






Languages
Pages
Legal


© 2006 The Authors Journal compilation © 2006 Blackwell Publishing Ltd.
Learning in Health and Social Care
,
5
, 2, 90–105
Original article
Blackwell Publishing Ltd
Re-generating the ‘self ’ in learning: developing a culture of supportive learning in practice
Valerie
Wilson
RSCN RN BEdSt. MN PhD
1
*
,
Brendan
McCormack
DPhil BSc Nursing PGCEA RGN RMN
2
& Glenice
Ives
PhD MEdSt. BAppSc (AdvNsg) DipAppSc (NsgEd) DHNWM RN
3
1
Director of Nursing Research and Practice Development, Nursing Research & Practice Development Unit, CHW School of Nursing, Monash University, Australia
2
Director of Nursing Research and Practice Development, University of Ulster at Jordanstown, Northern Ireland and Royal Hospital Trust, Belfast & School of Nursing, Monash University
3
Associate Professor of Nursing, School of Nursing, Monash University, Australia
Abstract
This article presents the findings of a project that focused on developing a culture of learning where practitioners were able to engage in supported work-based learning in a Special Care Nursery (SCN). The project was part of a larger study focusing on the implementation and evaluation of an emancipatory practice development programme in an SCN. The aim of this phase of the study was to gain an in-depth understanding of how the implementation of practice-development strategies could enable the creation of a culture of supportive learning in practice. The methodological and philosophical structure of the study was based on emancipatory practice development (ePD). The ePD strategies used are aimed at promoting the empowerment of nursing staff, utilizing staff knowledge and expertise to identify the need for change, encouraging reflection on and in practice, incorporating the views of service users in the change process, and supporting staff to challenge themselves and each other. Questions are framed to evaluate systematically the processes and outcomes of the study with a view to identifying changes in the learning culture that may have occurred as a result of PD strategies. Pre-intervention findings highlighted that tensions existed between what people espoused about learning and what actually occurred in practice. Through the use of PD processes, participants in the study began to focus on the learning environment. Key themes identified in the data included ‘learning about learning’, ‘movement from subservience to partnership’, movement from rituals to reflective questions’ and ‘movement from self-immersed to working with one another’. Taking self-responsibility for learning and ‘regenerating the self ’ in learning emerged as key issues underpinning these themes and are subthemes of ‘values and beliefs about learning’. It is argued that developing ‘responsible self ’ is key to the creation of a culture of learning where practitioners are able to develop mutually supportive relationships in order to learn in and from their practice. In conclusion, learning culture has a significant impact on how nurses go about their
Keywords
culture, learning,
nursing, practice
development
*Corresponding author. Tel.: +61 298453093; fax: +61 298451317; e-mail: [email protected]

Re-generating the ‘self ’ in learning 91
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
everyday practice. The implementation of PD processes enabled a cultural shift to occur. As a result of this, a supportive learning culture embedded within the workplace emerged. Learning about learning was seen as an important part of the context that
enabled the development of the responsible self.
Introduction
This article presents the findings of one component
of a research study focusing on the implementation
and evaluation of emancipatory practice development
(ePD) processes (Manley & McCormack 2003) in a
Special Care Nursery (SCN). The intent of ePD is to
increase effectiveness in patient-centred care through
enabling healthcare teams to transform the culture
and context of care (Garbett & McCormack 2002).
Reflective learning processes are central to an ePD
approach. Reflective processes are integrated with
other developmental processes and thus achieving
practice development is enabled through the changes
in the perspectives of individual practitioners to
recognize the need for change. Thus, unlike technical
approaches to practice development where learning
is a consequence of the work, in ePD, learning is
integrated with development activities and is a
primary intended outcome of development activities
(Manley & McCormack 2003). A study of the culture
was initially undertaken to evaluate, in a critical
manner, changes that may take place in the SCN as
a result of the implementation. These findings
have previously been reported (Wilson
et al
. 2005).
The present article presents the postintervention
findings related to the learning culture of the SCN
and draws upon findings of the previous work.
Learning culture
Learning is a process by which we gain knowledge
and proficiency (Knowles, Holton & Swanson 1998).
It is personally meaningful, makes sense of our
experiences and leads to changes in behaviour
(Knapper & Croppley 1999). However, sustained
learning only occurs within contexts that are
supportive and where learning is viewed as important
(Senge 1990). Thus, workplace culture and learning
culture are closely intertwined. An investment in
grass roots learning can influence cultural change
(Platzer
et al
. 2000; Clark 2001) and develop an
exciting workplace environment, where challenge is
part of everyday practice (Titchen & Binnie 1995;
Kaye & Jordan-Evans 2000) and learning extends
beyond the boundaries of the clinical unit (Platzer
et al
. 2000).
The key goal in the development of a positive
learning culture is to recognize and overcome
individual, group and organizational barriers (Hoff
et al
. 2004). Such barriers include the need to ‘fit in’
and ‘learn the rules’ of the workplace (Melia 1987;
Nolan 1998); inadequate facilitation and challenge
(Miller
et al
. 1994); practitioners who own routines
and rituals rather than embrace the notion of
reflection in practice (Johns 1994); team members
who dominate or disparage each other (Wade 1994);
and a perceived lack of self worth (Miller
et al
. 1994).
Establishing a positive learning culture is both
complex and challenging, but Dixon (1999) and
Ward & McCormack (2000) suggest that it can be
created through the implementation of strategies
which develop challenge, openness, debate and a
more supportive environment.
Aim
The aim of this phase of the study was to gain an
in-depth understanding of how the implementation
of practice development strategies could enable
the creation of a culture of supportive learning in
practice.
Methodology
The methodological and philosophical structure
of the study was based on ePD. The ePD strategies
used are aimed at promoting the empowerment of

92 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
nursing staff, utilizing staff knowledge and expertise
to identify the need for change, encouraging reflection
on and in practice, incorporating the views of
service users in the change process, and supporting
staff to challenge themselves and each other. This
work was supported by facilitators using systematic
and rigorous approaches to change (Garbett &
McCormack 2002). As the name ePD suggests, it
obviously focuses on the emancipatory intent of
developing clinical practice. It is not good enough
merely to impose a change on clinical practice;
the emancipatory function of ePD is linked to
transformative action and, in turn, to transforming
the culture in which practice takes place. This
approach is based on the theory of critical social
science, which is underpinned by the process of
enlightenment, empowerment and emancipation
(Fay 1987).
