






Languages
Pages
Legal


Role of Think Kidneys
Preventing the avoidable harm caused by acute kidney
injury
Julie Slevin UK Renal Registry
11/27/2017Think Kidneys Autumn 2017 | 1

UK Renal Registry
Collects data on all things Kidney
Think Kidneys Improvement programmes:
Acute Kidney Injury
Improving the care of people at risk of, or with, acute kidney injury.
Transforming Participation in CKD
A unique NHS programme to help people with CKD live their best life.
Kidney Quality Improvement Partnership
Working together to develop, support and share improvement in kidney services to improve people's health and add value
11/27/2017Think Kidneys Autumn 2017 | 2

Acute Kidney Injury
Acute kidney injury is a sudden and recent reduction in a person’s
kidney function. It is often referred to as AKI.
Acute kidney injury is identified by blood tests when a raised level of
creatinine shows the stage of AKI.
Acute kidney injury can be caused by a number of things such as:
Stress on the kidneys due to illness or infection
Severe dehydration
Side effects of some drugs when you are unwell
11/27/2017Think Kidneys Autumn 2017 | 3

Is Acute Kidney Injury (AKI) really a problem?
In the UK up to 100,000 deaths
each year in hospital are associated with acute kidney injury.
Up to 30% could be prevented with
the right care and treatment
11/27/2017Think Kidneys Autumn 2017 | 4
One in five people admitted to hospital in the UK each year
as an emergency has acute kidney injury
Just one in two people know their kidneys make urine
About 65% of acute kidney injury starts in
the community
NCEPOD. Adding insultto injury, 2009
Wang, et al. 2012 Ipsos MORI survey,July 2014
Selby, et al. 2012

The UK National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report ‘Adding insult to injury’ http://www.ncepod.org.uk/2009aki.html found:
Only 50% of care for AKI was considered good
Unacceptable delays in identifying post admission AKI in 43% of the patients
Considerable knowledge gaps in identifying and managing someone with AKI
A fifth of all cases were predictable and avoidable
Predictable, avoidable AKI should not occur
Acute Kidney Injury (AKI)

Shared purpose: reduce harm related to AKI
Support commissioners and organisational leads in driving and championing the need to improve acute kidney injury care.
Provide clinicians and patients with the education, information and access to and about acute kidney injury to inform individual care
Establish the data flows to allow successful audit and quality improvement
| 611/27/2017Think Kidneys Autumn 2017
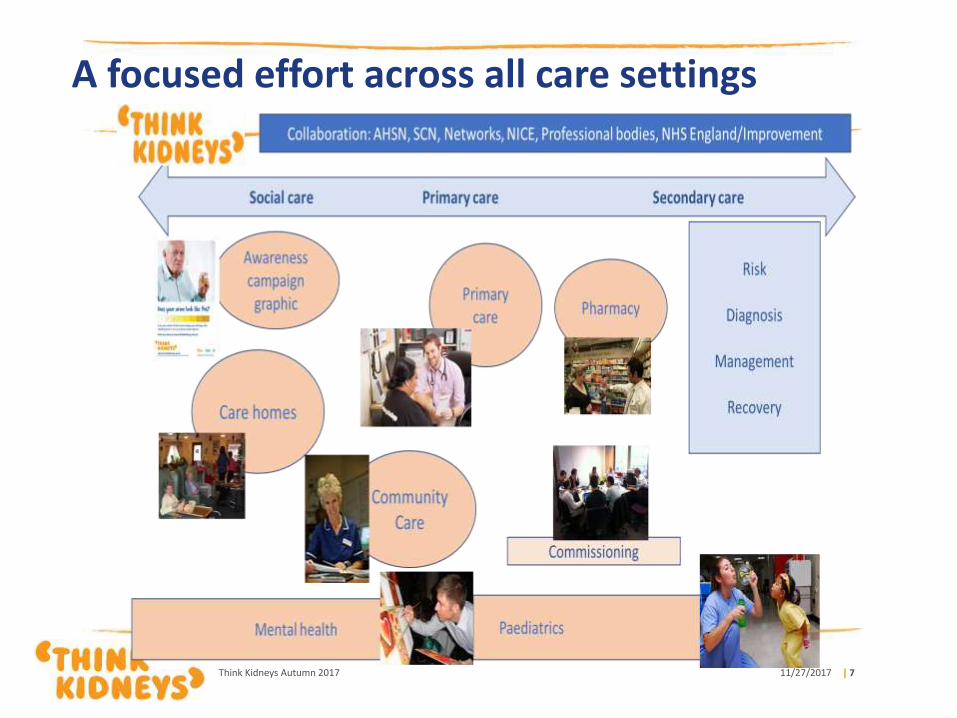
A focused effort across all care settings
| 711/27/2017Think Kidneys Autumn 2017

