






Languages
Pages
Legal


5/12/2021
1
Reversibility of Type 2 Diabeteswith Plant Diet Nutrition
John Kelly, MD, MPH, LM Specialist
Lead Faculty, ACLM ‘Reversing Type 2 Diabetes and Insulin
Resistance with Lifestyle Medicine’ Course
Co-author, Type 2 Diabetes Remission and Lifestyle Medicine: A
Position Statement From the American College of Lifestyle
Medicine
Adjunct Faculty, Preventive Medicine, Loma Linda University
Founding President, American College of Lifestyle Medicine
Disclosures
•No Conflicts of Interest or commercial interests

5/12/2021
2
Learning Objectives1. Discuss the definition and criteria for type 2 diabetes remission as
published in the ADA Diabetes Care Journal
2. Examine the evidence-based research that establishes that type 2 diabetes and insulin resistance are reversible
3. Summarize the ACLM Position Statement on Type 2 Diabetes Remission and Lifestyle Medicine

5/12/2021
3
Just imagine…
•A diet that could induce b-cell neogenesis
•A way of eating that could restore b-cell function in the pancreas without stem cells and the risks they pose…
•Well, you do not have to imagine it!
• It has been done twice in a mouse model of diabetes!
•Using an Intermittent Fasting-Mimicking Diet…
Wei, S., Han, R., Zhao, J. et al. Intermittent administration of a fasting-mimicking diet intervenes in diabetes progression, restores β cells and reconstructs gut microbiota in mice. Nutr Metab(Lond) 15, 80 (2018).

5/12/2021
4
Che
ng e
t al.
Fast
ing-M
imic
king
Die
t Pro
mote
s N
gn3
-Drive
n b
-
Cell
Regene
ration
to R
eve
rse D
iabete
s. C
ell.
2017;1
68:7
75-
788.
Just imagine…
• In mice a 4-day fasting-mimicking diet (FMD) induces a stepwise expression of Sox17 and Pdx-1, followed by Ngn3-driven generation of insulin-producing b-cells resembling that observed during pancreatic development
•FMD cycles restore insulin secretion and glucose homeostasis in both type 2 and type 1 diabetes mouse models
Cheng et al. Fasting-Mimicking Diet Promotes Ngn3-Driven b-Cell Regeneration to Reverse
Diabetes. Cell. 2017;168:775-788.
5/12/2021
5
Just imagine…
• In human type 1 diabetes pancreatic islets, fasting conditions reduce PKA and mTOR activity and induce Sox2 and Ngn3 expression and insulin production.
•The effects of the FMD are reversed by IGF-1 treatment and recapitulated by PKA and mTOR inhibition.
Cheng et al. Fasting-Mimicking Diet Promotes Ngn3-Driven b-Cell Regeneration to Reverse
Diabetes. Cell. 2017;168:775-788.
Authors conclusion…
“These results indicate that a FMD promotes the reprogramming of pancreatic cells to restore insulin generation in islets from T1D patients and reverse both T1D and T2D phenotypes in mouse models.”
Cheng et al. Fasting-Mimicking Diet Promotes Ngn3-Driven b-Cell Regeneration to Reverse
Diabetes. Cell. 2017;168:775-788.

5/12/2021
6
Discuss the definition and criteria for type 2 diabetes remission as published in the ADA Diabetes Care Journal
Progressive History of Diabetes Remission• For decades the official ADA position stated
that diabetes was an “incurable, progressive” condition, based upon UKPDS findings [1]
• With time multiple lines of evidence indicated that lifestyle change, with subsequent weight loss, could reverse the disease [2]
• A 2009 Consensus group proposed a definition with criteria for remission/reversal [3]
1. UK Prospective Diabetes Study Group. UKPDS 38. BMJ 1998 Sep 12;317(7160):703-13.
2. Trapp KB, Barnard ND. Curr Diab Rep. 2010;10:152-58. Lim EL, et al. Reversal of type 2 diabetes: normalization of beta cell function in
association with decreased pancreas and liver triacylglycerol. Diabetologia. 2011 Oct;54(10):2506-14. Lean MEJ, et al. Primary care-led
weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 2018 Feb;391:541-551.
3. Buse JB, et al. How do we define cure of diabetes? Diabetes Care 2009 Nov;32(11):2133-35.

5/12/2021
7
Criteria for DM Remission/Reversal• 2009 consensus statement definition and
clinical criteria for reversal/remission
Buse JB, et al. How do we define cure of diabetes? Diabetes Care 2009 Nov;32(11):2133-35.
Level of Remission .
Measure Partial Complete Prolonged
HbA1c <6.5 <5.7 <5.7
mmol/mol <39 <48 <48
Time ≥ 1 year ≥ 1 year ≥ 5 years
Therapy No active pharmacology or procedures
Criteria for DM Remission/Reversal• 2009 consensus statement definition and
clinical criteria for reversal/remission
Buse JB, et al. How do we define cure of diabetes? Diabetes Care 2009 Nov;32(11):2133-35.
Level of Remission .
Measure Partial Complete Prolonged
HbA1c % <6.5 <5.7 <5.7
mmol/mol <48 <39 <39
Time ≥ 1 year ≥ 1 year ≥ 5 years
Therapy No active pharmacology or procedures

5/12/2021
8
Criteria for DM Remission/Reversal• Association of British Clinical
Diabetologists and the Primary Care Diabetes Society published a different definition and criteria1. Glycemia below the threshold currently for
T2D diagnosis (HbA1c <48 mmol/mol, or fasting glucose <7.0 mmol/L, <126 mg/dL),
2. For ≥ 6 months,
3. With no glucose-lowering therapies.
Nagi D, Hambling C, Taylor R. Remission of type 2 diabetes: a position statement from the Association of
British Clinical Diabetologists (ABCD) and the Primary Care Diabetes Society (PCDS). Br J Diabetes.
2019;19:73-76.
Examine the evidence-based research that establishes that type 2 diabetes and insulin resistance are reversible

