







Languages
Pages
Legal


- AIRC -Associazione Italiana per la Ricerca sul Cancro
Associazione Italiana Ricerca CancroFondazione Ricerca Scientifica Termale
(FoRST)Year: 2008
Via Corridoni, 7 - 20122 MILANOtel.02/7797217-275 - fax 02/7797259
email: [email protected] informazioni tecniche tel.02/7797224
Codice Riferimento: 8509 Page 1 of 38

ASSOCIAZIONE ITALIANA PER LA RICERCA SUL CANCRO
Codice Riferimento: 8509
TITLE PAGE
Principal Investigator's full Name and QualificationProfessore Mutti Antonio - MD
Proposal TitleAssessment of lung dose of carcinogens and related pathobiology in COPD patients inhaling sulphurous water.
Type IG
Area Infection, inflammation and cancer
Sub Area
Budget 2008 (euro): 59.400,00 € Estimated budget 2008 - 2010 (euro): 184.140,00 €
InstitutionUniversità di Parma
Department/otherClinical Medicine, Nephrology and Health Sciences - Industrial Toxicology
StreetVia Gramsci 14
Town + Zip code43100 PARMA (PR)
Phone0521033075
Fax0521033076
Authorized Administrative OfficialPietro Schianchi (Department Administrative Secretary)
StreetVia Gramsci 14
Town + Zip code43100 PARMA (PR)
Phone0521033333
Fax0521033135
Proponent's signatureMutti Antonio
Date21/10/2008
Authorized Administrative Official's signaturePietro Schianchi (Department Administrative Secretary)
Date21/10/2008
Codice Riferimento: 8509 Page 2 of 38

EVALUATION FORM (2003 - 2008)
Principal Investigator's Full NameProfessore Mutti Antonio - MD
Total Papers and Reviews 27
Total Papers and Reviews with IF 24
Total IF 97,789
Average IF 4,1
Papers First/Last or Corresponding Author 23
Total IF 95,107
Average IF 4,1
Codice Riferimento: 8509 Page 3 of 38

ABSTRACT
Principal Investigator's Full Name
Professore Mutti Antonio
Institution and City
Università di Parma
Proposal Title
Assessment of lung dose of carcinogens and related pathobiology in COPD patients inhaling sulphurous water.
Area Infection, inflammation and cancer
Sub Area
Abstract in the next page
Codice Riferimento: 8509 Page 4 of 38

Background
Inhalation of thermal water has been used empirically in the treatment of chronic diseases of upper and
lower respiratory tract, including chronic obstructive pulmonary disease (COPD). The positive effects of the
activity of inhaled thermal waters has been partially based on the patients' subjective sense of wellbeing and
partially, but not always easy to quantify, symptomatic clinical improvements. Despite its widespread use,
much uncertainty exists about the indications and therapeutic mechanisms of thermal water inhalations in
the treatment of respiratory diseases.
The possible benefit of thermal sulphur water inhalation in patients with lower airway respiratory diseases,
such as CODP, could be attributed to the properties of water components, mainly sulphide species such as
hydrogen sulphide, hydrosulfide ion and sulphide anion, which are able to restore SH (e.g. thiols) groups
into airways, thus increasing the antioxidant activities and reducing airway inflammation.
Hypothesis
The main working hypothesis relies on the conception that, for lung disorders associated with depletion of
SH groups and increased production of reactive oxygen species, such as COPD, treatment with sulphur
thermal inhalation is able to replace or increase the SH pool, thus targeting oxidative stress.
The secondary working hypothesis is that thermal water is able to modify pulmonary concentration of
smoking related biomarkers, such as metallic elements and exhaled volatile organic compounds, either
thorough an improvement in rheological characteristics of the mucus or improving individual detoxifying
capacity.
Aims of the study
Primary aim is to assess exposure to selected components of tobacco smoke and biomarkers of pulmonary
effect in COPD patients inhaling thermal sulphurous water. Secondary aims are: i) to develop and validate a
system that allow a fractional sampling of exhaled air and the condensation of the last part of a slow vital
capacity; ii) to characterize some thermal water compounds retained in the lung and, conversely, the
exhaled concentration of toxic elements and other organic components of tobacco smoke.
Experimental design
An observation study will be carried in COPD patients receiving a short treatment (12 days) with sulphur
thermal water of Terme di Monticelli. Subjects will be assessed serially in terms of lung function test,
exhaled breath and induced sputum collection. Lung damage will be searched through the measurement of
oxidative stress/inflammatory compounds, in order to identify biomarkers of local effects, which may be
sensitive endpoints for characterizing early biochemical changes in the airways occurring after thermal
treatment.
The application of exhaled breath analysis will be also used for the development of new biomarkers of dose
in subjects exposed to pneumotoxic chemicals contained in tobacco smoke, in order to achieve a better
understanding of the possible relationship between environmental pollutants retained at the target organ
and the consequence of thermal treatment.
Codice Riferimento: 8509 Page 5 of 38

1
Background
Respiratory disorders are among the leading cause of morbidity and mortality worldwide, and further
increase is expected in the near future. In Europe, respiratory diseases rank second (after cardiovascular
diseases) in terms of mortality, incidence, prevalence and costs. Whereas there has been a substantial
reduction of infective lung diseases, such as tuberculosis and pneumonia, over the last decades there has
been a progressive increase of smoking related lung diseases, including COPD and lung cancer (Dal Negro et
al. 2003, Pouwels et al. 2004).
COPD is the 4th cause of death in the USA, its incidence being increasing despite the decreasing prevalence
of smokers. In addition to mortality, morbidity from COPD results in substantial use of secondary healthcare
resources (Pauwels et al. 2004, Hurd 2002).
Lung cancer is the leading cause of death from cancer worldwide, and tobacco smoking is associated with
90% of cases of lung cancer (Bliss et al. 2004). Cigarette smoking is also the most important risk factor for
chronic bronchitis and/or COPD (Houghton et al. 2008). Lung cancer, COPD, and chronic bronchitis therefore
share a common risk factor—tobacco smoking—through which they may also share similar pathogenetic
mechanisms. Squamous cell carcinoma has a stronger association with active tobacco smoking than other
non-small cell lung cancers, while smokers with chronic bronchitis are at a higher risk of developing lung
adenocarcinoma (Bliss et al. 2004, Bach et al. 2003). In a recent study designed to predict the risk of lung
cancer for African-Americans, it has been found that having a history of COPD increased the risk of
developing lung cancer by a factor of 6, irrespective of smoking history (Etzel et al. 2008).
Today, COPD and lung cancer loom as two of our greatest challenges in pulmonary medicine. Consequently,
measures aimed at primary and secondary prevention and studies aimed at identifying new therapeutic
strategies are highly desirable. Unfortunately, these goals remain elusive and COPD and lung cancer
represent a challenging unmet medical need. More research is needed to understand the cellular and
molecular mechanisms of COPD and to develop biomarkers and monitoring techniques to aid the
development of new therapies (Cazzola et al. 2008).
Inhalation of thermal water has been used empirically in the treatment of chronic diseases of upper (Staffieri
et al. 2007) and lower respiratory tract, including COPD (Pellegrini et al. 2004). The positive effects of the
activity of inhaled thermal waters has been partially based on the patients' subjective sense of wellbeing and
partially, but not always easy to quantify, symptomatic (or general) clinical improvements. Despite its
widespread use, much uncertainty exists about the indications and therapeutic mechanisms of thermal water
inhalations in the treatment of respiratory diseases.
To the best of our knowledge, only one study assessed the effect thermal water inhalation in COPD patients.
In this study, authors demonstrated that treatment with inhaled salt-bromide-iodine thermal water in COPD
PROPOSAL MAIN BODY
Codice Riferimento: 8509 Page 6 of 38

