






Languages
Pages
Legal


The Egyptian Journal of Radiology and Nuclear Medicine (2012) 43, 119–128
Egyptian Society of Radiology and Nuclear Medicine
The Egyptian Journal of Radiology andNuclearMedicine
www.elsevier.com/locate/ejrnmwww.sciencedirect.com
ORIGINAL ARTICLE
Value of contrast enhanced spoiled gradient (SPGR)
MR and MIP MR imaging in diagnosis of peri-anal fistula
Jehan A. Mazroaa, Sabry A. Elmogy a, Mohamed M. Elgendy b,*
a Diagnostic Radiology Department, Faculty of Medicine, Mansoura University, Egyptb General Surgery Department, Faculty of Medicine, Mansoura University, Egypt
Received 22 December 2011; accepted 11 January 2012Available online 15 February 2012
A
an
an*
E-
03
M
Pe
N
do
Op
KEYWORDS
MRI of peri-anal fistula;
Post contrast MRI of fistula
in ano;
MIP imaging in peri-anal
fistula
bbreviations: EAS, external an
esthesia; FSE, fast spin echo
al sphincter; MIP, maximumCorresponding author.
mail address: jehanras2@ho
78-603X � 2012 Egyptian
edicine. Production and host
er review under responsibility
uclear Medicine.
i:10.1016/j.ejrnm.2012.01.004
Production and h
en access under CC BY-NC-ND li
al sphinc
; SPGR, s
intensity
tmail.com
Society
ing by El
of Egyp
osting by E
cense.
Abstract Purpose: To assess the value of the combination of contrast enhanced T1 spoiled gradi-
ent (SPGR) MR and maximum intensity projection (MIP) MR imaging in the complete pre-oper-
ative evaluation of peri-anal fistula.
Patients and methods: This prospective study contained 28 patients with clinical diagnosis of peri-
anal fistula, they were performed MRI using the following sequences in both axial and coronal
planes: Pre contrast T2FSE, T1FSE and Post contrast SPGR. MIP reformated images were done
using the SPGR sequence. Fistulas were classified according to Parks (6) classification, they were
evaluated regarding site, type, extensions, complications and diagnostic accuracy of each sequence.
Our findings were correlated with operative findings.
Results: Fourteen patients had inter-sphincteric fistulas (50%), 8 patients had trans-sphincteric fis-
tulas (28.6%) and 6 patients had supra-sphincteric fistulas (21.4%). Simple non branching tracts
were found in 22 patients, branching tracts in 6 patients, abscess cavity in 5 patients, horseshoe
extension in 4 patients. Overall diagnostic accuracy of post contrast T1 SPGR was 97.3% and
MIP MR imaging was 100%. Post contrast T1 SPGR accurately evaluated all patients but missed
one faint horseshoe extension and other fine para anal branches. MIP imaging accurately evaluated
all the extensions and ramifications but was poor in depth orientation.
ter; EUA, examination under
poiled gradient; IAS, Internal
projection.
(M.M. Elgendy).
of Radiology and Nuclear
sevier B.V.
tian Society of Radiology and
lsevier

120 J.A. Mazroa et al.
Conclusion: MRI is a reliable diagnostic modality in the evaluation of peri-anal fistulas. Post con-
trast T1 SPGR sequence with its high resolution images and excellent anatomical orientation pro-
vides almost all the necessary details for accurate evaluation. Although MIP images lack depth
orientation their high sensitivity, rotational 2D and 3D capabilities exquisitely depict all the fine
ramifications and extensions. The combination of both provides complete evaluation and highest
possible diagnostic accuracy aiding successful surgical interventions, aiming to reduce complica-
tions and recurrences.
� 2012 Egyptian Society of Radiology and Nuclear Medicine. Production and hosting by Elsevier B.V.
Open access under CC BY-NC-ND license.
1. Introduction
Idiopathic perianal-fistulas result from anal gland sepsis lo-cated at the dentate line in the mid anal canal. However,peri-anal fistulas may also be caused by other conditions and
events, including Crohn’s disease, tuberculosis, trauma duringchildbirth, pelvic infection, pelvic malignancy, and radiationtherapy (1–5). Infection can penetrate the internal sphincter
to lie in the intersphincteric plane, tracking downward to theperi-anal skin in 70% of patients, alternatively, infectionmay pass through both layers of the anal sphincter to reachthe ischio-anal fossa and, eventually, the peri-anal skin
(trans-sphincteric fistulization) in 25%. In other cases, infec-tion tracks upward over the levator muscle to reach abovethe levator plane and then penetrate inferiorly through the
ischio-anal fossa (suprasphincteric fistulization) in 5%. Sepsisarising within the pelvis may track down to the skin throughthe ischio-rectal fossa, resulting in fistulas that are referred
to as extrasphincteric in less than 1%. Abscess cavities maydevelop along the course of fistulous tracts (6–10).
