





Languages
Pages
Legal


WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Antimicrobial resistance – Biological basis and public health consequences
John Stelling, MD, MPHWHO Collaborating Centre for
Surveillance of Antimicrobial ResistanceBoston, USA

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
What is antimicrobial resistance?
• If a drug has no effect on a bacteria, the bacteria is Resistant to the compound
• Some resistance is ancient – intrinsic– E. coli and vancomycin– M. tuberculosis and penicillin
• A lot of it is new since 1930 – acquired– S. aureus and oxacillin– N. gonorrhoeae and penicillin

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Our universe – an overview
Big Bang The Sun Earth Bacteria Humans
12 Billion 10 Billion 6 Billion 4 Billion
Organisms have been producing “antibiotics” for billions of years – on a tiny scale! Humans have been using antibiotics on massive scales for the past seven decades
Present
ASM, © David Phillips/Visuals Unlimited
Dinosaurs
“Antibiotics” Antibioticuse

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
pABA DHF THF
Folate Synthesis PLASMID
CHROMOSOME
Protein Synthesis
Gram Positive Bacteria Gram Negative Bacteria
Cell Wall Synthesis
RNA Synthesis
DNA Synthesis
CELL WALLCELL MEMBRANE BIOFILM
RIBOSOMES
OUTER MEMBRANE
WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
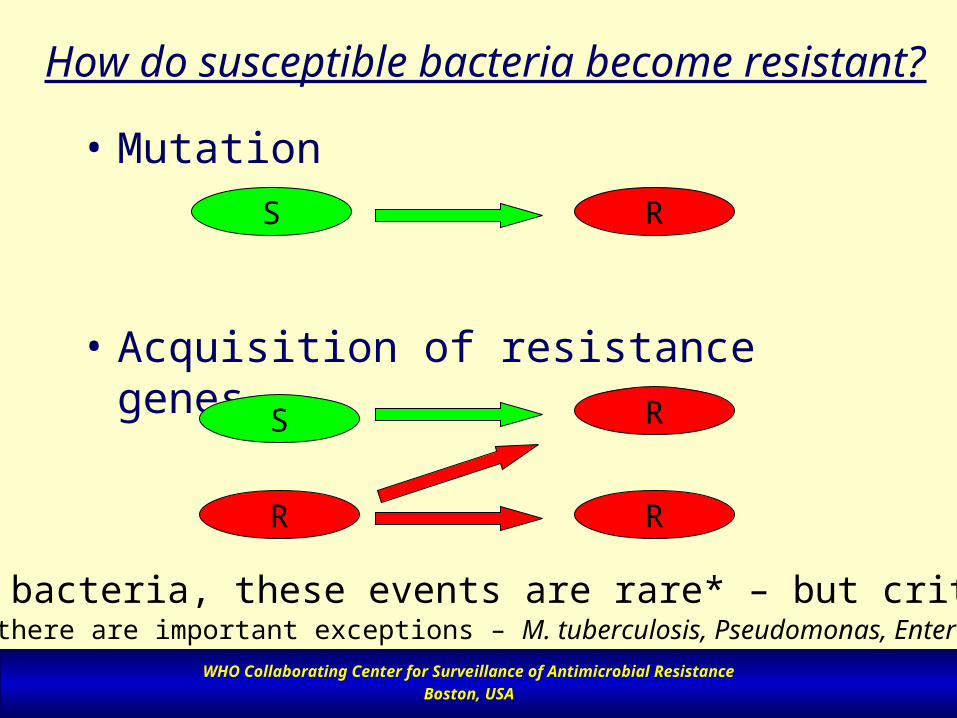
How do susceptible bacteria become resistant?
• Mutation
• Acquisition of resistance genes
S
R
S
R
R
R
In most bacteria, these events are rare* – but critical!* But there are important exceptions – M. tuberculosis, Pseudomonas, Enterobacter

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Why are resistant bacteria so common?
• Selection
• Spread

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Leading bacterial pathogens in 1900
Streptococcus pneumoniae Corynebacterium diphtheriaeStreptococcus pyogenes Mycobacterium tuberculosisStaphylococcus aureus Haemophilus influenzaeEscherichia coli Neisseria meningitidisVibrio cholerae Neisseria gonorrhoeaeShigella species Treponema pallidumSalmonella typhi

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Initial appearanceVancomycin-intermediate Staphylococcus aureus
Responses: confirmation, molecular characterization, diagnostic tools,active surveillance, notification of health care providers and generalpublic, review of treatment guidelines, development of new agents

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
SpreadStrep. pneumoniae: multi-resistant, virulent clones
Source: WHO Report WHO/CDS/BVI/95.7

