







Languages
Pages
Legal

The role of emotions in the omission vs commission dilemmas
Raffaella Di SchienaRaffaella Di SchienaGuglielmo BellelliGuglielmo Bellelli
University of Bari (Italy)University of Bari (Italy)
Tony MansteadTony MansteadUnivesity of Cardiff (UK)Univesity of Cardiff (UK)
Marcel ZeelenbergMarcel ZeelenbergUniversity of Tilburg (NL)University of Tilburg (NL)

Omission bias
The tendency to prefer inactive over active options, even when this leads to greater risks or worse outcomes
(Ritov & Baron, 1990)

Theoretical background
The vaccination dilemma (Ritov & Baron, 1990):
“Imagine you are parent of a child who is under three years old. In the country you live in there is an epidemic flu that can be fatal for children at this age (…) 10 out of 10,000 children can die because of the flu.
A vaccine for this kind of flu has been developed and tested (…). However, the vaccine is also risky. Because of its side effects, 5 out of 10,000 vaccinated children can die. Excluding these, neither the vaccine nor the flu have any long term effects”
“What would you choose in this situation?”
20%-40% choose the omission
“Which is the maximum level of risk from the action you would be willing to accept?”
Those who decide to act easily change their mind for slightly higher risk from the action, but still lower than risk from the omission

Why is OB important?
Theoretical reasons: It violates rationality axioms, according to which a rational choice
has to be based on expected consequences, like in E-U type models of choice (Von Neuman & Mortestern, 1947).
Omission choice is a non-consequential choice (Baron, 1994)
Practical reasons: Mainly public health concerns.
OB in real vaccination choices (Asch et al.,1994; Wroe et al., 2005)
OB in physicians’clinical practice (Aberegg, et al., 2005)
Additional evidence about OB in choice: closing the debate?
(3 studies) (R. Di Schiena, G. Bellelli, A.S.R. Manstead, M. Zeelenberg)
Emotion in OB: Where is it? (2 studies) (R. Di Schiena, G. Bellelli, M. Zeelenberg)
OB in health decision making: The role of emotion and trust in health care
(2 studies) (R. Di Schiena, G. Bellelli, A.S.R. Manstead)
Overview
Additional evidence about OB: Closing the debate?
R. Di Schiena, G. Bellelli, A.S.R. Manstead, M. Zeelenberg
Criticisms (Connolly & Reb, 2003).
• Fluctuating percentages of Ss choosing the omission do not necessarily imply that there is a bias towards the omission, as they can be due to other factors.
• Is it an experimental artefact, induced by the vaccination scenario?
Study 1
Study 2 & 3
Study 1 Hypothesis: If there is a bias towards the omission, then…
• Individuals might choose irrationally only when the irrational choice is an omission
• Individuals who choose to act might be less confident in the choice made than those who didn’t
• Those who choose the omission neglect consequences and rely more on the fact that one of the two options is an omission
• They might do that, controlling for attitude, previous experiences and/or other elements
Study 1 Three between Ss conditions: 1) Not to vaccinate (10/10000) VS Vaccinate (5/10000) (N = 48)
2) Not to vaccinate (6/10000) VS Vaccinate (5/10000) (N = 49)
3) Vaccination 1 (10/10000) VS Vaccination 2 (5/10000) (N = 48)
Main Measures: Choice behaviour Maximum level of risk accepted from the action (MLRA)
Additional measures: Risk information Frame of the two options Attitude towards vaccination Previous experiences Other elements

55,10%41,67%
6,25%
ACT 5 vs ACT 10 ACT 5 vs OM 10 ACT 5 vs OM 6
The number of Ss rationally choosing the less risky option was significantly higher in the Action vs Action condition (χ2 = 27.667; df = 2; p < .005)
A specific comparison between the two Action vs Omission conditions revealed a non significant difference(χ2 = 1.752; df = 1; p = .186)
Results on MLRA: Vaccinators where less confident in the choice made t (47) = 3.86, p < .005.
Riskier option
Less risky option
Study 1Results on behaviour

Study 1Questionnaire results split by behaviour
Vaccinators vs non Vaccinators
Importance of risk:
p < .005
Act5-Act10 Act5-Om10Act5-Om6
Importance of frame:
p < .001
Vaccinators Non Vaccinators
Non VaccinatorsVaccinators
…attitude, previous experiences and other elements didn’t significantly impact the choice
Study 1
The OB is real!
Individuals chose the riskier option only when this was an omission
Vaccinators were less confident in the choice made than Non- vaccinators
The omission choice was based on a higher consideration of aspects that have nothing to do with expected consequences
Omission choice can not be explained by attitude, previous experienes and so forth
Conclusions