2
patients is associated with a reduced proportion of neutrophils in induced sputum (Pellegrini et al. 2005).
There are no other published studies on COPD patients (at least not in Journals listed in pubmed), in which
the effect of sulphur thermal inhalation has been evaluated.
Rationale
The possible benefit of thermal sulphur water inhalation in patients with lower airway respiratory diseases,
such as CODP, could be attributed to the properties of water components, mainly sulphide species -
hydrogen sulphide (H2S), hydrosulfide ion (HS-), and sulphide anion (S2-) – which are able to restore HS
groups into airways, thus increasing the antioxidant activities and reducing airway inflammation.
Recent data indicate that H2S, which for a long time has been recognized as an exogenous toxic gas, is
endogenously generated in various mammalian tissues and may be a functional regulator in nervous and
cardiovascular systems (Wang et al. 2002); few data in COPD patients demonstrate that endogenous H2S is
involved in the pathogenesis of airway obstruction in COPD (Chen et al. 2005). Although the mechanism by
which H2S acts into airways of COPD patients and the source of endogenous H2S is unknown, studies
showed that H2S act as an inhibitor of hypochloric acid-mediated oxidative damage in the brain, a scavenger
of endogenous peroxynitrite in nervous tissues, and an antagonist of lipid peroxidation induced by oxygen-
free radicals in the heart (Hosoki et al. 1997, Geng et al. 2004, Du et al. 2004).
The main working hypothesis of this research proposal relies on the concept that, for lung
disorders associated with depletion of SH (thiols) groups and increased production of reactive
oxygen species, such as COPD, treatment with sulphur thermal inhalation can increase the SH
pool, thus targeting oxidative stress (see figure 1).
In addition, a new but fascinating working hypothesis will be also studied. In a recent study, we showed that
metallic elements and volatile organic compounds (VOCs) are easily detected in exhaled breath of COPD
patients, and that some toxic metals and VOCS are higher in exhaled breath of patients with smoking history,
even years after they quit smoking (Mutti et al. 2006, Poli et al. 2005). A possible explanation is that tobacco
smoke and polluted environments substantially increase the lung burden of pneumotoxic and carcinogenic
chemicals that, because of their stability, can also be used as tracers of environmental pollution. In
particular, biomarkers of exposure (Al, Cd, Cr, Ni, Pb, As) in airway fluids and selected VOCs (e.g. benzene)
in exhaled breath may provide a quantitative estimate of the target tissue dose of carcinogenic agents, thus
identifying those exposed subjects who retain more amount of agents into airways because of different
detoxifying capacity. Furthermore, some heavy metals (Cd, Pb, Hg) have a high affinity for SH groups, so
that they indirectly contribute to oxidative stress by reducing the scavenging potential (GSH depletion)
(Houston et al. 2007, Patrick et al. 2003, Valko et al. 2005, Kelly 1998, Mishra et al. 2006, Tiryakiouglu et al.
2006, Quig 1998, Rugstad et al. 1984). Interestingly, it has been hypothesized that thermal sulphurous
inhalation may increase GSH levels into airways (Braga et al. 2008).
Codice Riferimento: 8509 Page 7 of 38

3
Exhaled breath and induced sputum will be used to quantify metallic elements and VOCs as biomarkers of
exposure and susceptibility in COPD patients receiving thermal sulphur inhalation treatment. The working
hypothesis is that thermal water is able to modify pulmonary concentration of metallic
elements and exhaled VOCs, either thorough an improvement in rheological characteristics of
the mucus or improving the individual detoxifying capacity. Regarding the latter point, it can be
speculated that sulphur components can detoxify toxic elements, e.g., Hg, Cd and Pb, by making these
metallic elements soluble in water, thereby improving their clearance. It is known that the toxicity of Cd
(which, interestingly, was elevated in EBC of COPD patients) (Mutti et al. 2006) largely depends upon its
chemical species, the free Cd++ ion being considered to be the most toxic form. Thiol compounds (such as
glutathione and metallothioneins) play an important role in complexing Cd in biological systems and this
complexation is the primary mechanism of Cd detoxification in organisms (Quig 1998, Patrick et al. 2003,
Valko et al. 2005). Supplementation of SH groups with thermal water inhalation should accelerate the
excretion rate of the mobilized metals.
Aims of the study
Primary aim
1. To assess exposure to selected components of tobacco smoke and biomarkers pulmonary effect in COPD
patients inhaling thermal sulphurous water
Secondary aims are:
1. To develop and validate a system that allow a fractional sampling of exhaled air and the condensation of
the last part of a slow vital capacity,
2. To characterize some thermal water compounds retained in the lung and, conversely, the exhaled
concentration of toxic elements and other organic components of tobacco smoke.
Experimental design and research network
Each subject will be examined three times: before (visit 1), after six days (visit 2) and after 12-days (visit 3)
treatment with sulphur thermal water of Terme di Monticelli. The same types of treatment (Aerosol,
Humage) will be given in all patients. Each visit will include the evaluation of spirometry, exhaled breath
(VOCs, NO, CO), and EBC collection. Sputum induction will be performed at visit 1 and 3 only, being slightly
invasive. A time window of + 2 days among study visits will be considered acceptable. For current smokers,
it will be asked to refrain from smoking one hour before each study visit. For those subjects under
medication, no changes in scheduled therapy will be allowed.
Rationale for studying specific population, body fluids and biomarkers
The study will be performed in COPD patients with a relevant smoking history. We decided to study this
population (rather than asymptomatic smokers or patients with chronic bronchitis) for several reasons: 1)
the definition of COPD is easy to be obtained being well standardized (Rabe et al. 2007); 2) patients with
Codice Riferimento: 8509 Page 8 of 38

4
COPD have a great risk of developing lung cancer (at least some histo-types) than normal smokers (Papi et
al. 2004); 3) the degree of inflammation and oxidative stress is usually greater than in smokers without
COPD leaving, therefore, much room for changes after treatment (Barnes et al. 2003, Caramori et al. 2005).
Exhaled breath and induced sputum are suitable fluids to assess biomarkers of pulmonary inflammation,
which may be sensitive endpoints for identifying biochemical changes in the airways after specific treatment
(Cianchetti et al. 2004, Kharitonov et al. 2002); in addition, both fluids may be used to assess the lung
burden of selected carcinogenic agents, thus helping the identification of individual detoxifying capacities
into airways. Moreover, exhaled breath may be useful to characterize some thermal water
compounds retained in the lung in order to achieve a better understanding of the events
between exposure to sulphurous water and adverse effects on the lung (some preliminary data
are available).
Exhaled breath will be used to quantify gases, such as CO and NO, and vapours (VOCs). CO will be used to
assess current smoking status, whereas exhaled NO will be used being a well validated biomarkers of
inflammation (Kharitonov et al. 2002). Exhaled NO will be measured at different exhalation flow rates in
order to assess alveolar NO concentration and bronchial NO flux. This approach could help adding new
information to the use of exhaled NO in COPD patients, being the exhaled NO measured at fixed expiratory
flow (50 ml/s) is still clinically doubtful (Puckett et al. 2008).
EBC and exhaled VOCs will be collected in a specially-designed system which enables the collection of
exhaled breath into two separate and subsequent parts (air from proximal and distal airways). This approach
might be of particular interest to be applied in this study for two reasons: 1) alveolar inflammation
contributes to COPD pathogenesis (Rabe et al. 2007); 2) the effect of thermal water may be evident in
proximal and/or distal airways, due to the different size of inhaled water particles.
EBC will be used to assess those biomarkers of inflammation (LTB-4 and IL-8) and oxidative stress (8-
isoprostane, MDA, H2O2) which are known to be elevated in COPD patients (Barnes et al. 2003). EBC will be
also used to quantify pH. Using EBC, studies have shown that patients with COPD have airway acidification
(Horváth et al. 2005). The study of airway pH in patients receiving sulphur thermal inhalation might be of
particular interest, being the water rich in basic anions.
EBC will be also used to determinate nitroso-glutathione (GSNO). GSNO is considered to be a major source
of bronchodilator activity in the airway lining fluid and, more generally, may contribute to airway homeostasis
through its antimicrobial and anti-inflammatory properties (Corradi et al. 2001). We expect that sulphur
inhalation leads to the donation of HS groups, thus forming reduced glutathione.
EBC will be also used to characterize the lung burden of toxic metals (through the analysis of metallic
elements) and to evaluate the concentration of sulphate (being the determination of sulphide species
troublesome) in EBC; the latter, could be used as a tracer to assess the dose of thermal sulphur reaching the
Codice Riferimento: 8509 Page 9 of 38

5
airways. Preliminary data conducted at our laboratory showed that the concentration of inorganic anions,
including chloride, bromide, nitrate, nitrite, and sulphate, is measurable on EBC samples of both healthy
subjects and patients with different lung pathologies (Table 1). Sulphate was the most abundant anion, its
concentration ranging between 0.26 and 1.67 mg/l.
Table 1. Inorganic anion concentration in EBC
Sample ID Chloride Bromide Nitrate Nitrite Sulphate
#1 control 0.169 0.074 0.380 0.059 1.291
#2 control 0.111 0.016 0.101 0.047 0.330
#3 control 0.060 0.013 0.046 0.039 0.731
#4 control 0.121 0.025 0.033 0.023 0.261
#5 asthma 0.593 n.d. 0.315 0.105 1.325
#6 asthma 0.540 0.023 0.282 0.135 1.677
#7 COPD 0.435 0.117 0.325 0.095 0.741
#8 COPD 0.248 0.018 0.281 0.138 1.402
#9 COPD 0.033 0.025 0.018 0.081 0.281
#10 COPD 0.778 0.010 0.056 0.005 1.016
mean 0.473 0.042 0.218 0.032 1.154
median 0.209 0.023 0.191 0.088 0.879
Range 0.033 - 0.778 <0.01- 0.117 0.018 - 0.380 0.005-0.138 0.261-1.677
Selected exhaled vapours will be analysed: the process of free radical formation and consecutive
peroxidation of polyunsaturated fatty acids (which is of particular relevance in COPD patients) induces the
pulmonary formation of volatile hydrocarbons (e.g. endogenous compounds such as pentane, ethane),
which can be identified and quantified in breath samples (Paredi et al. 2002). Furthermore, selected
smoking-related substances will be also analysed (e.g. benzene and other mono-aromatic hydrocarbons).
Whereas it might be difficult to expect a reduction of smoking related substances in exhaled breath following
thermal inhalation (unless people stop smoking), some exhaled VOCs may be of interest, in particular those
which are related to lung oxidative stress, such as pentane and ethane (Paredi et al. 2002).
Induced sputum will be assessed in terms of inflammatory cells and mediator in the supernatant. There is an
abnormal pattern of inflammatory cells in COPD patients, with an increase in number of total inflammatory
cells in the percentage of neutrophils (Barnes et al. 2003). We expect to obtain a reduction in neutrophils in
sputum following thermal sulphur treatment. Many mediators have been reported to be increased in the
supernatant of COPD patients and most show a greater increase in normal smokers than in COPD. Induced
sputum will be also used to evaluate the expression of inflammatory mediators IL-8, TNF-α, INF-γ, by
means of commercially available ELISA kits. In addition, by western blot and ELISA techniques, the lung
Codice Riferimento: 8509 Page 10 of 38