5/12/2021
9
Evidence of Remission: More Dramatic Changes Required •UKPDS actually proved T2DM is progressive and irreversible with no lifestyle changes
•Gastric bypass has ~60-85% remission rate by ‘forcing’ reduction of caloric intake (starvation also puts T2DM in remission)
•Counterpoint very-low calorie diet (VLCD) reversed liver and pancreas triacylglycerol in 4-8 weeks
Mazur A. Why were "starvation diets" promoted for diabetes in the pre-insulin period? Nutr J. 2011;10;23.
Khorgami Z, Shoar S, Saber AA, et al. Outcomes of Bariatric Surgery Versus Medical Management for Type 2 Diabetes
Mellitus: a Meta-Analysis of Randomized Controlled Trials. Obes Surg. 2018 Nov 6.
Lim EL, et al. Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and
liver triacylglycerol. Diabetologia 2011 June 9.
Dramatic Changes Required: Counterpoint Study
Lim EL, et al. Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and
liver triacylglycerol. Diabetologia 2011 June 9.

5/12/2021
10
Dramatic Changes Required: Counterpoint Study
Lim EL, et al. Reversal of type 2 diabetes: normalisation of beta cell function in association with decreased pancreas and
liver triacylglycerol. Diabetologia 2011 June 9.
LookAHEAD Diabetes Trial•Remission rate of type 2 diabetes with lifestyle change unclear.
•Measured association of long-term intensive weight-loss intervention with remission of type 2 diabetes to prediabetes or normoglycemia.
•Observational analysis of 4-year randomized controlled trial (Aug 2001 - April 2008) comparing an intensive lifestyle intervention (ILI) with diabetes support & education controls (DSE) in 4,503 US adults with BMI (body mass index) 25 or higher and type 2 diabetes.
Gregg EW, et al. Association of Intensive Lifestyle Intervention with Remission of Type 2 Diabetes. JAMA
2012;308(23):2489-96.

5/12/2021
11
LookAHEAD Diabetes Trial
•Randomly assigned to ILI, which included weekly group and individual counseling in the first 6 months, followed by 3 sessions per month for the second 6 months, and twice-monthly contact and regular refresher group series and campaigns in years 2 to 4 (n=2,241), OR to
•DSE, which was an offer of 3 group sessions per year on diet, physical activity, and social support (n=2,262).
Gregg EW, et al. Association of Intensive Lifestyle Intervention with Remission of Type 2 Diabetes. JAMA
2012;308(23):2489-96.
LookAHEAD Diabetes Trial
•MEASURES: Partial or complete remission defined as transition from meeting diabetes criteria to prediabetes or nondiabetic glycemia (fasting glucose <126 mg/dL (<7 mmol/L) and hemoglobin A1c <6.5% (<48 mmol/mol) with no anti-hyperglycemic medication)
•RESULTS: ILI participants lost more weight than DSE participants at years 1 & 4, and had greater fitness increases at years 1 & 4 (P < .001)
Gregg EW, et al. Association of Intensive Lifestyle Intervention with Remission of Type 2 Diabetes. JAMA
2012;308(23):2489-96.

5/12/2021
12
LookAHEAD Diabetes Trial•RESULTS: •The ILI group was significantly more likely to experience any remission (partial or complete), with prevalence of 11.5% during year 1 and 7.3% at year 4, compared with 2.0% for the DSE group at both time points (P < .001)
•More ILI participants had continuous, sustained remission for at least 2, 3, and 4 years compared with DSE participants
•CONCLUSIONS: Intensive lifestyle intervention was associated with greater likelihood of partial remission of type 2 diabetes compared with diabetes support & education
Gregg EW, et al. Association of Intensive Lifestyle Intervention with Remission of Type 2 Diabetes. JAMA
2012;308(23):2489-96.
DiRECT Diabetes Trial• GOALS: Assess whether intensive weight management within routine
primary care would achieve remission of type 2 diabetes
• METHODS: • Open-label, cluster-randomized trial at 49 primary care practices in
Scotland and the Tyneside region of England. • Practices were randomly assigned (1:1) to provide either a weight
management program (intervention) or best-practice care by guidelines (control)
• Stratification for study site (Tyneside or Scotland) and practice size (>5,700 or ≤5,700)
• Inclusion criteria: 20-65 years who had been diagnosed with type 2 diabetes within the past 6 years, had a body-mass index of 27-45 kg/m2, not receiving insulin.
Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-
label, cluster-randomised trial. Lancet 2018 Feb;391:541-51.

5/12/2021
13
DiRECT Diabetes Trial• INTERVENTION: Withdrawal of antidiabetic and antihypertensive drugs, total diet replacement (825-853 kcal/day formula diet for 3-5 months), stepped food reintroduction (2-8 weeks), and structured support for long-term weight loss maintenance
•OUTCOMES: Co-primary weight loss of 15 kg or more, and remission of diabetes (defined as glycated hemoglobin (HbA1c) < 6·5% (<48 mmol/mol) after at least 2 months off all antidiabetic medications, from baseline to 12 months. These outcomes were analyzed hierarchically.
Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-
label, cluster-randomised trial. Lancet 2018 Feb;391:541-51.
DiRECT Diabetes Trial•FINDINGS:
•A 1-year weight loss of 15 kg or more in 36 (24%) intervention group vs none in control group (p<0·0001). Diabetes remission achieved in 68 (46%) intervention group vs six (4%) controls (odds ratio 19·7, p<0·0001).
•Remission correlated to weight loss: no remission in 76 participants who gained weight, six (7%) of 89 participants with 0-5 kg weight loss, 19 (34%) of 56 participants with 5-10 kg loss, 16 (57%) of 28 participants with 10-15 kg loss, and 31 (86%) of 36 participants who lost 15 kg or more.
Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-
label, cluster-randomised trial. Lancet 2018 Feb;391:541-51.

