Languages
Pages
Legal


OBESITYNOTE: Obesity is included in the ICD-10 but not in the DSM-
IV as it has not been established that it is consistently associated with a psychological or behavioural syndrome
(APA, 2000)
“ has identified obesity as one of the major chronic diseases that increases risk of non communicable diseases such as type 2 diabetes and high BP”

http://youtu.be/8HSqE1U_m_0
http://youtu.be/TyUu0EUjD-s
Watch the following clip...

1. What is obesity?2. Why are so many people obese?3. Who is most and least likely to be obese?4. How can you determine whether you are
obese?5. When are you considered underweight,
overweight and obese according to your BMI?
6. What are the consequences of obesity?
Quiz time!!

1 in 2 adults in the US were either overweight or obese in the 1990s (Tataranni, 2000)
In the UK there is an upward trend in obesity◦ 1\2 women and 2\3 men are either overweight or
obese Obesity shortens life by an average of 9
years (National Adult Office, 2001) Mokdad et al (1999) refer to an “obesity
epidemic”
Obesity – the facts
The World Health Organization increases risks of◦ Type 2 diabetes◦ High blood pressure◦ Reduced life expectancy (Must et al 1999)
Masso-Gonzalez (2009) estimated the incidence of diabetes in the UK between 1996 and 2005 aged 10-79◦ Type 1 was constant◦ Type 2 increased from 46% to 56%
Obesity – the facts (cont.)
1980- 6% men and 8% women, by 1997, 17% and 21%
Chinn and Rona (01)- English children 50% more obese compared to results in 1994
Highest rates of obesity- USA, Saudia Arabia, Tunisia and Canada
How common is Obesity?

Most common ways to define obesity are ◦ BMI (Body Mass Index) ◦ Waist circumference◦ Measuring thickness of fatty tissue using callipers
What is obesity?
BMI is calculated dividing a person’s weight by their height squared
BMI of less than 18.5=underweight BMI over 25=overweight BMI over 30=obese BMI over 40=morbidly obese http://www.nhlbisupport.com/bmi/
BMI (Body Mass Index)

Adominal fat rather than lower body fat can predict incidence of health problems
Lean et al (1998)- weight reduction recommended when waist circumference:
greater than 102cm in men (40 inches) greater than 88cm (35 inches) in women
Waist Circumference
What are the problems with
BMI as a measure of
obesity?
Psychological Explanationsto obesity
How would the psychodynamic, behavioural and
cognitive approach explain
obesity??
Behaviourist explanation of Obesity
Seen as a maladaptive, learned behaviour occurring through overeating in 3 ways:
1. Classical conditioning2. Operant conditioning3. Social learning theory
Matching time...
2. Operant conditioning
1.Classical conditioning
B. Obesity occurs by the observation and imitation of obese
role models
A. Obesity occurs due to food being used as
a reinforcer for desirable behaviour
3. Social learning theory
C. Obesity occurs because food is
naturally associated with pleasure and food
cues come to be associated with a
pleasurable response
Foster (2006): found treatments based on CC are successful as they help patients identify cues triggering inappropriate eating and then learn new responses to them
Jackson (2008): reinforcing children for eating creates compulsions leading to obesity, OC in childhood is to blame
Hardeman et al (2000): treating obesity by role models encouraging healthy lifestyles led to significant weight loss
Research

Wing et al (2002): treatments based on CC incur average weight loss of 15.6 kg in 18 months....it works!!
Devlin (1995): treatments based on OC resulted in weight loss not being maintained
Weight loss after SLT treatments tend to be short term, suggesting that other explanations should be considered
A02
food is associated with stress control
Emotional arousal =>dishinibition of restraint “ what the hell!”=>emotional eating
Heatherton (1993) suggests that overeating constitutes an escape from self-awareness in response to emotional pain
Emotional eating
Emotionality theory of obesity (Schachter, 1968)◦ People who become obese eat for emotional
reasons◦ Thin people eat for hunger
Overeating (hyperphagia) and under-eating (hypophagia) were also considered a way of managing emotions by Bruch (1965)
Emotional eating
+Polivy&Herman (1999) told women they had passed\failed a cognitive test – those who had failed chose to eat as much as they liked
-there is contrasting evidence on the link between stress and eating
Evaluation
+Verplanken et al. (2005) correlational analysis on mood, impulse buying and snack consumption◦ Those with low self-esteem were more likely to
impulse buy and also consume snacks◦ Possibly this behaviour is an attempt to cope with
the emotional distress caused by low self-esteem
-issues with causality: overeating might be the cause of low mood rather than the consequence!!
Evaluation

