







Languages
Pages
Legal

Testicular Cancer
Dr. AADITYA PRAKASH
DNB Resident, Radiation Oncology
BMCHRC, Jaipur
INTRODUCTION
Testicular cancers constitute 1% of all cancers.
GCTs are the most common solid tumors in men between the ages of 15 and 35 years.
In a man age 50 or older, a solid testicular mass is usually a lymphoma.
Approximately 90 % of GCTs originate in the testis, and 10 % are extragonadal.
Most curable solid neoplasm.
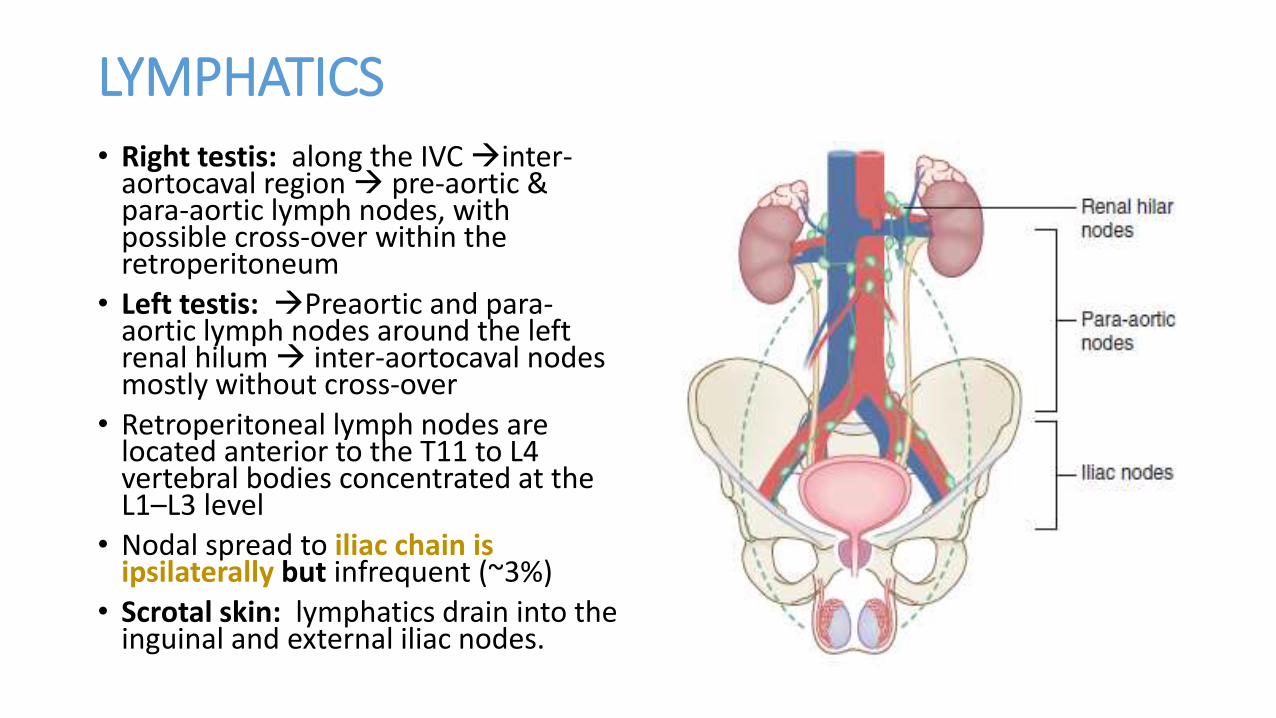
LYMPHATICS• Right testis: along the IVC inter-
aortocaval region pre-aortic & para-aortic lymph nodes, with possible cross-over within the retroperitoneum
• Left testis: Preaortic and para-aortic lymph nodes around the left renal hilum inter-aortocaval nodes mostly without cross-over
• Retroperitoneal lymph nodes are located anterior to the T11 to L4 vertebral bodies concentrated at the L1–L3 level
• Nodal spread to iliac chain is ipsilaterally but infrequent (~3%)
• Scrotal skin: lymphatics drain into the inguinal and external iliac nodes.
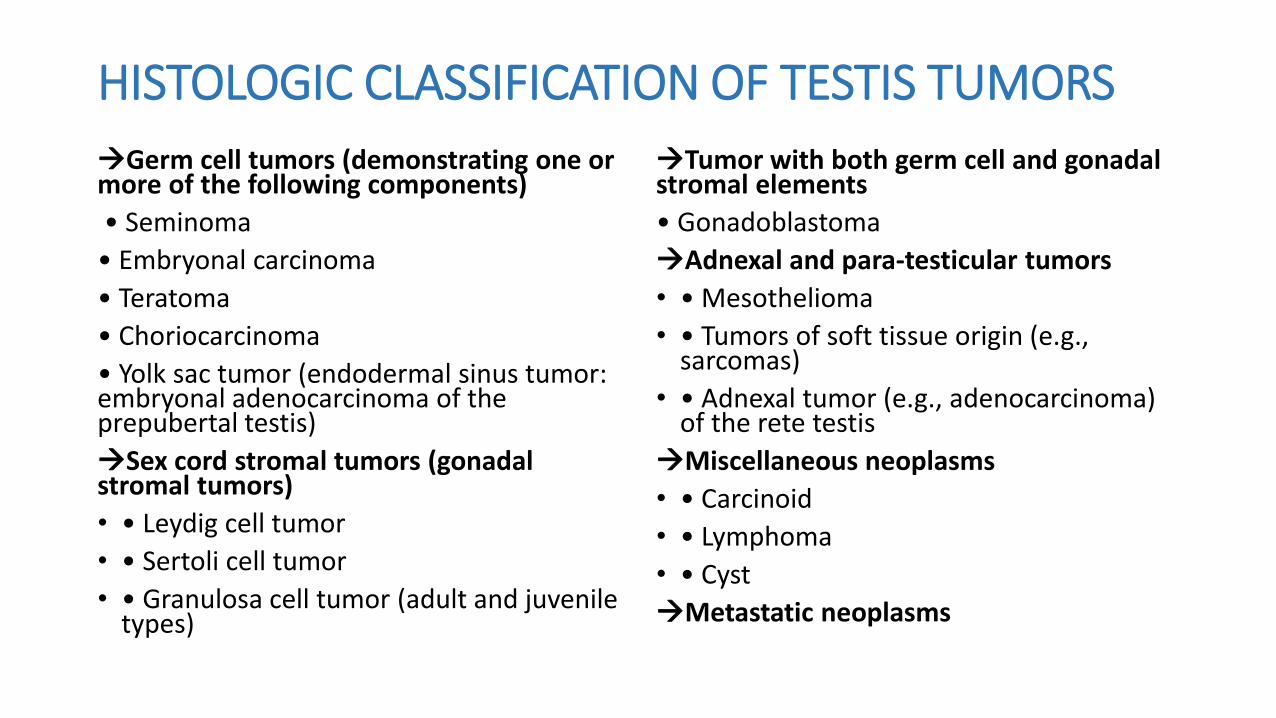
HISTOLOGIC CLASSIFICATION OF TESTIS TUMORS
Germ cell tumors (demonstrating one or more of the following components)
• Seminoma
• Embryonal carcinoma
• Teratoma
• Choriocarcinoma
• Yolk sac tumor (endodermal sinus tumor: embryonal adenocarcinoma of the prepubertal testis)
Sex cord stromal tumors (gonadal stromal tumors)
• • Leydig cell tumor
• • Sertoli cell tumor
• • Granulosa cell tumor (adult and juvenile types)
Tumor with both germ cell and gonadal stromal elements
• Gonadoblastoma
Adnexal and para-testicular tumors
• • Mesothelioma
• • Tumors of soft tissue origin (e.g., sarcomas)
• • Adnexal tumor (e.g., adenocarcinoma) of the rete testis
Miscellaneous neoplasms
• • Carcinoid
• • Lymphoma
• • Cyst
Metastatic neoplasms
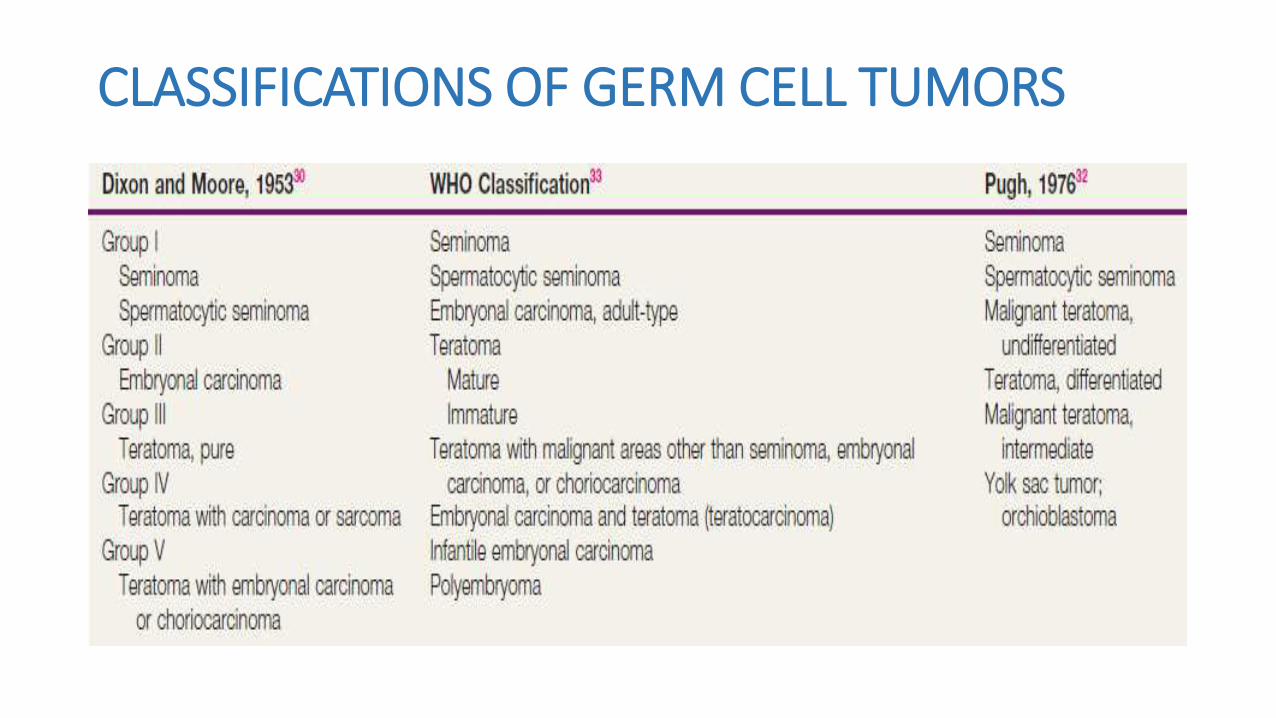
CLASSIFICATIONS OF GERM CELL TUMORS
STAGING OF TESTIS TUMORS BY THE AMERICAN JOINT COMMITTEE ON CANCER (AJCC)
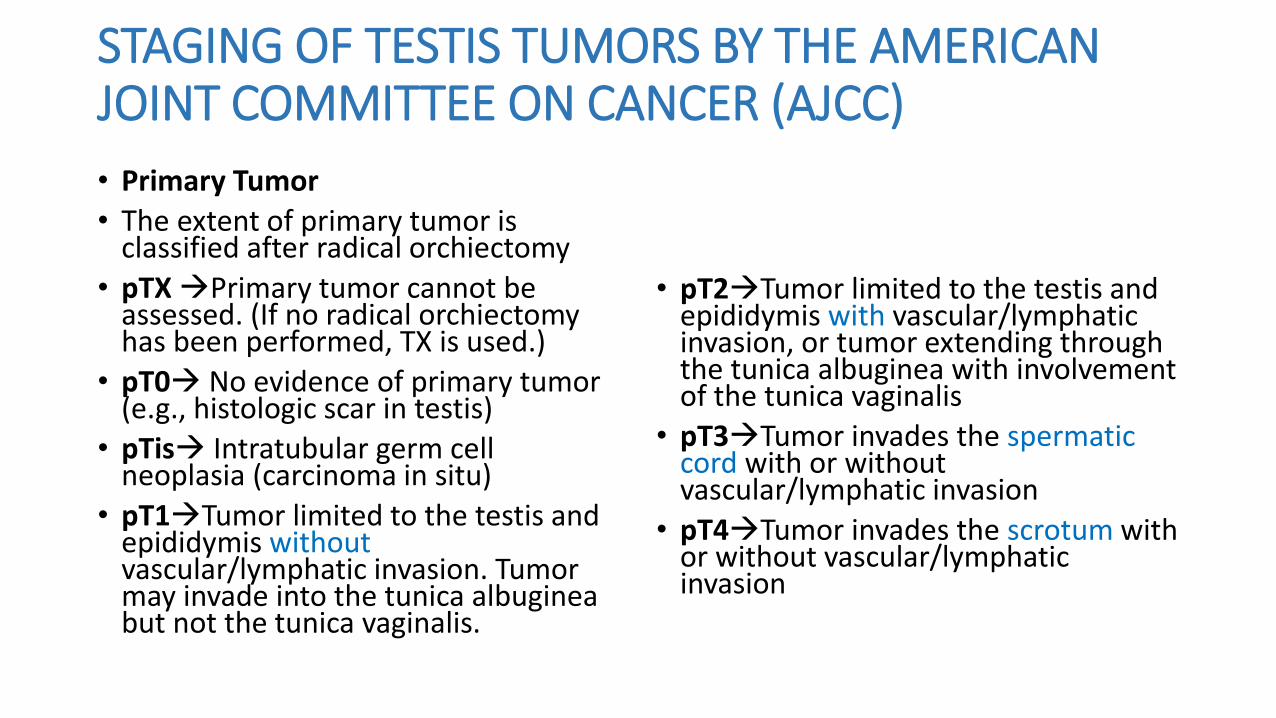
• Primary Tumor
• The extent of primary tumor is classified after radical orchiectomy
• pTXPrimary tumor cannot be assessed. (If no radical orchiectomy has been performed, TX is used.)