6
parenchymal destruction markers MMP-9, TIMP-1 and elastase/desmosin will be investigated in the same
sample.
Materials and Methods
Ethics
This research protocol will be approved by the Institutional Review Board of the University Hospital of Parma
before research under such a protocol can begin. Subjects will be informed on the scope of the study and
will sign a consent form before enrolment.
Inclusion/exclusion criteria
COPD patients will be defined as those with relevant smoking history (at least 10 pack/year), symptom
history (chronic cough, sputum production, dyspnoea wheeze), and spirometric measurements of post-
bronchodilator forced expiratory volume in one second (FEV1) <80% and FEV1/FVC <0.7 (Rabe et al. 2007).
Patients with a history of asthma or atopy, or with other clinically significant diseases, and patients who had
suffered a respiratory tract infection or exacerbation of their disease or had taken inhaled or systemic
corticosteroids in the previous month were excluded.
Both current and ex smokers are eligible. We will define ex smoker those COPD patients who stopped
smoking for at least six months. Smoking status will be assessed in terms of self reported smoking history
(cigarette/day, packs/year) and will be confirmed by the analysis of CO in exhaled air. Exhaled CO levels
greater that 8 parts per million will be considered as suggestive of active and current smoking (Bacha et
al.2007). Biomarkers of smoking history will be also used to assess the smoking habit during the two week
treatment. In all case of current smokers, smoking cessation will be strongly recommended.
Lung function tests
Spirometry will be performed with a pneumotachograph (Koko Spirometer, Sensormedics, Milan, Italy).
Mean values for FEV1, FVC and FEF25-75 will be obtained from the three best acceptable test values of lung
function, according to the recommendation of the European Respiratory Society (Miller et al. 2005).
Exhaled CO
Exhaled CO will be measured on a portable Bedfont EC50 analyzer (Bedfont Technical Instruments Ltd,
Sittingbourne, UK) in which subjects are asked to exhale fully, inhale deeply, and hold their breath for 20 s
before exhaling rapidly into a disposable mouthpiece. This procedure will be repeated three times, with
1 min of normal breathing between each repetition, and the mean value will be used for analysis
Exhaled NO
All exhaled NO measurements will be performed according to current guidelines (ATS 2005). Exhaled NO will
be measured with a new portable machine which enables the collection of eNO and different flow rates,
Codice Riferimento: 8509 Page 11 of 38

7
ranging from 50 ml/s to 250 ml/s. At each expiratory flow, subjects are requested to inhaled NO-free air
(through a filter which is placed in the machine) and subsequently exhaled at constant flow for
approximately 6-10 s., The mean of the first three technically acceptable measurements within 10%
performed will implicated into analysis. The machine is connected to a personal computer which is provided
with a software an iterative algorithm which calculates the three flow-independent NO exchange parameters
confined to the two compartments, the conducting airways, which are characterised by the Caw,NO and airway
transfer factor (or diffusing capacity) for nitric oxide (Daw,NO), and the alveoli, characterised by the alveolar
nitric oxide concentration (CA,NO). A fourth variable, J'aw,NO, was also used. J'aw,NO is calculated from
Daw,NO(Caw,NO–CA,NO).
Exhaled breath condensate
EBC will be collected using a specially designed condenser (Turbo Deccs, Italchill, Parma, IT). Subjects will
be asked to breath tidally for 15 minutes without nose clip in place, through a two-way non re-breathing
valve by which inspiratory and expiratory air is separated, and saliva is trapped. EBC produced during a 20
min manoeuvre (2-3 mL) will be collected in vials and stored immediately at -80 °C and kept frozen until
analysis. Biomarkers of inflammation and oxidative stress will be evaluated as previously described and
according to validated procedures (storage and analysis) (Horwath et al. 2005) which are currently used in
our lab (Corradi et al. 2004).
The elemental composition of EBC will be determined by means of ICP-MS, thus relying on a reference
analytical method. ICP-MS (ELAN 5000; Perkin Elmer; Wellesley, MA) analyses will be made using the
external calibration method and reference material 1643 from the National Institute of Standards and
Technology (Gaithersburg, MD) for the assessment of analytical accuracy.
Inorganic ions will be assessed by means of ion chromatography.
Exhaled vapours
Subjects will be asked to perform a single slow vital capacity breath in a one-way Teflon® bulb (Bio-VOC®
sampler, Markers International Ltd, Rhondda Cynon Taff, UK) which traps the last portion of exhaled breath
(Poli et al. 2005). This system allows the sampling of only one breath. After addition of Internal Standards
(I.S, n-heptane-d16 and styrene-d8 methanolic solution) the exhaled VOCs will be extracted using 75 µm-
Carboxen-PDMS SPME fibers (Supelco, Bellefonte, PA, USA). Analyses will be carried out in gas
chromatography mass spectrometry technique operating both in full scan (ion range 40-350 m/z) and in sim
(selected ion monitoring) mode.
Induced sputum
Sputum induction and analysis will be carried out following well standardised and published methods
(Cianchetti et al. 2004). Briefly, hypertonic saline (NaCl 4.5%) solution will be inhaled for 5 min periods up
to 15 min to induce sputum with an ultrasonic nebulizer. Before and every 5 min from the start of
nebulization, subjects will be asked to rinse their mouth and throat carefully to discard saliva and to try to
cough sputum into a container; FEV1 will be then measured. Nebulization will stop either after 15 min or
Codice Riferimento: 8509 Page 12 of 38
8
when FEV1 will fall by 20% or more from baseline. Sputum samples will be poured in to a Petri dish to select
more viscid and dense portions. Recovered plugs will be weighed and incubated for 15 min in a shaking bath
at 37° C with a volume of 0.1% DTT equal to four times the weight of selected portions. The suspension will
then be diluted with PBS reaching a final dilution of 1:20, filtered through a 53 µm nylon gauze to remove
debris and centrifuged at 400 g for 10 min. Supernatant will be collected and stored for further analysis. The
cell pellet will be resuspended in 1cc of PBS for viability and total cell count, then diluted to achieve a final
concentration of 0.75-1.0x106 cells/ml. Aliquots of the cell sospension will be cytocentrifuged and stained
with Diff-Quik for differential cell count. At least 300 inflammatory cells will be counted. Macrophage,
lymphocyte, neutrophil, eosinophil percentages will be expressed as percent of total inflammatory cells.
Biomarkers of in supernatant will be immunoassayed.
Fractioning of exhaled breath
The first months of this study will be devoted also to the development and validation of a new device which
will collect exhaled breath and EBC from the lower airways only, thus eliminating the first portion of exhaled
breath. The system will be equipped with a CO2 electronic valve which separate exhaled breath into two
subsequent aliquots. The system will overpass some of the recent concerns regarding exhaled breath
collection, such as the influence of ambient air on exhaled biomarker concentration and the pulmonary site
origin of exhaled substances.
Power of the study and statistical analysis
The sample size required for the study was calculated taking into account the mean and standard deviation
(SD) of FEV1 in selected published papers. The background of COPD population was calculated as the mean
among recently published studies about COPD (as absolute FEV1 values) and the SD as the mean of all SD.
The sample size was assessed considering a paired t-test with a beta value of 0.10 and a alpha value of
0.05. Considering a significant positive increase of 0.2 L in FEV1 values after therapy, the number of selected
subjects should be at least 50 (one sided). The data will be analyzed using SPSS 13.0 (SPSS, Chicago, IL,
USA) and PRISM 3.0 (Graphpad Software, San Diego, CA, USA).
Research Network
The research protocol will be based on a collaboration between the University of Parma and the Terme di
Monticelli. The project will be coordinated by the University of Parma. A Consortium Agreement will be
prepared by the coordinator and will be signed by all participants before the initiation of the project.
Antonio Mutti is the designated contact person for the group and will provide leadership in all activities of
the group. He will organize meetings and will have frequent exchanges with Gianfranco Gainotti, Medical
Director of Terme di Monticelli, who will be responsible for activities carried out in Monticelli.
Massimo Corradi (pulmonologist), coordinator, will be involved in all data and record management, monitor
the results of studies as they progress, preparing scientific reports. He will help to ensure that protocols are
performed to the best standards of clinical research, maximizing the opportunity for the patients to benefit
of modern and innovative approaches, with special attention to the subject's health, safety, and right to
Codice Riferimento: 8509 Page 13 of 38