Study 2 Hypothesis: Ob is a general effect if…
In other scenarios frequency of omission is significantly different from 0 and not significantly different from the vaccination scenario
Vaccination scenario (as control)
Managerial scenario: Imagine you are the owner of a big company, which is going through a very difficult crisis. (…) 60% risk of bankruptcy if you do not do anything (…) If you implement a recovery plan, it has a failure rate of 45%. Investment scenario: Imagine you have invested all your savings in stocks of company A, which is going through a very difficult crisis. (…) 60% risk of loosing all your savings. (…) If you switch, the risk of loosing is 45%.
Study 2
0
10
20
30
40
50
60
70
80
1 2 3
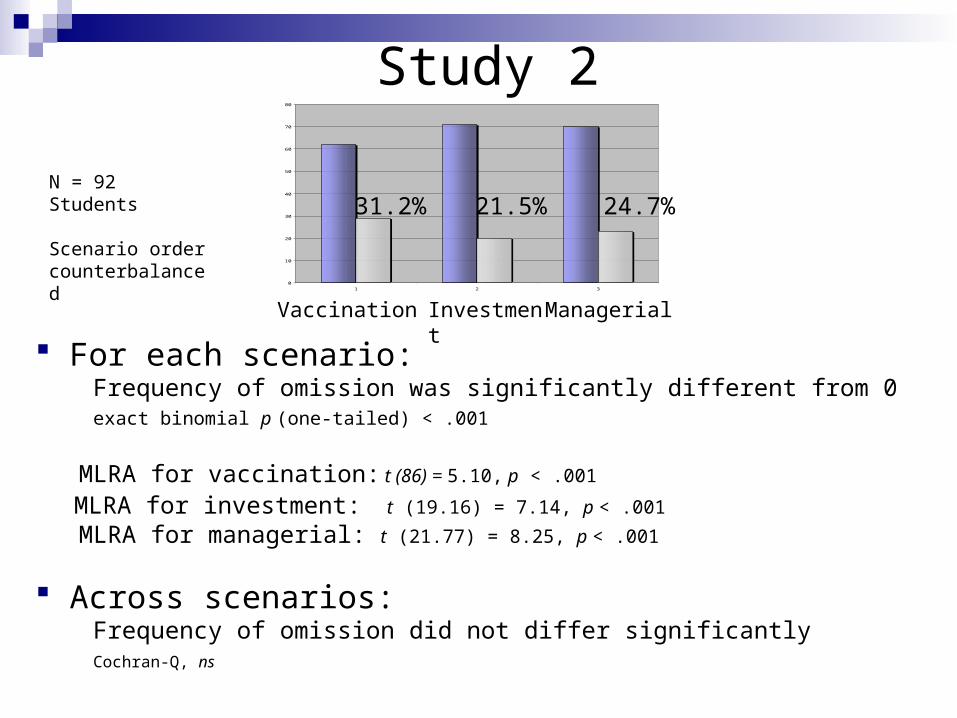
Vaccination Investment Managerial
31.2% 24.7% 21.5%
For each scenario: Frequency of omission was significantly different from 0 exact binomial p (one-tailed) < .001
MLRA for vaccination: t (86) = 5.10, p < .001 MLRA for investment: t (19.16) = 7.14, p < .001 MLRA for managerial: t (21.77) = 8.25, p < .001
Across scenarios: Frequency of omission did not differ significantly Cochran-Q, ns
N = 92 Students
Scenario ordercounterbalanced

Study 2Conclusions
Ob is a general effect across different domains
Concern: the choice situation is not relevant for a students’
sample?
Study 3
Study 3Replication of Study 2 with relevant samples
Hypothesys: The same as in Study 2
Materials and procedure: The same as in Study 2 (investment and managerial choices were used as a
unique choice)
Participants: 75 Financial advisors confronted with economic
scenarios 64 Parents of children in vaccination age confronted with
vaccination scenario

Study 3
0
10
20
30
40
50
60
70
1 2
For each scenario: Frequency of omission was significantly different from 0 (25%) exact binomial p (one-tailed) < .001
MLRA for economic: t (12.93) = - 5.48, p < .001 MLRA for vaccination scenario: t (55.02) = - 4.35, p < .001
Across scenarios: Frequency of omission was significantly higher in the vaccination choice χ² (1, N = 139) = 5.32, p < .05.
Vaccination Economic
20%34.4%
Additional evidence about OB in choice: Closing the debate?
The empirical test yield positive results: There is an irrational tendency to favour the omission that is not due to other factors over a bias towards it
This effect is general across domains, but to a different extent
Future work: Understand why there are different omission tendencies for different scenarios
May be the emotional vivdness of the situation?