Imaging of peri-anal fistula done previously by fistulogra-
phy is unreliable and difficult to interpret. Because the sphinc-ter complex and levator ani sling are not directly visualizedand secondary fistulous tracks often fail to fill with contrastmaterial. Anal endosonography has proved inferior to expert
clinical assessment. The sphincter mechanism and intersphinc-teric plane are usually well visualized with endosonography,but the external sphincter can be difficult to assess in some
individuals. In addition, infection cannot be distinguishedfrom fibrosis and insufficient depth penetration results in afailure to identify secondary ramifications and more distant
sepsis (11–13). In computed tomography, performed with rec-tally and intravenously administered contrast media, the atten-uation values for the sphincters, levator ani, fibrotic fistulous
tracks, and active fistulas are so similar that it is difficult tocharacterize these structures accurately, unless the track con-tains gas or leaked contrast material (11–13).
MRI has become the method of choice for evaluating peri-
anal fistulas due to its ability to display the anatomy of thesphincter muscles orthogonally. The MR imaging appearanceof this condition shows greater concordance with surgical find-
ings than does any other imaging evaluation. Spoiled gradientrecalled acquisition in the steady state (SPGR) MR sequence ischaracterized by superior soft tissue contrast compared with
T1-weighted spin echo (SE) technique. As SPGR can be per-formed in sections of 1 mm, the spatial resolution of the ac-quired images is improved. The use of gadolinium incombination with fat-suppression techniques increases the
conspicuity of the lesions, allowing the diagnosis to be made
with confidence (14–16). MIP subtraction MR fistulography
images (processed from post contrast T1 images) resulted invisualization of fistulas as high-signal tubular structures con-taining varying degrees of low-signal fluid with dark appear-
ance of the surrounding fat (21,22).
1.1. Aim of the work
The aim was to assess the value of the combination of contrast
enhanced T1 spoiled gradient (SPGR) MR and MIP MRimaging in the complete pre-operative evaluation of peri-analfistula.
2. Patients and methods
Our prospective study was conducted at a private center in
Mansoura, Egypt from the period of June 2010 till December2011. It contained 28 patients (21 males and 7 females), theirage ranged from 28 to 50 years with a mean age of 39 years,
all referred from surgical clinic ofMansouraUniversity hospitalto performMRI, they were initially diagnosed by the surgeon tohave peri-anal fistula or abscess by clinical examinations. Pa-
tients’ complaints were local pain ± discharge. No history ofdiabetes mellitus or recurrent perianal fistula or pelvic diseaseswas found. Fistulas were classified anatomically according toParks et al (6) classification: inter-sphincteric, trans-sphincteric
and supra-sphincteric fistulas. Location of internal opening wasdetermined in axial images with respect to the clock face with 12o’clock being directed anterior.
All patients performed MRI using GE 1.5 Tesla medicalsystem with a phased array body coil. Patients were placedin a supine head-first position with the coil centered on the
hip joints. No bowel preparation or catheterization of the analcanal or fistulas was required.
Sequences used were: pre contrast: axial, coronal T2FSE/T1FSE, post contrast: axial and coronal T1 SPGR. All images
were done with fat suppression. MIP reformatted algorithmswere done using the SPGR sequence. Oblique coronal imageswere obtained parallel to the anal canal, and axial images were
obtained perpendicular to the coronal plane.
2.2. Parameters used
2.2.1. Axial and coronal T2 FSE
TR/TE: 4820-6680/101-107, FOV: 26–31 · 26–31, NEX: 2,
matrix: 320 · 192–224, slice thickness: 4–5 mm, time: 2 min.

Value of contrast enhanced spoiled gradient (SPGR) MR 121
2.2.2. Axial and coronal T1 FSE
TR/TE: 480-600/9.5, FOV: 26 · 26, NEX: 2, matrix:
320 · 224, slice thickness: 5 mm, time: 1.40 min.