9
privacy. He will contribute to the preparation of the manual of procedures, of the informed consent and of
the data collection forms. He will assist in the implementation of the data collection procedures which he will
monitor periodically. He will serve as primary contact for the other members of the Consortium and will
perform site visits to ensure that in all the sites the data collection procedures are performed according to
the protocol approved by the Ethics Committee and GCP criteria.
Feasibility
Preliminary data have been reported in rationale section.
PI’s expertise
Antonio Mutti. Graduated summa cum laude in Medicine and Surgery (1974), Specialist in Occupational
Medicine (1977), Resident (1974), then research fellow (1976), and established university researcher (1980),
winner of the competition for full professorship of Occupational Medicine at the University of Turin (The
session 1999), Professor of Occupational Medicine at the university in Parma (2000). Coordinator of the
Doctorate in Health Sciences (since 2004), he is Director of the post-graduate School of Occupational
Medicine (since 2008).
Assistant director at the Institute of Clinical Medicine and Nephrology (since 1991) and of the Department of
Clinical Medicine, Nephrology and Health Sciences (from 1996), Responsible of the Regional Reference
Center of Industrial Toxicology (since 1997). He has been Director of the Program "Clinical Innovation and
Applied Research" of the University Hospital of Parma (2000-2006).
Delegate of the Rector for International Relationships and Biomedical Research (1996-2000). Since 2000 he
is delegate of the Rector in the Committee for the assistance to the personnel of the University of Parma.
Member of several scientific societies, he has been Secretary (1990-96) and then Chairman (from 1996 to
2003) of the Scientific Committee on Occupational Toxicology, International Commission on Occupational
Health (ICOH). Currently, he is member of the ICOH Board, and President of the Section Emiliano-
Romagnola of the Italian Society of Occupational Medicine and Industrial Hygiene.
SCIENTIFIC ACTIVITY
Author of over 400 scientific publications, he has been Project Leader or local Coordinator of the followings
projects funded by the European Commission within the 5° Framework Programme: HELIOS, QLK4-1999-
01308; GEOPARKINSON, QLK4-1999-01133; RANTIV, QLK4-1999-01356; SUSCEPSTYRENE, QLK4-1999-
01368. In the 6° Framework Programme he has been local Coordinator of the project DEVNERTOX. As
Principal Investigator, he was awarded with a grant form the US NIH - NHLBI (R01-HL72323) for the project
"Metals in exhaled condensed breath as biomarkers of COPD" (2002-2007).
List of 5 publications from January 2003, pertinent to the proposal project.
1: Balbi B, Pignatti P, Corradi M, Baiardi P, Bianchi L, Brunetti G, Radaeli A, Moscato G, Mutti A, Spanevello A, Malerba M.Bronchoalveolar lavage, sputum and exhaled clinically relevant inflammatory markers: values in healthy adults. Eur Respir J. 2007 Oct;30(4):769-81. IF 5.349
Codice Riferimento: 8509 Page 14 of 38

10
2: Bonetto G, Corradi M, Carraro S, Zanconato S, Alinovi R, Folesani G, Da Dalt L, Mutti A, Baraldi E. Longitudinal monitoring of lung injury in children after acute chlorine exposure in a swimming pool. Am J Respir Crit Care Med. 2006 Sep 1;174(5):545-9. Epub 2006 Jun 8. IF 9.09 3: Mutti A, Corradi M, Goldoni M, Vettori MV, Bernard A, Apostoli P. Exhaled metallic elements and serum pneumoproteins in asymptomatic smokers and patients with COPD or asthma. Chest. 2006 May;129(5):1288-97. IF 4.143 4: Caglieri A, Goldoni M, Acampa O, Andreoli R, Vettori MV, Corradi M, Apostoli P, Mutti A. The effect of inhaled chromium on different exhaled breath condensate biomarkers among chrome-plating workers. Environ Health Perspect. 2006 Apr;114(4):542-6. IF 5.636
5. Corradi M, Rubinstein I, Andreoli R, Manini P, Caglieri A, Poli D, Alinovi R, Mutti A.Aldehydes in exhaled breath condensate of patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2003 May 15;167(10):1380-6. Epub 2003 Jan 9. IF 9.09
The Laboratory of Industrial Toxicology of the Department of Clinical Medicine, Nephrology and Health
Sciences of the University Hospital of Parma (Head Prof. A. Mutti) consists of 6,000 square feet of research
and office spaces located in the same building. The laboratory is located inside the University Hospital area
and is close to the Clinics. The Laboratory is fully equipped with all the suitable facilities for sample handling,
storage and preparation and has a long-term experience with the measurement of biomarkers.
The Laboratory of Industrial Toxicology of the University of Parma has been involved for several years in the
risk assessment for among groups exposed to chemical pollutants and carcinogenic agents. Human studies
have been characterised by the development and simultaneous use of appropriate markers of exposure (or
internal dose) and of early effects on the critical organ(s) and/or system(s), including the lung, the kidney,
the neuro-endocrine, the nervous, and the immune system. A trait common to all such studies has been the
assessment of dose-effect (response) relationships in humans. A broad spectrum of studies have been
carried out in the fields of pneumo, neuro- and nephro-toxicology, including the development and validation
of biomarkers to assess early changes attributable to environmental pollutants.
In addition to field studies in workers occupationally exposed to known or suspected oxidant pollutants,
neuro- and nephro-toxins, experimental models have been set up, with the specific aim of interpreting the
patho-physiological meaning of biomarkers applied during epidemiological investigations. The Laboratory has
also long experience in the study of the metabolism of xenobiotics, aimed at validating biomarkers of
exposure, and more recently in the application of biomarkers of susceptibility applied in studies on gene-
environment interactions.
Basic laboratory equipment:
− Gilson 305-307 high-pressure HPLC pumps equipped with a Gilson 234 autoinjector;
− Hewlett-Packard Series 1100 quaternary HPLC pump equipped with a 1100 Series autosampler;
− ESA 5200 Electrochemical detector for HPLC provided with high sensitivity analytical cells;
Codice Riferimento: 8509 Page 15 of 38