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Emergence in hospitalsVancomycin-Resistant Enterococci, USA
0
2
4
6
8
10
12
14
% R
esis
tant
1989 1990 1991 1992 1993 1994
Intensive care units non-intensive care units
Source: National Nosocomial Infections Surveillance System, CDC, USA

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Emergence in the community Resistant E. coli in Healthy Children
0102030405060708090
100
% R
esis
tan
t
TetracyclineGentamicin Resistant to1 or more
drugs
Resistant to5 or more
drugs
United States
Venezuela
China
Source: Lester, NEJM 323:285-289

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Emergence in outbreaksShigella sp. in Rwanda, Amp+TMP Resistant
0
20
40
60
80
100
83 84 84 86 87 88 89 90 91 92 93
S. dysenteriae type1
S. flexneri
S. sonnei
S. boydii anddysenteriae 2-10
Resistance in S. dysenteriae type 1 has been high for many years.Resistance in other species has been increasing in recent years.

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
0
5
10
15
20
1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994
2 antimicrobial drugs 3 antimicrobial drugs
Pig isolates
Emergence in animals and humansResistant Salmonella Typhimurium, Netherlands
0
5
10
15
20
1984 1985 1986 1987 1988 1989 1990 1991 1992 1993 1994
Human isolates

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
The impact of 7 decades of antibiotic use and misuse on bacterial
populations
• Same pathogens as in 1930– BUT NOW WITH ACQUIRED RESISTANCE!!
• Plus many new species– Staph. epidermidis, Enterococcus, Pseudomonas, Klebsiella,
Acinetobacter, fungi, etc.– features:
• take advantage of changing societal demographics• take advantage of changes in health-care practice• intrinsic resistance to commonly used antimicrobials!!
The use of antibiotics has radically altered the microbial populations of the world and the epidemiology of infection

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
The impact of Antimicrobial resistance
• Consequences– morbidity and mortality– direct and indirect costs– transmission
• Antimicrobials are “societal” drugs. Antimicrobial use in one person affects us all

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Antimicrobial resistance as an unusual public health threat
• A problem created by medical innovation– antimicrobial use by patients, health-care providers,
food-producers, industry drives resistance trends
• A problem of dependence– Antimicrobial resistance is NOT a disease. It’s a
characteristic of many organisms which cause a wide variety diseases.
– If we can prevent or treat disease in other ways, resistance would cease to be a public health menace.

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Strategies for Containment of Antimicrobial resistance
John Stelling, MD, MPHWHO Collaborating Centre for
Surveillance of Antimicrobial ResistanceBoston, USA

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
• Target areas– Disease prevention and infection control– Access to antimicrobials– Appropriate use– Legislation and regulation– Surveillance– Focused research
• Target groups– patients and general community– hospitals, prescribers and dispensers– food animal industry– governments and health systems– international organizations– pharmaceutical and diagnostic industries– researchers
T h e M e d ic a l I m p a c t o f th e U s e o f A n t im ic r o b ia ls in F o o d A n im a ls
D iv is io n f o r E m e r g in g a n d o th e r C o m m u n ic a b le D is e a s e s S u rv e il la n c e a n d C o n tr o l
W o r ld H e a lth O r g a n iz a tio n
R e p o r t o f a W H O M e e t in g
B e r lin , G e r m a n y 1 3 -1 7 O c to b e r 1 9 9 7
W H O /E M C /Z O O /9 7 .4
D is t r . : G e n e r a l
E n g l ish o n ly
T h e M e d ic a l I m p a c t o f th e U s e o f A n t im ic r o b ia ls in F o o d A n im a ls
D iv is io n f o r E m e r g in g a n d o th e r C o m m u n ic a b le D is e a s e s S u rv e il la n c e a n d C o n tr o l
W o r ld H e a lth O r g a n iz a tio n
R e p o r t o f a W H O M e e t in g
B e r lin , G e r m a n y 1 3 -1 7 O c to b e r 1 9 9 7
W H O /E M C /Z O O /9 7 .4
D is t r . : G e n e r a l
E n g l ish o n ly

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
In using antimicrobials, we mustseek a balance:
• Increase appropriate use of antimicrobials– Ensure the provision of good quality therapy
to infected patients who needs antimicrobials: standard treatment guidelines, drug access, drug quality
• Decrease inappropriate use of antimicrobials– Through education, policy, and regulation,
decrease the use of antimicrobials where there is no benefit to patients

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Resistance emergence – Critical steps• New resistance
• Selection
• Spread
Mutations

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Factors promoting resistance
• Selection pressure – antibiotic use– intensive use: intensive care units, new antibiotics– indiscriminate use: for nonbacterial diseases– incorrect use: inappropriate agent, dosing, compliance– use in animals and food production
• Spread– poor sanitation and overcrowding in the community– inadequate control of infections in health care facilities– international travel