5/12/2021
14
DiRECT Diabetes Trial•Weight loss 10 kg intervention and 1 kg controls (diff -8·8 kg, p<0·0001).
•Quality of life, measured by the EuroQol 5 Dimensions visual analogue scale, improved by 7.2 points in intervention and decreased by 2.9 in controls (diff 6.4 points, p=0·0012).
• INTERPRETATION: Findings show that, at 12 months, almost half of participants had remission to non-diabetic state off antidiabetic drugs. “Remission of type 2 diabetes is a practical target for primary care.”
Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-
label, cluster-randomised trial. Lancet 2018 Feb;391:541-51.
Dramatic Changes Required: The DiRECT Study
Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-
label, cluster-randomised trial. Lancet 2018 Feb;391:541-51.

5/12/2021
15
Evidence of Remission: More Dramatic Changes Required (Higher Dosing)• DiRECT VLCD & weight-maintenance diet reversed 46% T2DM
• With ≥15 kg loss → reversed 86% (similar to gastric bypass, but without adverse side-effects)
• LookAHEAD study: DSE ~2% remission (partial or complete), intensive lifestyle intervention (ILI) ~12% year-1 and <6% year-4 (ILI ~300-400% better than DSE)
• Conclusion? ILI doesn’t work → need gastric bypass
• Actually demonstrates ILI treatment not dramatic enough (too mild)Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-
label, cluster-randomised trial. Lancet 2018 Feb;391:541-51.
Gregg EW, et al. Association of an Intensive Lifestyle Intervention With Remission of Type 2 Diabetes. JAMA
2012 Dec 19;308(23):2489-96.
Prevalence of Any Remission (%)
0%
10%
20%
30%
40%
50%
Year 1 Year 2 Year 3 Year 4
2.0% 2.3% 2.2% 2.0%
11.5% 10.4% 8.7% 7.3%
ADA Diab Support&EducLookAHEAD Intensive LifestyleDiRECT Very-Low Cal Diet
Gregg EW, et al. Association of Intensive Lifestyle Intervention with Remission of Type 2 Diabetes. JAMA
2012;308(23):2489-96.

5/12/2021
16
Prevalence of Any Remission (%)
0%
10%
20%
30%
40%
50%
Year 1 Year 2 Year 3 Year 4
2.0% 2.3% 2.2% 2.0%
11.5% 10.4% 8.7% 7.3%
46%ADA Diab Support&EducLookAHEAD Intensive LifestyleDiRECT Very-Low Cal Diet
Gregg EW, et al. Association of Intensive Lifestyle Intervention with Remission of Type 2 Diabetes. JAMA
2012;308(23):2489-96.
Evidence of Remission: Dramatic Changes Required (Higher Dosing)
Lean MEJ, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial.
Lancet 2018 Feb 10;391(10120):541-551.
Gregg EW, et al. Association of an Intensive Lifestyle Intervention With Remission of Type 2 Diabetes. JAMA 2012 Dec 19;308(23):2489-96.
Group Year 1 Year 4
LookAHEAD (DSE) 2.0% 1.5%
LookAHEAD (ILI ~17 lbs) 11.5% 7.3%
DiRECT (All ~22 lbs) 46% - %
DiRECT (≥33 lbs, 15kg) 86% - %

5/12/2021
17
Clinical Remission/ Reversal: Actual Patient Outcomes
•Years of LM specialty practice outcomes show consistent drop in insulin resistance (InsR) measured with HOMA-IR
•Medication reductions with glucose improvement can indicate InsR remission – not as certain or quantifiable as when measured with HOMA-IR
•Dramatic dietary and lifestyle changes essential for remission/reversal
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Weight, lbs 55 189 86.5 392 55 183 87.5 373 0 -5.6 -2.9 <0.000
BMI 55 31.2 16.1 62.0 55 30.3 16.3 59.0 0 -0.9 -2.9 <0.000
Waist, inch 55 40.2 22.5 60 52 39.4 23 57.5 -3 -0.8 -1.9 <0.000
SBP 55 126 84 170 54 112 68 150 -1 -14 -11 <0.000
≥140 12 152 142 " 1 126 82 142 -11 -27 -18 <0.000
DBP 55 83 50 138 54 73 54 100 -1 -9.4 -11 <0.000
≥90 18 106 90 " 2 78 54 " -16 -28 -27 <0.000
Glucose† 55 106 62 365 55 96 67 162 0 -10 -10 0.015
≥126 10 173 131 " 3 121 86 " -7 -52 -30 0.014
Insulin 22 15.2 3.7 39 21 11.4 2.4 30.1 -1 -3.8 -25 0.010
HOMA-IR 22 4.51 1.05 14.8 21 3.0 0.5 11.0 -1 -1.5 -33 0.004
TChol† 55 195.8 109 296 55 170 93 253 0 -26 -13 <0.000
>220 17 245 221 " 3 198 166 " -14 -46 -19 <0.000
LDL† 54 109 51 221 54 93 36 182 0 -16 -15 <0.000
>120 18 148 121 " 5 116 89 " -13 -31 -21 <0.000
HDL*† 55 58 26 120 55 52 22 104 0 -5.6 -9.7 <0.000
TGL† 55 144 40 532 55 124 38 405 0 -20 -14 0.007
>150 20 235 152 " 12 163 67 " -8 -72 -31 0.002
hsCRP 55 2.02 0.04 95.0 54 1.41 0.01 91.2 -1 -0.6 -30 0.048
>3 12 4.71 3.05 8.81 11 2.65 0.53 6.12 -1 -2.1 -44 0.003
Beck 55 15 0 48 30 8 0 31 -25 -7.4 -49 <0.000
>19 20 29 20 " 2 9 0 " -18 -20 -69 <0.000
SF36* 43 58 13 90 43 72 29 95 0 15 25 <0.000
<75 32 38 " 75 21 68 29 95 -11 29 76 <0.000
Notes: * higher values are lower risk; † mg/dL
LM Clinic convenience
sample of 55 patients
in an 18-day ITLC
Immersion program