11
− Gilson 119 UV/VIS detector for HPLC;
− Perkin-Elmer 785 A UV/VIS detector for HPLC;
− Waters 474 Scanning Fluorescence detector for HPLC;
− Gilson Unipoint software for instrumental control, data acquisition and data integration;
− Perkin-Elmer Series 200 binary HPLC system coupled with a PE-Sciex API 365 triple-quadrupole
mass spectrometer equipped with ionspray and heated nebulizer interfaces;
− Hewlett-Packard HP 6890 gas chromatograph coupled with a HP 5973 mass spectrometric detector,
provided with a source for chemical ionization;
− Hewlett-Packard HP 6890 Plus+ gas chromatograph with flame ionization detector (FID) and
electron-capture detector (ECD);
− Hewlett-Packard HP 7694 Head-space autosampler;
− CTC Analytics COMBI PAL autoinjector and SPME autosampler;
− Protofluor-Z fluorimeter;
− Beckman DU 640 UV-VIS spectrophotometer ;
− Varian 220Z Electrothermal atomic absorption spectrometer with fast Zeeman background
correction;
− Cells for horizontal and vertical electrophoresis;
− Transphor LKB2005 electroblotting unit;
− Equipment for bi-dimensional electrophoresis;
− Pharmacia Phast-System for microgel electrophoresis;
− Termostatic circulator LKB 2219-Multitemp II;
− BIORAD Genecycler Thermal cycler (24 wells);
− Gel DOC 1000: imaging system;
− BIORAD iCycler Thermal cycler (96 wells);
− Light Cycler Roche with real-time acquisition program;
− Beckman Allegra 21R Refrigerated centrifuge;
− Beckman Microfuge 18Microcentrifuge;
− TECAN robotic sample processor 5031;
− Titertek Multiscan Plus Multi-channel spectrophotometer;
− Horizontal shaker for ELISA plates;
− Incubator;
− Heraeus HERA cell CO2-incubator;
− Pharmacia FPLC system for protein chromatography;
− Olympus CK40-RFL inverted microscope equipped with a JVC Colour Video Monitor, an Olympus
digital camera and a device for fluorescence imaging;
− Spectrophotometer Serozyme II
− Refrigerators and freezers
− Cold room
− Laboratory miscellaneous items
Codice Riferimento: 8509 Page 16 of 38
12
Each key person has his/her computer with Internet connection and up-to-date software. Each key person
has his/her own office in the same building.
Relevant references (in alphabetic order)
American Thoracic Society; European Respiratory Society. ATS/ERS recommendations for standardized procedures for the online and offlinemeasurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am J Respir Crit Care Med. 2005 Apr 15;171(8):912-30. Bach PB et al. Variations in lung cancer risk amongsmokers. J Natl Cancer Inst 2003;95:470–8. Bacha ZA et al. Saliva cotinine and exhaled carbon monoxide levels in natural environment waterpipe smokers. Inhal Toxicol. 2007 Jul;19(9):771-7. Barnes PJ et al. Chronic obstructive pulmonary disease: molecular and cellular mechanisms. Eur Respir J. 2003 Oct;22(4):672-88. Bliss A et al. Lung cancer incidence among American Indians and Alaska Natives in the United States, 1999-2004. Cancer. 2008 Sep 1;113(5 Suppl):1168-78. Braga PC et al. Antioxidant effect of sulphurous thermal water on human neutrophil bursts: chemiluminescence evaluation. Respiration. 2008;75(2):193-201. Epub 2007 Sep 5. Caramori G et al. Is there a difference between chronic airway inflammation in chronic severe asthma and chronic obstructive pulmonary disease? Curr Opin Allergy Clin Immunol. 2005 Feb;5(1):77-83. Cazzola M et al. American Thoracic Society, European Respiratory Society Task Force on outcomes of COPD. Outcomes for COPD pharmacological trials: from lung function to biomarkers. Eur Respir J. 2008 Feb;31(2):416-69. Chen YH et al. Endogenous hydrogen sulfide in patients with COPD. Chest. 2005 Nov;128(5):3205-11. Cianchetti S et al. Granulocyte markers in hypertonic and isotonic saline-induced sputum of asthmatic subjects. Eur Respir J. 2004 Dec;24(6):1018-24. Corradi M et al. Increased nitrosothiols in exhaled breath condensate in inflammatory airway diseases. Am J Respir Crit Care Med. 2001 Mar;163(4):854-8. Corradi M et al Comparison between exhaled and sputum oxidative stress biomarkers in chronic airway inflammation. Eur Respir J. 2004 Dec;24(6):1011-7. Dal Negro R et al. The burden of COPD in Italy: results from the Confronting COPD survey. Respir Med. 2003 Mar;97 Suppl C:S43-50. Du al The possible role of hydrogen sulfide as a smooth muscle cell proliferation inhibitor in rat cultured cells. Heart Vessels 2004;19,75-80 Etzel C et al. Development and Validation of a Lung Cancer Risk Prediction Model for African-Americans. Cancer Prev Res 2008;1(4) September 2008 Geng, B et al . Endogenous hydrogen sulfide regulation of myocardial injury induced by isoproterenol. Biochem Biophys Res Commun 2004;318,756-763 Horváth I et al. Exhaled breath condensate: methodological recommendations and unresolved questions. Eur Respir J. 2005 Sep;26(3):523-48. Hosoki et al. The possible role of hydrogen sulfide as an endogenous smooth muscle relaxant in synergy with nitric oxide. Biochem Biophys Res Commun 1997;237,527-531
Codice Riferimento: 8509 Page 17 of 38
13
Houghton AM et al. Common origins of lung cancer and COPD. Nat Med. 2008 Oct;14(10):1023-4. Houston MC. The role of mercury and cadmium heavy metals in vascular disease, hypertension, coronary heart disease, and myocardial infarction. Altern Ther Health Med. 2007 Mar-Apr;13(2):S128-33. Hurd S et al. Global Initiative for Chronic Obstructive Lung Diseases (GOLD). Pulm Pharmacol Ther. 2002;15(4):353-5. Kelly GS. Clinical applications of N-acetylcysteine. Altern Med Rev. 1998 Apr;3(2):114-27. Kharitonov SA et al,. Dose-dependent onset and cessation of action of inhaled budesonide on exhaled nitric oxide and symptoms in mild asthma. Thorax. 2002 Oct;57(10):889-96. Miller MR et al. Standardisation of spirometry. Eur Respir J. 2005 Aug;26(2):319-38. Mishra S et al. Lead detoxification by coontail (Ceratophyllum demersum L.) involves induction of phytochelatins and antioxidant system in response to its accumulation. Chemosphere. 2006 Nov;65(6):1027-39. Epub 2006 May 8. Mutti A et al. Exhaled metallic elements and serum pneumoproteins in asymptomatic smokers and patients with COPD or asthma. Chest. 2006 May;129(5):1288-97. Papi A. COPD increases the risk of squamous histological subtype in smokers who develop non-small cell lung carcinoma. Thorax. 2004 Aug;59(8):679-81. Paredi P et al. Analysis of expired air for oxidation products. Am J Respir Crit Care Med. 2002 Dec 15;166(12 Pt 2):S31-7. Patrick L. Toxic metals and antioxidants: Part II. The role of antioxidants in arsenic and cadmium toxicity. Altern Med Rev. 2003 May;8(2):106-28. Pauwels RA et al. Burden and clinical features of chronic obstructive pulmonary disease (COPD). Lancet. 2004 Aug 14;364(9434):613-20. Pellegrini M et al. Effect of inhalation of thermal water on airway inflammation in chronic obstructive pulmonary disease. Respir Med. 2005 Jun;99(6):748-54. Epub 2004 Dec 13. Poli D. Exhaled volatile organic compounds in patients with non-small cell lung cancer: cross sectional and nested short-term follow-up study. Respir Res. 2005 Jul 14;6:71. Puckett JL et al. Partitioned exhaled nitric oxide to non-invasively assess asthma.Respir Physiol Neurobiol. 2008 Jul 31. Quig D. Cysteine metabolism and metal toxicity. Altern Med Rev. 1998 Aug;3(4):262-70. Rabe KF et al. Update in chronic obstructive pulmonary disease 2006. Am J Respir Crit Care Med. 2007 Jun 15;175(12):1222-32. Rugstad HE. Metallothionein--a unique protein with multiple detoxifying properties? Eur Surg Res. 1984;16 Suppl 2:102-12. Staffieri A et al. Sulphurous-arsenical-ferruginous (thermal) water inhalations reduce nasal respiratory resistance and improve mucociliary clearance in patients with chronic sinonasal disease: preliminary outcomes. Acta Otolaryngol. 2007 Jun;127(6):613-7. Tiryakioglu M et al. Antioxidant defense system and cadmium uptake in barley genotypes differing in cadmium tolerance. J Trace Elem Med Biol. 2006;20(3):181-9. Epub 2006 Jun 2.
Codice Riferimento: 8509 Page 18 of 38

14
Valko M et al. Metals, toxicity and oxidative stress. Curr Med Chem. 2005;12(10):1161-208. Vestergaard M et al. Chelation of cadmium ions by phytochelatin synthase: role of the cysteine-rich C-terminal. Anal Sci. 2008 Feb;24(2):277-81. Wang, R. Two’s company, three’s a crowd: can H2S be the third endogenous gaseous transmitter? FASEB J 2002;16,1792-1798
Collaborations
The sample size requested to recruit 50 patients. Considering that 24 months will be devoted to patients’
recruiting, 25 patients per year could be easily recruited. A formal letter of collaboration from Terme di
Monticelli is attached.
The study will be facilitated by the short distance between the Thermal Institute and the University Hospital
of Parma (10 km): personnel from the University will be on site in Monticelli to assess patients and to collect
biological samples. Therefore, for those biological markers which lack stability in frozen samples (e.g. H2O2,
VOCs), the assay will be done within 24 hours.
Potential limitations of the study
This study is not placebo controlled, therefore the therapeutical conclusions will be tapered by this bias.
However, it is really difficult to perform a placebo controlled study as sulphur water has a typical smell,
making the creation of a placebo impossible (especially in a thermal institute).
One possible solution should have been ask to the patient to attend clinic visit at the hospital (rather then
attending thermal institute) administrating them, for instance, nebulized thermal water and placebo. Again, a
part from difficulties in creating placebo, we do think that, in order to understand the effect of a complete
cycle of thermal water inhalation on putative biomarkers, we should mimic the same situation to whom
patients refer to.
Therefore, the study is not aimed at demonstrating a therapeutical efficacy of thermal water inhalation, but
rather at verifying whether a short term inhalation program with thermal sulphurous water is able to modify
biomarkers of tobacco/environmental exposure (target tissue dose) and possibly associated markers of
pulmonary effect in COPD patients (markers of lung pathobiology and lung function tests).
The sample size was calculated on the basis of function consideration, and we do know that spirometry,
being effort related, may be biased by the lack of placebo. However, this is not the case for inflammatory
biomarkers, which cannot (or at least a small contribution) be influenced by the lack of placebo.In order to
ensure an objective assessment, all biological analysis will be done by personnel who is not aware of
patients codes. To this end, we will study only those biomarkers which have been proven to be reproducible
over weeks. However, an unpredictable day to day variation can not be totally excluded. Therefore, in this
Codice Riferimento: 8509 Page 19 of 38
15
protocol we will also recruit 10 clinically stable COPD patients (with similar characteristics than
those receiving thermal treatment) volunteering to perform three biological samplings at the
clinic and at the same time points than that in COPD patients receiving thermal treatment. This
will be useful in order to take into account a possible biomarker variability.
Finally, we can not exclude that some changes in biomarker levels may occur weeks after the end of thermal
treatment. Ideally, a fourth sampling should have been done, but this is difficult to be apply in practice, as
the majority of the persons who refer to thermal institutes are not resident in Parma. For those COPD
patients who leave around Parma will be asked to re-assessed one month later.
Codice Riferimento: 8509 Page 20 of 38

