






Languages
Pages
Legal


Primary health care:Concept launched at Alma Ata,
Kazakhstan, USSR in 1978

Essential health care based on practical, scientifically sound and socially acceptable methods and technology, made universally accessible to individuals and families in the community, through their full participation, and at a cost that the community and country can afford to maintain at every stage of their development, in the spirit of self-reliance and self-determination.
What is the definition of primary health care

It forms an integral part of the country's health care system, of which it is the central function and main focus – and of the social and economic development of the community.
It is the first level of contact with individuals, the family and the community …. Bringing health care as close as possible to where people live and work and constitutes the first element in the continuum of health care.

PrinciplesSet of principles and strategies for organising health systems
that would lead to “health for all” - health is a fundamental human right :
1. Health promotion
2. Accessibility: Equity, social justice and universal coverage
3. Community participation and accountability: in assessing risks, priorities and interventions.
4. Inter-sectoral action at local level to address the root causes of ill-health.
5. Appropriate use of technology
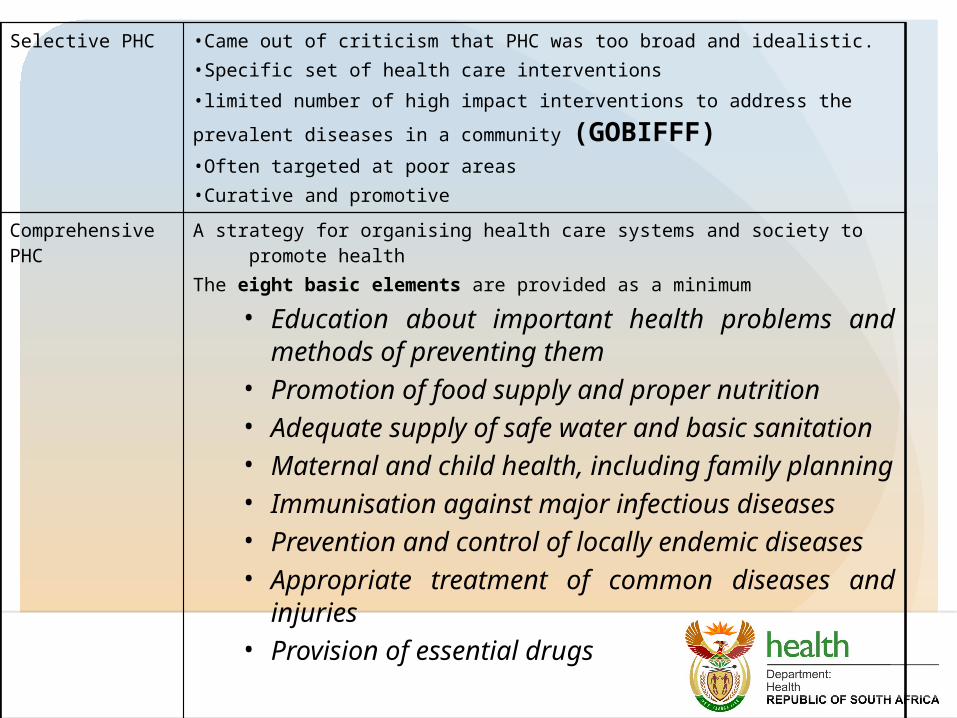
Selective PHC •Came out of criticism that PHC was too broad and idealistic. •Specific set of health care interventions
•limited number of high impact interventions to address the prevalent
diseases in a community (GOBIFFF)•Often targeted at poor areas•Curative and promotive
Comprehensive PHC
A strategy for organising health care systems and society to promote health
The eight basic elements are provided as a minimum
• Education about important health problems and methods of preventing them
• Promotion of food supply and proper nutrition• Adequate supply of safe water and basic
sanitation• Maternal and child health, including family
planning• Immunisation against major infectious
diseases• Prevention and control of locally endemic
diseases• Appropriate treatment of common diseases
and injuries• Provision of essential drugs

Equity Equity is different from equality as it is about fairness not
sameness
Definitions ‘equal access for equal need’ ‘equal utilisation for equal need’
Individuals should contribute according to ability to pay, and benefit according to their need

Social justice
• The fair and proper administration of laws
• All persons, irrespective of ethnic origin, gender, possessions, race, religion are to be treated equally and without prejudice.
• Social justice generally refers to the idea of creating a society or institution that is based on the principles of equality and solidarity, that understands and values human rights and that recognizes the dignity of every human being
• Institutions are justly arranged, resources are equitably distributed
• Right and responsibilities observed for all health care workers and users

Universal coverage• Universal health coverage (UHC), is defined (by WHO) as ensuring
that all people can use the promotive, preventive, curative, rehabilitative and palliative health services they need, of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user to financial hardship.
• This definition of UC embodies three related objectives:
• equity in access to health services - those who need the services should get them, not only those who can pay for them;
• that the quality of health services is good enough to improve the health of those receiving services; and
• financial-risk protection - ensuring that the cost of using care does not put people at risk of financial hardship

Inter-sectorial collaboration
Improving the health of the community needs not only the health sector, but also the involvement of other sectors (e.g. education, housing, agriculture).
Need inter-sectorial action to address root causes of ill-health.