How can we evaluate behaviourism according to...
ISSUESDEBATES
APPROACHESAO3

Approaches◦ alternative explanations (eg social; cognitive)◦ Cognitive approach: motivation CAN reflect action
(social cognition models)◦ Social approach: importance of cultural factors and
availability Issues Gender bias Debates
◦ Free will vs determinism◦ Nature vs nurture
AO3◦ Lack of ecological validity (artificial setting)◦ PPs mostly females (lack of generalisability)
IDAs and AO3s
Unresolved conflicts, e.g. Emotional deprivation during the oral stage
Libido becomes locked onto oral gratification
Psychodynamic explanation of obesity

Linked to poor childhood experiences
Felliti (2001)- reported 5 cases of sleep eating obesity all had suffered from abuse in childhood
Behaviour as an unconscious anxiety reducer
Psychodynamic approach
Most obese people haven’t suffered abuse or indulged in sleep eating...cannot be only account
No evidence of a parallel rise in unresolved childhood conflict
Just ideas...cant prove or disprove
Evaluation
Food as a symbol of love- compensate for absence of love
Creates a circle of overeating
Psychodynamic approach to obesity
overweight
No loveovereat
Support for Freudian construct of mother love- loving bond established by mother and baby is through food
Breast milk is sweet and high in fat content
Overweight people eat food high in sugar/fat
Evaluation

Occurring as a result of maladaptive thought processes
information processing having an elevated focus for food related stimuli
Cognitive explanations of obesity
Brat and Crombez (2001)- obese children were hypersensitive to food related words, suggesting an info processing bias for food stimuli leading to obesity
Cserjesi et al (2007)- examined cog profiles of obese boys and found them deficient in attention capabilities, suggesting childhood obesity involved cognitive deficits.
Research

Cause and effect- Elias (2003) found that early onset, long term obesity leads to a decline in cog functioning
But successful therapies suggest cog
factors may be involved in developing obesity
O’Rourke (2008) found that CBT sig improved weight loss
Evaluation
Complete the gap fill task WITHOUT using your
notes

Biological explanations of obesity
•Genetic theories•Neural model of obesity•Evolutionary model of obesity
Read the handout on the genetic
explanation of obesity and answer the
following questions