Principles of professional learning underpinned
the activities as this fitted with the philosophical and
methodological intent of the overall ePD study. The
adoption of these principles enabled participants
to choose from a ‘menu’ of learning activities that
constituted the ‘education intervention’. The menu
consisted of items such as action learning, high
challenge with high support, a variety of workshops,
teamwork development, journal club and one-to-
one clinical support. By offering a menu such as this,
the study worked with the principle of respecting
individual learning styles, whilst focusing the evalu-
ation on the effectiveness of the overarching educa-
tion intervention, as it was hypothesized (through
the stated aim) that the implementation of ePD
activities based on individual learning choices would
enable the development of a learning culture. Thus,
the effectiveness of the individual learning activities
was not the focus of the study (although information
about these has been collected).
Context
The study reported here was set in an SCN that
provided level two services for unwell newly born
infants and their families (referred to as ‘neonatal
nursing’). This was a funded study based on changing
nursing practice and therefore the key participants
were nurses, although other staff, such as doctors,
allied health and clerical staff, did participate in
some aspects of the study. Thirty nursing staff
participated in the study, the majority of whom were
both registered nurses and midwives. All staff were
women and the length of neonatal nursing experience
ranged from a few months (newly recruited experienced
nurses who had not worked with neonates before) to
> 25 years. The unit provided a 4-month placement for
one new graduate nurse and occasionally had either
an undergraduate or a postgraduate student. The
nurse unit manager started in her post 2 months
prior to the study, and one of her five associate unit
managers, or nurse leaders, was in charge of each
shift. Nurse educators worked with staff on the unit
for two half-days per week. The staff-patient ratio
was one to three.
The practitioner-researcher
McCormack & Garbett (2003) suggest that ‘credibility’
of practitioner-researchers is a key factor in the
success or otherwise of practice development projects.
The lead practitioner-researcher had not worked
with staff in the SCN before. However, as an
experienced childrens’ nurse and educator, the lead
practitioner-researcher had both ‘practice’ and
‘facilitation’ credibility amongst nursing staff. This
enabled engagement with staff whilst simultaneously
knowing the boundaries of such interactions in
research practice. The practitioner-researcher worked
with staff in the SCN for 1 day per week during the
lifetime of the study.
Participants
The study site self-selected for inclusion into the
study when a request for volunteers was circulated
within the healthcare organization. After the initial
agreement with the unit manager, information
sessions were held with nursing staff in order to
inform them about the study, clarify any queries
they had, outline the voluntary nature of the
study and to ensure they were happy to proceed.
The sample included all nursing staff. Process
consent was undertaken, whereby the practitioner-
researcher negotiated consent at each new stage
of the study (Dewing 2002). Ethical approval
Re-generating the ‘self ’ in learning 93
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
was obtained from the local research ethics
committees of the healthcare organization and the
University.
Data collection and analysis
To evaluate, in a systematic manner, the processes
and outcomes of the study, several approaches to
data collection were undertaken, including:
• a nursing staff survey taken prior to implementa-
tion of ePD activities;
• participant observation (PO) pre- and post-
implementation of ePD activities;
• field notes taken during the practitioner-researcher’s
clinical time on the unit; and
• interviews with nursing staff pre- and post-
implementation of ePD activities.
This multimethod approach provided the
opportunity to use differing sources of evidence to
assist with creating a more meaningful and deeper
understanding of the changing context on the unit
from a variety of perspectives and enhanced the
credibility of the findings (Patton 1990). Cognitive
mapping was used to manage and analyse data, and
is defined by Eden
et al
. (1983, p. 39) as a ‘modelling
technique which intends to portray ideas, beliefs,
values and attitudes and their relationship to one
another in a form which is amenable to study and
analysis’. Thematic analysis was utilized in the process
of map formation and refinement (Boyatzis 1998).
An independent researcher examined the labels and
refinement of themes to enhance credibility.
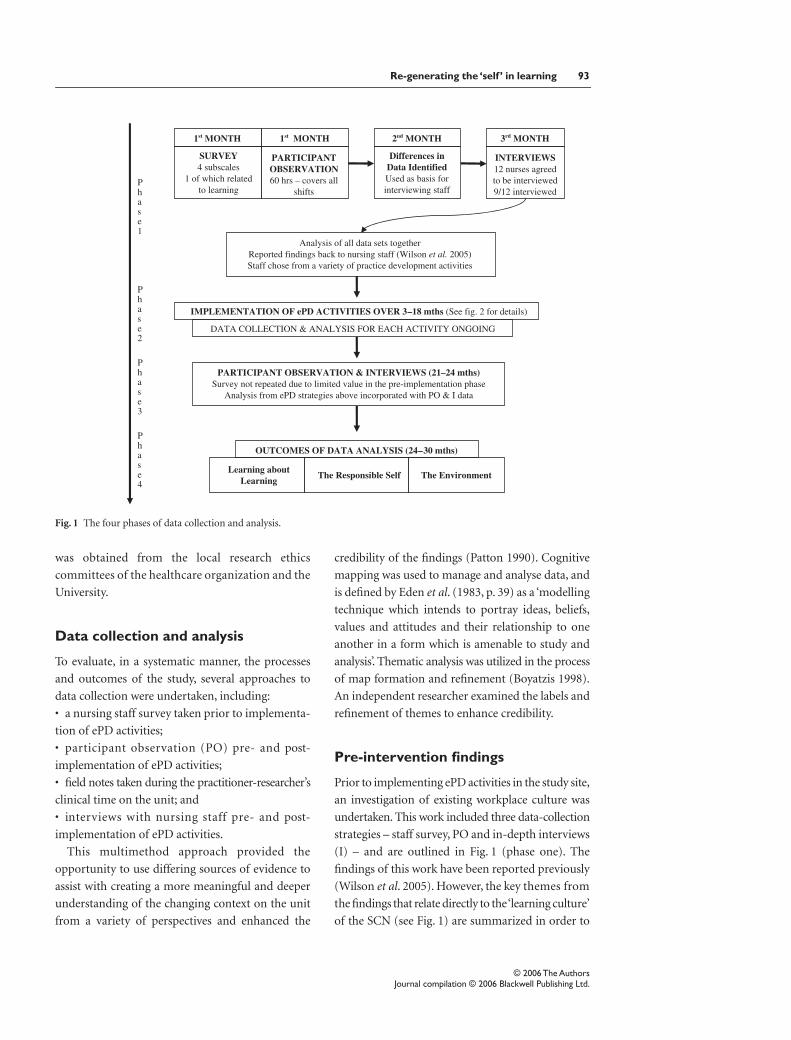
Pre-intervention findings
Prior to implementing ePD activities in the study site,
an investigation of existing workplace culture was
undertaken. This work included three data-collection
strategies – staff survey, PO and in-depth interviews
(I) – and are outlined in Fig. 1 (phase one). The
findings of this work have been reported previously
(Wilson
et al
. 2005). However, the key themes from
the findings that relate directly to the ‘learning culture’
of the SCN (see Fig. 1) are summarized in order to
Fig. 1 The four phases of data collection and analysis.