The role of emotion in the OB: Where is it?
R. Di Schiena, G. Bellelli, M. Zeelenberg
Theoretical background Emotion and Decision Making Emotionality of the process:• Choices can be based on gut feelings, instead of a thorough analysis (Epstein & Pacini, 1999)
Anticipated emotions:• Decisions can be aimed at avoiding future regret, instead of simply maximizing
possible gains (Zeelenberg, 1999)
Experienced emotions:• Negative emotions elicited by a difficult choice situation can make individuals adopt an avoidant behavior (Luce, 1998)• Risk itself can evoke anxiety and fear that make people adopt a non consequential
choice (Loewenstein, Weber, & Hsee, 2001).
Study 1OB in a dual process perspective
Theoretical background:
• According to dual-process theories, decision makers process the available information relying on the analytical system or on the affective-experiential system (Epstein & Paccini, 1999; Slovic et al., 2004)
• Evidence shows that, when they activate an affective-experiential
process, irrational choices are more likely (Finucane et al., 2000)
Hypothesys:
• When relying on the affective-experiential system, Ss will show a higher OB

SCENARIO Think aloud
CHOICE+
MLRA
SCENARIOCHOICE
+MLRA
Materials and procedure
Time pressure (N = 60)
Control (N = 58)
Scenario: Immagine you have a serious brain infection that can bring about permanent brain damage (…). Omission: Not to have the intervention (20% risk of brain damage) Action: To have an intervention that would stop the brain infection (15% risk of brain damage) Conditions:
Think aloud
Rational Experiential Inventory (Epstein & Pacini, 1999) as control measure
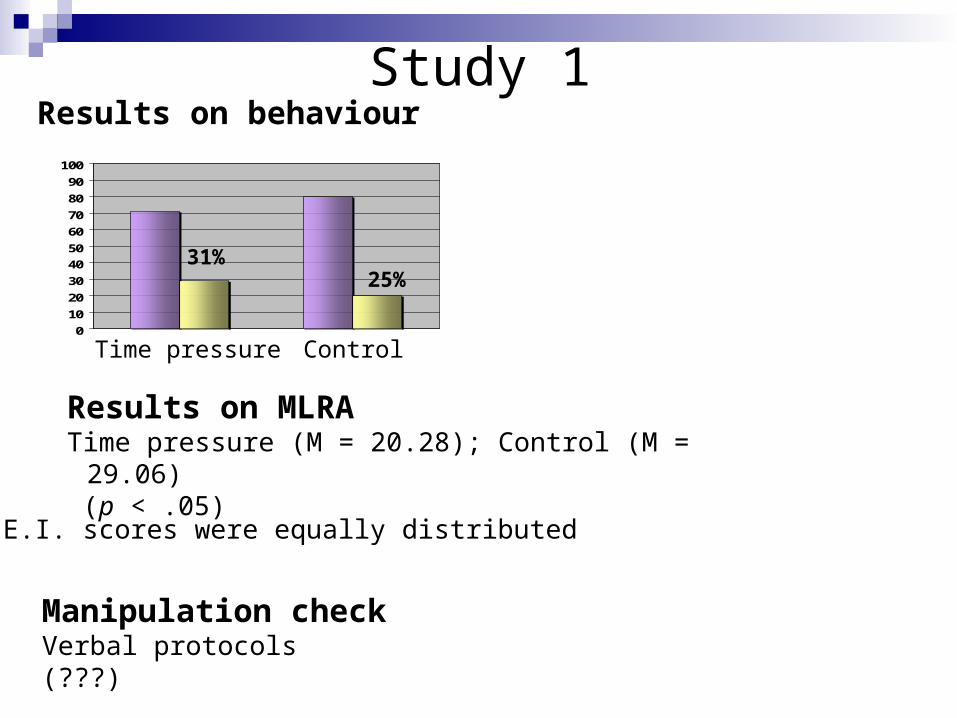
Study 1
0
10
20
30
40
50
60
70
80
90
100
Results on MLRA Time pressure (M = 20.28); Control (M = 29.06) (p < .05)
31%25%
Time pressure Control
Results on behaviour
Manipulation checkVerbal protocols(???)
R.E.I. scores were equally distributed
Study 2Anticipated regret and OB
Theoretical background:
• Some scholars suggest that individuals prefer the omission because they expect to feel less regret in case of negative outcome (Anderson, 2003)
• Evidence shows that, being consequences equal, individuals regret more the action than the omission (Landman, 1987; Kahneman & Tversky, 1982)
Study 2Anticipated regret and OB
Hypothesys: If anticipated regret caused OB, then…
• In the choice phase: When possible regret is more salient, Ss are more likely to choose
the omission
• In the Post-choice Pre-resolution: Ss are expected to feel more anxious if they have choosen the
action
• In the Post-choice Post-resolution: If the outcome is negative, Ss are expected to regret more when
they have chosen the action than when they have chosen the omission (Landman, 1987; Kahneman & Tversky, 1982)
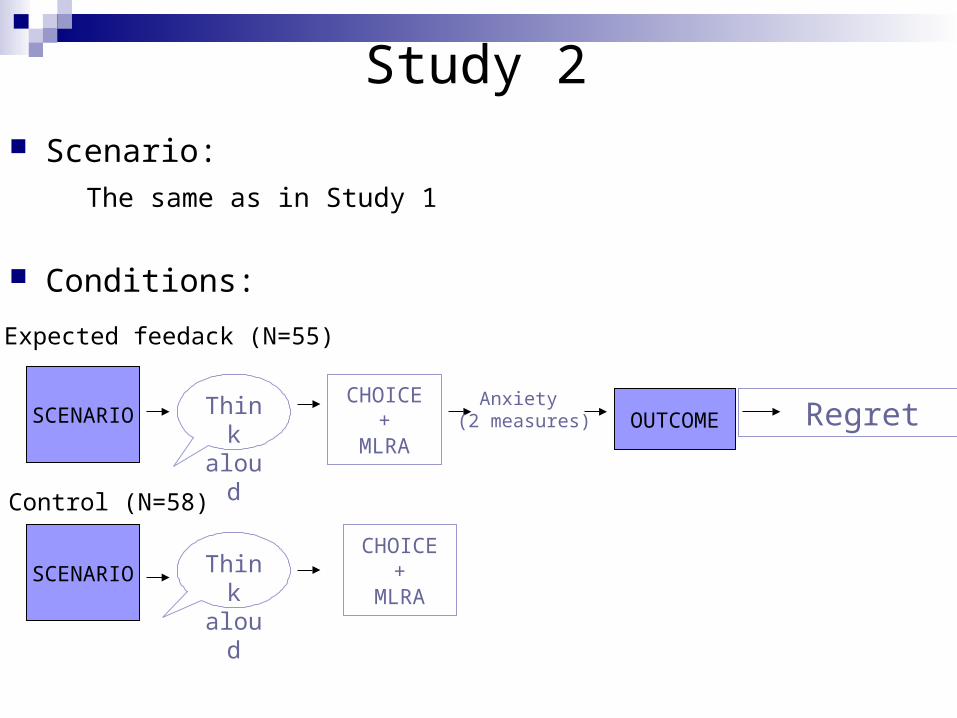
SCENARIO Think aloud
CHOICE+
MLRAOUTCOME
SCENARIO Think aloud
Anxiety (2 measures) Regret
CHOICE+
MLRA
Study 2 Scenario:
The same as in Study 1
Conditions: Expected feedack (N=55)
Control (N=58)

