





Languages
Pages
Legal


Stress Echocardiography;Which Method?
Seung Woo Park, MD.
CVIC, Samsung Medical CenterSungkyunkwan University School of Medicine

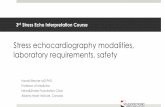
Sequence of Events During PTCAIschemic Cascade
Sigwart, 1984Sigwart, 1984
OcclusionOcclusion
Relaxation failureRelaxation failure
Contraction failureContraction failure
filling pressurefilling pressure
ECG changesECG changesAnginaAngina
IschemiaIschemia
SecondsSeconds1010 2020 3030

Stress ModalitiesExercise
•Treadmill•Bicycle – upright or supine
Pharmacologic•Dobutamine•Dipyridamole•Adenosine•Ergonovine
Other•Transesophageal atrial pacing•Combined modalities

Echo Parameter
Regional wall motionDoppler parameters
•Diastolic function of LV•Coronary flow reserve (CFR)•Myocardial velocity•Strain, Strain rate
Other•2-D strain, strain rate•Perfusion with contrast agent

Qantitative Assessment
• May be future• Simplification for measurement• More validation
ASE guideline 2007

Exercise vs Nonexercise
A patient’s exercise capacity carries prognostic information, independent of demonstration of ischemia
McCully: JACC, 1998 (exercise echo)Goraya: Ann Int Med, 2000 (exercise ECG)

Exercise Echocardiography
•Detection of CAD
•Quantification of CAD
•Prognostic value

Exercise Echo Protocol
Exercise Echo Protocol
• Baseline images• Baseline HR, BP, ECG• Symptom-limited exercise test. BP, HR,
ECG monitoring• Post-exercise (peak for bicycle) images• Side by side display of rest and stress
images

TMET Stress Echo
Advantages
• Physiologic
• ECG predictable
• Exercise information
• 2 sets of Images
Disadvantages
• Must be able to walk
• ? Reach target HR
• Peak images only and
may be difficult

Bicycle Stress Echo
Advantages• Continuous Imaging
• Ischemic threshold
• Hemodynamics
• ? Detect more ischemia
Disadvantages• Exercise awkward
• Lower work load
• HR lower, BP higher

Recovery time (min)Recovery time (min)
HRHR
60708090
100110120130140150160170
Peak 1 2 3 4 5 6 7 8 9 10exercise
Peak 1 2 3 4 5 6 7 8 9 10exercise
AtropineAtropineSalineSaline*P<0.05*P<0.05
**
****
** ** ** ** ** **
Attenhoffer et al: Echocardiography, 2000
Heart Rate Decline After Exercise

82
67
888075
60
8190
0
20
40
60
80
100Supine bikeSupine bike
Overall 1 vessel 2 vessel n=10n=57 n=15 n=42
Sensitivity Specificity
%
TreadmillTreadmill
Badruddin et al: JACC, 1999
Sensitivity and Specificity of SupineBike vs Treadmill Exercise Echo

Disadvantages• Not as physiologic
• Low dose - contractility
• High dose - HR
• Need IV
• Dynamic LVOT
• Arrhythmias
Dobutamine Stress Echo
Advantages• No exercise
• Target HR reached
• Continuous imaging
• Ischemic threshold
• Hemodynamics
• Viability
• Images easier

Dobutamine PharmacologyDobutamine Pharmacology
• Synthetic catecholamine, B1• Increases myocardial oxygen demand
Increases contractilityIncreases heart rate
• Half-life 2 minutes

Dobutamine Stress EchoContraindications
Dobutamine Stress EchoContraindications
• DobutamineUncontrolled hypertensionUncontrolled dysrhythmia
• AtropineUntreated narrow angle glaucomaSevere urinary retention

Dobutamine Stress EchoProtocol
Dobutaminedose(mcg/kg/min)
Dobutaminedose(mcg/kg/min)Time (min)BPEchoECG
Time (min)BPEchoECG
00 33 66 99 1212 1515
55
1010
2020
Atropine 0.5 mg,repeat 0.25 q minuteAtropine 0.5 mg,repeat 0.25 q minute
4040
3030

Dobutamine Stress Echo Endpoints
Dobutamine Stress Echo Endpoints
• Peak dose• Target heart rate .85 (220-age)• Moderate or extensive wall motion
abnormalities• Significant arrhythmia• Hypotension, severe hypertension• Intolerable symptoms

Dobutamine-side effectsDobutamine-side effects• Palpitations• Chest pain• Tremor or shivering• Headache• Urinary urgency• Nausea• Dyspnea• Lightheadedness• Hypertension, hypotension• Arrhythmias

Dobutamine Stress EchoAssessment of Myocardial Viability
Early after MI(stunned)Early after MI(stunned)
Chronic LV dysfunction(hibernating)Chronic LV dysfunction(hibernating)
TimeTime CABG orPCICABG orPCI
Improved contractility with dobutamine
Predicts recovery of LV function

