![Sphincter saving and abdomino-perineal resections ... · patients continues to require abdominoperineal resection [2]. The aim of this study was to explore the possible advantages](https://static.fdocuments.net/doc/165x107/5f6f697a921db411ba3706ce/sphincter-saving-and-abdomino-perineal-resections-patients-continues-to-require.jpg)







Languages
Pages
Legal


Procedures
Advanced Format:
Abdominoperineal Resection

Definition/Purpose of Procedure
• Through combined abdominal and perineal incisions, the anus, rectum, and sigmoid colon are removed en bloc.
• Also called Miles Resection
• The proximal end of the bowel is exteriorized thru a separate stab wound as a colostomy. The distal end is pushed into the hollow of the sacrum and removed via perineum
• Performed to treat cancer of the lower rectum—and diseases are too low for use of EEA stapling devices

Pathophysiology
• Cancer of lower rectum: usually the lower third of the rectum, but may extend into the anal canal
• The sigmoid colon is the primary site of colon cancer and is the section of colon most susceptible to volvulus.

Abdominoperineal Resection

Surgical Intervention:Special Considerations
• Patient Factors– Requires the formation of a permanent colostomy in the
abdominal wall for drainage of bowel contents– An indwelling foley catheter will be inserted and
attached to closed drainage– Upper body thermia blanket
• Room Set-up– Organize the room for space! If 2 teams, one works at
abdomen and one works on perineal portion (ABD: ST stands slightly behind assistant and must take special care not to contaminate! Perineal: ST Stands next to surgeon)

Surgical Intervention: Positioning
• Position during procedure: when performed as two simultaneous procedures, modified lithotomy
• Supplies and equipment– Probable Allen stirrups or “high impact knee-crutch stirrups” for
positioning—can be adjusted for knee flexion and extension; Be sure to have additional padding (gel or foam)
– Sequential Compression Devices
• Special considerations: high risk areas: cause pressure to back of knees and lower extremities and may jeopardize the popliteal vessels and nerves

Surgical Intervention: Draping/Incision
• Types of drapes (Depends on position)– Laparotomy and perineal: Under buttocks, folded
towels, Lap T-sheet (cut hole for perineal exposure)
• Order of draping– Abdomen and perineal
• Special considerations: “clean” closure of abdomen requires regowning, regloving, redraping, and a new minor tray
• State/Describe incision: Abdominal midline

Surgical Intervention: Supplies
• Specific– Suture: Dexon and silk free ties; 3-0 chromic catgut
(colostomy); closure: ) chromic catgut or Dexon
– Medications on field (name & purpose)– Catheters & Drains
• NG tube, Penrose drains (large and med available), Hemovac

Surgical Intervention: Supplies cont’d
• Special– Hemoclip appliers– Extra glove and umbilical tape (for proximal
end of specimen before passed thru perineal wound
– Vessel loop or umbilical tapes for retraction– Marking pen for stoma site

Surgical Intervention: Instruments
• Specific (If done simultaneously, 2 separate instrument set ups)– Major laparotomy short set– Long instrument set and intestinal set– Rectal set– Possibly a separate minor set for closure

Surgical Intervention: Equipment
• Specific– ESU, Suction, Stirrups

Surgical Intervention: Overview of Procedure Steps
• The abdomen is entered
• The lesion is located and the bowel mobilized
• The colon is divided in an area proximal to the lesion
• A colostomy is performed and the abdomen is closed
• Through a perineal incision, the lower sigmoid colon, rectum, and anus are mobilized and removed
• The perineal incision is closed.
Be sure to use multiple resources: concise but complete!

Surgical Intervention: Procedure Steps Cont’d
• Mobilization process: isolation of mesenteric tissue and omentum that caused diseased lymph nodes
• Double-clamp
• Divide tissue (cut using Metz scissors or ESU)
• Sections ligated
• Large blood vessels are clamped and ligated
• Dissection and mobilization to level of levator muscles in pelvic floor
• (2) clamps to proximal end of the mobilized area
• Bowel is divided, distal end placed in pelvis

Surgical Intervention: Procedure Steps Cont’d
• To reconstruct the pelvic floor, a portion of omentum may be sutured to it.
• Prepare colostomy site by incising small circle in abdomen w/skin knife. Deepened to inner abdomen with cautery. Specimen (small disk) is passed to STSR.
• Proximal end of bowel is brought through the circular incision and temporarily clamped in place while the abdominal incision is closed in layers.