Results on behaviour
0
10
20
30
40
50
60
70
80
90
100
Feedback (M = 21.68); No feedback (M = 29.87) (p = .063)
Results on MLRA
29% 20%
Feedback Control
Study 2
Study 1Results on emotion measures
Post-choice pre-resolution: Ss who decided to act where more anxious than those who omitted
on both the anxiety measures (p <.05 and p =.052)
Post-choice post-resolution: Those who acted felt more regret than those who did not act
(p<.005);
Manipulation check: Verbal protocols (???)
Relying on the affective-experiential system induces a higher OB, but this effect is weak
Regret anticipation induces a higher OB, but the effect is weak as well
Weak manipulations?
Small samples?
The role of emotion in the OB: Where is it?
OB in health decision making: The role of emotion and trust in health care
R. Di Schiena, G. Bellelli, A.S.R. Manstead
Strange results of previous studies: In the brain infection situation, many Ss did not only prefer
the action, but even wanted to have the intervention when
it was riskier than doing nothing
(action bias, Patt & Zakhauser, 1997)
Decision making as emotion focused coping (Luce, 1998):
• When facing a risky decision, Ss are motivated to cope with negative emotions the risk evokes, and this can push them into acting paradoxically…
• Sometimes this could bring about OB…
• But…
• coping goals are mediated by subjects’ beliefs
• Ss’ beliefs that physician or health-care system is trustworthy can interact with the effect of emotion
(Benin et al., 2006).
Theoretical background
Hypothesis: When the choice situation is highly emotional: - Ss with high trust will tend to favour the action, even when it’s
riskier (ACTION BIAS) - Ss with low in trust will tend to favour the omission, even when it’s
riskier (OMISSION BIAS)
Trust manipulation by priming: Ss are provided with a page illustrating the health care
achievements (the dramatic occurrence of medical errors), and a story, in a box, as vivid example
Emotionality manipulation by different instructions:
High Em.: Try to imagine vividly how you would feel in this situation and how this could affect your life
Low Em.: Try to be objective and detached, in order to give your acquaintance the best advice
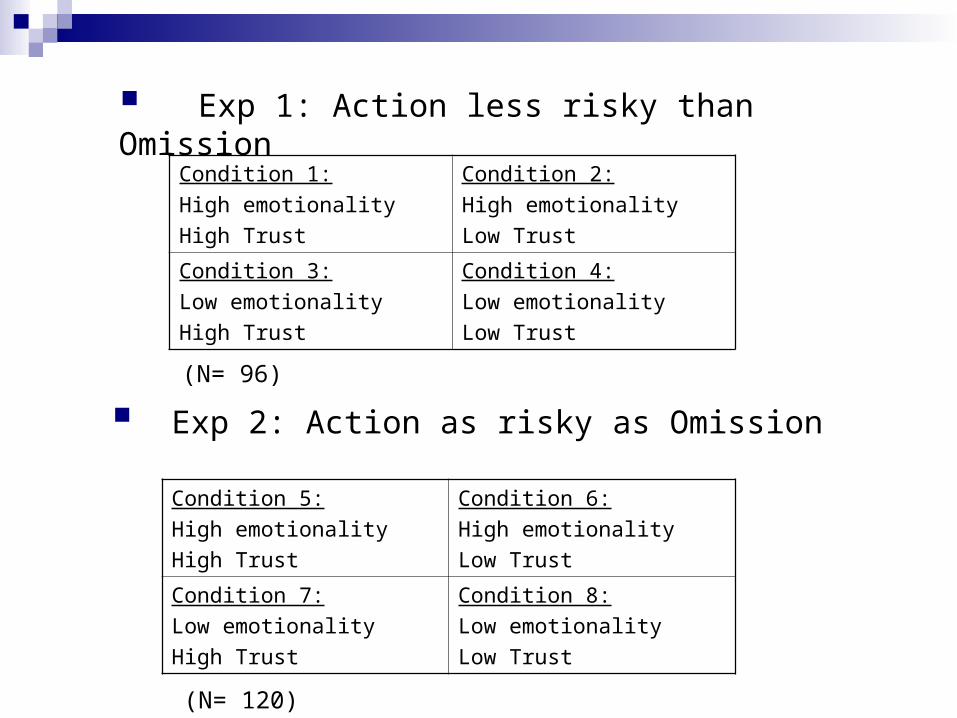
Condition 1:
High emotionality
High Trust
Condition 2:
High emotionality
Low Trust
Condition 3:
Low emotionality
High Trust
Condition 4:
Low emotionality
Low Trust
Exp 1: Action less risky than Omission
Exp 2: Action as risky as Omission
Condition 5:
High emotionality
High Trust
Condition 6:
High emotionality
Low Trust
Condition 7:
Low emotionality
High Trust
Condition 8:
Low emotionality
Low Trust
(N= 96)
(N= 120)
3 scenarios in counterbalanced order Brain surgery:(cfr. previous studies)
Vaccination scenario:(cfr. previous studies)
Slow growing cancer:Omission:
risk of dying from the cancer: 20%
Action:
To have chemotherapy that would cure your slow growing
cancer permanently, but implies a risk of dying from a myelodysplastic
syndrome: 15% (20%)
Materials