94 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
form the basis of this article. The term ‘staff ’ in this
article refers to nursing staff, unless otherwise stated.
Consistently, the findings uncovered contradictions
and tensions that were evident in everyday practice
and which created a distorted view of how learning
was being managed within the SCN. The survey
findings which related to learning (see Table 1)
suggested that the team believed that they were
highly skilled, had ample opportunity to learn and
were able to access information that would inform
their practice. However, this existed alongside other
opinions, which suggested that not all staff felt that
their learning requirements were being met.
This notion of tension was made more explicit in
the analysis of the observation data. Taking what
appeared to be differing views, these were explored
through individual interviews with staff members.
What emerged was a clearer picture of the tensions
that existed within individuals and the team in rela-
tion to learning in and from practice. Tensions were
both interpersonal and intrapersonal in nature and
this created confusion and inconsistency within the
learning environment. Three themes (partnership
vs. subservience, questioning vs. rituals, and team
vs. self-focused) were developed from the pre-
intervention data which illustrate the tensions that
existed for staff. An example of how these tensions
played out in practice can be found in Table 2 and
have been reported in greater detail previously
(Wilson
et al
. 2005).
Table 1 Survey results (learning subscale) pre-intervention
Learning in practice Mean Inference
1. Utilizing nursing skills effectively 3.37 1. Staff believe that they are highly skilled and use skills effectively
2. I regularly attend
in-service/short courses
3.16 2. Key elements of structural empowerment, such as access to
information, resources and support, as well as opportunities to learn
(Laschinger et al. 2001; Almost & Laschinger 2002) are evident
from the survey findings
3. Opportunity to attend courses regularly 3.16
4. Access to information
to inform practice
2.79 3. Less positive scores, with not all staff feeling that their learning
requirements are met within the existing culture
5. In-service meeting staff needs 2.53a
The survey was sent to all staff (n = 27). However, during the survey collection period, a number of staff were absent from the
unit and did not complete the survey on time. The survey return was 19/27–70%. Higher mean scores are indicative of greater
satisfaction; scores of > 3 indicate a positive response, and scores of < 3 contain a mixed result but tend towards more positive
responses.aThe score included ≈ 50% positive/50% negative responses.
Table 2 Overview of the pre-intervention findings
Partnership TENSIONS Subservience
I am now finding they (consultants)
are listening to me and asking for my input
Nurses are not valued for their input,
and have little involvement in the decision-making process
Questioning Rituals
I am trying to challenge practice, challenging
staff approaches to care in a non-threatening way
Keeping to the schedule, straight into tasks,
always done this way, do my chores
Team focused Self-focused
Sharing information and challenging
one another, that’s refreshing
Fear of new staff, disequilibrium,
having to begin a teaching role
Re-generating the ‘self ’ in learning 95
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
The learning culture was underpinned by existing
tensions that restricted the effectiveness of work-
place learning and ensured that little sustainable
work was undertaken to change the workplace cul-
ture. Indeed, although there was significant evid-
ence of people engaging in learning activities, there
was little evidence to suggest that this learning was
shared with others or was impacting on the delivery
of care. There appeared to be an over-reliance on ritu-
alistic practice, with little evidence of nursing staff
challenging their own practice or indeed that of
members of the multidisciplinary team. Exploring
the learning culture enabled staff to identify what
was happening in practice and to develop a set of
values and beliefs related to what they believed
the learning culture should be. These were framed
around three central themes of the learning
environment, person-centred learning and the
process of learning.
Education intervention
With the initial data collection and analysis
complete, the intervention phase of the study began.
One strand of the overall ePD programme of work
was a specific project that focused on developing a
culture of learning in the SCN as a means of sustaining
long-term changes in practice. Elsewhere, it has been
argued that creating an effective learning culture is
crucial to the long-term sustainability of practice
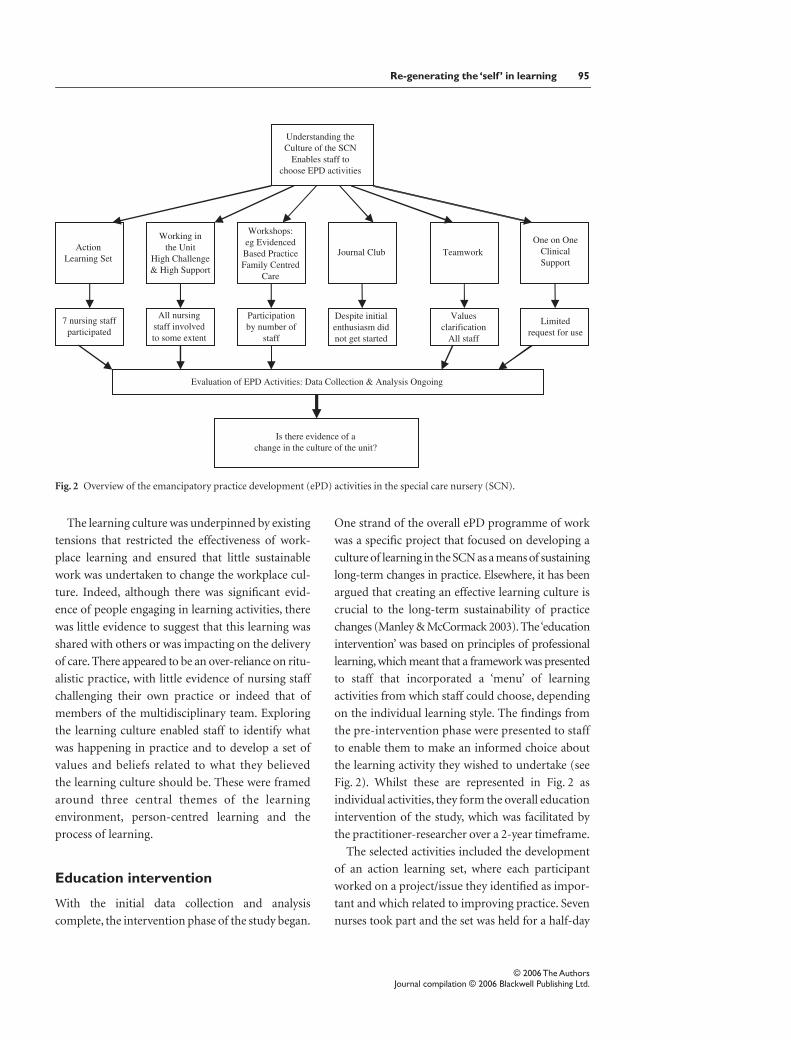
changes (Manley & McCormack 2003). The ‘education
intervention’ was based on principles of professional
learning, which meant that a framework was presented
to staff that incorporated a ‘menu’ of learning
activities from which staff could choose, depending
on the individual learning style. The findings from
the pre-intervention phase were presented to staff
to enable them to make an informed choice about
the learning activity they wished to undertake (see
Fig. 2). Whilst these are represented in Fig. 2 as
individual activities, they form the overall education
intervention of the study, which was facilitated by
the practitioner-researcher over a 2-year timeframe.