Using IT: improving diagnosis
| 811/27/2017Think Kidneys Autumn 2017

Using IT: Awareness, education, sharing, information
| 911/27/2017Think Kidneys Autumn 2017

Think Kidneys public campaign
11/27/2017Think Kidneys Autumn 2017 | 10
https://www.thinkkidneys.nhs.uk/campaign/

Identifying AKI
AKI is detected by a rise in Creatinine (Cr) and/or a decrease in urine outputIt’s severity (stage) is related to the change from the patients baseline CrIt can occur without symptoms

chronic kidney disease
heart failure
liver disease
diabetes
history of acute kidney injury
oliguria (urine output less than 0.5
ml/kg/hour)
Hypovolaemia
Sepsis
deteriorating early warning scores
(NICE Guideline 169, 2014)
Risk factors
Drugs can also affect kidney
function, these include:
NSAIDs,
angiotensin-converting enzyme
[ACE] inhibitors,
angiotensin II receptor
antagonists [ARBs] and
diuretics within the past week,
especially if hypovolaemic
use of iodinated contrast agents
symptoms or history of urological
obstruction, or conditions that may
lead to obstruction
Age 65 years or over
Are any of your patients at risk??

Pre- Renal
Most common cause of AKI and caused by reduced blood flow to the kidneys
Causes include:
• Hypotension• Dehydration• Heart Failure
Assess hydration and NEWS
With prompt correction this AKI rapidly resolves
Intrinsic
Involves damage to the kidney itself. Some causes include:
• Acute tubular necrosis• Glomerulonephritis• Drugs/toxins
Hardest to treat and likely to need Renal Team involvement
A urine dip will aid diagnosis
All AKI will eventually become intrinsic if it is not treated promptly
Post-RenalA consequence of urinary tract obstruction
• Blocked catheter• Enlarged prostate• Tumours
An obstruction can be above or below the bladder so consider bladder scan +/-USS KUB
May need a Urology review
Treatment of AKI depends on its cause
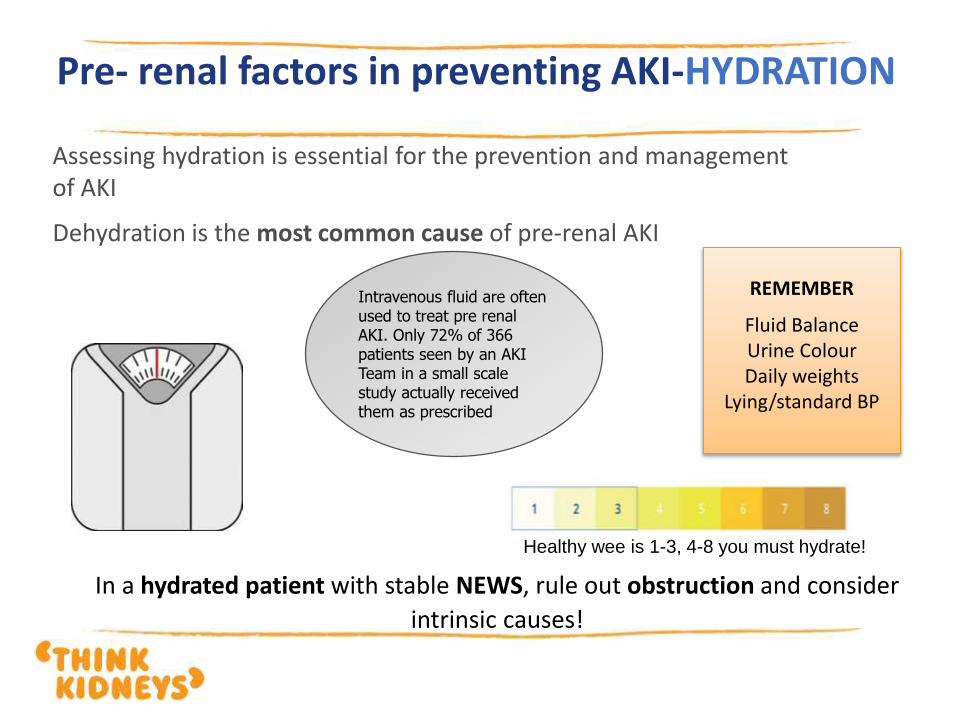
Pre- renal factors in preventing AKI-HYDRATION
Assessing hydration is essential for the prevention and management of AKI
Dehydration is the most common cause of pre-renal AKI
REMEMBER
Fluid BalanceUrine ColourDaily weights
Lying/standard BP
Intravenous fluid are often used to treat pre renal AKI. Only 72% of 366 patients seen by an AKI Team in a small scale study actually received them as prescribed
Healthy wee is 1-3, 4-8 you must hydrate!
In a hydrated patient with stable NEWS, rule out obstruction and consider
intrinsic causes!