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
-lactam consumption and TEM -lactamase resistance in M. (B.) catarrhalis from Finnish
children
0%
20%
40%
60%
80%
100%
1978 1983 1988 1993 1998
Year
Resis
tanc
e
50.9% increase
Nissinen et al. (1995), Clinical Infectious Diseases, 21: 1193-6
Total -lactam consumption
4
5
6
7
8
9
1978 1981 1984 1987 1990 1993
Year
DD
Ds/1
000 in
habitants
Penicillins Cephalosporins

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
AMR Containment Interventions:Approaches
• General– Disease prevention: improved hygiene, water
quality, nutrition– Disease therapy: decreasing inappropriate use
of antibiotics, development of new agents
• Disease-specific– Disease prevention: vaccination– Disease therapy: improved disease diagnosis,
standard treatment guidelines

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Strategy 1: Reduce the need for antibiotics
• Disease prevention– use existing vaccines and develop new ones– improve nutrition, hygiene, and general health status
• New approaches for disease therapy– immune modulators, bacteriophages
• Evaluate the use of antibiotics in food production– decrease the use of antimicrobial growth promoters

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Strategy 2: Improve the use of antibiotics
• Do not use antibiotics when they do not benefit the patient
– Educate health workers and patients• Ensure quality of drug supply
– Regulation and control of the quality of antimicrobials available on the market
• Use standard treatment guidelines adapted for local resistance issues
– use narrow-spectrum where appropriate– reserve highly effective drugs– regulate and monitor antimicrobial prescription– do susceptibility testing when possible– optimize surgical prophylaxis– improve patient compliance

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
0
5
10
15
20
25
30
35
FR GR LU PT IT BE SK HR PL IS IE ES FI BG CZ SI SE HU NO UK DK DE LV AT EE NL
DD
D p
er 1
000
inh
. per
day
Total Outpatient antibiotic use in 26 European countries in 2002

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Consumption of the Fourth Generation Cephalosporins in Ambulatory Care in 26
European Countries in 2002
0.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
IT GR BG PL LV LU CZ BE AT FI SE SK DE NL FR PT ES HU HR IE SI IS UK DK EE NO
DD
D p
er 1
000
inh
. per
day
Cefpirome
Cefepime

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Factors Influencing Drug Use
DRUG USE
Cultural Beliefs
Knowledge Deficits Unbiased
Information
RelationWith Peers
Authority &Supervision
Influence of Industry
Workload & Staffing
Infra-structure
Acquired Habits
Patient Demand
Interpersonal
Workplace
Workgroup
PersonalInformational

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Penicillin consumption (1991-1996) and penicillin resistance (1988-2000) in S. pneumoniae from
Icelandic children
0%
5%
10%
15%
20%
25%
1988 1990 1992 1994 1996 1998 2000
Year
Resis
tanc
e
12.9% reduction
No intervention
Antimicrobial consumption
15
15.5
16
16.5
17
17.5
18
18.5
19
19.5
1991 1992 1993 1994 1995 1996
Year
DD
Ds/
1000
child
ren

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Strategy 3: Decrease transmission
• Communities– improve sanitation and hygiene
• Health-care facilities– strengthen hospital infection control: hand-
washing, sterilization techniques, quality control, use of face masks

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
New Drug Development – 1995 -2005
• 80 FDA Drug Approvals for Anti-Infectives– 17 Antibacterials– 27 Anti-HIV– 23 Other antivirals– 7 Antifungals– 6 Antiparasitics

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
FDA Approved Antibacterials – 1995-2006
• 17 Antibacterials– 10 “New” Compounds – but no novel drug classes
• Ceftibuten, cefditoren• Moxifloxacin, trovafloxacin, gatifloxacin• Telithromycin, dirithromycin• Ticarcillin+clavulanic acid• Quinupristin/dalfopristin• Rifaximin
– 7 Reformulations of existing compounds• Clarithromycin, azithromycin• Metronidazole• Clindamycin• Cefazolin
• Two removed from market because of toxicity concerns
– Trovafloxacin, gatifloxacin

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Disincentives to New Drug Development
• Because of resistance, anti-infectives lose efficacy over time
• Short courses of patient therapy• Tight restrictions on the use of new agents• Many competitors with very good safety
profiles• For “me too” drugs, resistance can emerge
rapidly

WHO Collaborating Center for Surveillance of Antimicrobial ResistanceBoston, USA
Conclusion
• Resistance is an unavoidable consequence of the use of anti-infective agents on diverse microbial populations
• Prudent antimicrobial use must thus aim to balance– the necessity of treating infected patients today with– the need for efficacious treatment options in
the future
Top Related