







Languages
Pages
Legal

16/09/2014
1
Visual function in early macular disease
Michael Crossland PhD MCOptom DipRVI
Moorfields Eye Hospital NHS Foundation Trust
UCL Institute of Ophthalmology
LVI-Dagarna 2014, Vaxjo, Sweden, September 2014
Talk outline
• Visual function in early macular disease • Dark adapted visual function
• Visual function when a scotoma has developed • The development of the preferred retinal locus
• (Other talk) • Rehabilitation options in early macular disease
Visual function in early macular disease
Why early eye disease?
In time, everyone will have only early eye disease
SI/SSI registration in Leeds: AMD
Rostron & McKibbin, Eye 2012
Assessing early macular disease

16/09/2014
2
Structure Function Performance
Dark-adapted function in early macular disease • Structure: Rod loss in ARM
• Curcio, 1996; Curcio, 2001
• Function: Reduced scotopic sensitivity in ARM • Scholl, 2004
• Performance: Reduced dark-adapted function in ARM • Scilley, 2002
Functional measurement of dark-adapted visual function
21st century measurement of visual fields
Adaptation made to MP-1
• Shielding of stray light
• 2 log unit + short pass filters over display system
• Reduction of IR illumination for retinal imaging
• Now adopted by Nidek in MP-1S
Crossland, 2011
Optical path of
display systemOptical path of
imaging systemFilters
1: ABW (1586439) VA: 0.3 logMAR (6/12, 20/40)
CONVENTIONAL DARK-ADAPTED
16/09/2014
3
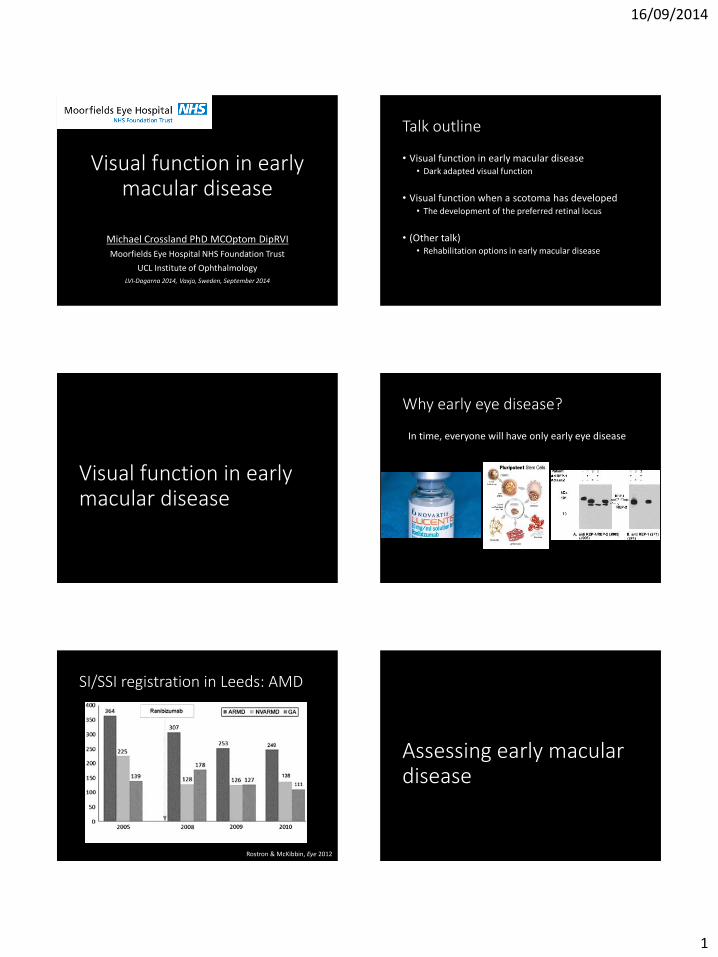
7: PF (1724597) VA: 0.6 logMAR (6/24, 20/80)
CONVENTIONAL DARK-ADAPTED
11: WR (1282157) VA: 0.22 logMAR (6/9.5, 20/32)
CONVENTIONAL DARK-ADAPTED
Dark adapted vision is worse in people with early macular disease…
…does this affect them?
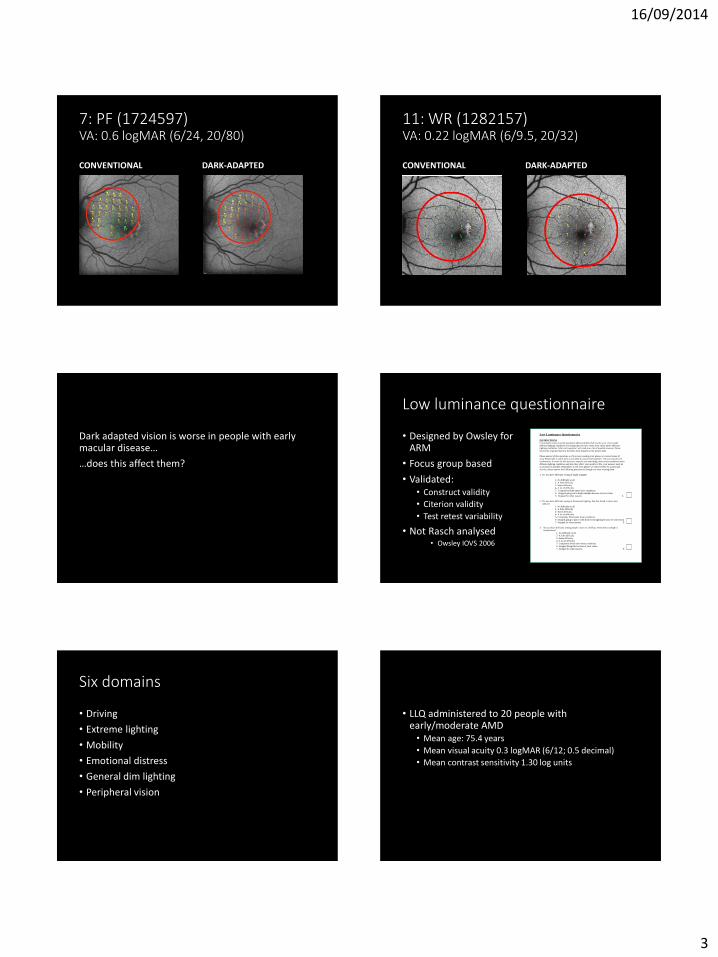
Low luminance questionnaire
• Designed by Owsley for ARM
• Focus group based
• Validated: • Construct validity
• Citerion validity
• Test retest variability
• Not Rasch analysed • Owsley IOVS 2006
Low Luminance Questionnaire
INSTRUCTIONS
I�m going to read you some statements about problems that involve your vision under
different lighting conditions or feelings that you have about your vision under different
lighting conditions. After each question I will read you a list of possible answers. Please
choose the response that best describes your situation at the present time.
Please answer all the questions as if you were wearing your glasses or contact lenses (if
any). Please take as much time as you need to answer each question. All your answers are
confidential. In order for this survey to improve our knowledge about vision problems under
different lighting conditions and how they affect your quality of life, your answers must be
as accurate as possible. Remember, if you wear glasses or contact lenses for a particular
activity, please answer the following questions as though you were wearing them.
1. Do you have difficulty seeing in bright sunlight?
1- No difficulty at all
2- A little difficulty
3- Some difficulty 4- A lot of difficulty
5- Completely blind under these conditions
6- Stopped going out in bright sunlight because of your vision
7- Stopped for other reasons 1.
2. Do you have difficulty seeing in fluorescent lighting, like that found in stores and
offices?
1- No difficulty at all
2- A little difficulty
3- Some difficulty 4- A lot of difficulty
5- Completely blind under these conditions
6- Stopped going to places with fluorescent lighting because of your vision
7- Stopped for other reasons 2.
3. Do you have difficulty seeing people�s faces in a hallway when direct sunlight is
behind them?
1- No difficulty at all
2- A little difficulty
3- Some difficulty
4- A lot of difficulty
5- Completely blind under these conditions
6- Stopped doing this because of your vision
7- Stopped for other reasons 3.
Six domains
• Driving
• Extreme lighting
• Mobility
• Emotional distress
• General dim lighting
• Peripheral vision
• LLQ administered to 20 people with early/moderate AMD • Mean age: 75.4 years
• Mean visual acuity 0.3 logMAR (6/12; 0.5 decimal)
• Mean contrast sensitivity 1.30 log units

