase bile cholesterol saturation)
Progesterone may contribute by relaxing smooth muscle
and impairing gallbladder emptying.
Age
Increased age is associated with lithogenic bile and
increased rate of gallstones
GALLSTONES SYMPTOMS
Abdominal pain
Nausea and vomiting
Jaundice
Fatigue
Weight loss
Fatty food intolerance
STEATORRHEA
An increase in stool fat excretion of > 6% of dietary fat
Absence of bile acids, fats become indigestible and are
excreted in feces.
OBSTRUCTIVE JAUNDICE
Jaundice resulting from blockage of the bile ducts
or abnormal retention of bile in the liver.
CAUSES
gallstones
inflammation
tumors
trauma
pancreatic cancer
narrowing of the bile ducts
structural abnormalities present at birth
MCQ
The major site for synthesis of conjugated
bilirubin in human body is
A. Liver
B. Spleen
C. Kidney
D. Pancreas
MCQ
Primary bile acids are produced from cholesterol
in
A intestine
B kidney
C liver
D gall bladder
MCQ
Every day amount of cholesterol excreted in bile
A 3gm
B 2gm
C 4gm
D 1gm
ENTEROHEPATIC CIRCULATION