5/12/2021
18
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Weight, lbs 55 189 86.5 392 55 183 87.5 373 0 -5.6 -2.9 <0.000
BMI 55 31.2 16.1 62.0 55 30.3 16.3 59.0 0 -0.9 -2.9 <0.000
Waist, inch 55 40.2 22.5 60 52 39.4 23 57.5 -3 -0.8 -1.9 <0.000
SBP 55 126 84 170 54 112 68 150 -1 -14 -11 <0.000
≥140 12 152 142 " 1 126 82 142 -11 -27 -18 <0.000
DBP 55 83 50 138 54 73 54 100 -1 -9.4 -11 <0.000
≥90 18 106 90 " 2 78 54 " -16 -28 -27 <0.000
Glucose† 55 106 62 365 55 96 67 162 0 -10 -10 0.015
≥126 10 173 131 " 3 121 86 " -7 -52 -30 0.014
Insulin 22 15.2 3.7 39 21 11.4 2.4 30.1 -1 -3.8 -25 0.010
HOMA-IR 22 4.51 1.05 14.8 21 3.0 0.5 11.0 -1 -1.5 -33 0.004
TChol† 55 195.8 109 296 55 170 93 253 0 -26 -13 <0.000
>220 17 245 221 " 3 198 166 " -14 -46 -19 <0.000
LDL† 54 109 51 221 54 93 36 182 0 -16 -15 <0.000
>120 18 148 121 " 5 116 89 " -13 -31 -21 <0.000
HDL*† 55 58 26 120 55 52 22 104 0 -5.6 -9.7 <0.000
TGL† 55 144 40 532 55 124 38 405 0 -20 -14 0.007
>150 20 235 152 " 12 163 67 " -8 -72 -31 0.002
hsCRP 55 2.02 0.04 95.0 54 1.41 0.01 91.2 -1 -0.6 -30 0.048
>3 12 4.71 3.05 8.81 11 2.65 0.53 6.12 -1 -2.1 -44 0.003
Beck 55 15 0 48 30 8 0 31 -25 -7.4 -49 <0.000
>19 20 29 20 " 2 9 0 " -18 -20 -69 <0.000
SF36* 43 58 13 90 43 72 29 95 0 15 25 <0.000
<75 32 38 " 75 21 68 29 95 -11 29 76 <0.000
Notes: * higher values are lower risk; † mg/dL
LM Clinic convenience
sample of 55 patients
in an 18-day ITLC
Immersion program
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Weight, lbs 55 189 86.5 392 55 183 87.5 373 0 -5.6 -2.9 <0.000
BMI 55 31.2 16.1 62.0 55 30.3 16.3 59.0 0 -0.9 -2.9 <0.000
Waist, inch 55 40.2 22.5 60 52 39.4 23 57.5 -3 -0.8 -1.9 <0.000
SBP 55 126 84 170 54 112 68 150 -1 -14 -11 <0.000
≥140 12 152 142 " 1 126 82 142 -11 -27 -18 <0.000
DBP 55 83 50 138 54 73 54 100 -1 -9.4 -11 <0.000
≥90 18 106 90 " 2 78 54 " -16 -28 -27 <0.000
Glucose† 55 106 62 365 55 96 67 162 0 -10 -10 0.015
≥126 10 173 131 " 3 121 86 " -7 -52 -30 0.014
Insulin 22 15.2 3.7 39 21 11.4 2.4 30.1 -1 -3.8 -25 0.010
HOMA-IR 22 4.51 1.05 14.8 21 3.0 0.5 11.0 -1 -1.5 -33 0.004
TChol† 55 195.8 109 296 55 170 93 253 0 -26 -13 <0.000
>220 17 245 221 " 3 198 166 " -14 -46 -19 <0.000
LDL† 54 109 51 221 54 93 36 182 0 -16 -15 <0.000
>120 18 148 121 " 5 116 89 " -13 -31 -21 <0.000
HDL*† 55 58 26 120 55 52 22 104 0 -5.6 -9.7 <0.000
TGL† 55 144 40 532 55 124 38 405 0 -20 -14 0.007
>150 20 235 152 " 12 163 67 " -8 -72 -31 0.002
hsCRP 55 2.02 0.04 95.0 54 1.41 0.01 91.2 -1 -0.6 -30 0.048
>3 12 4.71 3.05 8.81 11 2.65 0.53 6.12 -1 -2.1 -44 0.003
Beck 55 15 0 48 30 8 0 31 -25 -7.4 -49 <0.000
>19 20 29 20 " 2 9 0 " -18 -20 -69 <0.000
SF36* 43 58 13 90 43 72 29 95 0 15 25 <0.000
<75 32 38 " 75 21 68 29 95 -11 29 76 <0.000
Notes: * higher values are lower risk; † mg/dL
LM Clinic convenience
sample of 55 patients
in an 18-day ITLC
Immersion program