• pT0 No evidence of primary tumor(e.g., histologic scar in testis)
• pTis Intratubular germ cell neoplasia (carcinoma in situ)
• pT1Tumor limited to the testis and epididymis withoutvascular/lymphatic invasion. Tumor may invade into the tunica albugineabut not the tunica vaginalis.
• pT2Tumor limited to the testis and epididymis with vascular/lymphatic invasion, or tumor extending through the tunica albuginea with involvement of the tunica vaginalis
• pT3Tumor invades the spermatic cord with or without vascular/lymphatic invasion
• pT4Tumor invades the scrotum with or without vascular/lymphatic invasion
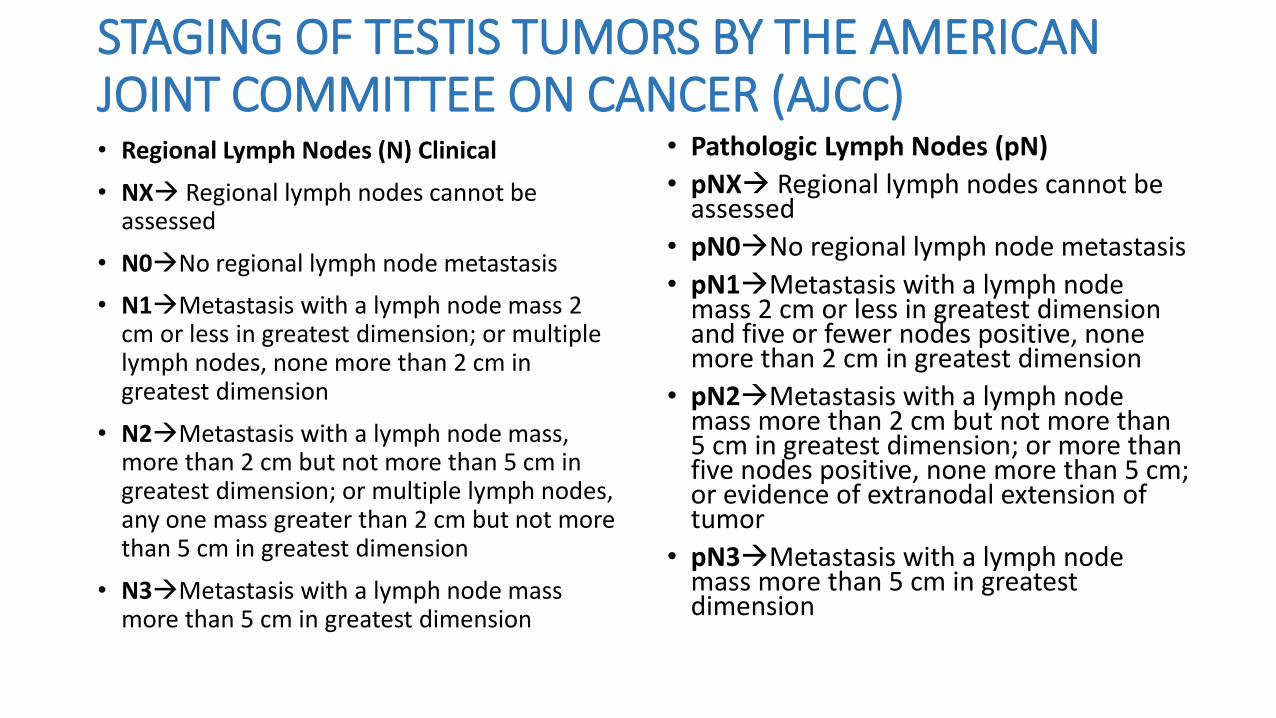
STAGING OF TESTIS TUMORS BY THE AMERICAN JOINT COMMITTEE ON CANCER (AJCC)• Regional Lymph Nodes (N) Clinical
• NX Regional lymph nodes cannot be assessed
• N0No regional lymph node metastasis
• N1Metastasis with a lymph node mass 2 cm or less in greatest dimension; or multiple lymph nodes, none more than 2 cm in greatest dimension
• N2Metastasis with a lymph node mass, more than 2 cm but not more than 5 cm in greatest dimension; or multiple lymph nodes, any one mass greater than 2 cm but not more than 5 cm in greatest dimension
• N3Metastasis with a lymph node mass more than 5 cm in greatest dimension
• Pathologic Lymph Nodes (pN)
• pNX Regional lymph nodes cannot be assessed
• pN0No regional lymph node metastasis
• pN1Metastasis with a lymph node mass 2 cm or less in greatest dimension and five or fewer nodes positive, none more than 2 cm in greatest dimension
• pN2Metastasis with a lymph node mass more than 2 cm but not more than 5 cm in greatest dimension; or more than five nodes positive, none more than 5 cm; or evidence of extranodal extension of tumor
• pN3Metastasis with a lymph node mass more than 5 cm in greatest dimension
STAGING OF TESTIS TUMORS BY THE AMERICAN JOINT COMMITTEE ON CANCER (AJCC)