2.2.3. Contrast enhanced axial and coronal T1 SPGR
TR/TE: 410-460/3, FOV: 26 · 26, NEX: 2, matrix: 512 · 192,
slice thickness: 4–5 mm, time: 2.30 min. Dose of I.V. Gadolin-ium was: 0.1 mmol/kg body, injected automatically at a rate of1 mL/s.
Post contrast MIP reformat in axial, coronal and obliqueprojections, time: 2.30 min.
Images covered the levator muscle, the anal canal, the
sphincter muscles, the ischio-rectal fossa, and the pelvis toevaluate the presence of supralevator extension.
MRI findings were correlated with the surgical results and
exploration.Written consent was obtained from our patients. Approval
of the ethics committee was taken.
2.3. Image analysis
In each case, careful evaluation of the following data wasmade: type of the fistula according to the Parks classification:
intersphincteric, transsphincteric, suprasphincteric and extra-sphincteric, the radial site and location of the internal opening(defined as either the continuation of the primary tract itself
into the anal mucosa or the site closest to the maximal inflam-mation found in the intersphincteric region), fistulous tractwhether simple or branching, abscess formation, possible sec-
ondary tracts, possible supralevator extension, horseshoetracts (crossing the midline), distance between the internalopening and anal verge.
3. Results
Our study contained 28 patients (21 males, 7 females) withtheir age ranging from 28 to 50 years with a mean age of
39 years. Fourteen patients had inter-sphincteric fistulasFig. 1, 8 had trans-sphincteric (Figs. 2 and 5) and 6 had su-pra-sphincteric fistula (Figs. 3 and 4). All patients had active
fistulous tract (containing fluid inside). Twenty-two patientsshowed non branching fistulas (inter and trans-sphincteric)while 6 patients showed branching fistulas (trans and supra
sphincteric). Five patients showed para anal abscess .Four pa-tients showed horseshoe extension, these findings were shownin Table 1.
T2 FSE with fat suppression revealed simple non branchingtract in 20 patients (out of 22), revealed 4 patients with branch-ing tracts (out of 6). It detected the internal opening in 25 pa-tients (out of 28), horseshoe extension in 2 patients (out of 4),
supra levator extension in 4 patients (out of 6). It successfullydetected all patients with para anal abscess (5).
Post contrast T1 SPGR revealed simple non branching
tract in all the 22 patients, revealed 5 patients with branchingtracts (out of 6). It detected the internal opening in all the 28patients, horseshoe extension in 3 patients (out of 4), supra
levator extension in all the 6 patients. It successfully detectedall patients with para anal abscess (5).
Post contrast MIP reformat revealed simple non branchingtract in all the 22 patients, revealed all the 6 patients with
branching tracts. It detected the internal opening in all the28 patients horseshoe extension in all the 4 patients, supralevator extension in all the 6 patients. It successfully detected
all patients with para anal abscess (5).Overall, diagnostic accuracy of T2 FSE was: 84.9%, post
contrast T1 SPGR was: 97.3%, post contrast MIP imaging
was: 100%. These findings are shown in (Table 2).
4. Discussion
The aim of surgical treatment of peri-anal fistulas is to treat thepatient’s symptoms, with low recurrence rates and risk ofincontinence. The anal canal is 2.5–4 cm long. The dentate line
(histologic junction between anal squamous epithelium andrectal columnar epithelium) runs underneath the anal valves.Accurate anatomical mapping of fistulas and potential peri-
anal suppuration, secondary extensions and relationship tothe pelvic floor, sphincters and adjacent peri-rectal structuresis of paramount importance for treatment decisions and sur-gery planning (17,18).
External anal sphincter is striated muscle (is the continua-tion of pelvic floor musculature) appears on MRI as hypoin-tense signal on T1WI, T2WI, and fat suppressed T2WI.
Internal sphincter is smooth muscle (is the continuation ofthe inner circular muscle layer of the lower rectum) appearshypointense on T1WI, T2WI, and relatively hyperintense on
fat suppressed T2WI, shows enhancement in post contraststudy. The pubo-rectalis ring is thickening of the superior fi-bers of EAS, merges superiorly with levator plate (19,20).