Myocardial ViabilityDobutamine Stress Echocardiography
RestRest Low doseLow dose High doseHigh doseX XX XX XX X
Open
Scar
Open
Viable
Viable

Normal Response in DSE

Stunned Myocardium in DSE

Nonviable Myocardium in DSE

Hibernating Myocardium in DSE
Low Dose
Baseline
High Dose

SensitivitySpecificitySensitivitySpecificity
Echo vs Nuclear ImagingPrediction of Contractile Recovery
%%
Studies (no.) 32 22 11 20 20Patients (no.) 1,090 557 301 488 598Studies (no.) 32 22 11 20 20Patients (no.) 1,090 557 301 488 598
81 80 86
59
88
50
8166
93
58
Bax, et al Curr Prob Cardiol, Feb 2001

Vasodilator Stress Pharmacology
•DipyridamoleIncreases endogenous levels of adenosine
•AdenosineDecreases resistance

Dipyridamole Stress EchoProtocol I
Infusion of 0.14 mg/kg/minx 4 min (0.56 mg/kg)
• Additional 0.28 mg/kg x 2 min • Atropine, handgrip exercise
Imaging if no RWMA for 4
min
EAE guideline 2008

Dipyridamole Stress Echo Protocol II
EAE guideline 2008

AdenosineAdenosine
50 g/kg/min50 g/kg/min
EchoEcho1 min1 min
4 min4 min7575
100100
140140
HandgripHandgrip
Adenosine Stress EchoProtocol

Vasodilator Stress Contraindications
• DipyridamoleHypotensionUnstable carotid disease
• Adenosine or dipyridamoleSevere bronchospasmHeart block: 2nd or 3rd degree

Response for Stress Modalities

Rest Stress Interpretation
Normal Hyperdynamic Normal
Normal New wall motion Ischemiaabnormality
Wall motion Worsening Ischemiaabnormality
Wall motion Unchanged Infarctabnormality
Wall motion Biphasic Viableabnormality
Interpretation of Regional Wall Motion

Stress EchocardiographyValidation with Coronary Angiography
No. Sens SpecTreadmill 1,020 88 82
Bike 676 89 83
Dobutamine 1,240 85 83
Pellikka: Prog in CV Dis, 1997

88 82 8782 77 8274
9477
0
20
40
60
80
100
Sensitivity Specificity Accuracy
%%
ExerciseExercise DobutamineDobutamine DipyridamoleDipyridamole
n=119n=119 n=17n=17 n=136n=136
P=0.002P=0.002 P=0.001P=0.001
n=136
Beleslin et al. Circulation, 1994
Comparison of Tests in Detecting CAD

Dip-stress vs Exe-stress EchoCG for detection of coronary artery disease
Sensitivity Specificity Accuracy Feasibility
EAE guideline 2008

Dip-stress vs Dob-stress EchoCG for detection of coronary artery disease
EAE guideline 2008

Esophageal Pacing Stress Echo
Lee et al JACC,1999
Protocol
1. Small esophageal lead placed
2. Begin pacing 10 beats/min above baseline
3. Increase pacing 20 beats/min every 2 min until 85% HR reached or other endpoints

Esophageal Pacing Stress Echo
Advantages• Fast protocol
• Reach target HR
• Continuous imaging
• Avoid arrhythmias
• Avoid HTN response
Disadvantages• Esophageal intubation
• Rare sedation needed
• IV start
• BP response variable
• Atropine +/-

• Role of stress echo in predicting cardiac events has been documented in >40 studies in >10,000 patients
• Positive study identifies patients at risk of events during follow-up
• Normal study predicts a good outcome
Stress EchocardiographyPrognostic Value

50
60
70
80
90
100
0 1 2 3 4
%%
Follow-up (years)Follow-up (years)
Median follow-up 23 mo
ObservedExpected
McCully et al: JACC, 1998
Normal Exercise EchoOverall Survival in 1,325 Patients

0
20
40
60
80
100
0 1 2 3 4 5Years
%Exercise WMSI =11 exercise WMSI 1.5Exercise WMSI 1.5P<0.001
Arruda et al: JACC, 2001
Effect of Exercise WMSI on Survival Free ofAll Cardiac Events in 2,632 Patients > 65 years

0
50
100
150
200
X2X2 0.0030.0030.00010.0001
0.00010.0001
Clinical and Rest EchoClinical and Rest Echo + Exercise ECGClinical and Rest Echo + Exercise ECG + Exercise Echo
Cardiac death or myocardial infarctionArruda et al: JACC, 2001
Incremental Value of Exercise Echocardiography in 2,632 Patients 65 years

Conclusion
• Various stress echo modalities significantly improve the diagnostic and prognostic power in the evaluation of patients with CAD.
• The choice of imaging modality in a particular setting depends on several factors including availability, feasibility, experience and cost considerations.

Top Related