Genetic theories Family clusters
◦ If one parent is obese, 40% chance of child being obese◦ If both parents are obese, 80%◦ Probability of thin parents producing obese offspring is only
7%! Twin studies
◦ MZ twins reared separately are more similar in weight than DZ twins reared together!!!
◦ Stunkard et al (1990) examined the BMI of 93 pairs of MZ twins reared apart and found that genetic factors accounted for 66-70% of variance in body weight
◦ HOWEVER, role of genetics seems stronger in lighter twin pairs than in heavier ones
Metabolic rate theory◦ ‘resting metabolic rate’s highly inheritable◦ Tataranni et al (2003) study on Pima Indians
Appetite control may depend on a genetic predisposition
A gene connected with profound obesity in small animals has been identified BUT still unclear for humans
Montague et al (1997) two children have been identified with a defect in their ‘ob gene’, which produces leptin ◦ They were given daily injections of leptin◦ They lost 1-2 kg per month
Genetic theories – appetite regulation
How could we explain obesity according to the
neural explanation?
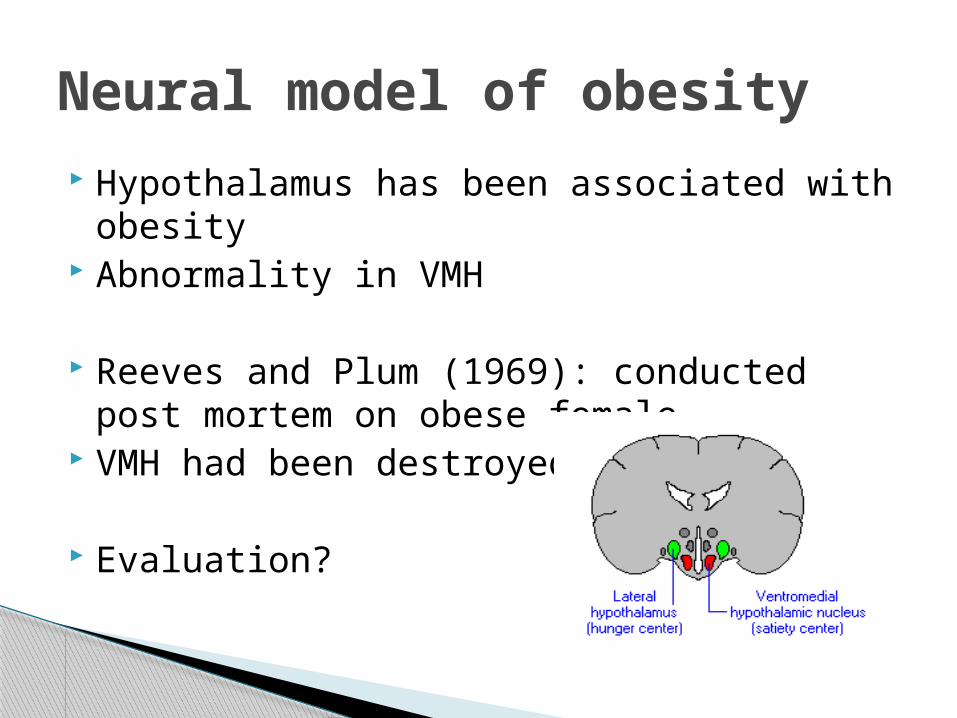
Hypothalamus has been associated with obesity
Abnormality in VMH
Reeves and Plum (1969): conducted post mortem on obese female
VMH had been destroyed
Evaluation?
Neural model of obesity

Friedman (2005) reported that 2 hypothalamic neurons regulate appetite
Key role in establishing weight NPY= starts eating POMC= stops eating Both controlled by Leptin In obese people, Leptin is unable to
suppress POMC, so appetite stays high and they gain weight
Neural model of obesity

Evaluation
Leptin injections could be an effective treatment in treating obesity
However, only works in a few people Casts doubt on the importance of Leptin
Neural model of obesity

Evolutionary model of obesity
Read the article and answer the
questions......How could evolution
explain obesity??
Our eating habits are more suited to the EEA where food was not universally available
Evolved to find high calorific foods desirable Store excess energy as fat for times of
scarcity Evolved to minimise physical activity to
preserve fat stores
Evolutionary model of obesity
Those individuals who were most energy efficient in terms of burning off excess energy and remaining thin would have been less successful
Evolutionary mechanisms would have favoured those who stored excess fats and were less efficient in burning it off= Aid survival!!
Thrifty Gene hypothesis (Neel, 1962)
How we have evolved is not suited to our sedentary world of ever available fatty foods
Vulnerable to overeating foods which were scarcely available in our evolutionary past
Environment no longer requires thrifty genes so this results in obesity, health problems, such as type 2 diabetes!
How does evolution explain obesity then?
Sedentary lifestyle is a medical term used to denote a type of lifestyle with no or irregular physical activity.[1] A person who lives a sedentary lifestyle may colloquially be known as a couch potato. It is commonly found in both the developed and developing world. Sedentary activities include sitting, reading, watching television and computer use for much of the day with little or no vigorous physical exercise. A sedentary lifestyle can contribute to many preventable causes of death.

+explain why obesity often runs in family
+there is evidence for certain ethnic groups being more predisposed to obesity
+reduce the risk of stigmatisation of obese individuals....
-BUT might reduce effectiveness of dieting
Biological explanations - evaluation
- doesn’t explain why obesity is on the increase today, whereas our gene pool has remained constant
-doesn’t explain why geographical relocation to obesogenic environment often causes individuals to gain weight
-it is still unclear how genes are involved in obesity and to what extent...
Biological explanations - evaluation

Biological explanation of obesity
Metabolic rate
theory
Thrifty Gene
hypothesis

Ob gene
Ventromedial
hypothalamus