Low peri-anal fistulas are defined as fistulas of which the fis-
tula tract is located in the lower third of the external analsphincter. High fistulas are fistulas in which the fistula tractruns through the upper two-thirds of the external sphincter
muscle. Low peri-anal fistulas can be treated safely by fistulot-omy. At present, rectal advancement is the gold standard forthe surgical treatment of high trans sphincteric peri-anal fistu-
las (21,22).Investigators in a large study in which endo-anal MRI was
compared with body coil MRI found a surgical concordance
rate of 68% for endo-anal MRI as compared to 96% for bodycoil MRI because endoluminal coils are susceptible to motionartifact, has limited field of view (about 2–3 cm from the coil)missing distant extensions, sometimes difficult to place owing
to anal stenosis or local pain as a result of extensive infectionand expensive tools [single use] (23–24), in our study, body coilMRI with different sequences successfully detected all fistulous
tracts and extensions.The exact location of the internal opening can be difficult to
define, whatever the imaging modality used. Two questions
need to be answered. What is the radial site, and what is its le-vel? The vast majority of anal fistulas open into the anal canalat the level of the dentate line. Furthermore, most fistulas alsoenter posteriorly, around the 6-o’clock position (4). In our
study, T2FSE accurately detected the internal opening in 25 pa-tients. Post contrast T1 SPGR and MIP images detected theinternal opening in all the 28 patients, they were located
approximately at the dentate line, half of them around 6 o’clock(Figs. 3–5), other half in other different sites (Figs. 1 and 2).
The commonest type of extension is one that arises from the
apex of a transsphincteric tract and extends into the roof of theischioanal fossa. The major benefit of MR imaging findings is

Fig. 1 (A–G) Patient with LT. Inter-sphincteric fistula(Park type I). (A and B) Axial and coronal T2FSE respectively showing no evident
abnormalities. (C–E) Axial (C,D) and coronal (E) post contrast T1 SPGR revealed small LT. inter sphincteric fistula (arrow),with no
extension beyond the external sphincter (double arrows) or ischio-anal fossa(arrow heads). Fistula with its internal opening is seen at 1
o’clock. (F,G) Axial and coronal MIP imaging respectively clearly revealed the inter-sphincteric fistula with clear peri-anal fat. Note good
differentiation between internal and external anal sphincters in coronal plane (G).
122 J.A. Mazroa et al.
that they can alert the surgeon to extensions that would other-wise be missed. It is also important to search for supralevatorextensions since these are not only difficult to detect but pose
specific problems with regard to treatment. In the contraststudy, the internal sphincter muscle enhances to a higher de-gree than the external sphincter muscle. Therefore, the delinea-
tion of intersphincteric fistulous tracts and horseshoeextensions in the intersphincteric space may be improved(21,22). In our study, SPGR and MIP images accurately de-tected all the 6 patients with supralevator extensions. T2FSE
detected 4 patients (Figs. 3 and 4).Horseshoe extensions spread across both sides of the inter-
nal opening and are recognized on MR images by their unique
configuration. Horseshoe extensions may be intersphincteric,ischio-anal, or supralevator. Complex extensions are especiallycommon in patients with recurrent fistula in ano or in those
who have Crohn’s disease (24–27). Our study revealed 4 pa-tients with horseshoe extension, all detected by MIP imaging,while post contrast SPGR and T2FSE revealed 3 and 2 pa-
tients, respectively (Figs. 2 and 5).Active tracts are filled with pus and granulation tissue
and, thus, appear as hyperintense longitudinal structures onT2-weighted or STIR images .On contrast-enhanced T1-
weighted images, active granulation tissue will enhance whilefluid in the tract itself remains hypointense. Active tracts areoften surrounded by hypointense fibrous walls, which can be
relatively thick, especially in patients with recurrent diseaseand previous surgery. Occasionally, some hyperintensity inthis fibrous area may be seen, probably reflecting edema.
Hyperintensity may also extend beyond the tract and its fi-brous sleeve, where it represents adjacent inflammation (24–27). Post contrast SPGR and MIP images in our study clearlydepicted the fibrous tract, internal fluid and surrounding
edema.Abscess cavities may develop along the course of fistulous
tracks. Characteristically, the abscesses associated with inter-
sphincteric fistulas are peri-anal or indeed encysted withinthe inter-sphincteric space. Trans sphincteric fistulas are typi-cally associated with ischiorectal fossa abscesses.
Intersphincteric abscesses and secondary fistulous tracksare well shown by dynamic contrast-enhanced MR imaging.On these contrast-enhanced images, the pus in the central cav-
ity has low signal intensity and is surrounded by a brightlyenhancing rim (2). In our study, abscess cavities were correctlyidentified using the three sequences: T2FSE, post contrastSPGR and MIP imaging (Figs. 2 and 4).