5/12/2021
19
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Weight, lbs 55 189 86.5 392 55 183 87.5 373 0 -5.6 -2.9 <0.000
BMI 55 31.2 16.1 62.0 55 30.3 16.3 59.0 0 -0.9 -2.9 <0.000
Waist, inch 55 40.2 22.5 60 52 39.4 23 57.5 -3 -0.8 -1.9 <0.000
SBP 55 126 84 170 54 112 68 150 -1 -14 -11 <0.000
≥140 12 152 142 " 1 126 82 142 -11 -27 -18 <0.000
DBP 55 83 50 138 54 73 54 100 -1 -9.4 -11 <0.000
≥90 18 106 90 " 2 78 54 " -16 -28 -27 <0.000
Glucose† 55 106 62 365 55 96 67 162 0 -10 -10 0.015
≥126 10 173 131 " 3 121 86 " -7 -52 -30 0.014
Insulin 22 15.2 3.7 39 21 11.4 2.4 30.1 -1 -3.8 -25 0.010
HOMA-IR 22 4.51 1.05 14.8 21 3.0 0.5 11.0 -1 -1.5 -33 0.004
TChol† 55 195.8 109 296 55 170 93 253 0 -26 -13 <0.000
>220 17 245 221 " 3 198 166 " -14 -46 -19 <0.000
LDL† 54 109 51 221 54 93 36 182 0 -16 -15 <0.000
>120 18 148 121 " 5 116 89 " -13 -31 -21 <0.000
HDL*† 55 58 26 120 55 52 22 104 0 -5.6 -9.7 <0.000
TGL† 55 144 40 532 55 124 38 405 0 -20 -14 0.007
>150 20 235 152 " 12 163 67 " -8 -72 -31 0.002
hsCRP 55 2.02 0.04 95.0 54 1.41 0.01 91.2 -1 -0.6 -30 0.048
>3 12 4.71 3.05 8.81 11 2.65 0.53 6.12 -1 -2.1 -44 0.003
Beck 55 15 0 48 30 8 0 31 -25 -7.4 -49 <0.000
>19 20 29 20 " 2 9 0 " -18 -20 -69 <0.000
SF36* 43 58 13 90 43 72 29 95 0 15 25 <0.000
<75 32 38 " 75 21 68 29 95 -11 29 76 <0.000
Notes: * higher values are lower risk; † mg/dL
LM Clinic convenience
sample of 55 patients
in an 18-day ITLC
Immersion program
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Weight, lbs 55 189 86.5 392 55 183 87.5 373 0 -5.6 -2.9 <0.000
BMI 55 31.2 16.1 62.0 55 30.3 16.3 59.0 0 -0.9 -2.9 <0.000
Waist, inch 55 40.2 22.5 60 52 39.4 23 57.5 -3 -0.8 -1.9 <0.000
SBP 55 126 84 170 54 112 68 150 -1 -14 -11 <0.000
≥140 12 152 142 " 1 126 82 142 -11 -27 -18 <0.000
DBP 55 83 50 138 54 73 54 100 -1 -9.4 -11 <0.000
≥90 18 106 90 " 2 78 54 " -16 -28 -27 <0.000
Glucose† 55 106 62 365 55 96 67 162 0 -10 -10 0.015
≥126 10 173 131 " 3 121 86 " -7 -52 -30 0.014
Insulin 22 15.2 3.7 39 21 11.4 2.4 30.1 -1 -3.8 -25 0.010
HOMA-IR 22 4.51 1.05 14.8 21 3.0 0.5 11.0 -1 -1.5 -33 0.004
TChol† 55 195.8 109 296 55 170 93 253 0 -26 -13 <0.000
>220 17 245 221 " 3 198 166 " -14 -46 -19 <0.000
LDL† 54 109 51 221 54 93 36 182 0 -16 -15 <0.000
>120 18 148 121 " 5 116 89 " -13 -31 -21 <0.000
HDL*† 55 58 26 120 55 52 22 104 0 -5.6 -9.7 <0.000
TGL† 55 144 40 532 55 124 38 405 0 -20 -14 0.007
>150 20 235 152 " 12 163 67 " -8 -72 -31 0.002
hsCRP 55 2.02 0.04 95.0 54 1.41 0.01 91.2 -1 -0.6 -30 0.048
>3 12 4.71 3.05 8.81 11 2.65 0.53 6.12 -1 -2.1 -44 0.003
Beck 55 15 0 48 30 8 0 31 -25 -7.4 -49 <0.000
>19 20 29 20 " 2 9 0 " -18 -20 -69 <0.000
SF36* 43 58 13 90 43 72 29 95 0 15 25 <0.000
<75 32 38 " 75 21 68 29 95 -11 29 76 <0.000
Notes: * higher values are lower risk; † mg/dL
LM Clinic convenience
sample of 55 patients
in an 18-day ITLC
Immersion program

5/12/2021
20
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Weight, lbs 55 189 86.5 392 55 183 87.5 373 0 -5.6 -2.9 <0.000
BMI 55 31.2 16.1 62.0 55 30.3 16.3 59.0 0 -0.9 -2.9 <0.000
Waist, inch 55 40.2 22.5 60 52 39.4 23 57.5 -3 -0.8 -1.9 <0.000
SBP 55 126 84 170 54 112 68 150 -1 -14 -11 <0.000
≥140 12 152 142 " 1 126 82 142 -11 -27 -18 <0.000
DBP 55 83 50 138 54 73 54 100 -1 -9.4 -11 <0.000
≥90 18 106 90 " 2 78 54 " -16 -28 -27 <0.000
Glucose† 55 106 62 365 55 96 67 162 0 -10 -10 0.015
≥126 10 173 131 " 3 121 86 " -7 -52 -30 0.014
Insulin 22 15.2 3.7 39 21 11.4 2.4 30.1 -1 -3.8 -25 0.010
HOMA-IR 22 4.51 1.05 14.8 21 3.0 0.5 11.0 -1 -1.5 -33 0.004
TChol† 55 195.8 109 296 55 170 93 253 0 -26 -13 <0.000
>220 17 245 221 " 3 198 166 " -14 -46 -19 <0.000
LDL† 54 109 51 221 54 93 36 182 0 -16 -15 <0.000
>120 18 148 121 " 5 116 89 " -13 -31 -21 <0.000
HDL*† 55 58 26 120 55 52 22 104 0 -5.6 -9.7 <0.000
TGL† 55 144 40 532 55 124 38 405 0 -20 -14 0.007
>150 20 235 152 " 12 163 67 " -8 -72 -31 0.002
hsCRP 55 2.02 0.04 95.0 54 1.41 0.01 91.2 -1 -0.6 -30 0.048
>3 12 4.71 3.05 8.81 11 2.65 0.53 6.12 -1 -2.1 -44 0.003
Beck 55 15 0 48 30 8 0 31 -25 -7.4 -49 <0.000
>19 20 29 20 " 2 9 0 " -18 -20 -69 <0.000
SF36* 43 58 13 90 43 72 29 95 0 15 25 <0.000
<75 32 38 " 75 21 68 29 95 -11 29 76 <0.000
Notes: * higher values are lower risk; † mg/dL
LM Clinic convenience
sample of 55 patients
in an 18-day ITLC
Immersion program
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Servings /week
Chol foods 41 18 0 84 5 3.6 0 10 -36 -14 -80 <0.000
High fat 42 17 0 67 20 4.7 0 10 -22 -12 -71 <0.000
Sweets 41 13 0 84 19 4.2 0 12 -22 -8.9 -68 <0.000
Sodas 19 2.8 0 10 2 2.0 0 3 -17 -0.8 -89 <0.000
Water*, cup /d 46 6.1 1 24 46 8.7 5 20 0 2.5 41 <0.000
Big suppers 19 0 -19 -100
No breakfast 15 2 -13 -87
Sleep <6hr 18 17 -1 -6
Exercise*, min 45 73 /wk 46 85 /d 1 440 605
Ex <30m /wk 19 15 1 15 /d -19 -100
Ex 30-90m /wk 10 60 30 60 /d -10 -100
Ex 1.5-3h /wk 7 135 14 135 /d -7 -100
Ex >3h /wk 6 240 1 240 /d -6 -100
Ex ≥30m /d 10 30 /d 45 87 /d 35 57 190
MetS 48 1.9 40 1.6 -8 -0.3 -15 0.031
≥3 16 9 -7 -44
≥4 7 3 -4 -57
5 0 0 0
Notes: * higher values are lower risk; † mg/dL