The selected activities included the development
of an action learning set, where each participant
worked on a project/issue they identified as impor-
tant and which related to improving practice. Seven
nurses took part and the set was held for a half-day
Fig. 2 Overview of the emancipatory practice development (ePD) activities in the special care nursery (SCN).

96 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
each month over 15 months. The practitioner-
researcher facilitated the set using the principles
outlined by McGill & Beaty (2001). Participants
were encouraged to involve other nurses in the work
they were undertaking. In addition, staff participated
in workshops held at various times throughout the
intervention period, which focused on factors such
as evidence-based practice and family-centred care.
All staff (including medical, nursing allied health
and clerical staff) participated in a values clarification
activity aimed at developing effective teamwork.
This was undertaken over a 2-month period at
the beginning of the study and included a series
of workshops, as well as individual work.
Another activity was the use of high challenge/
high support (hc/hs) where the practitioner-
researcher spent 1 day per week, for the duration
of the study, working alongside all nursing staff, chal-
lenging their everyday assumptions about practice
and supporting them to look at the effectiveness of
practice and the provision of family-centred care.
The model of hc/hs used in this study was adapted
from the clinical supervision strategies described
by Titchen & Binnie (1995), which are aimed at
helping nurses to think more deeply, enabling them
to share their experiences, as well as learning from
one another through working together. The
practitioner-researcher fosters a climate of critical
intent through reflective discussion and challenge to
increase nurses’ awareness about what is happening
around them and to question the subconscious acts
of everyday practice, in other words a process of
enlightenment (Grundy 1982). When this process
is focused on empowered practice, the resultant
heightened awareness enables the development of
expertise (Rolfe 1996). Learning about self through
enhanced self-awareness is an essential part of reflec-
tion (Atkins & Murphy 1993; Freshwater 1998) and
is probably one of the most challenging aspects of
this way of working. When processes to encourage
learning about self are used, the necessary high
challenge must be accompanied by high support
(Johns 1998). Working in this way enabled the
practitioner-researcher to establish credibility in a
much stronger and more personal way than could
be achieved by previous reputation. Further details
of each activity are presented in Table 3.
Findings postintervention
Acknowledging that tensions existed before any
practice development work commenced, the themes
identified in the pre-intervention phase (partner-
ship vs. subservience; questioning vs. rituals; team
focused vs. self-focused), as well as a new theme
(values and beliefs about learning), were used to
frame the outcomes arising from the education
intervention.
Partnership vs. subservience
Previously, some nursing staff working in the SCN
were striving for a partnership with medical staff,
especially senior medical staff. However, tensions
existed and some staff were happier for the status quo
to remain and to act in a subservient role to ensure
that they did not ‘rock the boat’. One of the greatest
challenges for nurses was their role during clinical
rounds. Previously, they had strived to be part of the
decision-making process, but often felt that their ideas
were not acknowledged or asked for. The culture had
begun to change during the ePD project as staff engaged
in activities such as high challenge-high support
and establishing effective teamwork. This resulted
in nurses learning to challenge doctors more often;
they were less willing to assume a subservient role
and were supported (by nurse leaders) to speak up
during clinical rounds. Doctors now actively
sought nurses’ input and considered what they said
as part of the decision-making process. The change
in how the clinical rounds were conducted illustrates
the development of nursing staff themselves and
the relationship that they had begun to foster with
medical staff:
I think there has been a significant change actually, rather than just being told … I think it is more of one where we are more in partnership and contributing more than we ever have.
The move was then one of prevailing over sub-
servience and developing partnerships.

Re-generating the ‘self ’ in learning 97
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
Table 3
Post-intervention findings
ePD activity Involvement by staff Achievements Impact factor
Working in the unit: high
challenge/high support, one day
per week spent working alongside
nursing staff, challenging their
everyday assumptions about
practice and supporting them to
look at the effectiveness of practice
and the provision of family-
centred care
All nursing staff involved,
with a flow-on effect to
other staff within the SCN
(e.g. medical staff)
This was undertaken
during normal working
hours
Babies are recognized as
unique individuals
Development of a
supportive environment
Introduction of care that
is developmentally
appropriate
Increased awareness of
how language and
behaviour impacts on care
Increase in problem solving
and critical thinking
Family-centred care
drives nursing practice
Nursing staff now pro-
active in changes in the unit
Nurses participate in
decision making about care
Creation of an
environment that
supports the baby, the
family and staff
Emphasis on providing
developmental care
Families made to feel
welcome and encouraged
to participate in their
baby’s care
Nursing staff eager to
suggest potential changes
for improving practice
Nurses less subservient
and now act as advocates
Action learning set
Staff worked on issues related to
improving practice [see
Wilson
et al
. (2003) for details]
Seven nurses participated
half a day, meeting once a
month for 15 months.
Time funded by the unit
budget
Various achievements
based on the work of
participants, (e.g. change
from ritualistic nursing
handover to using a multi-
disciplinary database)
Multi-disciplinary
communication improved
in the unit.
Developed template for
changing practice
Workshops: evidence-based
practice 2 h over 4–5-week period
Around five staff
participated in the
workshops
Developed skills is
searching for evidence,
reviewing research
literature and using
evidence in practice
Use of evidence to inform
staff and to base practice
changes such as ‘reducing
noise levels in the nursery’
Workshop: family-centred care
Full day workshop
Seven staff participated in
the workshop
Staff clearer about the
barriers to FCC as well as
the difference between
what we say we do and
what we actually do in
practice
FCC becomes the
authentic philosophy that
drives care
Teamwork: values clarification
over a 2-month period.
Included workshops and
individual work
All staff (including
medical, nursing allied
health and clerical staff) in
the unit involved
Developed a shared vision
for teamwork. Worked
towards realizing vision
in practice.
See Wilson (2005b) for
further details
Improved teamwork, staff
morale, sense of
collegiality and
multidisciplinary
communication
One on one clinical support over
18 months
Limited use by a few
nursing staff
Staff feel challenged and
supported by the
facilitator
Individual staff take on
new challenges
Journal club Not established Nil Nil
ePD, emancipatory practice development; FCC, family-centred care; SCN, Special Care Nursery.