16
Timetable of the project
A. Study Planning covers Semester 1 and includes:
1) definition of the study protocol and its approval by all partners;
2) clearance from ethical committees;
3) questionnaire preparation and distribution to all involved units;
4) method validation: all the preliminary measures necessary to validate the analyses planned in this study.
At the end of this phase, a Plan of Analysis will be produced and shared (beginning of Semester 2): it will
contain the approved study protocol, a copy of the standard questionnaire, details about method validation
and a plan of future statistical analyses.
B. Recruitment of Patients: it will cover 4 semesters (semester 2 – semester 5) and comprehends:
1) sample collection from patients;
2) sample storage and shipping to all involved groups;
3) laboratory tests.
Two interim reports (at the beginning of semester 3 and at the end of semester 4) containing preliminary
data will be created and shared. A final statistical report with both sets will be evaluated and shared in
Semester 5, at the end of patient’s recruitment. It will contain all statistical analyses to be included in the
final clinical report and to be considered in publication plan.
A. Evaluation of results
1. A central database available for all partners will be created (Access, Microsoft) and shared by all
partners (internet website with restricted access – Semester 2). It will contain all the masks provided by
the study protocol and questionnaire.
2. Central database will be continuously cleaned and updated from semester 2 to semester 5. “Ad interim”
reports and final statistical report will be created on the basis of the data contained in it.
3. On the basis of the final statistical report, dissemination of knowledge will imply the collection of all the
main results in a final clinical report (Semester 5-6). It will contain an introduction, a description of data
and a discussion. Clinical report will be shared and discussed among all partners and a public version of
it will be published on the website. A final database containing all the literature of interest published
from 2008 to 2010 will be finally created and shared.
4. Publication plan (Semester 6): main results will be published in one or more international scientific
journals.
Codice Riferimento: 8509 Page 21 of 38

17
Figure 1. Working hypothesis
Disease
(COPD)
Restoring SH
groups
SH group
depletion
detoxification
activity
Toxic m
etals in tobacco smoke
Transition elements
(Cr, Cu, Mn)
Heavy m
etals
(Cd, Pb, Hg)
Strong oxidants
Oxidative stress
High affinity
for SH groups
Cell injury
Inflammation
Sulphur
therm
al water
Codice Riferimento: 8509 Page 22 of 38

18
Codice Riferimento: 8509 Page 23 of 38

PERSONNEL INVOLVED IN THE RESEARCH
Name Date of birth Role on project FellowshipRequired
Effort onproject
Man/yeareffort
Professore Antonio Mutti 10/03/1949 Principal Investigator 20 0,2
Dottore Massimo Corradi 25/08/1970 Researcher 30 0,3
Dottore Matteo Goldoni 04/05/1973 Post-Doc 20.000,00 100 1
Dottoressa Paola Manini 22/02/1967 Post-Doc 40 0,4
Dottoressa Rossella Alinovi 15/10/1960 Technician 30 0,3
Dottoressa Olga Acampa 13/05/1976 PhD Student 80 0,8
Dottoressa Diana Poli 23/02/1974 Post-Doc 20.000,00 100 1
Dottore Gianfranco Gainotti 15/10/1948 Investigator 20 0,2
Dottoressa Olga Touranjanin 16/04/1970 Fellow 20 0,2
Dottore Andrea Caglieri 23/04/1975 Post-Doc 30 0,3
Dottoressa Roberta Andreoli 14/02/1972 Post-Doc 30 0,3
Total Man/Year on project 5
Codice Riferimento: 8509 Page 24 of 38

BUDGET FORM
2008 2009 2010 Total
Research costs 10.000,00 € 15.000,00 € 10.000,00 € 35.000,00 €
Fellowships 40.000,00 € 40.000,00 € 40.000,00 € 120.000,00 €
Indirect costs 5.000,00 € 5.500,00 € 5.000,00 € 15.500,00 €
Subtotal 55.000,00 € 60.500,00 € 55.000,00 € 170.500,00 €
Overhead 4.400,00 € 4.840,00 € 4.400,00 € 13.640,00 €
Total 59.400,00 € 65.340,00 € 59.400,00 € 184.140,00 €
Justificatons
RESEARCH COSTSThe following supplies are requested:-€ 3,000 for solvents and reagents;-€ 5,000 for HPLC columns-€ 4,000 for ELISA kits-€ 2,000 for tubes, pipettes, disposable glassware-€ 2,000 for disposable mouthpiece and EBC collecting devices.-€ 2,000 for travel expenses-€ 1,000 for is requested to cover advertising and photocopying costs, computer supplies and preparation of slides and manuscripts forpublication.-€ 8.000 for exhaled NO analyzer-€ 8.000 for two Turbo Deccs condensers
Total € 35.000
FELLOWSHIPS COSTSDiana poli. She will devote 100 % effort to perform measurements on exhaled breath and induced sputum by gas chromatographycoupled with mass spectrometry,and for the development of novel candidate markers possibly emerging from the study.Salary requested as post-doc (professional).
Goldoni Matteo. He will devote 100 % effort to develop a system to fraction exhaled breath and to perform elemental analysis of EBC.Salary requested as as post-doc (professional).
INDIRECT COSTSThe Department of Clinical Medicine, Nephrology and Health Sciences will charge indirect costs of 10 %, covering costs related totelephone, instrument maintenance, and facilities.
OVERHEAD COSTSThe University of Parma will charge overhead costs of 8 %, covering costs related to facilities, insurance, percentage of salaries andother administrative costs incurred by the Central Administration.
Codice Riferimento: 8509 Page 25 of 38

University of Parma
Antonio Mutti (MD, Full Professor, Occupational Medicine physician) is the designated contact person for
the group and will provide leadership in all activities of the group. He will organize meetings and will have
frequent exchanges with Gianfranco Gainotti, who will be responsible for activities carried out in Monticelli.
Massimo Corradi (MD, Pulmonologist), coordinator, will be involved in all data and record management,
monitor the results of studies as they progress, preparing scientific reports. He will help to ensure that
protocols are performed to the best standards of clinical research, maximizing the opportunity for the
patients to benefit of modern and innovative approaches, with special attention to the subject's health,
safety, and right to privacy. He will contribute to the preparation of the manual of procedures, of the
informed consent and of the data collection forms. He will assist in the implementation of the data collection
procedures which he will monitor periodically. He will serve as primary contact for the other members of the
Consortium and will perform site visits to ensure that in all the sites the data collection procedures are
performed according to the protocol approved by the Ethics Committee and GCP criteria.
Rossella Alinovi (Biologist) will be responsible for immunoassays in EBC and induced sputum processing
and analysis.
Diana Poli (Chemist, post doc), will be in charge of GC-MS analyses of VOCs.
Matteo Goldoni (Physic, post doc), will be responsible for elemental analysis in EBC and data storage and
analysis.
Paola Manini (Chemist, post doc) will be in charge of LC-MS/MS analysis in EBC.
Olga Acampa (MD, Occupational Medicine Physician, PhD student) will be in charge of clinical evaluation
and biological samplings.
Roberta Andreoli (Chemist, post doc) will be in charge of LC-MS/MS and for ion chromatographic analysis
of sulphurous compounds.
Andrea Caglieri (Biologist, post doc) will be in charge of colorimetric analysis of selected compounds in
EBC and induced sputum.
Terme di Monticelli
Gianfranco Gainotti (MD, Internal medicine specialist, medical director of Terme di Monticelli), will
supervise all medical activities carried out in Terme di Monticelli.
Touranjianin Olga (MD,Medical Hydrology specialist), will be in charge of patient selection and
recruitment.
DESCRIPTION OF THE WORK FOR EVERY UNIT OF PERSONNEL
Codice Riferimento: 8509 Page 26 of 38