Fig. 2 (A–H). Patient with RT trans-sphincteric peri-anal fistula and abscess formation(Park type II). (A and B) Axial and coronal T2
FSE respectively showing faint RT trans-sphincteric fistula extending to peri-anal fat (arrow) with abscess formation (arrow head). (C–F)
post contrast axial (C,D: from superior to inferior) and coronal (E,F: from posterior to anterior) T1 SPGR clearly showing fistulous tract
with internal opening at 12 o’clock(arrow), fistulous tract (arrow head) and abscess formation (curved arrow). Note no supra levator
extension. (G,H) Axial and coronal MIP imaging clearly depicts the fistulous tract extensions and ramifications.
Value of contrast enhanced spoiled gradient (SPGR) MR 123
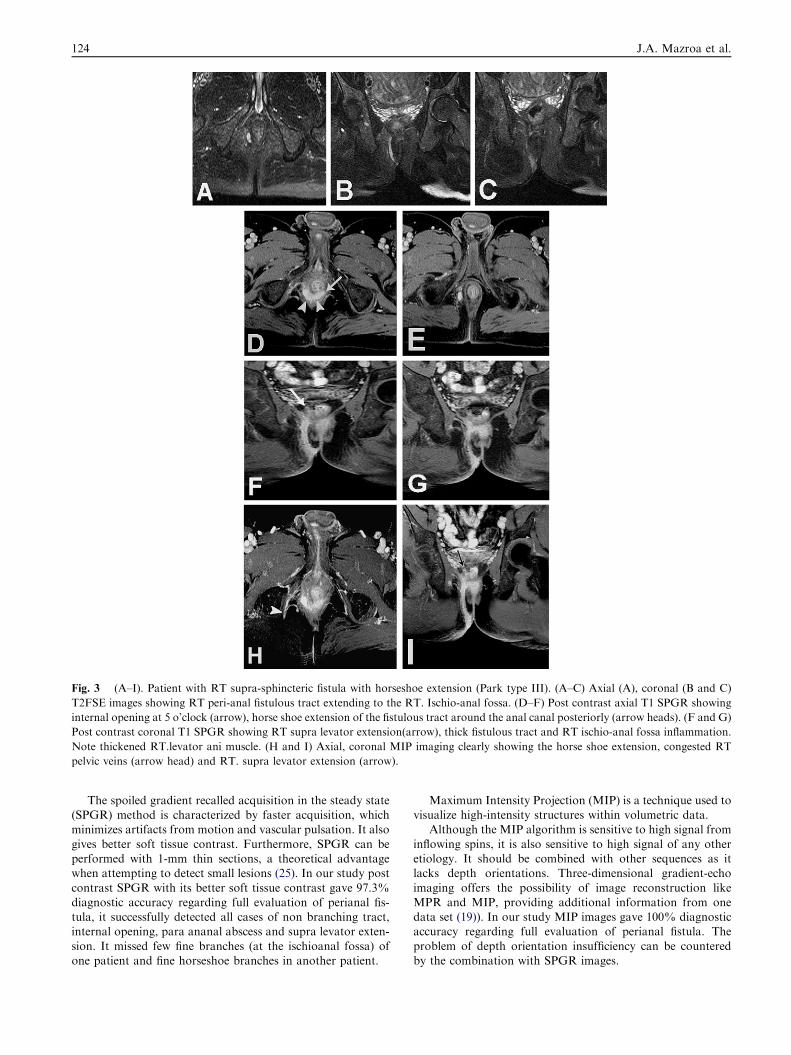
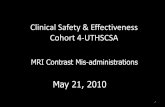
Fig. 3 (A–I). Patient with RT supra-sphincteric fistula with horseshoe extension (Park type III). (A–C) Axial (A), coronal (B and C)
T2FSE images showing RT peri-anal fistulous tract extending to the RT. Ischio-anal fossa. (D–F) Post contrast axial T1 SPGR showing
internal opening at 5 o’clock (arrow), horse shoe extension of the fistulous tract around the anal canal posteriorly (arrow heads). (F and G)
Post contrast coronal T1 SPGR showing RT supra levator extension(arrow), thick fistulous tract and RT ischio-anal fossa inflammation.
Note thickened RT.levator ani muscle. (H and I) Axial, coronal MIP imaging clearly showing the horse shoe extension, congested RT
pelvic veins (arrow head) and RT. supra levator extension (arrow).