98 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
Questioning vs. rituals
The tension that existed in the unit between ritual-
centred care and questioning practice resulted in
staff pulling in differing directions and care being
delivered in an inconsistent way. Nursing staff
worked hard on this as they undertook learning in
facilitated workshops, through hc/hs and teamwork
activities, as well as through the action learning
process. The dominant ritualistic approach to practice
changed as nurses reflected on their own practice
and questioned each other about the ways in which
they delivered care. This resulted in a heightened
awareness about everyday practice, a reduction of
rituals and an increased use of evidence, as most
staff moved towards a more patient-centred mode
of delivery. That being said, there were still a few
staff who remained loyal to inappropriate rituals
and were unable or unwilling to change their
practice. This, however, had little influence on the
dominant culture, where critical inquiry was not
only encouraged but expected, thereby reducing
rituals and increasing reflective questioning:
I think now with that challenge … people need to have a reasoning … with the challenge and thinking more about what we are doing, people will think ‘why did I do that?’ or ‘why am I doing this?
Team focused vs. self-focused
In the pre-intervention findings, learning was seen
as central to the evolving development of each staff
member and the unit as a whole. However, tensions
did exist between the needs of the individual learner
and the constant demand of teaching newly recruited
nursing and medical staff. This resulted in some staff
not engaging in learning at all, or learning only for
themselves where they were unwilling or unable to
take on a team learning role. Over the 2-year inter-
vention period, nursing and medical staff worked
more closely together (through team activities), which
ensured that the underlying tensions were reduced.
This resulted in them actively questioning one another
as they supported one another to learn. As they engaged
in more hands-on teaching (especially with new and
junior members of staff), they gained confidence in
their knowledge and skills, had greater questioning
ability and improved support and learning for all
staff within the SCN. This shifted the focus from
learning only for self onto working with one another:
… you feel that you have to know what you are doing and be confident with what you are doing … we have got junior nurses coming in to join the team, which is fantastic, I have to be there to be confident enough to support them, therefore they can trust me with what they are doing.
Table 4 Overview of the post-intervention findings
Prevailing over subservience TRANSITIONAL Developing partnerships
‘Learning now to challenge the doctors … we
have never done that before.
I’d have rolled out the red carpet, I would have
ages ago, not so much now’
I think there has been a significant change actually,
rather than just being told … we are more in partnership
and contributing more than we ever have
Reducing rituals Reflective questioning
There is still ‘a select few’ that are ‘ritualistic or
task orientated, not that they don’t listen … but
they don’t put it into practice’
A lot of the staff that were probably fixed at the start are
now questioning more what they are doing
Self-immersed Working with
There are some ho hum people that come to work,
do their work and go home
Everyone will work with you and help you … most
people are accessible … supported

Re-generating the ‘self ’ in learning 99
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
For a few staff there still appeared to be a level of
disengagement as they kept to themselves. The
emphasis on being self-immersed was, however,
less evident with the strong move towards working
collaboratively.
In reviewing a summary of each aspect of these
findings (see Table 4), it can be seen that the unit
worked through a transitional phase whereby sig-
nificant changes occurred and development was an
ongoing process. These findings were greatly influ-
enced by the values and beliefs about learning held
by nurses.
Values and beliefs about learning
The theme of ‘values and beliefs about learning’
is articulated through the three subthemes of, ‘the
learning environment’, ‘learning about learning’
and ‘the responsible self ’. These themes were
explored and verified with staff at the completion
of the study. The practitioner-researcher worked
closely with the nurse manager and nurse educators
to develop their knowledge and skills about
practice development and to ensure that a con-
sistent approach to the education intervention was
adopted.
The learning environment
Whilst there have always been elements of the
requirements for structural empowerment (see Table 1)
within the SCN, such as access to education and
resources, these had not necessarily been utilized
effectively in the past. Staff could now be seen actively
to use educational opportunities and resources
to inform their learning, such as surfing the ‘net’,
engaging in clinical discussions and attending
tutorials. The unit had transformed into an active
learning environment:
… there is a lot of education which I think is really good. A lot more than I have had in any of the other wards.
Learning was seen as a fundamental component
of everyday work, and this was supported by en-
gagement in activities such as exploring the use of
evidence in practice.
The manager played a pivotal role in actively
supporting staff, ensuring that they had the oppor-
tunity and time to learn, which they were really
enthused by. This resulted in staff undertaking
specialist courses provided by another hospital:
It seemed that half the staff were there, which shows me that they want to learn more … it wasn’t just people who were new to the unit either.
Staff actively discussed their learning from courses
they attended and questioned one another in order
to deepen their learning. Supporting one another to
learn is an important aspect of the learning culture
and was conducive to positive learning experiences.
This was achieved in part by providing an environment
where learning was about challenge with support
and not about constructing negative judgements:
… a lot of them will ask questions they know they are not going to be put down if they don’t know something … I think that it is a fairly supportive environment for learning.
This level of support also ensured most people
enjoyed learning, it was ‘fun and enjoyable’ and
ensured staff connected with learning activities. The
learning environment was evolving and developing
and whilst progress had been made, staff indicated
the need for continuous improvement:
I think we have come a long way, it’s positive … there is still lots we need to do and there will always be lots we need to do.
Learning about learning
In exploring their values and beliefs about learning,
staff in phase one were able to identify processes
that may enable them to learn within the context of
the SCN. Over the 2-year intervention period, they
were able to adopt some of these activities, such as

100 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
up-skilling programs, benchmarking and problem-
based learning packages, as they engaged in active
learning. Staff recognized and utilized different ways
of learning, which ranged from reading articles to
reflection on learning, as well as learning through
observation:
I am learning by observation and after I maybe read something … it is good to do both theory and practice together.
It was also important to utilize learning opportu-
nities when they arose, even though these might
be in a stressful situation with a very sick baby. Staff
were still able, ‘to learn, to observe, to listen’.
The staff in the unit themselves were a very
important component of the learning experience
and individuals were identified as preceptors, role
models and mentors. They provided appropriate
information in a systematic way, facilitated learning
experiences and modelled practice behaviours:
I try to copy them … I sort of go to them, and at a distance observing them.
The unit manager again played a pivotal role in
learning. She was a respected team leader and was
perceived to be a role model and mentor because of
her expertise and knowledge.
One area that was identified as not being used
effectively was giving and receiving feedback, which
staff found difficult and suggested that it was
probably one of the areas of which people were most
afraid. This was compounded when feedback was
not well received. This not only presented additional
challenges for effective workplace learning, but also
created personal challenge for the individual:
… some people will be able to give feedback quite easily because the person will accept that and maybe appreciate that, but the person who takes it the wrong way or is quite difficult … probably need it the most and that’s the people that don’t get it.
Staff, however, did recognize this and were trying
to improve this aspect of the learning culture to
ensure that feedback was viewed as non-threatening
and became part of everyday practice.