16/09/2014
4
LLQ performance in early AMD
0
500
1000
1500
2000
2500
3000
3500
Driving Extreme lighting Mobility Emotional
distress
General dim
lighting
Peripheral vision TOTAL
* * * * *
*
LLQ and clinical tests
Visual acuity Contrast sensitivity
R² = 0.396
0
500
1000
1500
2000
2500
3000
3500
-0.2 0 0.2 0.4 0.6 0.8
LLQ
VA (logMAR)
R² = 0.2381
0
500
1000
1500
2000
2500
3000
3500
1 1.2 1.4 1.6 1.8
LLQ
CS (log units)
LLQ and microperimetry
Conventional Dark-adapted
R² = 0.2348
0
500
1000
1500
2000
2500
3000
3500
0 5 10 15 20
LLQ
so
cre
Conventional microperimetry: Mean sensitivity (dB)
R² = 0.4299
0
500
1000
1500
2000
2500
3000
3500
0 5 10 15 20
LLQ
so
cre
Dark-adapted microperimetry: Mean sensitivity (dB)
Visual acuity Contrast
sensitivity Conventional
microperimetry Dark-adapted
microperimetry
General dim lighting 0.12 0.47* 0.37* 0.44*
Extreme lighting 0.20* 0.29* 0.23* 0.53*
Driving 0.46* 0.16 0.21 0.38*
Emotional distress 0.06 0.01 0.01 0.00
Mobility 0.36* 0.23* 0.01 0.21*
Peripheral vision 0.01 0.00 0.00 0.04
Total LLQ 0.40* 0.24* 0.23* 0.43*
Summary
• Early vision loss is becoming more common
• People with early macular disease report poor performance in low light conditions
• Early low vision intervention may be useful
• Lighting advice, consumer electronics and tints may be important to consider
• Further research is needed
After a scotoma develops: the development of the preferred retinal locus