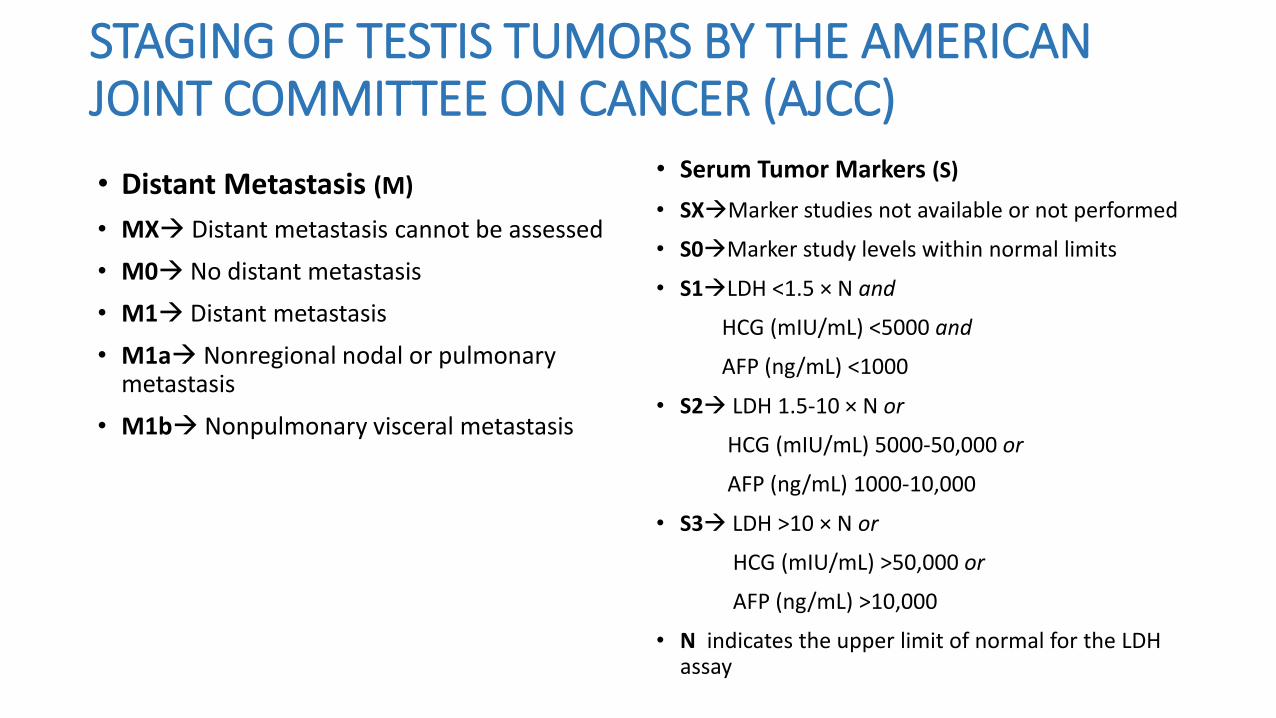
• Distant Metastasis (M)
• MX Distant metastasis cannot be assessed
• M0 No distant metastasis
• M1 Distant metastasis
• M1a Nonregional nodal or pulmonary metastasis
• M1b Nonpulmonary visceral metastasis
• Serum Tumor Markers (S)
• SXMarker studies not available or not performed
• S0Marker study levels within normal limits
• S1LDH <1.5 × N and
HCG (mIU/mL) <5000 and
AFP (ng/mL) <1000
• S2 LDH 1.5-10 × N or
HCG (mIU/mL) 5000-50,000 or
AFP (ng/mL) 1000-10,000
• S3 LDH >10 × N or
HCG (mIU/mL) >50,000 or
AFP (ng/mL) >10,000
• N indicates the upper limit of normal for the LDH assay
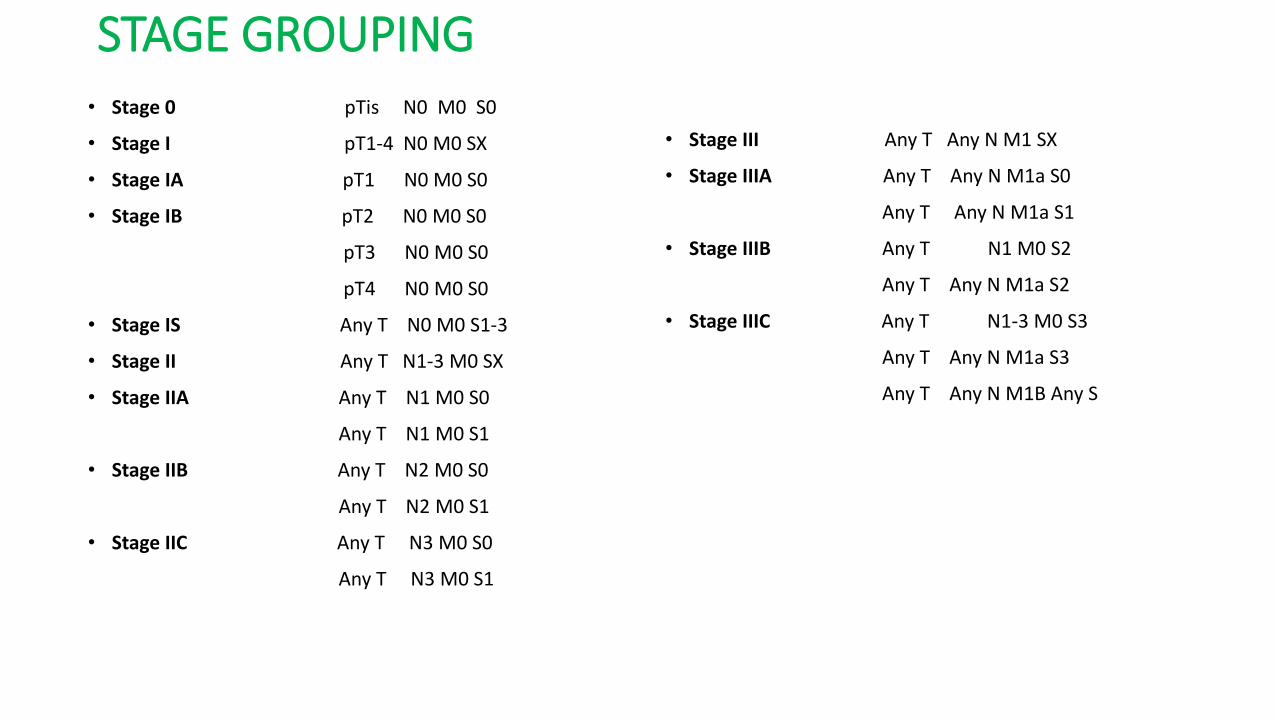
STAGE GROUPING• Stage 0 pTis N0 M0 S0
• Stage I pT1-4 N0 M0 SX
• Stage IA pT1 N0 M0 S0
• Stage IB pT2 N0 M0 S0
pT3 N0 M0 S0
pT4 N0 M0 S0
• Stage IS Any T N0 M0 S1-3
• Stage II Any T N1-3 M0 SX
• Stage IIA Any T N1 M0 S0
Any T N1 M0 S1
• Stage IIB Any T N2 M0 S0
Any T N2 M0 S1
• Stage IIC Any T N3 M0 S0
Any T N3 M0 S1
• Stage III Any T Any N M1 SX
• Stage IIIA Any T Any N M1a S0
Any T Any N M1a S1
• Stage IIIB Any T N1 M0 S2
Any T Any N M1a S2
• Stage IIIC Any T N1-3 M0 S3
Any T Any N M1a S3
Any T Any N M1B Any S
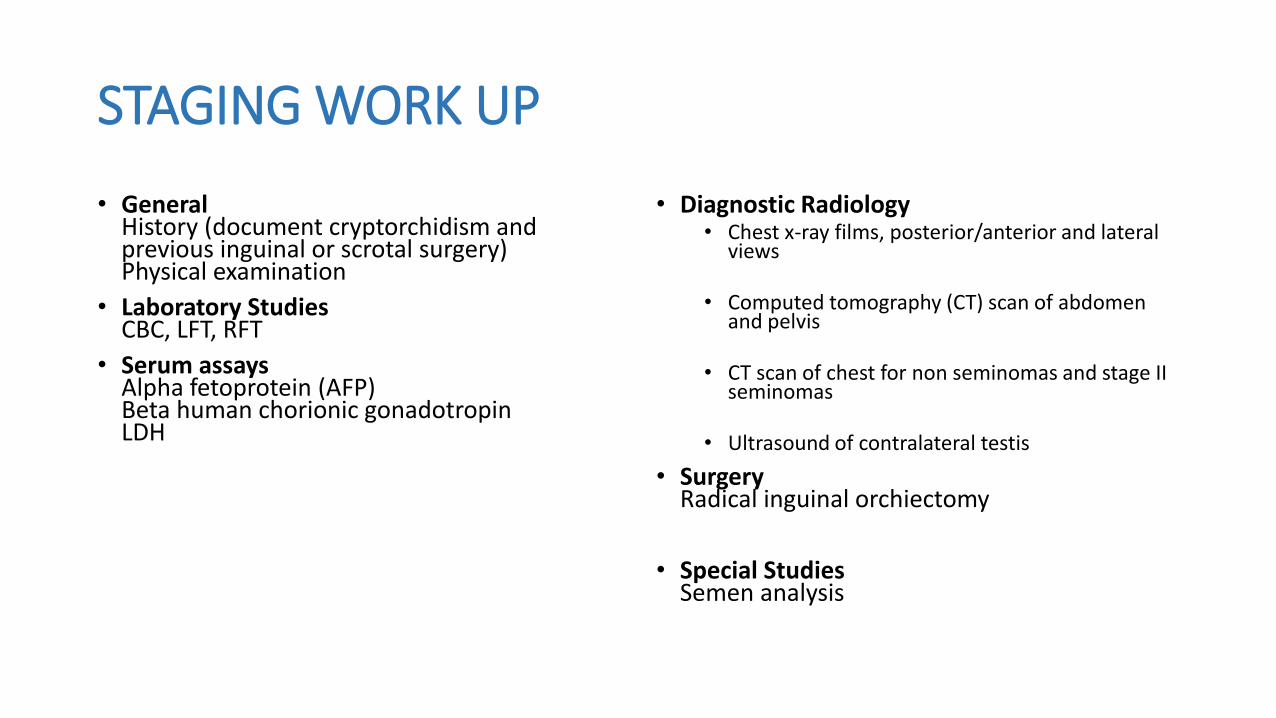
STAGING WORK UP
• GeneralHistory (document cryptorchidism and previous inguinal or scrotal surgery)Physical examination
• Laboratory StudiesCBC, LFT, RFT
• Serum assaysAlpha fetoprotein (AFP)Beta human chorionic gonadotropinLDH
• Diagnostic Radiology• Chest x-ray films, posterior/anterior and lateral
views
• Computed tomography (CT) scan of abdomen and pelvis
• CT scan of chest for non seminomas and stage II seminomas
• Ultrasound of contralateral testis
• SurgeryRadical inguinal orchiectomy
• Special StudiesSemen analysis
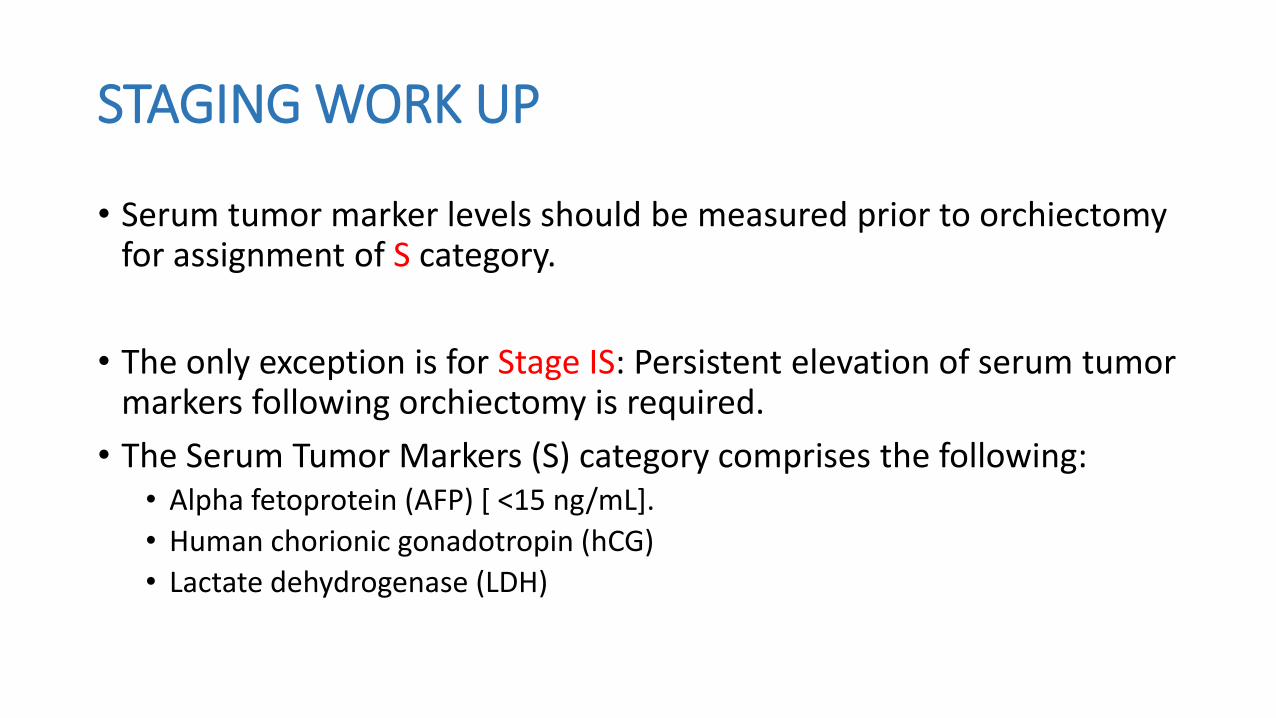
STAGING WORK UP
• Serum tumor marker levels should be measured prior to orchiectomy for assignment of S category.