The responsible self
For a few staff a tension remained in the unit
between learning for self and feeling obliged to
‘keep up to date’. Whilst they were encouraged to
participate in choices about their own learning,
some staff did not want to take ownership and
responsibility for this and thought it was ‘their
given right that someone do it for them’. This
proved to be an ongoing challenge for education
and, in particular, the practitioner-researcher and
educators in the unit who tried to engage all staff
in active learning. The majority of staff however,
did take on responsibility for their own learning,
were open to suggestions for self development and
actively engaged in learning activities they chose to
suit their needs:
I enjoy the learning I choose, I don’t just go and do something because I feel I have to … we have all got different expertise or a different interest.
The notion of ‘knowing self ’ was reflected in
those staff (the majority) who developed an
understanding of their limitations and wanted to
further develop themselves. Others (the minority)
had little insight or were afraid to admit their
limitations, which resulted in them defending their
practice expertise to ensure that they were not
thought to be lacking in skills or knowledge. This
was considered to be unsafe practice and was
being increasingly challenged in the unit. Never-
theless, it was encouraging to note that in general,
staff were willing to be more honest in their
approach to knowing self, to admit when they
didn’t know something and to use opportunities to
think things through, develop knowledge and skills,
build their confidence and gain understanding.
They were able to use this sense of knowing to teach
others:

Re-generating the ‘self ’ in learning 101
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
I can teach them, give them knowledge of what I have gained. It was also the acknowledgement that the importance of learning was something that needed to be prioritized and not lost in the rush of everyday practice: I suppose for me it’s not forgetting that I need to … keep on learning and developing.
Learning did indeed become integral to everyday
practice and was used as a basis to improve care.
Learning was continuous and improved staff
satisfaction with work and with self. Whilst learning
could be seen as a challenge, it was the individuals’
commitment to lifelong learning that created the
greatest influence to the learning culture of the unit
and ensured that for the majority of staff learning
became part of the
responsible self
:
I always feel I’m going to be challenged intellectually because there is no way I would ever say I know everything in this place you are going to learn something new everyday, every baby is different … If you said you knew everything you are going to have to quit your job.
Outcomes
The nature of ePD work and the fact that a number
of activities were used in the unit simultaneously
impacts on the ability to attribute outcomes to
specific activities. Indeed, outcomes are strengthened
by the cumulative nature of the work undertaken and
the interactions between activities. However, Table 3
illustrates each ePD activity, the involvement of staff,
and the potential links between the achievements
to date and the related impact of the initiatives.
Evidence for these achievements have been sourced
from the data collected in the overall study, including
participant observation, action learning data, focus
group and individual interviews. A discussion of each
of these findings is beyond the scope of this article,
but they are discussed in detail in Wilson (2005a).
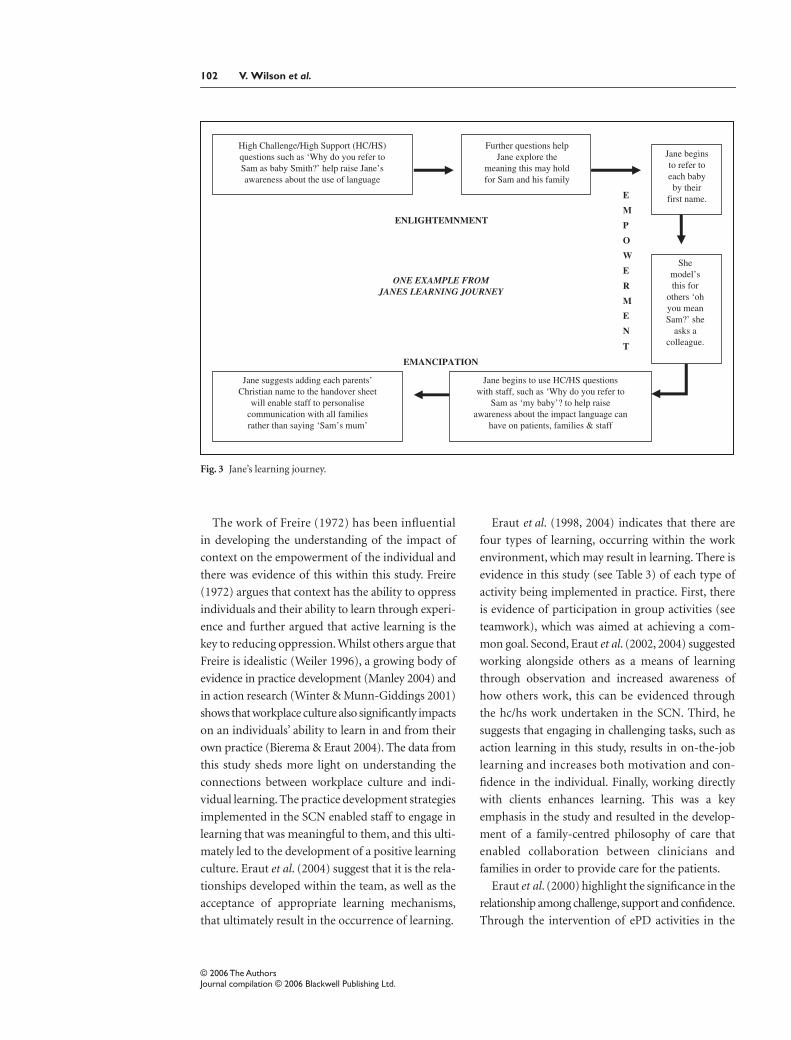
The postintervention findings relate to the overall
outcomes for the SCN and within that contain the
experiences of the individual. In order to illustrate
how this is manifested for the individual, Fig. 3
highlights an example from the journey of one nurse
as she engaged in one of the education mechanisms
adopted in the unit. Within this journey, Jane moves
through the stages of enlightenment as she becomes
aware of ‘self ’ within the practice context and how
this impacts upon the delivery of care. Jane then acts
as a positive role model within the SCN as she is
empowered to adopt new behaviours. The final
stage of emancipation occurs as Jane challenges
others (using the hc/hs intervention) to look at their
practice, and she, in turn, develops new initiatives,
which support her new way of working.
Discussion
There was little evidence in this study of the
underlying assumptions associated with an adult
learning approach, such as being self-directed; a
readiness to learn, using accumulated experience
as a resource for learning; and adopting a problem-
centred approach to learning (Knowles 1977).
Clinicians seemed to be switched off from adult
learning principles and were reliant instead on
education being available for consumption, if and
when they desired it, rather than something in
which they actively engaged or necessarily wanted.
This may have been influenced by their previous
experience as learners, which embraced a more
pedagogical approach and a teacher-centred model
of education, whereby they expected, and at times
demanded, that others take responsibility for their
learning. This is consistent with other studies, such
as those of Platzer
et al
. (2000), who identified the
challenges associated with engendering a sense of
self-responsibility for learning amongst adult learners.