Why is fluid balance so important?
Accurate fluid balance charting can also prevent life threatening complications of AKI
Optimum fluid balance
Assessment of fluid
Fluid overload
Oedema
Hypertension
Reduced oxygenation
Fluid loss
Hypotension
Shock
AKI
Too much fluidToo little fluid

DIP, MEASURE & DOCUMENTAll patients with AKI should have a urine dip. Blood and Protein in urine is a sign of kidney disease and intrinsic AKI
THINK: Have your patients passed urine in the last 6 hours?Cumulative totals should be done every 6 hours as
well as dailyIs your fluid balance chart accurate? In a small scale
study in one trust 85% of 570 patients seen by the AKI team did NOT have accurate in/out put monitoring!
Symptoms of AKI
In the early stages there may be no real symptoms or signs. A blood test
is needed to detect it.
However, someone with AKI can deteriorate quickly and suddenly
experience any of the following:
Changes to urine output, particularly a major reduction in the
amount of urine passed
Changes to urine colour/smell
Nausea, vomiting
Abdominal pains and feeling generally unwell, similar to a hangover
Dehydration or thirst
Confusion and drowsiness
11/27/2017Think Kidneys Autumn 2017 | 17
Treatment of AKI
Treatment of AKI is about identifying the cause to help you address the actions needed.
Certain drugs can affect the kidneys and these include:
Non-steroidal anti-inflammatory drugs (eg Ibuprofen)
Drugs that lower blood pressure (eg Ramipril)
Drugs used for people with diabetes (eg Metformin)
Drugs used by Mental Health patients (eg Lithium)
The doctor may decide that some of drugs need to be stopped for a day or two
The patient will need some more blood tests
The doctor might recommend to increase fluids or to admit the patient to hospital to have some fluid replacement
11/27/2017Think Kidneys Autumn 2017 | 18

Think Kidneys
The kidneys don’t usually complain
The kidneys can lose up to 90% of their function before you may even begin to notice
The kidneys are clever organs but need a good blood supply to work effectively
11/27/2017Think Kidneys Autumn 2017 | 19


Context for TP-CKD Programme
11/27/2017 21
The Wanless report (2002): Costs will be unsustainable unless radical reform takes place in the NHS with patients enabled to take more responsibility for their care
NHS England’s Five Year Forward View: (2014): “a more engaged relationship with patients and communities to promote well-being and prevent ill-health”
“to support people to manage their own health and care”
Collaboration between NHSE and UKRR