• The only exception is for Stage IS: Persistent elevation of serum tumormarkers following orchiectomy is required.
• The Serum Tumor Markers (S) category comprises the following:• Alpha fetoprotein (AFP) [ <15 ng/mL].
• Human chorionic gonadotropin (hCG)
• Lactate dehydrogenase (LDH)
• Serum tumor markers can document persistent or recurrent cancer after surgery or chemotherapy and may predict the responsiveness of nonseminomas to treatment.
• The level of beta-HCG should decrease by 90% or more every 21 days with each successful treatment cycle of chemotherapy.
• The decline of AFP is less predictable.
WORKUP (NCCN)
• H&P
• LDH
• Beta HCG
• AFP
• Biochemical Profile
• Chest X-ray
• Testicular Ultrasound
• Discuss sperm banking
• Followed by Radical Inguinal Orchidectomy
• Consider contralateral testis biospsy if• Suspicious ultrasound• Cryptorchid• Marked atrophy
NCCN GUIDELINES FOR MANAGEMENT• PURE SEMINOMA (pure seminoma histology and AFP negative;may
have elevated beta-hCG):-
• POST DIAGNOSTIC WORK UP
I. ABD/PELVIC CT
II. CHEST CT IF:- ABD CT +VE , or, ABNORMAL CHEST X-RAY
III. REPEAT beta-hCG, LDH, AFP since TNM staging based on post-orchiectomy values
IV. BRAIN MRI,if clinically indicated
V. Bone scan ,if clinically indicated
VI. Discuss about sperm banking.
PURE SEMINOMA• STAGE IA,IB Surveillance for pT1-pT3 tumors (cat 1)(pref.)
1. H&P,AFP,LDH,beta-HCGevery 3-4 mth for years 1-2 every 6-12 mth for years 3-4 annually
2.abd./pelvic CT every 6 mth for years 1-2every 6-12 mths for year 3annually 4-5 years
3. CXR as clinically indicated for years 1-5RECURRENCE,TREAT ACCORDING TO EXTENTOF DISEASE AT RELAPSE.
OR,
SINGLE AGENT CARBOPLATIN(CAT 1)(AUC =7X1 CYCLE OR AUC= 7X2 CYCLE)
1. H&P,AFP,LDH,beta-HCGevery 3 mth for years 1 every 4 mth for year 2every 6 for years 3annually
2. abd./pelvic CT annually for years 1-3
3. CXR AS CLINICALLY INDICATED
OR,
RT(CAT 1)
1.H&P,AFP,LDH,beta-HCG every 4 mth for years 1-2annually FOR 3-10 YEARS
2. abd./pelvic CT annually for 3 years( FOR pt. status post only para-aortic RT)
3. CXR AS CLINICALLY INDICATED
PURE SEMINOMA
• STAGE IS:-repeat elevated serum tumor marker & assess with
abd./pelvic pelvic CT scan for evaluable disease.
Stage IS is uncommon and generally treated with radiation.
Recurrence, treat according to extent of disease at relapse
PURE SEMINOMA• STAGE IIA:-RT to include para-aortic and ipsilateral iliac lymph nodes to a dose
of 30-36 Gy (pref.)
1.H&P,AFP,LDH,beta-HCG every 3 mth for year 1 every 6 mth for years 2-5 annually FOR 6-10 YEARS
2.CXR every 6 mth for years 1-2
3.abd./pelvic CT every 6-12 mths for years 1-2 then annually for year 3
• Recurrence, treat according to extent of disease at relapse
Or,
PURE SEMINOMA
PRIMARY CHEMOTHERAPY :EP4 CYCLES , OR, BEP3 CYCLES For multiple +ve nodes
post-chemo follow up©
• STAGE IIB:-PRIMARY CHEMOTHERAPY :(pref. if adenopathy >3 cm)
EP4 CYCLES OR, BEP3 CYCLES
post-chemo follow up©
Or,
STAGE IIBRT to include para-aortic and ipsilateral iliac lymph nodes to a dose
of 30-36 Gy (pref.)
1. H&P,AFP,LDH,beta-HCG every 3 mth for year 1 every 6 mth for years 2-5 annually FOR 6-10 YEARS
2. CXR every 6 mth for years 1-2
3. abd./pelvic CT every 6-12 mths for years 1-2 then annually for year 3
• Recurrence, treat according to extent of disease at relapse
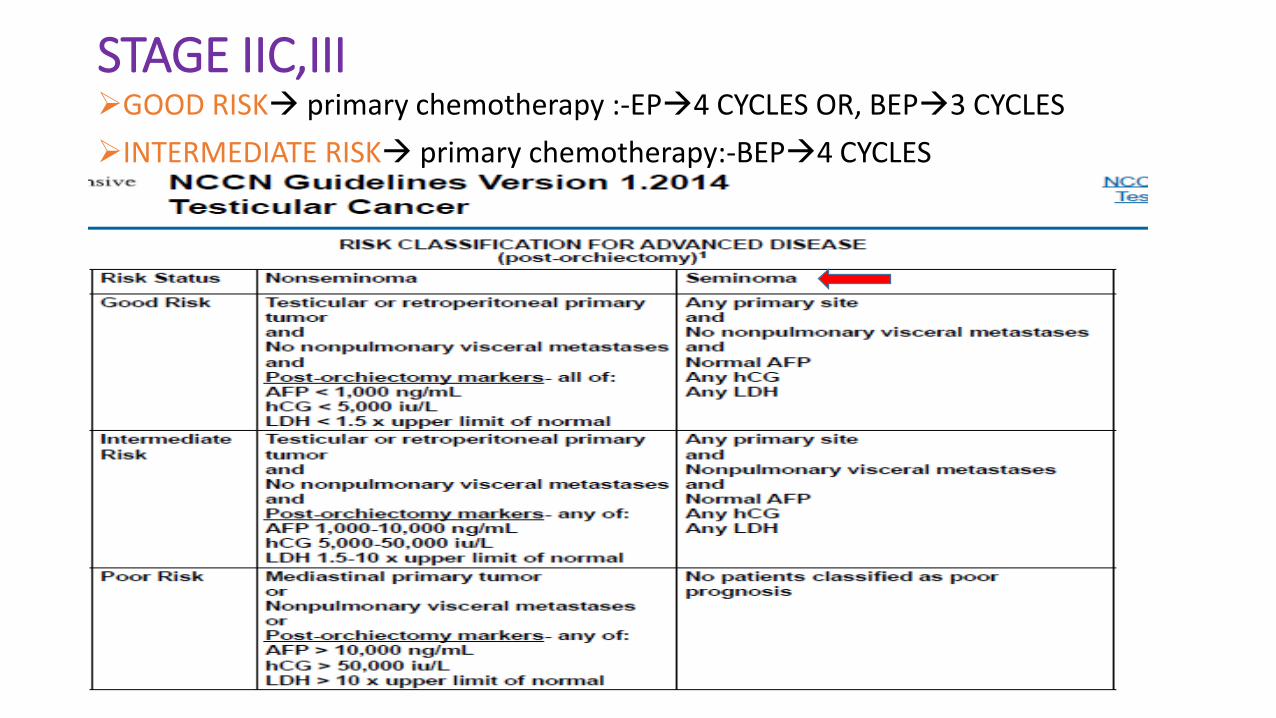
STAGE IIC,IIIGOOD RISK primary chemotherapy :-EP4 CYCLES OR, BEP3 CYCLES
INTERMEDIATE RISK primary chemotherapy:-BEP4 CYCLES
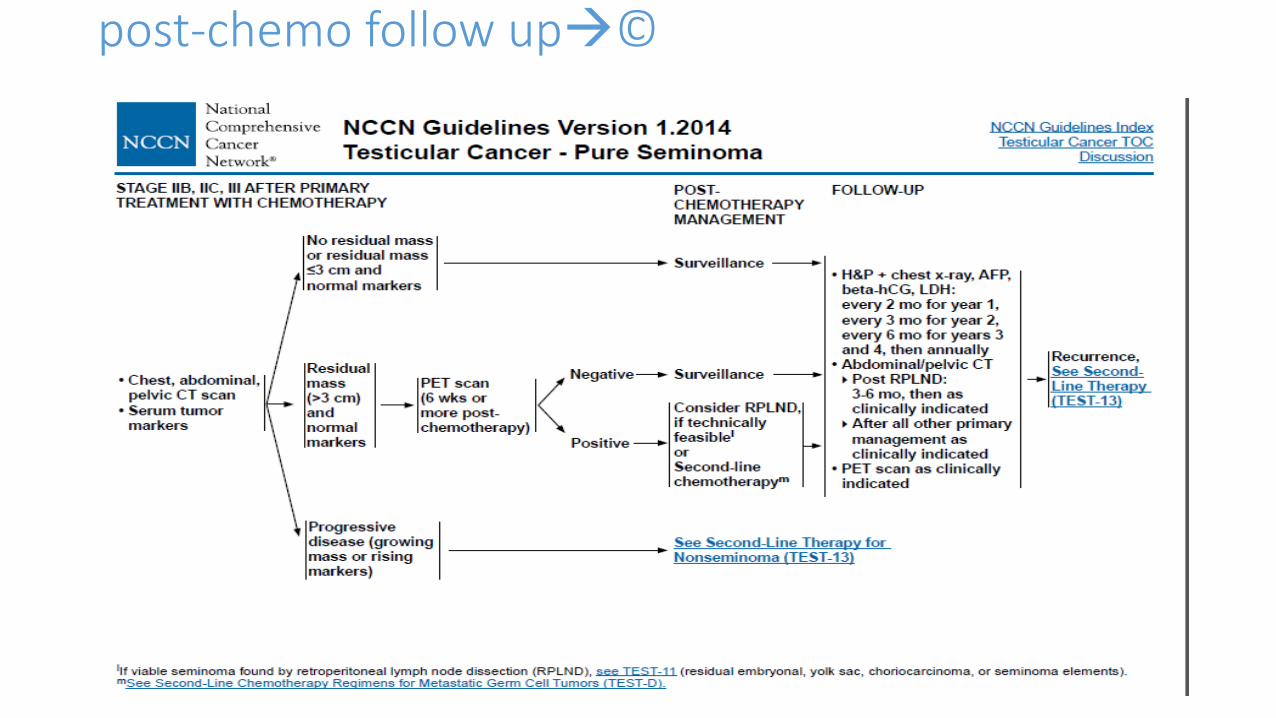
post-chemo follow up©
STRATEGIES TO REDUCE RADIOTHERAPY MORBIDITY(pure seminoma)
• SURVEILLANCE:-
Warde et al. (2002):-
638 patients with stage I seminoma followed with surveillance with 7-
year follow-up.
Increased relapse with tumors >4 cm, LVSI, and rete testis involvement.
Relapses:-
0 risk factors = 12%,
1 risk factor = 16%,
2 risk factors = 30%.Prior study showed age <34 years also increased risk of failure.
