







Languages
Pages
Legal


USAID TB Technical Assistance Model
June 19, 2014

Overview
• TA in the Context of USG TB Strategy• Accomplishments and Approach of TB Strategy• USAID TA Model
2

USAID TB Funding Trends 1998–2013
Fu
nd
i ng
Level ( M
illion
s
US
$)
* FY funds including all accounts

4
By 2012, TB prevalence in 27 USAID-supported countries decreased by 40%.
5
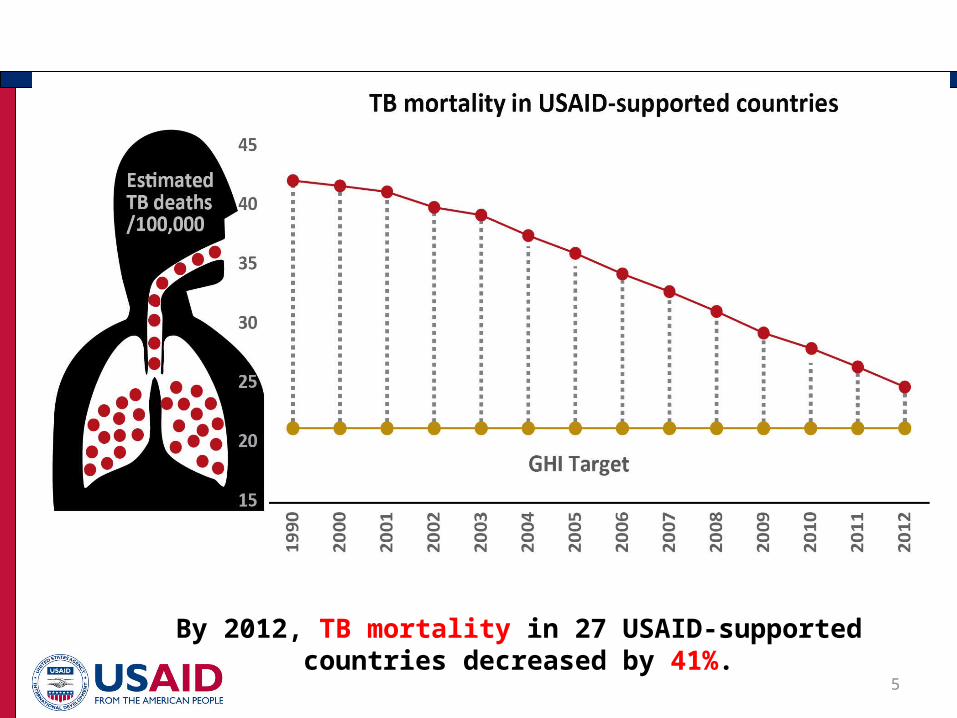
By 2012, TB mortality in 27 USAID-supported countries decreased by 41%.

Treatment Success Rate in Select Countries
6

Case Detection Rate in Select Countries (all forms of TB)
7

New patients with MDR TB initiated on treatment each year: (USAID focus countries)
8
Target
* These numbers differ from the past reports because they are adjusted to include only the current USAID countries to accurately reflect the trends.

9
USG TB Strategy: Key Approaches
Approach Examples
Promote country ownership
• Develop 5-year NTP Strategic Plans • Support development and implementation of GF
grants• Support NTP routine monitoring and supervisory
systems• Support participatory MOH led external
evaluations• Joint annual work planning with NTP and other
partners
Sustainable systems
• Strengthen drug/supply chain management • Strengthen facility level routine M&E system• Develop/improve lab network at all levels• Build primary health care capacity
Leverage resources • Develop GF proposals to cover unmet needs in NSPs
• Coordinate TB/HIV funds through PEPFAR • Expand health platforms (community, lab, drug
mgmt.)
Provide global technical leadership
• Develop and pilot new tools, policies, guidelines • Provide TA to countries/in targeted technical areas• Participate in WHO core working groups and
STAG-TB• Lead USG international TB efforts

Field level support:•Response to local needs/gaps based on NTP Strategic Plan, GF grant, and PEPFAR COP
•TA to MOHs, private sector, and NGOs; coordinate with other partners
•Expansion of new approaches/technologies (e.g., PMDT and Xpert)
•Global Drug Facility (GDF)
GH/regional bureaus support: •Global policy and guideline development
•Global operational and implementation research
•Technical support for evaluation, program design, monitoring, mentoring, and project management
Implementers: STB Partnership, WHO, CDC, TB CARE I and II, TO 2015, TREAT TB, SIAPS, USP, TB Alliance, GLC, TB TEAM
Field and Regional
84% ($188 in FY13)
GH 16% ($36m in FY13)
Country Level Focus – supporting the field
10• In FY13, Washington managed 51% of the total USAID TB funding and
36% of the field support resources.
USAID TB Technical Assistance Model
11
• USG convenes and leverages existing USAID bilateral program support to NTPs, preventing duplication, optimizing areas coverage and dovetailing
• Focus and concentrate in response to the GF changes, the new funding model, and evolution of the TB grants
Principles of Approach • Mirrors the inherently disease-specific NFM • Focus on development and implementation of
National TB Strategic Plans• On-going Country dialogue• Development of a disease-specific concept note
and funding envelope – assist with technical trade-offs
• Disease-specific TA to ensure quality programming

Convener: Model focuses on actively triangulating information among all partners
12
USAID TB Team Convener Role
•Regular country phone calls with key stakeholders•Ensure clear roles and responsibilities of stakeholders•Monitor and evaluate progressGF/FPM PR/NTP
In-country technical partners

USG Approach to Address GF grant TA support
• Shift in prioritized focus on a number of countries covering:
• 70% of the total GF grant funding for TB• 88% of TB prevalence • 88% of MDR-TB • 84% of TB/HIV co-infection
• Focus on quality programming and areas of technical expertise required
• Focus on more in-country approach: more consistent TA providers that less fly-in and fly-out TA
• More strategically wrap around USG bilateral program and USG TB working group partners

Priority Country Selection & Analysis
14
Criteria:•Burden (TB, MDR-TB, TB/HIV)•Global Fund Performance Data (rating, disbursement rate, expenditures)•Number and size of grants•For MDR-TB: minimum of 1,000 projected treatments for 2012-2014
Analysis of types of TA needed:•Burden and performance thus far (are things moving?)•Review types of TA currently available through USG mechanisms•Review of issues within countries based on past performance, stakeholders meetings/calls, discussions with partners and FPMs

PRINCIPLES TO RESULTS
15
RESULTS1.Full Implementation of National Strategic Plan2.Meets GF grant targets with quality3.Expends funds appropriately
USG TA
Model
In-country TA:•TB CARE I and II•PATH TB TOTargeted TA:•GDI (GLC)•CDCMulti-partner TA:•TBTEAM•SIAPS•GDF

USAID Country Mapping Example: Bangladesh
16
Technical experts visit countries to provide MDR-TB TA, and then project in country follows up. Experts provide additional virtual assistance to ensure things are moving forward
In-country advisor works with partners/USG project to ensure that grant is moving forward and expanding, and identifies any TA needs. Also ensures that countries understand all CPs
Ensures that country is doing proper quantification and that there is an adequate supply of drugs. Works with in-country advisor on any GF grant bottlenecks related to drug management
Assists with partner coordination meetings/calls and Phase 2 renewal preparation

THANK YOU!
Top Related