Dependent measures: Frequency of omission MLRA from the action (and from the OMISSION in exp. 2) Option evaluation
Emotionality manipulation check: PANAS scale
(Watson, Clark, & Tellegen, 1988)
Trust manipulation check: four items right after the manipulation
Covariate: A revised version of the Trust in Physician Scale (TPS) (Anderson & Dedrick, 1990)
Measures (Exp. 1 & 2)
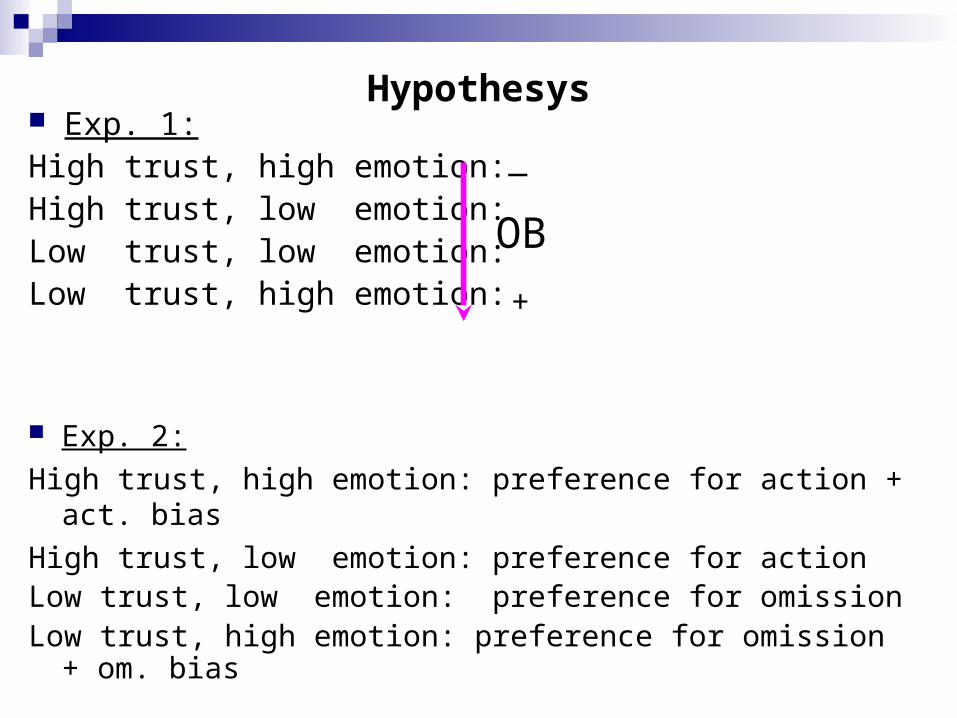
Exp. 1:High trust, high emotion:High trust, low emotion: Low trust, low emotion: Low trust, high emotion:
OB
Exp. 2:
High trust, high emotion: preference for action + act. bias
High trust, low emotion: preference for actionLow trust, low emotion: preference for omissionLow trust, high emotion: preference for omission + om. bias
_
+
Hypothesys
Provisional results…(exp. 1 and 2)
• Both manipulations were effective:
Emotionality (.018 < p < .080)
Trust manipulation (p < .01)

Provisional results…(exp.1 and 2)
• Log linear analysis on frequencies doesn’t show any significant interaction
• ANOVA on continuous DVs doesn’t show any significant interaction
However…
• There is a main effect of trust in the expected direction, that is never significant but stable across scenarios and dependent measures
• In Exp. 2, brain surgery scenario, there was also an interaction
effect between emotionality and trust, that was not significant but stable across all of the dependent measures
General conclusions There is an OB and is general across domains, so we still need to
be concerned about it
Evidence about the role of emotions is non significant but in the expected direction and reliable..a fruitful direction?
What is needed? Larger samples and stronger manipulations!!
The pure “emo-cognitive” perspective is not enough, since domain specific factors are surely involved (i.e. Trust in health care; manager are expected to act)
Future work should deepen the interaction btween these factors and the emotions

Many thanks for your attention
Top Related