With this challenge in mind, the findings from this
study would suggest that re-engaging clinicians with
the concepts of an andragogical approach, such as
uncovering their internal desire to learn, and
creating learning opportunities that were relevant
to everyday practice, are important mechanisms in
enabling the discovery of self within the learning
context (Knowles, Holton & Swanson 1998). Context
is increasingly seen as the key factor in influencing
the development of practice (Rycroft-Malone 2004).
102 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
The work of Freire (1972) has been influential
in developing the understanding of the impact of
context on the empowerment of the individual and
there was evidence of this within this study. Freire
(1972) argues that context has the ability to oppress
individuals and their ability to learn through experi-
ence and further argued that active learning is the
key to reducing oppression. Whilst others argue that
Freire is idealistic (Weiler 1996), a growing body of
evidence in practice development (Manley 2004) and
in action research (Winter & Munn-Giddings 2001)
shows that workplace culture also significantly impacts
on an individuals’ ability to learn in and from their
own practice (Bierema & Eraut 2004). The data from
this study sheds more light on understanding the
connections between workplace culture and indi-
vidual learning. The practice development strategies
implemented in the SCN enabled staff to engage in
learning that was meaningful to them, and this ulti-
mately led to the development of a positive learning
culture. Eraut
et al
. (2004) suggest that it is the rela-
tionships developed within the team, as well as the
acceptance of appropriate learning mechanisms,
that ultimately result in the occurrence of learning.
Eraut
et al
. (1998, 2004) indicates that there are
four types of learning, occurring within the work
environment, which may result in learning. There is
evidence in this study (see Table 3) of each type of
activity being implemented in practice. First, there
is evidence of participation in group activities (see
teamwork), which was aimed at achieving a com-
mon goal. Second, Eraut
et al
. (2002, 2004) suggested
working alongside others as a means of learning
through observation and increased awareness of
how others work, this can be evidenced through
the hc/hs work undertaken in the SCN. Third, he
suggests that engaging in challenging tasks, such as
action learning in this study, results in on-the-job
learning and increases both motivation and con-
fidence in the individual. Finally, working directly
with clients enhances learning. This was a key
emphasis in the study and resulted in the develop-
ment of a family-centred philosophy of care that
enabled collaboration between clinicians and
families in order to provide care for the patients.
Eraut
et al
. (2000) highlight the significance in the
relationship among challenge, support and confidence.
Through the intervention of ePD activities in the
Fig. 3 Jane’s learning journey.

Re-generating the ‘self ’ in learning 103
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
SCN and, in particular, the hc/hs approach, it can
be seen that an increased level of challenge enabled
clinicians to engage in learning. With this came an
increase in motivation to learn and the development
of the responsible self, where practitioners not only
understood learning but were active in seeking out
learning opportunities and sharing their learning
with one another. It is suggested that supporting
grassroots learning is important in creating a learn-
ing climate (Eraut
et al
. 1998). In order to support
this kind of learning, the role of the manager is
pivotal, yet managers themselves are given little
training in how to facilitate this kind of workplace
learning (Eraut
et al
. 2002). In this study, the role of
the manager was indeed pivotal in the engagement
of staff in learning and the overall outcomes for the
SCN. The manager herself engaged in most of the
learning strategies and adopted the techniques as
she became a positive role model and a facilitator of
practice development, which ensured that others
were motivated to participate.
Through the adoption of practice development
strategies that supported professional learning
principles (Knowles 1990; Ward & McCormack
2000), nurses who were actively engaged in learning
about learning were able to understand and chal-
lenge the role of self within the learning culture as
they moved from dependent to independent learner
and took on the role of responsible self, as depicted
in Fig. 4.
Figure 4 illustrates the strong links of the environ-
ment, learning about learning and the responsible
learner, as well as the influence that each aspect has
on one another. Nurses re-generated their perception
of self within the learning culture as they embraced
the notion of responsible self and reconnected with
enthusiasm and excitement to learning. They were
able to empower themselves (Gibson 1991) and
develop lifelong learning skills based on their own
vision for learning (Senge 1990), which held per-
sonal meaning for self: ‘learning is something I want
to do more, so that I can do the best job that I can do’
(Rogers 1969). This resulted in those who had pre-
viously dominated with negative attitudes toward
learning, having a reduced impact on the overall
learning culture, and those staff who had been
passive, developed greater autonomy as they were
supported through the changing context. This was
of utmost importance in building a sustainable
culture where challenge became part of everyday
practice.
Practice development is concerned with creating
a culture that is not only sustainable, but where
developing practice is not dependent on any one
individual (Garbett & McCormack 2004). It would
therefore be a failure if the practice development
work ground to a halt once the practitioner-researcher
had left the unit, as the emphasis is on developing
practitioners who carry on the work long after the
intervention is completed. One-year postintervention,
one-third of the staff have now undertaken formal
education in their speciality. They continue to
implement new initiatives, including ideas such
as the ‘hug a bub program’, where volunteers work
alongside staff to reduce the distress of babies
withdrawing for narcotic addiction, and the ‘babies
like books too’ initiative, which introduces reading
to babies from birth. These projects have enabled
staff to put into action the skills they developed
during the study as they strive to improve care:
I think we have come a long way, it’s positive … there is still lots we need to do and there will always be lots we need to do.
Fig. 4 Re-generating the ‘self ’ in learning.

104 V. Wilson
et al.
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
Conclusion
It can be seen, from this study, that the learning
culture has a significant impact on how nurses go
about their everyday practice. Cultural shift can be
achieved through the intervention of ePD activities.
In this study, the learning culture of the unit was
shaped by a series of tensions where staff were, at
times, working against one another. When these
tensions were revealed it enabled them to look at
their existing practice and to move forward with the
help of the practitioner-researcher. In doing this
they were able to turn the tensions around and work
towards a more effective learning culture. This was
achieved by freeing the oppressive elements of the
tension-laden culture as they worked towards being
an effective team. A supportive learning culture was
created that was embedded within the environment,
where learning about learning was seen as an important
part of the context that enabled the development of
the responsible self.
References
Almost J. & Laschinger H. (2002) Workplace
empowerment, collaborative work relationships, and
job strain in nurse practitioners.
Journal of American
Academy of Nurse Practitioners
14
, 408–420.
Atkins S. & Murphy K. (1993) Reflection; a review of
the literature.
Journal of Advanced Nursing
18
,
1188–1192.
Bierema L. & Eraut M. (2004) Workplace-focused
learning: perspectives on continuing professional
education and human resource development.
Advances
in Developing Human Resources
6
, 52–68.
Boyatzis R. (1998)
Transforming Qualitative Information
.
Sage, Thousand Oaks.
Clark P. (2001) What residents are not learning.
Observations in an NICU.
Academic Medicine
76
,
419–424.
Dewing J. (2002) From ritual to relationship: a
person-centred approach to consent in qualitative
research with older people who have dementia.
Dementia
2
, 157–171.