BIOGRAPHICAL SKETCH
BIOGRAPHICAL SKETCH
NameProfessore Mutti Antonio
PositionMD
Date of birth10/03/1949
Education and Training (include degrees and post-doctoral training)
Institution and Location Degree Year (from/to) Field of Study
University of Parma - Parma MD 1968/1974 Occupational Medicine
University of Parma - Parma Specialist inOccupationalMedicine
1974/1978 Occupational Medicine
RESEARCH AND PROFESSIONAL EXPERIENCE
Year (from/to) Institution Position City Country
1974/1980 University of Parma MD Fellow Parma Italy
1976/1980 University of Parma Research fellow Parma Italy
1980/2000 University of Parma Senior Researcher Parma Italy
2000/2008 University of Parma Full Professor Parma Italy
Codice Riferimento: 8509 Page 27 of 38
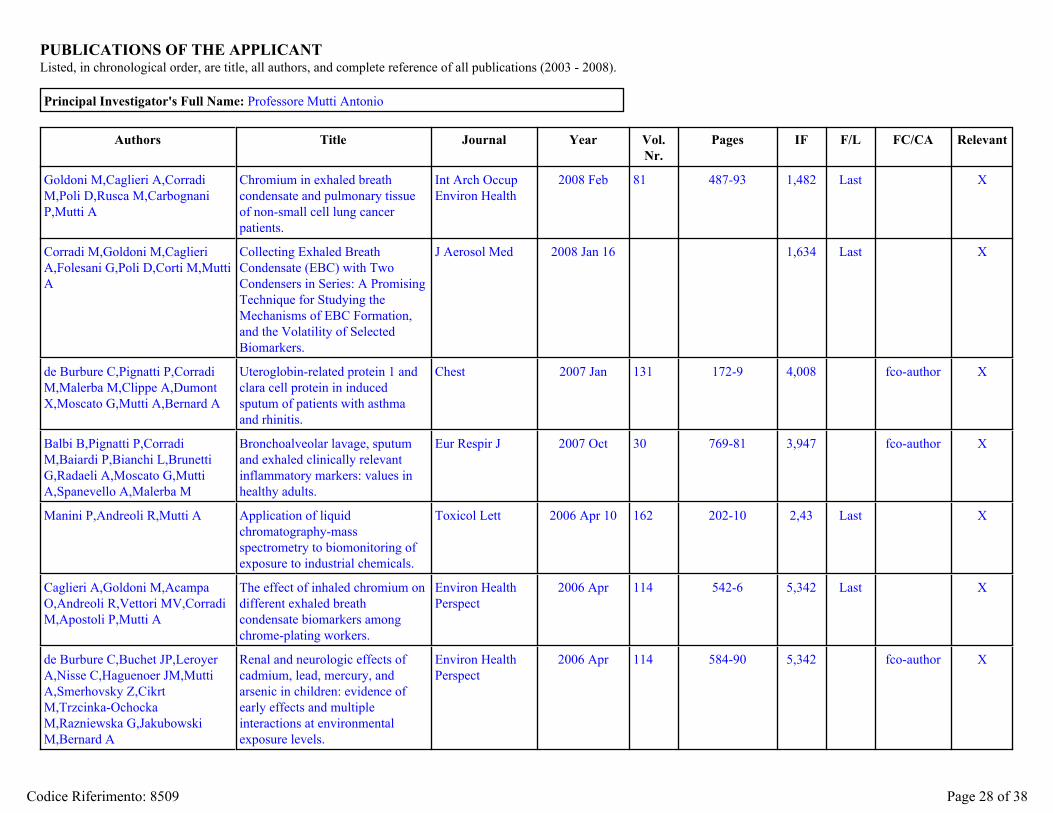
PUBLICATIONS OF THE APPLICANTListed, in chronological order, are title, all authors, and complete reference of all publications (2003 - 2008).
Principal Investigator's Full Name: Professore Mutti Antonio
Authors Title Journal Year Vol.Nr.
Pages IF F/L FC/CA Relevant
Goldoni M,Caglieri A,CorradiM,Poli D,Rusca M,CarbognaniP,Mutti A
Chromium in exhaled breathcondensate and pulmonary tissueof non-small cell lung cancerpatients.
Int Arch OccupEnviron Health
2008 Feb 81 487-93 1,482 Last X
Corradi M,Goldoni M,CaglieriA,Folesani G,Poli D,Corti M,MuttiA
Collecting Exhaled BreathCondensate (EBC) with TwoCondensers in Series: A PromisingTechnique for Studying theMechanisms of EBC Formation,and the Volatility of SelectedBiomarkers.
J Aerosol Med 2008 Jan 16 1,634 Last X
de Burbure C,Pignatti P,CorradiM,Malerba M,Clippe A,DumontX,Moscato G,Mutti A,Bernard A
Uteroglobin-related protein 1 andclara cell protein in inducedsputum of patients with asthmaand rhinitis.
Chest 2007 Jan 131 172-9 4,008 fco-author X
Balbi B,Pignatti P,CorradiM,Baiardi P,Bianchi L,BrunettiG,Radaeli A,Moscato G,MuttiA,Spanevello A,Malerba M
Bronchoalveolar lavage, sputumand exhaled clinically relevantinflammatory markers: values inhealthy adults.
Eur Respir J 2007 Oct 30 769-81 3,947 fco-author X
Manini P,Andreoli R,Mutti A Application of liquidchromatography-massspectrometry to biomonitoring ofexposure to industrial chemicals.
Toxicol Lett 2006 Apr 10 162 202-10 2,43 Last X
Caglieri A,Goldoni M,AcampaO,Andreoli R,Vettori MV,CorradiM,Apostoli P,Mutti A
The effect of inhaled chromium ondifferent exhaled breathcondensate biomarkers amongchrome-plating workers.
Environ HealthPerspect
2006 Apr 114 542-6 5,342 Last X
de Burbure C,Buchet JP,LeroyerA,Nisse C,Haguenoer JM,MuttiA,Smerhovsky Z,CikrtM,Trzcinka-OchockaM,Razniewska G,JakubowskiM,Bernard A
Renal and neurologic effects ofcadmium, lead, mercury, andarsenic in children: evidence ofearly effects and multipleinteractions at environmentalexposure levels.
Environ HealthPerspect
2006 Apr 114 584-90 5,342 fco-author X
Codice Riferimento: 8509 Page 28 of 38

Authors Title Journal Year Vol.Nr.
Pages IF F/L FC/CA Relevant
Mutti A,Corradi M,GoldoniM,Vettori MV,Bernard A,ApostoliP
Exhaled metallic elements andserum pneumoproteins inasymptomatic smokers andpatients with COPD or asthma.
Chest 2006 May 129 1288-97 4,008 First X
Carnevali S,Luppi F,D'ArcaD,Caporali A,Ruggieri MP,VettoriMV,Caglieri A,AstancolleS,Panico F,Davalli P,MuttiA,Fabbri LM,Corti A
Clusterin decreases oxidativestress in lung fibroblasts exposedto cigarette smoke.
Am J Respir CritCare Med
2006 Aug 15 174 393-9 8,689 fco-author X
Bonetto G,Corradi M,CarraroS,Zanconato S,Alinovi R,FolesaniG,Da Dalt L,Mutti A,Baraldi E
Longitudinal monitoring of lunginjury in children after acutechlorine exposure in a swimmingpool.
Am J Respir CritCare Med
2006 Sep 1 174 545-9 8,689 fco-author X
Olivieri M,Talamini G,CorradiM,Perbellini L,Mutti A,TantucciC,Malerba M
Reference values for exhaled nitricoxide (reveno) study.
Respir Res 2006 Jun 30 7 94 2,682 X
Goldoni M,Caglieri A,PoliD,Vettori MV,Corradi M,ApostoliP,Mutti A
Determination of hexavalentchromium in exhaled breathcondensate and environmental airamong chrome plating workers.
Anal Chim Acta 2006 Mar 15 562 229-235 2,76 Last X
Manini P,De Palma G,AndreoliR,Poli D,Mozzoni P,FolesaniG,Mutti A,Apostoli P
Environmental and biologicalmonitoring of benzene exposure ina cohort of Italian taxi drivers.
Toxicol Lett 2006 Dec 1 167 142-51 2,43 Last
Corradi M,Mutti A Exhaled breath analysis: fromoccupational to respiratorymedicine.
Acta Biomed 2005 76Suppl 2
20-9 Last X
Poli D,Manini P,AndreoliR,Franchini I,Mutti A
Determination of dichloromethane,trichloroethylene andperchloroethylene in urine samplesby headspace solid phasemicroextraction gaschromatography-massspectrometry.
J Chromatogr BAnalyt TechnolBiomed Life Sci
2005 Jun 5 820 95-102 2,391 Last X
Poli D,Carbognani P,CorradiM,Goldoni M,Acampa O,BalbiB,Bianchi L,Rusca M,Mutti A
Exhaled volatile organiccompounds in patients withnon-small cell lung cancer: crosssectional and nested short-termfollow-up study.
Respir Res 2005 Jul 14 6 71 2,682 Last X
Codice Riferimento: 8509 Page 29 of 38
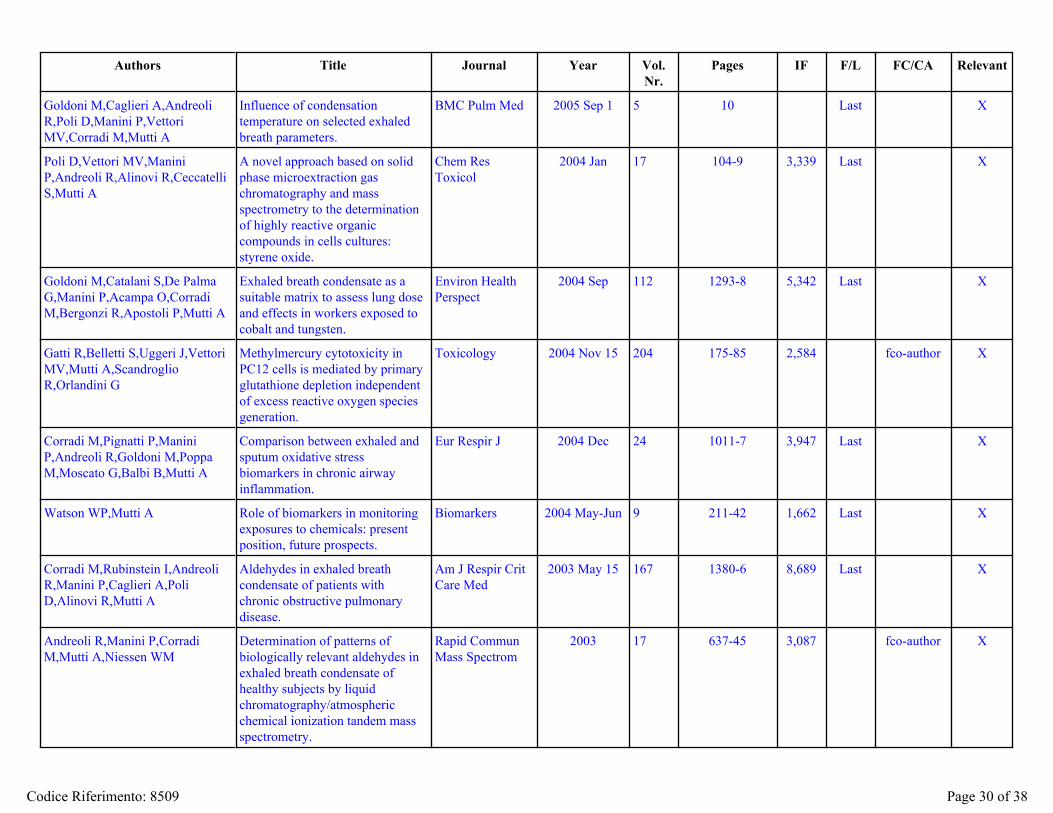
Authors Title Journal Year Vol.Nr.
Pages IF F/L FC/CA Relevant
Goldoni M,Caglieri A,AndreoliR,Poli D,Manini P,VettoriMV,Corradi M,Mutti A
Influence of condensationtemperature on selected exhaledbreath parameters.
BMC Pulm Med 2005 Sep 1 5 10 Last X
Poli D,Vettori MV,ManiniP,Andreoli R,Alinovi R,CeccatelliS,Mutti A
A novel approach based on solidphase microextraction gaschromatography and massspectrometry to the determinationof highly reactive organiccompounds in cells cultures:styrene oxide.
Chem ResToxicol
2004 Jan 17 104-9 3,339 Last X
Goldoni M,Catalani S,De PalmaG,Manini P,Acampa O,CorradiM,Bergonzi R,Apostoli P,Mutti A
Exhaled breath condensate as asuitable matrix to assess lung doseand effects in workers exposed tocobalt and tungsten.
Environ HealthPerspect
2004 Sep 112 1293-8 5,342 Last X
Gatti R,Belletti S,Uggeri J,VettoriMV,Mutti A,ScandroglioR,Orlandini G
Methylmercury cytotoxicity inPC12 cells is mediated by primaryglutathione depletion independentof excess reactive oxygen speciesgeneration.
Toxicology 2004 Nov 15 204 175-85 2,584 fco-author X
Corradi M,Pignatti P,ManiniP,Andreoli R,Goldoni M,PoppaM,Moscato G,Balbi B,Mutti A
Comparison between exhaled andsputum oxidative stressbiomarkers in chronic airwayinflammation.
Eur Respir J 2004 Dec 24 1011-7 3,947 Last X
Watson WP,Mutti A Role of biomarkers in monitoringexposures to chemicals: presentposition, future prospects.
Biomarkers 2004 May-Jun 9 211-42 1,662 Last X
Corradi M,Rubinstein I,AndreoliR,Manini P,Caglieri A,PoliD,Alinovi R,Mutti A
Aldehydes in exhaled breathcondensate of patients withchronic obstructive pulmonarydisease.
Am J Respir CritCare Med
2003 May 15 167 1380-6 8,689 Last X
Andreoli R,Manini P,CorradiM,Mutti A,Niessen WM
Determination of patterns ofbiologically relevant aldehydes inexhaled breath condensate ofhealthy subjects by liquidchromatography/atmosphericchemical ionization tandem massspectrometry.
Rapid CommunMass Spectrom
2003 17 637-45 3,087 fco-author X
Codice Riferimento: 8509 Page 30 of 38