Surgical Intervention: Procedure Steps Cont’d
• To create colostomy, surgeon everts edges of bowel stoma and sutures edges of skin using interrupted sutures of 3-0 chromic catgut on a fine cutting needle.

Surgical Intervention: Procedure Steps Cont’d
• Perineal portion: surgeon places heavy silk pursestring suture through the anus to occlude it and perineum is incised and deeped with ESU.
• Large bleeding vessels are double-clamped and ligated w/silk or Dexon
• Peans are used to grasp bowel attachments.
• Have sponge sticks and suction at all times during mobilization and dissection.
• Mobilization continues until surgeon reaches previously mobilized area
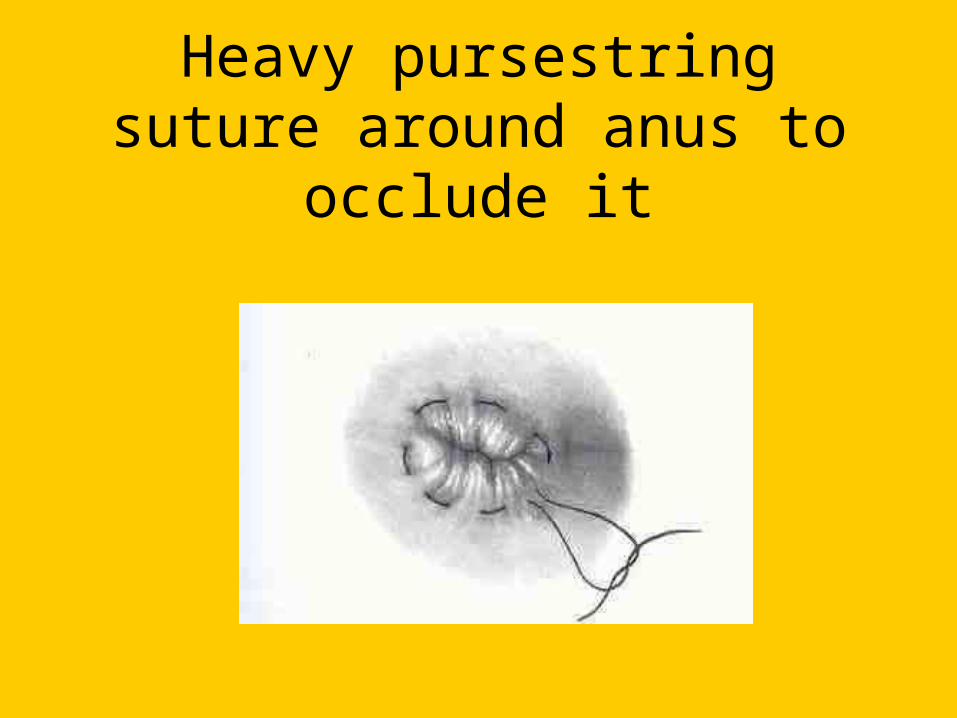
Heavy pursestring suture around anus to occlude it

Area of incision around the rectum

Surgical Intervention: Procedure Steps Cont’d
• The entire specimen is delivered through the perineal incision, then irrigates the wound
• Present trend is to obliterate the “dead space” with many interrupted sutures; achieve hemostasis
• One or two Penrose drains are placed in the wound, which
is then closed with size 0 chromic catgut or Dexon.• Skin is approximated with nonabsorbable suture.

Colon and Rectum are delivered through the perineal resection

Counts
• Initial: Sponges, sutures & blades, Instruments
• First closing
• Final closing– Sponges
– Sutures and Blades
– Instruments

Dressing, Casting, Immobilizers, Etc.
• Types & sizes– Abdominal incision and on colostomy:Bulky
abdominal pad and gauze sponges– Perineal pad for rectal drainage possibly
• Type of tape or method of securing

Specimen & Care
• Identified as anus, rectum, and sigmoid colon
• Handled: Usually routine/in formalin
• Need a large container for storage and transport—formalin should cover specimen

References
• Alexander’s p. 385
• Berry and Kohn p. 665
• Fuller pp. 262-263
• STST p. 425-426
Top Related