Dixon D. (1999) Achieving results through
transformational leadership.
Journal of Nursing
Administration
12
, 17–21.
Eden C., Jones S. & Sims D. (1983)
Messing About in
Problems
. Pergamon, Oxford.
Eraut M., Alderton J., Cole G. & Senker P. (1998)
Learning from other people at work. In:
Supporting
Lifelong Learning
(eds R. Harrison
et al
.), pp. 127–145.
Routledge, London.
Eraut M., Alderton J., Cole G. & Senker P. (2000)
Development of knowledge and skills at work.
In:
Differing Visions of a Learning Society
, Vol. 1.
(ed. F. Coffield), pp. 231–262. The Policy Press, Bristol.
Eraut M., Alderton J., Cole G. & Senker P. (2002) The
impact of the manager on learning in the workplace.
In:
Supporting Lifelong Learning, Volume 2, Organising
Learning
(eds F. Reeve
et al.
), pp. 91–108. Routledge,
London.
Eraut M., Maillardet F., Miller C., Steadman S., Ali A.,
Blackman C. & Furner J. (2004)
Learning in the
Professional Workplace: Relationships between Learning
Factors and Contextual Factors
. AERA Conference
Paper, San Diego.
Fay B. (1987)
Critical Social Science
. Polity Press, Cambridge.
Freire P. (1972)
Pedagogy of the Oppressed
. Herder &
Herder, New York.
Freshwater D. (1998)
Transformatory learning in nurse
education. PhD Thesis. University of Nottingham,
Nottingham.
Garbett R. & McCormack B. (2002) The qualities
and skills of practice developers. Nursing Standard 16,
33–36.
Garbett R. & McCormack B. (2004) A concept analysis
of practice development. In: Practice Development in
Nursing (eds B. McCormack, K. Manley & R. Garbett),
pp. 10–32. Blackwell Publishing, Oxford.
Gibson G. (1991) A concept analysis of empowerment.
Journal of Advanced Nursing 16, 354–361.
Grundy S. (1982) Three modes of action research.
Curriculum Perspectives 2, 23–34.
Hoff T., Pohl H. & Bartfield J. (2004) Creating a learning
environment to produce competent residents: the
roles of culture and context. Academic Medicine 6,
532–540.
Johns C. (1994) Guided reflection. In: Reflective Practice in
Nursing (eds A. Palmer, S. Burns & C. Bulman),
pp. 110–130. Blackwell Science, Oxford.
Johns C. (1998) Opening the doors of reflection. In:
Transforming Nursing Through Reflective Practice (eds
C. Johns & D. Freshwater), pp. 1–20. Blackwell Science,
Oxford.
Kaye B. & Jordan-Evans S. (2000) Retention: Tag you’re it!
Training and Development 54, 29–33.
Knapper C. & Croppley A. (1999) Lifelong Learning and
Higher Education, 3rd edn. RoutledgeFalmer,
London.
Re-generating the ‘self ’ in learning 105
© 2006 The AuthorsJournal compilation © 2006 Blackwell Publishing Ltd.
Knowles M. (1977) The Adult Education Movement in the
United States, 2nd edn. Krieger Publishing Co, New
York.
Knowles M. (1990) The Adult Learner: a Neglected Species,
4th edn. Gulf Publishing Co., Texas.
Knowles M., Holton E. & Swanson R. (1998) The
definitive classic in adult education and human
resource development. In: The Adult Learner, 5th edn.
Chapter 11, pp. 198–201. Gulf Publishing Co., Texas.
Laschinger H., Finegan J., Shamian J. & Almost J. (2001)
Testing Karasek’s demands-control model in
restructured healthcare settings: effects of job strain on
staff nurses’ quality of work life. The Journal on Nursing
Administration 31, 233–243.
Manley K. (2004) Workplace culture: is your workplace
effective? How would you know? Nursing in Critical
Care 9, 1–3.
Manley K. & McCormack B. (2003) Practice development:
purpose, methodology, facilitation and evaluation.
Nursing in Critical Care 8, 22–29.
McCormack B. & Garbett R. (2003) The characteristics,
qualities and skills of practice developers. Journal of
Clinical Nursing 12, 317–325.
McGill I. & Beaty L. (2001) Action Learning: A Guide for
Professional, Management and Educational
Development, 2nd edn. Kogan Page Ltd, London.
Melia K. (1987) Learning and Working: the Occupational
Socialization of Nurses. Tavistock Publication Ltd,
London.
Miller C., Tomlinson A. & Jones M. (1994) Researching
Professional Education: Learning Styles and Facilitating
Reflection. English National Board of Nursing,
Midwifery and Health Visiting, London.
Nolan C. (1998) Learning on clinical placement: the
experience of six Australian student nurses. Nurse
Education Today 18, 622–629.
Patton M. (1990) Qualitative Evaluation and Research
Methods, 2nd edn. Sage, California.
Platzer H., Blake D. & Ashford D. (2000) Barriers
to learning from reflection: a study of the use of
groupwork with post-registration nurses. Journal
of Advanced Nursing 5, 1001–1008.
Rogers C. (1969) Freedom to Learn. Charles E. Merrill,
Ohio.
Rolfe G. (1996) Closing the Theory Practice Gap: a New
Paradigm for Nursing. Butterworth Heinmann,
Oxford.
Rycroft-Malone J. (2004) The PARIHS Framework – a
framework for guiding the implementation of
evidenced-based practice. Journal of Nursing Care
Quality 19, 297–304.
Senge P. (1990) The Fifth Discipline: The Art and Practice of
the Learning Organization. Doubleday Currency, New
York.
Titchen A. & Binnie A. (1995) The art of clinical
supervision. Journal of Clinical Nursing 4, 327–334.
Wade R. (1994) Teacher education students’ views on class
discussion: implications for fostering critical reflection.
Teaching and Teacher Education 10, 231–243.
Ward C. & McCormack B. (2000) Creating an adult
learning culture through practice development. Nurse
Education Today 20, 259–266.
Weiler K. (1996) Myths of Paulo Freire. Harvard
Educational Review 66, 353–371.
Wilson V. (2005a) Developing a culture of family-centred
care: an emancipatory practice development approach.
PhD Thesis, Monash University, Melbourne.
Wilson V. (2005b) Developing a vision for teamwork.
Practice Development in Health Care 4, 40–48.
Wilson V., Keachie P. & Engelsmann M. (2003) Putting the
Action into Learning: the experience of an action
learning set. Collegian 10, 22–26.
Wilson V., McCormack B. & Ives G. (2005) Understanding
the workplace culture of a special care nursery. Journal
of Advanced Nursing 50, 27–38.
Winter R. & Munn-Giddings C. (2001) A Handbook for
Action Research in Health and Social Care. Routledge,
London.
Top Related