5/12/2021
21
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Servings /week
Chol foods 41 18 0 84 5 3.6 0 10 -36 -14 -80 <0.000
High fat 42 17 0 67 20 4.7 0 10 -22 -12 -71 <0.000
Sweets 41 13 0 84 19 4.2 0 12 -22 -8.9 -68 <0.000
Sodas 19 2.8 0 10 2 2.0 0 3 -17 -0.8 -89 <0.000
Water*, cup /d 46 6.1 1 24 46 8.7 5 20 0 2.5 41 <0.000
Big suppers 19 0 -19 -100
No breakfast 15 2 -13 -87
Sleep <6hr 18 17 -1 -6
Exercise*, min 45 73 /wk 46 85 /d 1 440 605
Ex <30m /wk 19 15 1 15 /d -19 -100
Ex 30-90m /wk 10 60 30 60 /d -10 -100
Ex 1.5-3h /wk 7 135 14 135 /d -7 -100
Ex >3h /wk 6 240 1 240 /d -6 -100
Ex ≥30m /d 10 30 /d 45 87 /d 35 57 190
MetS 48 1.9 40 1.6 -8 -0.3 -15 0.031
≥3 16 9 -7 -44
≥4 7 3 -4 -57
5 0 0 0
Notes: * higher values are lower risk; † mg/dL
Beginning Ending Difference
Item Count Mean Min Max Count Mean Min Max Count Mean % p-val
Servings /week
Chol foods 41 18 0 84 5 3.6 0 10 -36 -14 -80 <0.000
High fat 42 17 0 67 20 4.7 0 10 -22 -12 -71 <0.000
Sweets 41 13 0 84 19 4.2 0 12 -22 -8.9 -68 <0.000
Sodas 19 2.8 0 10 2 2.0 0 3 -17 -0.8 -89 <0.000
Water*, cup /d 46 6.1 1 24 46 8.7 5 20 0 2.5 41 <0.000
Big suppers 19 0 -19 -100
No breakfast 15 2 -13 -87
Sleep <6hr 18 17 -1 -6
Exercise*, min 45 73 /wk 46 85 /d 1 440 605
Ex <30m /wk 19 15 1 15 /d -19 -100
Ex 30-90m /wk 10 60 30 60 /d -10 -100
Ex 1.5-3h /wk 7 135 14 135 /d -7 -100
Ex >3h /wk 6 240 1 240 /d -6 -100
Ex ≥30m /d 10 30 /d 45 87 /d 35 57 190
MetS 48 1.9 40 1.6 -8 -0.3 -15 0.031
≥3 16 9 -7 -44
≥4 7 3 -4 -57
5 0 0 0
Notes: * higher values are lower risk; † mg/dL
5/12/2021
22
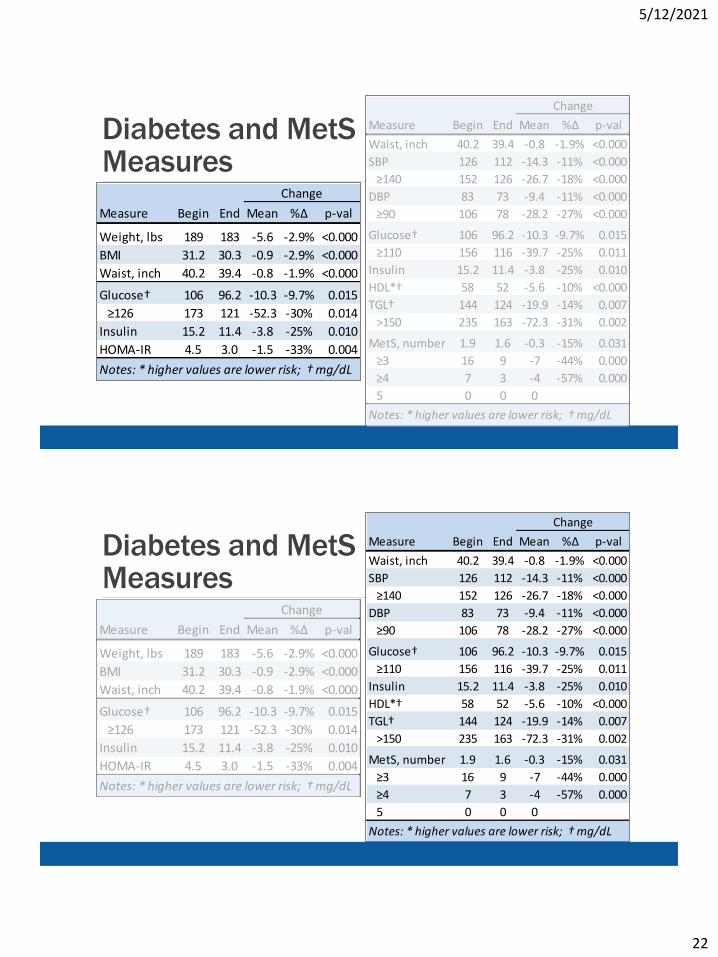
Diabetes and MetSMeasures
Measure Begin End Mean %Δ p-val
Weight, lbs 189 183 -5.6 -2.9% <0.000
BMI 31.2 30.3 -0.9 -2.9% <0.000
Waist, inch 40.2 39.4 -0.8 -1.9% <0.000
Glucose† 106 96.2 -10.3 -9.7% 0.015
≥126 173 121 -52.3 -30% 0.014
Insulin 15.2 11.4 -3.8 -25% 0.010
HOMA-IR 4.5 3.0 -1.5 -33% 0.004
Notes: * higher values are lower risk; † mg/dL
Change
Measure Begin End Mean %Δ p-val
Waist, inch 40.2 39.4 -0.8 -1.9% <0.000
SBP 126 112 -14.3 -11% <0.000
≥140 152 126 -26.7 -18% <0.000
DBP 83 73 -9.4 -11% <0.000
≥90 106 78 -28.2 -27% <0.000
Glucose† 106 96.2 -10.3 -9.7% 0.015
≥110 156 116 -39.7 -25% 0.011
Insulin 15.2 11.4 -3.8 -25% 0.010
HDL*† 58 52 -5.6 -10% <0.000
TGL† 144 124 -19.9 -14% 0.007
>150 235 163 -72.3 -31% 0.002
MetS, number 1.9 1.6 -0.3 -15% 0.031
≥3 16 9 -7 -44% 0.000
≥4 7 3 -4 -57% 0.000
5 0 0 0
Notes: * higher values are lower risk; † mg/dL
Change
Diabetes and MetSMeasures
Measure Begin End Mean %Δ p-val
Weight, lbs 189 183 -5.6 -2.9% <0.000
BMI 31.2 30.3 -0.9 -2.9% <0.000
Waist, inch 40.2 39.4 -0.8 -1.9% <0.000
Glucose† 106 96.2 -10.3 -9.7% 0.015
≥126 173 121 -52.3 -30% 0.014
Insulin 15.2 11.4 -3.8 -25% 0.010
HOMA-IR 4.5 3.0 -1.5 -33% 0.004
Notes: * higher values are lower risk; † mg/dL
Change
Measure Begin End Mean %Δ p-val
Waist, inch 40.2 39.4 -0.8 -1.9% <0.000
SBP 126 112 -14.3 -11% <0.000
≥140 152 126 -26.7 -18% <0.000
DBP 83 73 -9.4 -11% <0.000
≥90 106 78 -28.2 -27% <0.000
Glucose† 106 96.2 -10.3 -9.7% 0.015
≥110 156 116 -39.7 -25% 0.011
Insulin 15.2 11.4 -3.8 -25% 0.010
HDL*† 58 52 -5.6 -10% <0.000
TGL† 144 124 -19.9 -14% 0.007
>150 235 163 -72.3 -31% 0.002
MetS, number 1.9 1.6 -0.3 -15% 0.031
≥3 16 9 -7 -44% 0.000
≥4 7 3 -4 -57% 0.000
5 0 0 0
Notes: * higher values are lower risk; † mg/dL
Change