STRATEGIES TO REDUCE RADIOTHERAPY MORBIDITY
REDUCTION OF RADIATION FIELD SIZE
• MRC TE10 :- 478 patients randomised to traditional dog-leg or para-aortic radiotherapy
REDUCTION IN DOSE
• MRC TE18 :- 625 patients randomised to 30 Gray in 15 # over 3 weeks ,or, 20 Gray in 10 # over 2 weeks.
MRC TE10 (Fossa et al 1999)• Survival at 3 years, 99% for PA vs 100% for DL
• RFS 96% PA vs 96.6% DL
• Acute toxicity ( nausea, vomiting, leukopenia) was less frequent and less severe in PA group
• Within the first 18/12 of F/U the sperm counts were significantly higher after PA than after DL radiotherapy.
• CONCLUSION: Adjuvant radiotherapy confined to the paraaortic LNs is associated with decreased haematologic, GI and gonadal toxicity, but with a higher risk of pelvic recurrence compared with dog-leg radiotherapy.
MRC TE 18 (Jones et al 2001 & 2005)
• 625 patients
• 5 year relapse free survival 97.0% after 30Gy
96.4% after 20Gy
• Better Quality of Life scores for acute effects in lower dose arm:-20 Gy arm had decreased lethargy and inability to carry out normal work 1 month after treatment.
• CONCLUSION :
• Standard radiotherapy for stage 1 seminoma should be:- 20 Gy in 10 fr. over 2 weeks to para-aortic strip (unless previous inguino/pelvic/scrotal surgery when “dog-leg” field is used)
MRC/EORTC (Oliver et al. 2005)• Carboplatin vs. RT, 2005 →
• 1,477 patients were randomly assigned to receive radiotherapy (paraaortic strip or dog-leg field) or one injection of carboplatin (dose based on the formula 7× [glomerular filtration rate + 25] mg.
• With a median follow-up of 4 years, relapse-free survival rates for radiotherapy and carboplatin were similar (96.7 vs. 97.7% at 2 years; 95.9 vs. 94.8% at 3 years, respectively).
• Patients given carboplatin were less lethargic and less likely to take time off work than those given radiotherapy.
• New, second primary testicular germ cell tumors were reported in ten patients allocated irradiation (all after paraaortic strip field) and in two allocated carboplatin (5-year event rate 1.96 vs. 0.54%, p = 0.04).
• One seminoma-related death occurred after radiotherapy, and none after carboplatin.
• This trial has shown the noninferiority of carboplatin to radiotherapy in the treatment of stage I seminoma.
• Update (Oliver et al. 2008): no difference in 5-year RFS (95% chemo, 96% RT), fewer new GCTs with chemo (2 patients vs. 15 with RT).