Authors Title Journal Year Vol.Nr.
Pages IF F/L FC/CA Relevant
de Burbure C,Buchet JP,BernardA,Leroyer A,Nisse C,HaguenoerJM,Bergamaschi E,Mutti A
Biomarkers of renal effects inchildren and adults with lowenvironmental exposure to heavymetals.
J Toxicol EnvironHealth A
2003 May 9 66 783-98 Last X
Mutti A,Corradi M,Rubinstein I Reporting data on exhaled breathcondensate.
Am J Respir CritCare Med
2003 Sep 15 168 719; authorreply 719
8,689 First X
Buzio L,De Palma G,MozzoniP,Tondel M,Buzio C,FranchiniI,Axelson O,Mutti A
Glutathione S-transferases M1-1and T1-1 as risk modifiers forrenal cell cancer associated withoccupational exposure tochemicals.
Occup EnvironMed
2003 Oct 60 789-93 1,934 Last X
Codice Riferimento: 8509 Page 31 of 38

EXISTING/PENDING SUPPORT
Funding Agency Project Title From To Amount
Ministero della Salute -Istituto Superiore per laPrevenzione e laSicurezza del Lavoro
“Novel approaches to assess the carginogenicpotential of genotoxic pollutants”
2008 2011 € 118.001,00
Ministero della Salute -Istituto Superiore per laPrevenzione e laSicurezza del Lavoro
“Sviluppo di nuovi indicatori per la valutazione dieffetti precoci polmonari in soggettiprofessionalmente esposti a sostanze in grado diindurre una patologia infiammatoria delle vie aeree:analisi dell’aria esalata”
2008 2011 € 34.629,00
Ministero dell’Istruzione,dell’Università e dellaRicerca - PRIN
“Traslocazione di nanomateriali dalle vie respiratoriedi ratti trattati per instillazione tracheale ebiomarcatori di stress ossidativo locale e sistemico”
2008 2010 € 62.871,00
Codice Riferimento: 8509 Page 32 of 38

1. Ministero della Salute - Istituto Superiore per la Prevenzione e la Sicurezza del Lavoro “Novel approaches to assess the carginogenic potential of genotoxic pollutants”
from 15/02/2008 to 15/02/2011
€ 118.001,00
Antonio Mutti, 10 % of time committed Massimo Corradi, 10 % of time committed Roberta Andreoli, 50 % of time committed Giuseppina Folesani, 50 % of time committed 2. Ministero della Salute - Istituto Superiore per la Prevenzione e la Sicurezza del Lavoro
“Sviluppo di nuovi indicatori per la valutazione di effetti precoci polmonari in soggetti professionalmente esposti a sostanze in grado di indurre una patologia infiammatoria delle vie aeree: analisi dell’aria esalata”
from 15/02/2008 to 15/02/2011
€ 34.629,00
Antonio Mutti, 10 % of time committed Massimo Corradi, 10 % of time committed Andrea Caglieri, 50 % of time committed Paola Mozzoni, 50 % of time committed 3. Ministero dell’Istruzione, dell’Università e della Ricerca - PRIN
“Traslocazione di nanomateriali dalle vie respiratorie di ratti trattati per instillazione tracheale e biomarcatori di stress ossidativo locale e sistemico”
from 22/09/2008 to 30/10/2010
€ 62.871,00
Antonio Mutti, 10 % of time committed Massimo Corradi, 10 % of time committed Sara Tagliaferri, 50 % of time committed Domenica Mangeri, 50 % of time committed
EXISTING/PENDING SUPPORT JUSTIFICATION
Codice Riferimento: 8509 Page 33 of 38

UNDESIRABLE REVIEWERS
Name Institution - Department Address E-mail
Prof. Montuschi Paolo Catholic University of the Sacred Heart- Department of Pharmacology
Largo F. Vito, 1,00168 Italy (Roma)
Codice Riferimento: 8509 Page 34 of 38

BIO-ETHICAL REQUIREMENTS
Does the proposed research involve:
HUMAN EXPERIMENTATION YES X NO
Human experimentation includes involvement of human subjects and other issues with ethical implications.If yes include clearance from the competent ethical committee (as addendum E). If approval of the ethical committee is not available atmoment of submission, include as addendum E, a signed statement from the proponent pledging to obtain it before the start of theresearch. AIRC will not erogate funds in the absence of an ethical committee clearance.
ANIMAL EXPERIMENTATION YES NO X
If yes the following statement will have to be signed in the paper submission:The Ethical Committee for animal use in cancer research has evaluated the proposal.The Committee considers that the preliminary results, obtained in in-vitro experiments deserve a preclinical study.The procedures related to animal use are accurately described in the proposal and conform to all regulations protecting animals used forresearch purposes, including those of the DL 116/92. The experiments described in the proposal will be performed following the detailedInternal Regulation drawn-up according to: Workamn P., et al. (1998) United Kingdom Coordinating Committee on Cancer Research(Guidelines for the welfare of animals in experimental neoplasia. Br. J. Cancer 77: 1-10).
Date:21/10/2008
Name of PIProfessore Mutti Antonio
Signature
Codice Riferimento: 8509 Page 35 of 38

Addendum
B - [Form
al letter of collaboration]
Codice R
iferimento: 8509
Page 36 of 38

Addendum C - [Institutional indirect cost/overhead]
Codice Riferimento: 8509 Page 37 of 38

Addendum D - [Clearance form ethical commitee]
Codice Riferimento: 8509 Page 38 of 38
Top Related