124 J.A. Mazroa et al.
The spoiled gradient recalled acquisition in the steady state(SPGR) method is characterized by faster acquisition, whichminimizes artifacts from motion and vascular pulsation. It also
gives better soft tissue contrast. Furthermore, SPGR can beperformed with 1-mm thin sections, a theoretical advantagewhen attempting to detect small lesions (25). In our study post
contrast SPGR with its better soft tissue contrast gave 97.3%diagnostic accuracy regarding full evaluation of perianal fis-tula, it successfully detected all cases of non branching tract,internal opening, para ananal abscess and supra levator exten-
sion. It missed few fine branches (at the ischioanal fossa) ofone patient and fine horseshoe branches in another patient.
Maximum Intensity Projection (MIP) is a technique used tovisualize high-intensity structures within volumetric data.
Although the MIP algorithm is sensitive to high signal from
inflowing spins, it is also sensitive to high signal of any otheretiology. It should be combined with other sequences as itlacks depth orientations. Three-dimensional gradient-echo
imaging offers the possibility of image reconstruction likeMPR and MIP, providing additional information from onedata set (19)). In our study MIP images gave 100% diagnosticaccuracy regarding full evaluation of perianal fistula. The
problem of depth orientation insufficiency can be counteredby the combination with SPGR images.

Fig. 4 (A–J) Patient with RT supra-sphenctric fistula with large para anal abscess (Park type III). (A and B) Axial and coronal T2FSE
showing large RT. Para anal abscess. (C–E) Post contrast axial T1 SPGR from superior to inferior showing large RT. Para anal abscess,
internal opening at 6 o’clock (arrow). (F–H) Post contrast coronal T1 SPGR from posterior to anterior showing large RT. Para anal
abscess with mild supra levator extension (arrow). Note thickened RT levator ani muscle. (I and J) Axial and coronal MIP imaging
showing the exact location of internal opening (at 6 o’clock, arrow). Note dirty RT para rectal fat above the levator ani muscles (arrow
heads).
Value of contrast enhanced spoiled gradient (SPGR) MR 125
MR fistulography subtracted images means visualization offistulas as high-signal tubular structures containing varying de-grees of low-signal fluid. The surrounding fat appeared dark
because of the associated fat suppression technique. Becauseof the 3D data set, multiplanar reconstruction (MPR) andmaximum intensity projection (MIP), generate an imageimpression similar to fistulography (3,21,22), in our study,
we used MIP images to visualize the extensions due to theirhigh sensitivity but without subtraction to avoid anatomicaldisorientation.
Magnetic resonance imaging (MRI) has become an integralpart of the assessment of fistula as it can distinguish betweensepsis and granulation tissue from sphincter muscles (28). Aprospective study compared the preoperative MRI assessment
Fig. 5 (A–H) Patient with RT trans-sphenctric fistula with small horseshoe extension evident on MIP images not SPGR images (Park
type III). (A and B) Axial and coronal T2FSE showing RT. Trans-sphincteric fistula extending to RT ischio-anal fassa. (C and D) Post
contrast axial T1 SPGR showing internal opening at 6 o’clock (arrow) with caudal abscess formation. (E and F) Post contrast coronal T1
SPGR showing branching fistulous tract with no supra levator extension (arrow). (G and H) Axial and coronal MIP imaging showing
small horseshoe extension of the fistula tract to LT side (crossing mid line, arrow). MIP images clearly visualize fistulous tract and
extensions.
126 J.A. Mazroa et al.

Table 1 Classification and imaging findings in our patients.
Imaging findings Fistula type
Inter-sphincteric (50%) Trans-sphincteric (28.6%) Supra-sphincteric (21.4%)
Patients No. 14 8 6
Simple non branching fist. 12 8 2
Branching fist. – 2 4
Para anal abscess – 2 3
Horseshoe extension – 1 3
Table 2 The imaging findings by different sequences obtained.
Findings MR sequence
T2 FSE Post contrast T1 SPGR MIP MR imaging*
Simple non branching fistulous tracts (22) 20 22 22
Branching fist.tracts (6) 4 5 6
Internal opening detec. (28) 25 28 28
Para anal abscess (5) 5 5 5
Horseshoe extension (4) 2 3 4
Supralevator extension (6) 4 6 6
Diagnostic accuracy 84.9% 97.3% 100%
* Reformated from post contrast T1 SPGR.
Value of contrast enhanced spoiled gradient (SPGR) MR 127
of the anal fistula and intra-operative findings. High concor-dance rates were reported in terms of recognizing the course
of primary tracks [86%], demonstrating secondary tracks[91%], and horseshoe extension [97%], as well as identifyinginternal opening [80%] (29).