5/12/2021
23
Depression and Standard Function (QoL)
0
10
20
30
40
50
60
70
80
SF36 SF-36 <75 Beck Beck >19
Begin EndMeasure Begin End Mean %Δ p-val
Beck 15 8 -7 -49% <0.000
>19 29 9 -20 -69% <0.000
SF36* 58 72 15 25% <0.000
<75 38 68 29 76% <0.000
Notes: * higher values are lower risk; † mg/dL
Change
Clinical Remission/ Reversal• So… how can we best reduce calories, without losing nutrients?
• Reduce caloric density without dropping essential nutrients (health = nutrients / calories)
• Simplest way: greatly increase whole, unprocessed plant foods of color
• Plants high in nutrients, fiber and water, low in fats and calories

5/12/2021
24
Clinical Remission/ Reversal• Fills up stomach but with fewer calories (low calorie density)
• Michael Pollan’s 3 rules:
1. eat food - not ‘food-like’ substances (manufactured),
2. not too much,
3. mostly plants.
• Fasting-mimicking diet cycles (FMD)
• Intermittent fasting (routinely put body briefly in fasting state)
Summarize the ACLM Position Statement on Type 2 Diabetes Remission and Lifestyle Medicine

5/12/2021
25
Kelly J, Karlsen M, Steinke G. Type 2 Diabetes Remission and Lifestyle Medicine: A Position Statement From the American College of
Lifestyle Medicine. American Journal of Lifestyle Medicine. 2020;14(4):406-419. doi:10.1177/1559827620930962
CONCLUSION: As incidence of T2D continues
to rise, the current best evidence from multiple
intervention studies supports remission with
intensive lifestyle modifications as the prefer-
red treatment and standard of care. To
achieve remission, appropriate, therapeutic
dosing of lifestyle modifications is necessary,
including a hypocaloric diet.
Future research should focus on high-quality
intervention trials to further quantify the
potential of different lifestyle modifications,
including consumption of a whole-food plant
diet, to achieve remission of T2D in
comparison to standard pharmacologic
treatment and surgical interventions.
ACLM’s Position1. Sufficiently intensive lifestyle modifications are capable of producing
clinical improvements and/or remission in T2D patients.
2. The optimal treatment to bring about remission includes a whole food, plant-based (WFPB) dietary pattern, coupled with regular moderate exercise.
Therefore:
3. Remission should always be the preferred clinical goal, and lifestyle medicine interventions shown to produce remission should therefore become the standard of care.