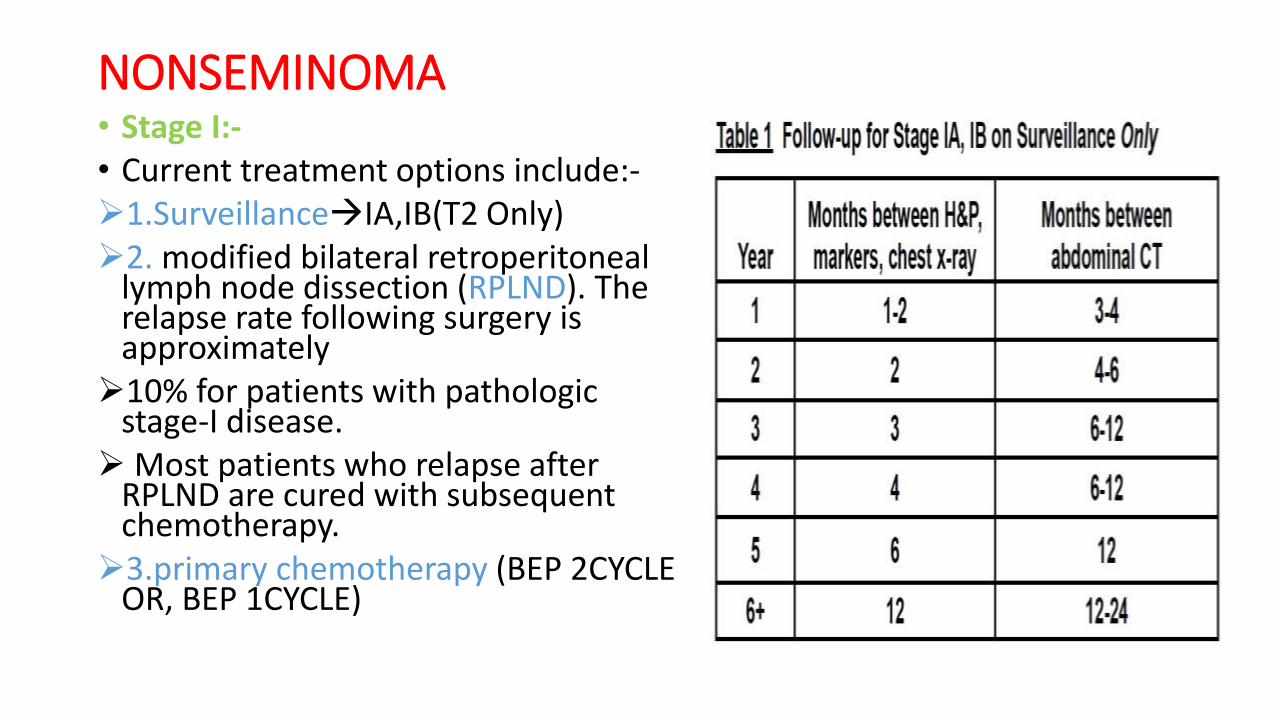
NONSEMINOMA• Stage I:-• Current treatment options include:-1.SurveillanceIA,IB(T2 Only)2. modified bilateral retroperitoneal
lymph node dissection (RPLND). The relapse rate following surgery is approximately10% for patients with pathologic
stage-I disease.Most patients who relapse after
RPLND are cured with subsequent chemotherapy.3.primary chemotherapy (BEP 2CYCLE
OR, BEP 1CYCLE)
NONSEMINOMA• Stage II:-
• The cure rate for stage II nonseminoma is approximately 98%.
• Patients with stage IIA disease with marker elevations (AFP,β-HCG, or LDH) or stage IIB disease regardless of marker status should be treated with chemotherapy(BEP 3 CYCLES OR, EP 4 CYCLES)
• IF,primary tumor histologic type is pure embryonal carcinoma, either short-term observation to see if the nodes regress or immediate treatment with chemotherapy is a reasonable option.
• IF,primary tumor is of a mixed histologic type or a teratoma, either short-term observation or immediate RPLND is the preferred option. After RPLND, surveillance or adjuvant chemotherapy may be employed .
• For patients with pathologic stage IIA or IIB disease, the risk of relapse with no adjuvant treatment after surgery is 30% to 50%.
• Relapses occur almost exclusively outside the retroperitoneum.
• Adjuvant chemotherapy with two cycles of BEP in all pathologic stage IIA or IIB patients after RPLND reduces this risk of relapse to 0% to 7%.
NONSEMINOMA
• Stage III Disease AND PERSISTENT MARKER ELEVATION(STAGE IS,IIA,IIB):-
The standard first-line chemotherapy for all patients isbleomycin, etoposide, and cisplatin (BEP) using a 5-day schedule.
Modifications in BEP, such as substitution of cisplatin with carboplatin to reduce toxicity or improve convenience, should be avoided because they may reduce efficacy.
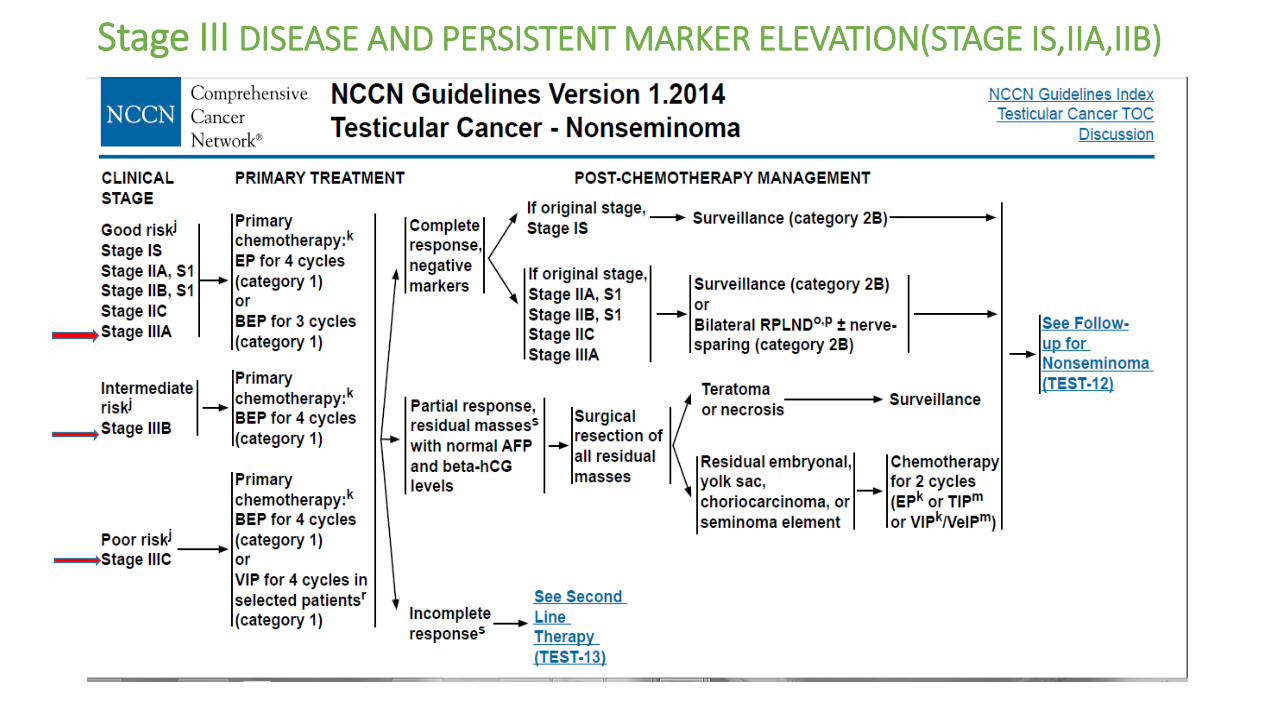
Stage III DISEASE AND PERSISTENT MARKER ELEVATION(STAGE IS,IIA,IIB)
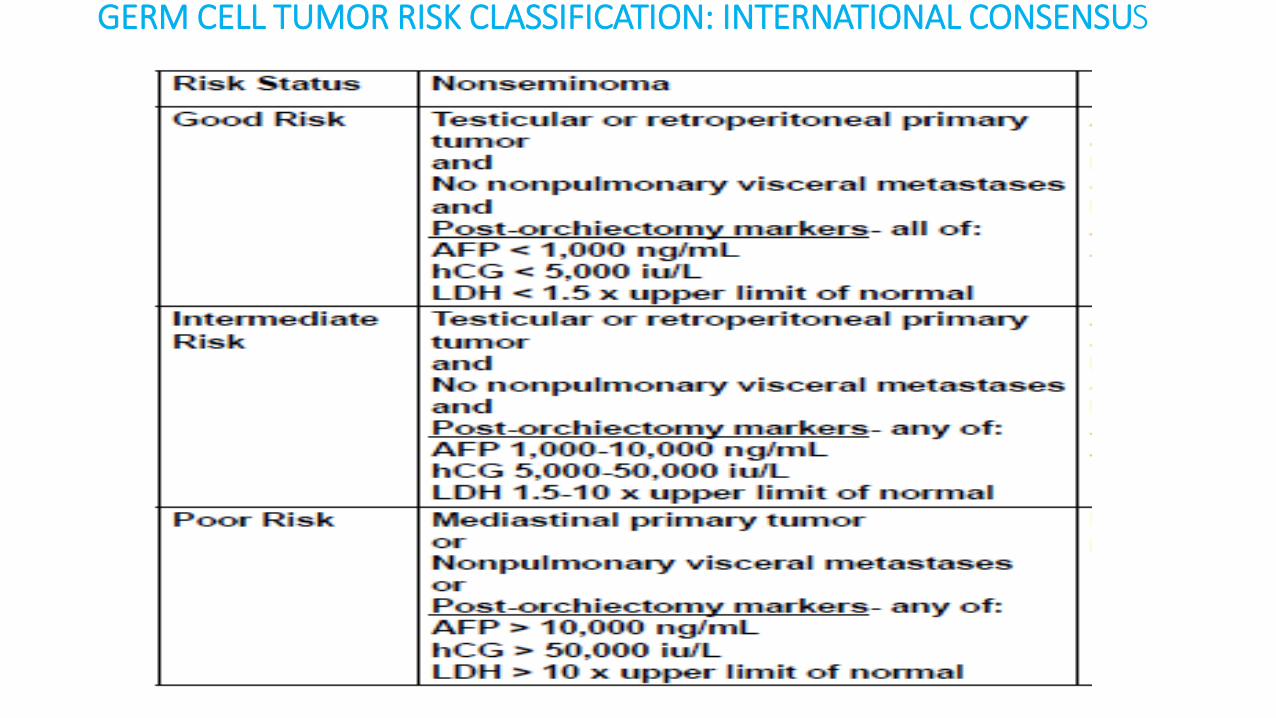
GERM CELL TUMOR RISK CLASSIFICATION: INTERNATIONAL CONSENSUS
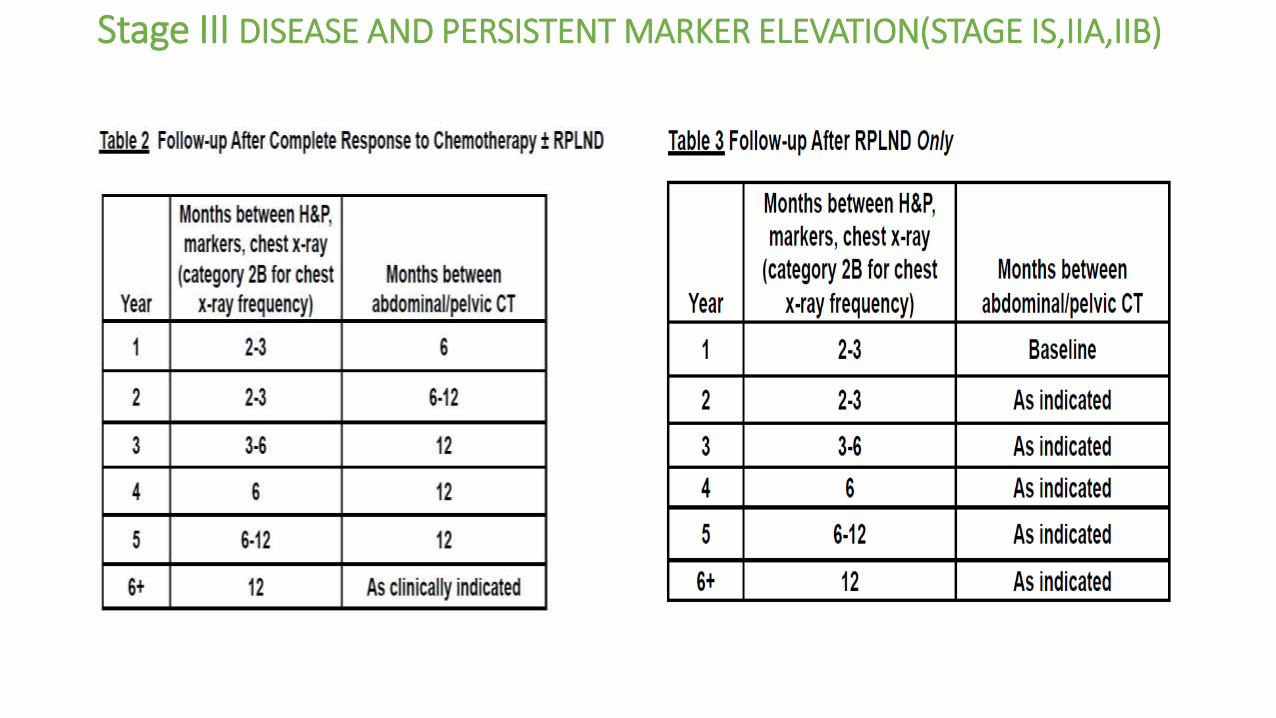
Stage III DISEASE AND PERSISTENT MARKER ELEVATION(STAGE IS,IIA,IIB)
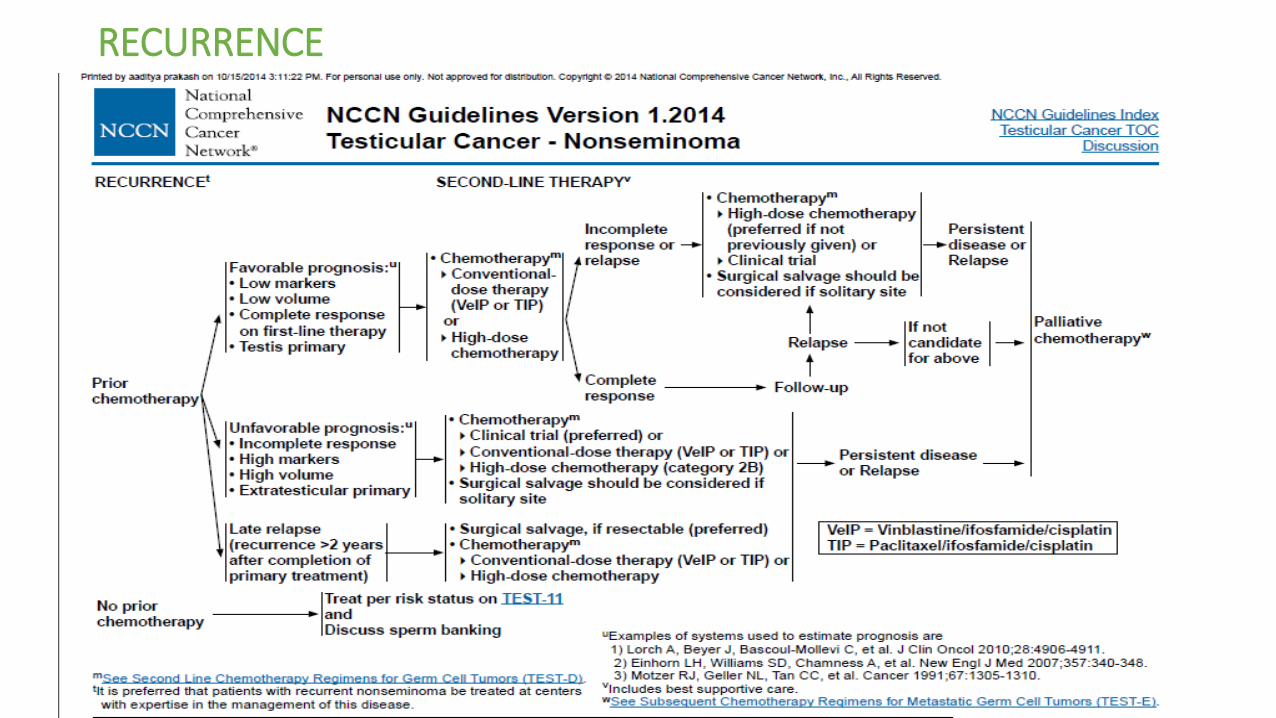
RECURRENCE
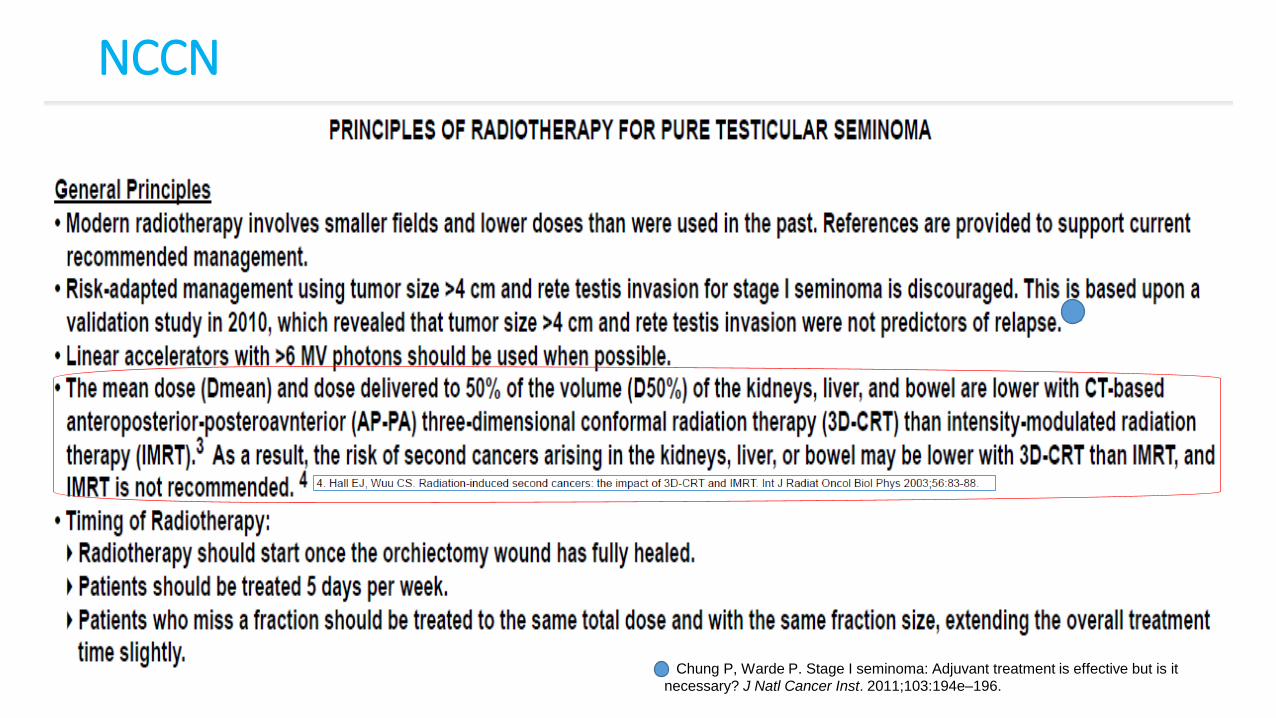
NCCN
Chung P, Warde P. Stage I seminoma: Adjuvant treatment is effective but is it
necessary? J Natl Cancer Inst. 2011;103:194e–196.