In their study, John A. Spencer et al. (30) stated that for thediagnosis of seven surgically confirmed cases of horseshoetracks, STIR imaging had a specificity of 100% and a sensitiv-
ity of 71%, compared with dynamic contrast-enhanced MRimaging which had a sensitivity and a specificity of 100%.
Beckingham et al. (31) in their study reported MR sensitiv-ity of 97%, specificity of 100% in detection of fistula in ano.
Buchanan et al. (32) showed that fistula surgery guided byMRI can reduce anal fistula recurrence by 75%. Moreover,recurrence in patients with discordant findings by MRI and
EUA, respectively, was always at the site identified by MRI,suggesting that surgery based on MRI would have preventedrecurrence.
Our study revealed MR diagnostic accuracy for post con-trast SPGR and MIP images (for detection of peri-anal fistulacompared to surgical findings) 97.3% and 100% respectively.
Limitations of our study are the lack of the 4th fistula type
presentation (extra sphincteric) as there were no patients withprimary pelvic diseases were found in our study. Larger pa-tients group probably would represent all the fistula types.
5. Conclusion
MRI is a reliable diagnostic modality in the evaluation of peri-
anal fistulas. Post contrast T1 SPGR sequence with its highresolution images and excellent anatomical orientation pro-vides almost all the necessary details for accurate evaluation.
Although MIP images lack depth orientation but its high sen-sitivity, rotational 2D and 3D capabilities exquisitely depict all
the fine ramifications and extensions. The combination of bothprovides complete evaluation and highest possible diagnostic
accuracy aiding successful surgical interventions, aiming to re-duce complications and recurrences.
References
(1) Khera Pushpinder S, Badawi Hesham A, Afifi Ahmed H. MRI in
perianal fistulae. Indian J Radiol Imaging 2010;20(1):53–7.
(2) John Morris, John A Spencer, Simon Ambrose N. Imaging
classification of perianal fistulas and its implications for patient
management. Radiographics 2000;20:623–35.
(3) Bhaya AK, Kumar N. MRI with MR fistulogram for perianal
fistula: a successful combination. Clin Gastrointest Magnetom
2007;1:56–9.
(4) Steve Halligan, Stoker Jaap. Imaging of fistula in ano. Radiology
2006;239:18–33.
(5) Beets-Tan RG, Beets GL, van der Hoop AG, Kessels AG, Vliegen
RF, Baeten CG, et al. Pre operative MR imaging of anal fistulas:
does it really help the surgeon. Radiology 2001;218:75–84.
(6) Park AG, Gordon PH, Hardcastle JD. A classification of fistula-
in-ano. Br J Surg. 1976;63:1–12.
(7) Champagne BJ, O‘Connor LM, Ferguson M, Orangio GR,
Schertzer ME, Armstrong DN. Efficacy of anal fistula plug in
closure of cryptoglandular fistulas: long-term follow-up. Dis
Colon Rectum 2006;49:1817–21.
(8) Swinscoe MT, Ventakasubramaniam AK, Jayne DG. Fibrin glue
for fistula-in-ano: the evidence reviewed. Tech Coloproctol
2005;9:89–94.
(9) Buchanan GN, Halligan S, Williams AB, et al. Magnetic
resonance imaging for primary fistula in ano. Br J Surg 2003;90:
877–81.
(10) Maier AG, Funovics MA, Kreuzer SH, Herbst F, Wunderlich M,
Teleky BK, et al. Evaluation of perianal sepsis: comparison of
anal sonography and MRI. J Magn Reson Imaging 2001;14:
254–60.

128 J.A. Mazroa et al.
(11) Chapple KS, Spencer JA, Windsor AC, Wilson D, Ward J,
Ambrose NS. Prognostic value of magnetic resonance imaging in
the management of fistula in ano. Dis Colon Rectum
2000;43:511–6.
(12) Schwartz DA, Wiersema MJ, Dudiak KM, et al. A comparison
of endoscopic ultrasound, magnetic resonance imaging, and exam
under anesthesia for evaluation of Crohn’s perianal fistulas.
Gastroenterology 2001;121:1064–72.
(13) Hussain SM, Outwater EK, Joekes EC, et al. Clinical and MR
imaging features of cryptoglandular and Crohn’s fistulas and
abscesses. Abdom Imaging 2000;25:67–74.
(14) Schmidt S, Chevallier P, Bessoud B, Meuwly J-Y, Felley C, Meuli
R, Schnyder P, Denys A. Diagnostic performance of MRI
for detection of intestinal fistulas in patients with compli-
cated inflammatory bowel conditions. Eur Radiol 2007;17:
2957–63.