5/12/2021
26
Appropriate Therapeutic Dosing
• Intensity of lifestyle interventions must be matched to the severity and acuteness of the condition being treated (just as with medication and surgery)
•Reversal of advanced hyperglycemia requires intensive lifestyle interventions that produce significant weight loss
•Counterpoint, Counterweight and DiRECT trials demonstrate that liquid meal substitutes can achieve this
Clinical Experience with Plant Diet
•ACLM members and others have shown that WFPB diets can also achieve remission, esp. combined with fasting
•The position paper reviewed multiple intervention studies and found that dosing intensity largely determines success or failure to achieve remission
•Research needed to compare meal substitutes with WFPB diet, and other diets and interventions

5/12/2021
27
Clinical Goal of T2D Remission
•Weight of evidence shows that properly-dosed lifestyle interventions can produce remission in a major portion of T2D patients
•Medication-based treatment alone is insufficient to achieve remission
•Surgical interventions can achieve remission, but with significant risk and undesired side-effects
Questions?

5/12/2021
28
Fasting-mimicking Diet•The FMD is a plant-based diet designed to attain fasting-like effects on the serum levels of IGF-1, IGFBP-1, glucose, and ketone bodies while providing both macro-and micronutrients to minimize the burden of fasting and adverse effects.
•Day 1 of the FMD supplies ~4600 kJ (11% protein, 46% fat, and 43% carbohydrate), whereas days 2 to 5 provide ~3000 kJ (9% protein, 44% fat, and 47% carbohydrate) per day.
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.
Fasting-mimicking Diet•The FMD comprises proprietary formulations belonging to USC and L-Nutra (www.prolonfmd.com) of vegetable-based soups, energy bars, energy drinks, chip snacks, tea, and a supplement providing high levels of minerals, vitamins, and essential fatty acids (fig. S4).
•All items to be consumed per day were individually boxed to allow the subjects to choose when to eat while avoiding accidentally consuming components of the following day.
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.

5/12/2021
29
Fasting-mimicking Diet Content• The human version of the FMD is a propriety (L-Nutra) plant-based diet designed to
attain fasting-like effects on the serum levels of IGF-I, IGFBP1, glucose and ketone bodies while providing both macro and micronutrients to minimize the burden of fasting and adverse effects (Brandhorst et al., 2015).
• Day 1 of the FMD supplies ~4600 kJ (1060 kcal; 11% protein, 46% fat, 43% carbohydrate), whereas days 2-5 provide ~3000 kJ (690 kcal; 9% protein, 44% fat, 47% carbohydrate) per day.
• The FMD comprises proprietary formulations of vegetable-based soups, energy bars, energy drinks, chip snacks, tea, and a supplement providing high levels of minerals, vitamins and essential fatty acids (Figure S3). All items to be consumed per day were individually boxed to allow the subjects to choose when to eat while avoiding accidentally consuming components of the following day. For the human subjects, a suggested FMD meal plan was provided that distributes the study foods to be consumed as breakfast, lunch, snacks, and dinner. See lists below for ingredients and supplements.
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.
Fasting-mimicking Diet Ingredients• Mushroom Soup: Rice flour, Carrot powder, Dried onion, Champignon
mushroom powder, Inulin (chicory fiber), Dried champignon mushroom, Salt, Yeast extract, Potato starch, Olive oil, Dried parsley, Natural flavor.
• Vegetable Soup: Rice flour, Dried onion, Inulin(chicory fiber), Dried tomato, Dried carrot, Salt, Dried red pepper, Dried leek, Potato starch, Olive oil, Freeze-dried basil, Spinach powder, Dried parsley, Natural flavor.
• Tomato Soup: Rice flour, Dried tomato powder, Dried onion, dried tomato pieces, dried carrot, chicory fiber, potato starch, olive oil, Salt, Yeast extract, Dried basil, Dried parsley, Natural flavor.
• Pumpkin Soup: Pumpkin powder, rice flour, inulin (chicory fiber), dried carrot, salt, yeast extract, potato starch, olive oil, dried onion, dried parsley, natural flavor.
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.

5/12/2021
30
Fasting-mimicking Diet Ingredients• Energy Bar: Almond meal, Macadamia nut butter, Honey, Pecan,
Coconut, Flaxseed meal, Coconut oil, Vanilla extract, Sea salt.
• Kale Crackers: kale, golden flax seeds, sunflower seeds, cashews, Sesame seeds, nutritional yeast, apple cider vinegar, hemp seeds, pumpkin seeds, sea salt, onion powder, dill week, black pepper.
• Algal Oil Capsule: Algal oil, Gelatin, Glycerin, Purified water, Turmeric, Annatto extract.
• Teas: chamomile, spearmint, or Lemon.
• Energy drink: Purified water, natural vegetable glycerin, polylysine.
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.
Fasting-mimicking Diet Supplements• Vitamin A (as Beta Carotene), Vitamin C (Ascorbic Acid), Vitamin D
(as Cholecalciferol), Vitamin E (as DL-Alpha Tocopherol Acetate), Vitamin K (as Phytonadione), Thiamine (as Thiamine Mononitrate), Riboflavin, Niacin (as Niacinamide), Vitamin B6 (as Pyridoxine HCI), Folic Acid, Vitamin B12 (as Cyanocobalamin), Biotin, Pantothenic Acid (as Calcium-D-Pantothenate), Calcium (as Calcium Carbonate and Tribasic Calcium Phosphate), Iron (as Ferrous Fumarate), Phosphorous (as Tribasic Calcium Phosphate), Iodine (as Potassium Iodine), Magnesium (as Magnesium Oxide), Zinc (Zinc Oxide), Selenium (as Sodium Selenate), Copper (as Cupric Sulfate), Manganese (as Manganese Sulfate), Chromium (as Chromium Picolinate), Molybdenum (as Sodium Molybdate).
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.

5/12/2021
31
Fasting mimicking Diet Supplements
•Proprietary Blend: Beet Root Powder, Spinach Leaf Powder, Tomato Fruit Powder, Carrot Root Powder, Collards Greens Powder, Collards (Kale) Leaf Powder. Other Ingredients: Stearic Acid, Microcrystalline Cellulose, Dicalcium Phosphate, Croscarmellose Sodium, Magnesium Stearate, Silicon Dioxide, Pharmaceutical Glaze.
Wei M, et al. Fasting-mimicking diet and markers/risk factors for aging, diabetes, cancer, and
cardiovascular disease. Sci Transl Med 2017 Feb 15;9:eaai8700.