Terminology – Your Health Survey
| 22
PAMPatient Activation MeasureSkills, knowledge and confidence to manageyour long term condition
PROMsPatient Reported Outcome MeasureQuality of life
GenericDisease specific
PREMPatient Reported Experience MeasureQuestions relating to their healthcare experienceAll Renal Units X 1 per year
EQ-5D-5L
POS – S Renal
Self developed
Patient Activation
Measure (PAM)
Clinician-support for
PAM (CS-PAM)

Implementation
| 23
14 of the 52 adult renal units in England participated in the implementation of ‘Your Health Survey’ to measure patient activation, disease symptoms and quality of life outcomes.
Each unit used a different approach to implementation resulting in survey returns across the whole patient pathway.
The survey was handed out to patients as a paper copy by patient volunteers, nursing and medical staff who had previously attended an initiation event and was supported by information such as leaflets and posters.
Completed surveys were returned to the UK Renal Registry (UKRR) and scanned into a database. Results returned to patients via Patient View and units via nhs.net

Achievements
| 24
3,700 Your Health Surveys collected from patients across 14 renal unitsOver 450 CS-PAM Surveys collected from renal unit staff across 14 renal unitsAnnual Patient Experience survey has been rolled out nationally – 10,000 surveys collected in 2017 across England and Wales
How can we use this data to support the patient?Tailor conversations to individualsAcknowledge symptom burdenAddressing things that matter to themBuilding knowledge, skills and confidence – PAM level
Can interventions improve activation for teams and patients? Intervention Toolkit developed by patients and professionals in the Interventions work-stream

Kidney Quality Improvement
Partnership (KQuIP)
Graham Lipkin, Co Chair KQuIP
Louise Wells Co chair KQuIP
James McCann, KQuIP Programme Lead
Victoria Powell, KQuIP Regional Project
Manager
TBC, KQuIP Regional Project Manager
| 25

Kidney Quality Improvement Partnership (KQuIP)
26
KQuIP is a dynamic network of
kidney health professionals, patients
and carers who are committed to
developing, supporting and sharing
quality improvement in kidney
services in order to enhance
outcomes and quality of life for
patients with kidney disease.

KQuIP Structure
KQuIP Board
A representation of the KQuIP Partnering organisations and
stakeholder groups that meet twice a year.
KQuIP Chairs
Chairs of the workstreams that meet every six weeks
KQuIP Operational Group
GWL, LW, RC, KT and JM that meet on a monthly basis.
KQuIP Workstreams
Development, Projects and Measurement and Understanding
workstreams
04/07/2017 27

KQuIP project priorities
Improving access to kidney transplantation; Transplant First
Pre-emptive transplant listing and kidney transplantation rates vary widely. Transplant First, developed in the West Midlands under KQuIP. This has been packaged to provide resources and support to enable other interested regions to implement.
Improving access to home therapies for suitable patients
There is wide variation of access for patients to peritoneal and home haemodialysis. KQuIP is currently developing a national QI project to increase home therapies.
Improving vascular access; MAGIC - Managing Access by Generating Improvements in Cannulation
Aiming to reduce variation, improve incidence and prevalence rates, improve patient
experience, and reduce complications of cannulation of arteriovenous fistulae and
grafts.
04/07/2017 28

KQuIP regional days and delivery
West Midlands
Yorkshire and the Humber
East Midlands
North West
Potential future regions: South West, North East, Oxford and Thames Valley, Wales, Paediatrics and SPR club….
04/07/2017 29

KQuIP Website, Hub and E-Learning
KQUIP is working with the renal community to identify a suitable online E-learning platform that will:
Be owned by the renal community
Be free to use at the point of access
Support the sustainability of embedded quality improvement
The KQuIP Hub features:
QI stories from renal teams around the country
abstracts from presentations on QI projects
Signposting to educational resources to help enhance QI knowledge
Tools to help with QI projects as well as renal specific tools.
The hub aims to bring all of these resources and tools together in one place to help
the renal community deliver their quality improvement projects.04/07/2017 30

KQuIP welcomes you……enabling you and your team to improve quality and
safety
www.thinkkidneys.nhs.uk/kquip/

For further information and resources regarding
Acute Kidney Injury, Transforming Participation in CKD and KQuIP, please see the
Think Kidneys website
www.thinkkidneys.nhs.uk
Top Related