(15) Nuran Sabir, Ugur Sungurtekin, Ergun Erdem, Mehmet Nessar.
Magnetic resonance imaging with rectal Gd-DTPA: new tool
for the diagnosis of perianal fistula. Int J Colorectal Dis
2000;15(5–6):317–22.
(16) Sygut A, Zajdel R, Kedzia-Budziewska R, Trzcinski R, Dziki A.
Late results of treatment of anal fistulas. Colorectal Dis
2007;9:151–8.
(17) Abdel Azeim M Ali, Ahmed M Seleim, Ibrahim E Dawoud,
Mohamed Y El Gindy, Ahmed A Abdel Razik. Improving
outcome of surgery for high perianal fistula. Egypt J Surg
2001;20(2).
(18) Chi-Ming Poon, Chung-Kei Ng Dennis, Ho-Yin Cheung
Michael, Shiu-Ki Li Raymond, Heng-Tat Leong. Recurrence
pattern of fistula-in-ano in a Chinese population. J Gastrointestin
Liver Dis 2008;17(1):53–7.
(19) Yıldırım Nalan, Gokalp Gokhan, Ozturk Ersin, Zorluoglu
Abdullah, Yılmazlar Tuncay, Ercan _Ilker, SavcıIdeal Gursel.
Combination of MRI sequences for perianal fistula classification
and the evaluation of additional findings for readers with varying
levels of experience. Turk Soc Radiol 2011.
(20) Malouf AJ, Buchanan GN, Carapeti EA, et al. A prospective
audit of fistula-in-ano at St. Mark‘s hospital. Colorectal Dis
2002;4:13–9.
(21) Schaefer Oliver, Lohrmann Christian, Langer Mathias. Digital
subtraction MR fistulography: new diagnostic tool for the
detection of fistula in Ano. AJR 2003;181(6):1611–3.
(22) Schaefer Oliver, Lohrmann Christian, Langer Mathias. Assess-
ment of anal fistulas with high-resolution subtraction MR-
fistulography: comparison with surgical findings. J Magn Reson
Imaging 2004;19(1):91–8.
(23) Al-Khawaria HA, Guptaa R, Sinana TS, Prakashb B, Al-Amerb
A, Al-Bolushic S. Role of magnetic resonance imaging in the
assessment of perianal fistulas. Med Princ Pract 2005;14:46–52.
(24) van Koperen PJ, Horsthuis K, Bemelman WA, Stoker J, Slors JF.
Perianal fistulas: developments in the classification and diagnostic
techniques, and a new treatment strategy. Ned Tijdschr Geneeskd
2008;152(51–52):2774–80, Dec 20.
(25) Patronas Nicholas, Bulakbasi Nail, Stratakis Constantine A,
Lafferty Antony, Oldfield Edward H, Doppman John, Nieman
Lynnette K. Spoiled gradient recalled acquisition in the steady
state technique is superior to conventional postcontrast spin echo
technique for magnetic resonance imaging detection of adreno-
corticotropin-secreting pituitary tumors. J Clin Endocrinol Metab
2003;88(4):1565–9.
(26) Ickard Atthew JFXR. Anal abscesses and fistulas. ANZ J Surg
2005;75:64–72.
(27) Shawki Sherief, Wexner Steven D. Idiopathic fistula-in-ano.
World J Gastroenterol 2011 July 28;17(28):3277–85.
(28) Halligan S. Imaging fistula-in-ano. Clin Radiol 1998;53:85–95.
(29) Lunniss PJ, Barker PG, Sultan AH, Armstrong P, Reznek RH,
Bartram CI, Cottam KS, Phillips RK. Magnetic resonance
imaging of fistula-in-ano. Dis Colon Rectum 1994;37:708–18.
(30) Spencer John A, Ward Janice, Beckinıham Ian J, Adams Clare,
Ambrose N Simon. Dynamic contrast-enhanced MR imaging of
perianal fistulas. AJR 1996;167:735–41.
(31) Beckingham IJ, Spencer JA, Ward J, Dyke GW, Adams C,
Ambrose NS. Prospective evaluation of dynamic contrast
enhanced magnetic resonance imaging in the evaluation of fistula
in ano. Br J Surg 1996;83:1396–8.
(32) Buchanan G, Halligan S, Williams A, et al. Effect of MRI on
clinical outcome of recurrent fistula-in-ano. Lancet
2002;360:1661–2.
Top Related