16/09/2014
5
Preferred retinal locus (PRL)

16/09/2014
6
• Prospective, observational study
• New vision loss in better eye
• Observation of fixation position and eye movements at 0, 1, 3, 6, 12 months
• Study performed in the pre-anti-VEGF era
Rodenstock SLO-101 Development of the PRL
0
20
40
60
80
100
0 2 4 6 8 10 12
% of people
Time (months)
Crossland, Kabanarou, Culham & Rubin, Ophthalmology 2005
PRL location
0
2
4
6
8
10
12
Above Below Left Right Central
Baseline
Exit
Crossland, Kabanarou, Culham & Rubin, Ophthalmology 2005
PRL location & reading speed
Reading speed: F(df=2,24)=0.67, p=0.52
Crossland, Kabanarou, Culham & Rubin, Ophthalmology 2005 Fletcher & Schuchard, Ophthalmology 1997 Fletcher, Schuchard & Watson, J Rehab Res Dev 1999
0
10
20
30
40
50
60
Below Left Right Above
% o
f p
eop
le
Crossland 2005
Fletcher 1997
Fletcher 1999

16/09/2014
7
What does affect reading speed? Fixation stability and reading
Crossland, Culham & Rubin, Ophth Physiol Opt 2004
Fixation stability and reading
Amore, Crossland et al Ophth Physiol Opt 2013
R2=0.51
Changes in fixation stability
Crossland, Culham, Rubin 2004
Can we compensate for poor fixation stability?
PC1
read this words
eyetracker
control
Ethernet cable
PC2
« stimulus displayEYELINK I
SETUPSampling rate 250 Hz
Can we compensate for poor fixation stability? • RSVP presentation of text
• N=10, AMD, Stargardt, Best disease
• Condition 1: Baseline
• Condition 2: Stabilise all eye movements
• Condition 3: Stabilise microsaccades, drift, tremor; allow intra-word saccades
• Condition 4: Exaggerate eye movements

16/09/2014
8
Can we compensate for poor fixation stability?
Baseline Instability corrected; within-word saccades allowed
Macedo, Crossland, Rubin, 2011
Can fixation stability be improved with training?
Can fixation stability be improved with training?
• Training improves fixation stability in control subjects using peripheral fixation
(Zeevi, JOSA, 1979)
• Target shooters have better fixation stability than controls
(Di Russo, Vision Research, 2003)
• Reading speed improves after fixation training in patients
(no control groups, stability not measured) (Nilsson Optom Vis Sci 1998 ; Contestabile Eye 2002; Seiple IOVS
2005)
Fixation stability training
• Eccentric viewing training • Backman and Inde, Sweden • Goodrich and Quillman, USA
• Eye movement training • Seiple Invest Ophthalmol Vision Sci, 2005
• Intensive in-patient rehabilitation • E.g. Veterans Administration, USA
• Intensive outpatient training • E.g. Nilsson Vision Research 2003
• Training by people with MD • E.g. “Train the trainer”, Macular Disease Society, UK
• Training by exercises at home
Fixation stability training
• Is fixation training better than placebo?
• What is the best way of training the PRL?
• Should we be training people for reading? • If so, will this negatively affect performance on other
tasks?
• Is training cost-effective?
Fixation stability training
• Lack of clear evidence • EFFECT trial (Eccentric Fixation From Enhanced Clinical
Training)

16/09/2014
9
EFFECT trial
• Four arm RCT • PRL training
• TRL training
• Supervised reading practice
• Standard care only
• Outcomes • Massof Activity Inventory
• Reading speed
• Health economic analysis
Progress
• Sample size calculation: 200 participants
• Currently recruited: 140
Conclusions
• People develop a preferred retinal locus within six months of scotoma development
• Fixation instability is strongly associated with reading difficulty
• Compensating unstable fixation may improve reading ability
• Training fixation may improve reading ability
Clinical implications
• Early vision loss is becoming more common
• Rehabilitation options will be different • Tints
• Lighting
• Consumer devices…
• Fixation stability is important for people with macular disease
• Training may help people hold their fixation more steadily
Thank you for your attention
Top Related