3D PLANNING 3D planning is preferred due to potential of marginal miss, with 2D
planning based on bony anatomy .
3D planning improves target definition and kidney/small bowel shielding.
Definition of the GTV for lymph node–positive disease:-
GTV node = positive lymph nodes seen on imaging.
Definition of the CTV:-CTV = Retroperitoneal +/− ipsilateral iliac lymph node region
Definition of the PTV:- PTV = CTV + 0.5 cm.
CTVnode = GTVnode + 0.8 cm, excluding bone and bowel
PTVnode = CTVnode + 0.5 cm.
Incorporate a 7 mm expansion around the PTVs to block edge to account for beam penumbra.
3D PLANNING
■
■ Para-aortic field: retroperitoneal lymph node coverage
● Contour the inferior vena cava and aorta separately from 2 cm below the top of the kidneys down to the point where these vessels bifurcate.
● Use a 1.2 cm expansion radially around the inferior vena cava and a 1.9 cm expansion around the aorta, excluding bone and bowel.
■ Dogleg field: Ipsilateral iliac lymph node coverage ● In addition to the para-
aortic field described above, contour the ipsilateral common, external, and proximal internal iliac veins and arteries down to the upper border of the acetabulum.● Use a 1.2 cm expansion
on the iliac vessels, excluding bone and bowel.
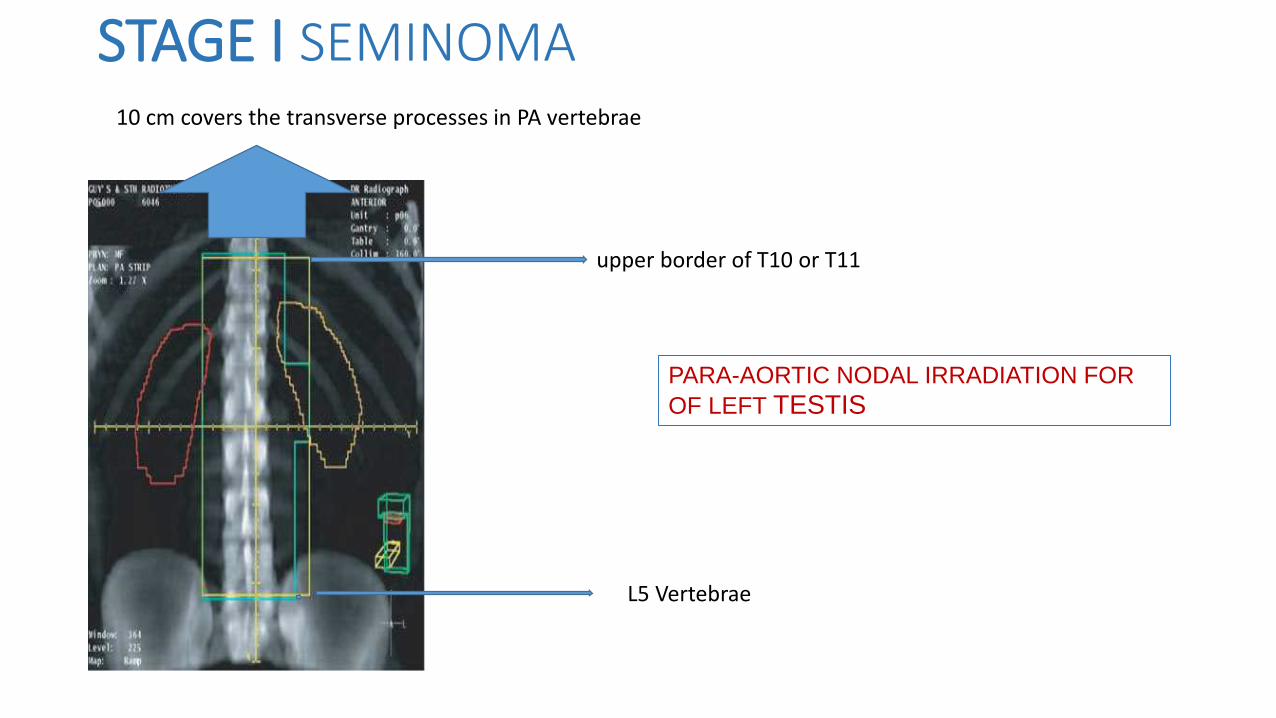
STAGE I SEMINOMA
PARA-AORTIC NODAL IRRADIATION FOR
OF LEFT TESTIS
10 cm covers the transverse processes in PA vertebrae
upper border of T10 or T11
L5 Vertebrae
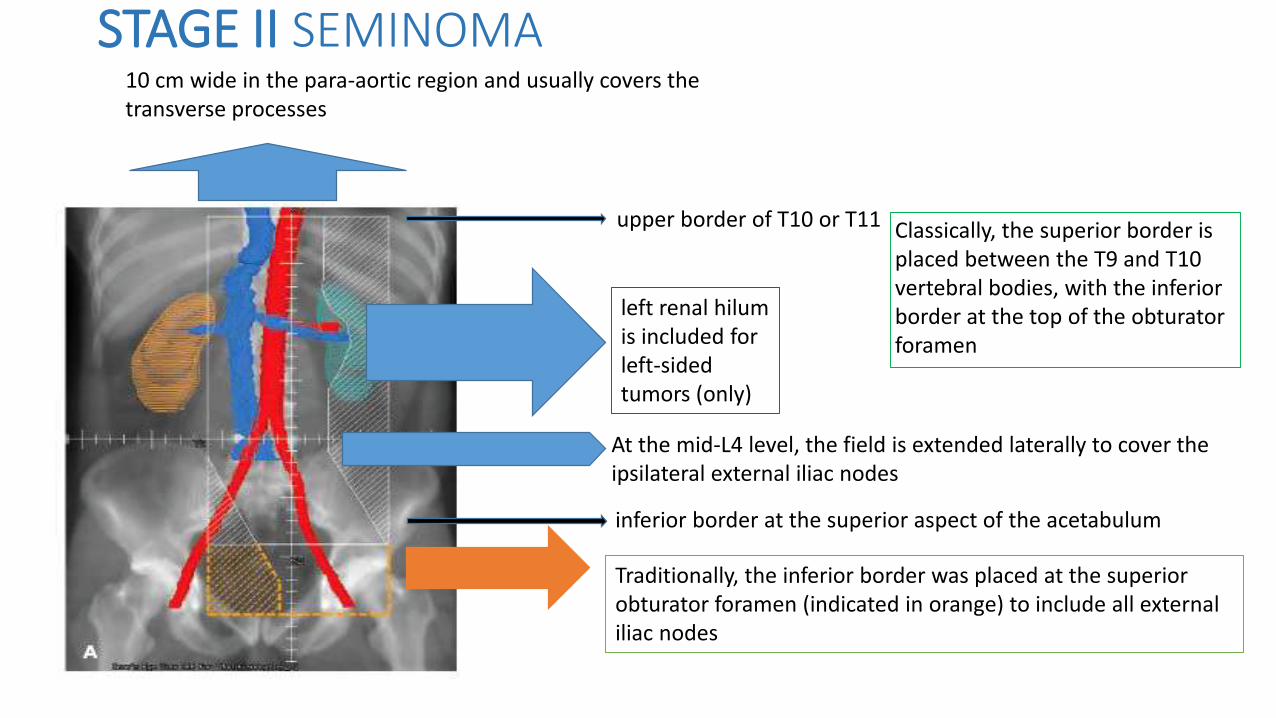
STAGE II SEMINOMA
upper border of T10 or T11 Classically, the superior border is placed between the T9 and T10 vertebral bodies, with the inferior border at the top of the obturator foramen
left renal hilum is included for left-sided tumors (only)
inferior border at the superior aspect of the acetabulum
Traditionally, the inferior border was placed at the superior obturator foramen (indicated in orange) to include all external iliac nodes
10 cm wide in the para-aortic region and usually covers the transverse processes
At the mid-L4 level, the field is extended laterally to cover the ipsilateral external iliac nodes
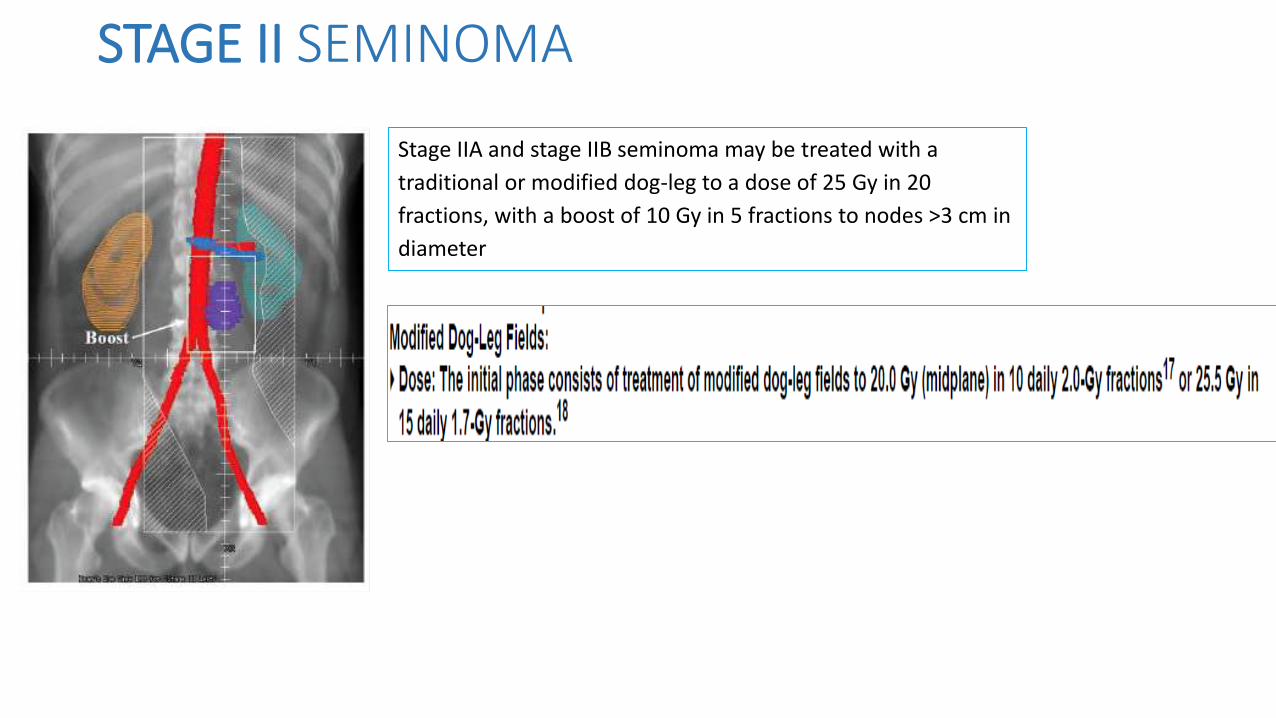
STAGE II SEMINOMA
Stage IIA and stage IIB seminoma may be treated with a
traditional or modified dog-leg to a dose of 25 Gy in 20
fractions, with a boost of 10 Gy in 5 fractions to nodes >3 cm in
diameter
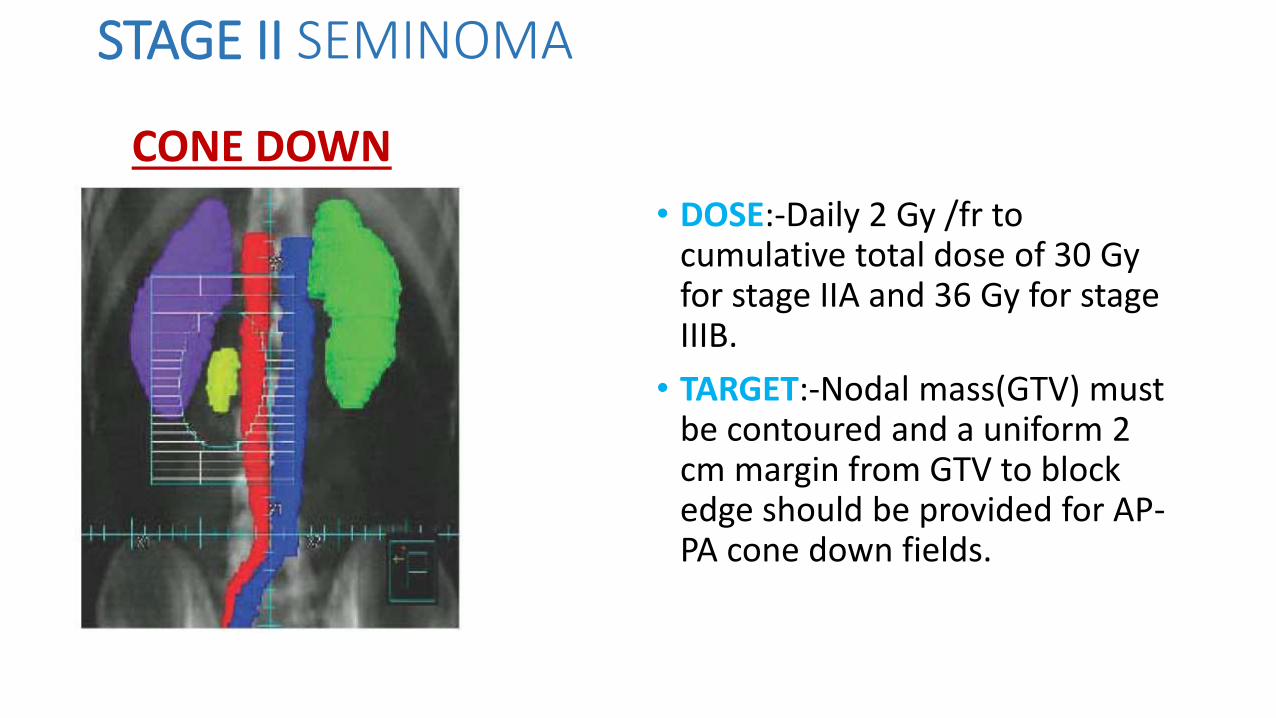
STAGE II SEMINOMA
• DOSE:-Daily 2 Gy /fr to cumulative total dose of 30 Gyfor stage IIA and 36 Gy for stage IIIB.
• TARGET:-Nodal mass(GTV) must be contoured and a uniform 2 cm margin from GTV to block edge should be provided for AP-PA cone down fields.
CONE DOWN
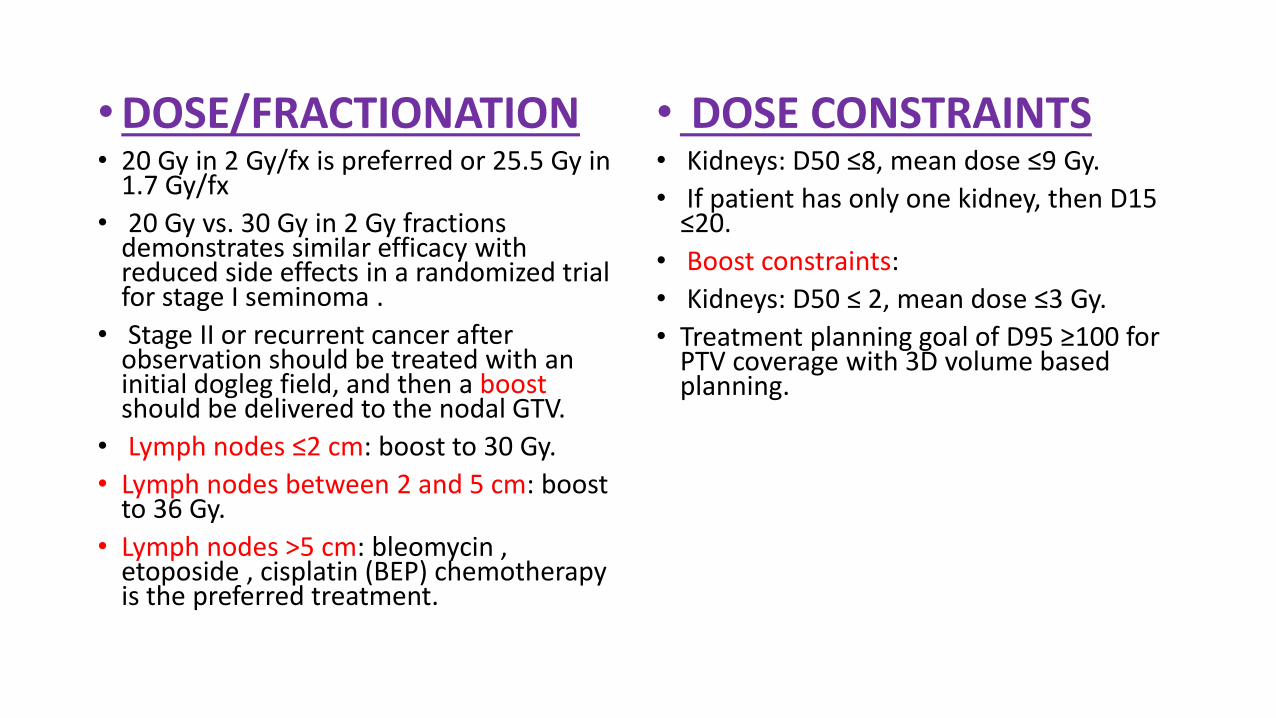
•DOSE/FRACTIONATION• 20 Gy in 2 Gy/fx is preferred or 25.5 Gy in
1.7 Gy/fx
• 20 Gy vs. 30 Gy in 2 Gy fractions demonstrates similar efficacy with reduced side effects in a randomized trial for stage I seminoma .
• Stage II or recurrent cancer after observation should be treated with an initial dogleg field, and then a boostshould be delivered to the nodal GTV.
• Lymph nodes ≤2 cm: boost to 30 Gy.
• Lymph nodes between 2 and 5 cm: boost to 36 Gy.
• Lymph nodes >5 cm: bleomycin , etoposide , cisplatin (BEP) chemotherapy is the preferred treatment.
• DOSE CONSTRAINTS• Kidneys: D50 ≤8, mean dose ≤9 Gy.
• If patient has only one kidney, then D15 ≤20.
• Boost constraints:
• Kidneys: D50 ≤ 2, mean dose ≤3 Gy.
• Treatment planning goal of D95 ≥100 for PTV coverage with 3D volume based planning.
SHIELDING
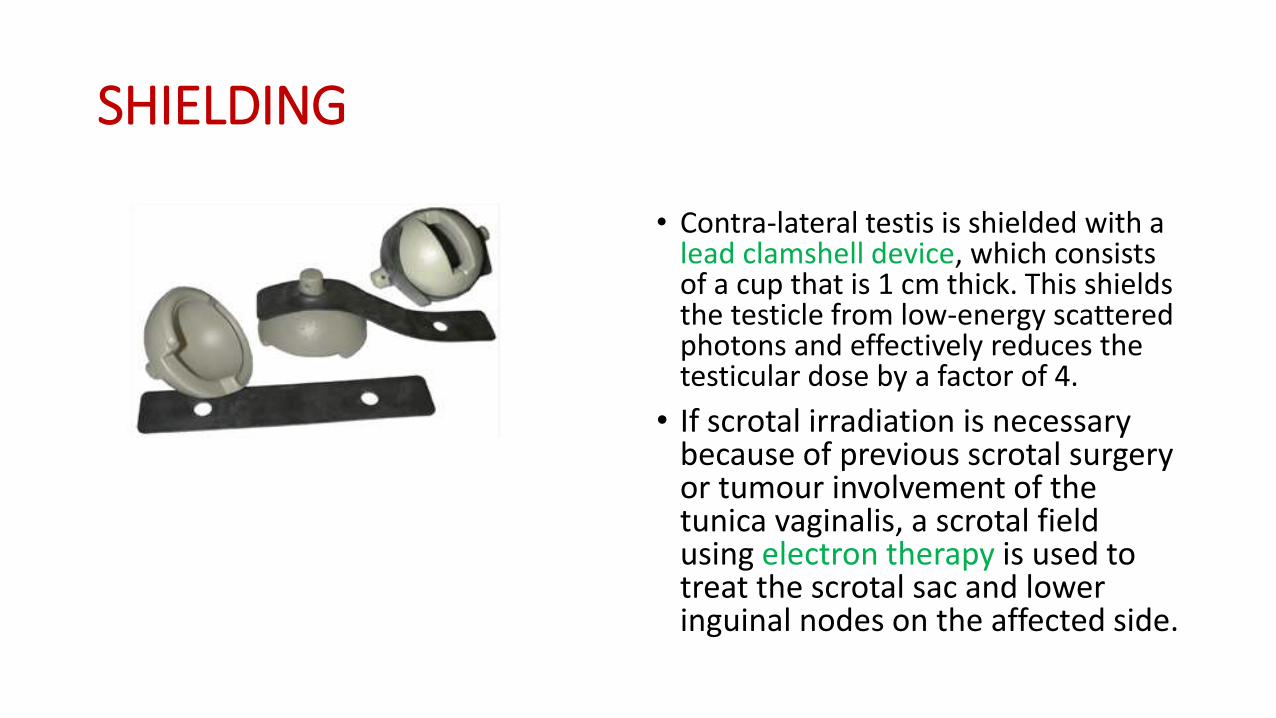
• Contra-lateral testis is shielded with a lead clamshell device, which consists of a cup that is 1 cm thick. This shields the testicle from low-energy scattered photons and effectively reduces the testicular dose by a factor of 4.
• If scrotal irradiation is necessary because of previous scrotal surgery or tumour involvement of the tunica vaginalis, a scrotal field using electron therapy is used to treat the scrotal sac and lower inguinal nodes on the affected side.

THANK YOU
Top Related