Community participation• PHC requires and promotes
maximum community and individual self reliance
• Community participation is about ensuring meaningful engagement with our communities.
• People have the right – and duty – to participate, individually and collectively – in the planning and implementation of their health care
• Health services are accountable to communities.
Community participation• There are a number of terms used to describe working with
communities.
• Community action for health is the collective efforts by communities directed towards increasing community control over the determinants of health, and thereby improving health.
• Community engagement is where the community is empowered to apply its’ collective skills and resources to increase its’ level of influence and control over their own health. This might be to improve the community’s health needs and address the local determinants of health.
• Community participation relies on health workers having a good understanding of the communities, groups and individuals we work with. Effective interventions rely on community participation. Effective interventions are achieved when the community supports the identified health needs, priorities, capacity and any barriers to action.

Criticism of PHC include: • Reductionist approach • “Primitive health care”, • Simplified technology, • Cheap- poor health care for the poor, • 2nd class health care, etc

Primary health care is featured in SA leadership, governance and policy
frameworks since 1994
ANC health plan and RDP
“the whole NHS must be driven by the Primary Health Care (PHC) approach.
1997 – White Paper on Transformation of Health System
'The health system will focus on districts as the major locus of implementation, and emphasise the primary health care (PHC) approach
National Health Act (act 61 of 2003)
District Health System - the formalisation of the legal status of the District Health System in the 2003 National Health Act (61 of 2003)
which establishes the District Health System along the boundaries of District and Metropolitan Municipalities

PROGRESS SO FAR
Building block
Progress
Health financing
• Removal of user fees for public PHC
• Removal all fees (including at hospitals) for pregnant women and children under the age of 6 years
Medical products
• The development and implementation of an Essential Drugs List
• Standard Treatment Guidelines for Primary Health Care ensuring generally good drug availability, with few exceptions, in the PHC system
Information • The implementation of the District Health Information System (DHIS).
Building block
Progress
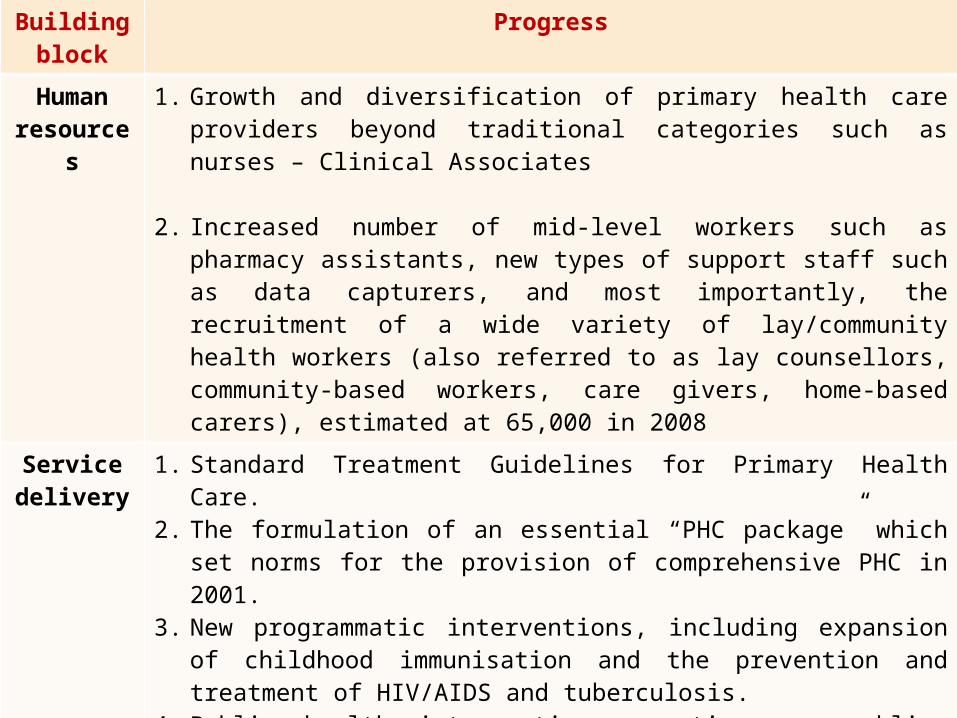
Human resource
s
1. Growth and diversification of primary health care providers beyond traditional categories such as nurses – Clinical Associates
2. Increased number of mid-level workers such as pharmacy assistants, new types of support staff such as data capturers, and most importantly, the recruitment of a wide variety of lay/community health workers (also referred to as lay counsellors, community-based workers, care givers, home-based carers), estimated at 65,000 in 2008
Service delivery
1. Standard Treatment Guidelines for Primary Health Care. 2. The formulation of an essential “PHC package” which set
norms for the provision of comprehensive PHC in 2001.3. New programmatic interventions, including expansion of
childhood immunisation and the prevention and treatment of HIV/AIDS and tuberculosis.
4. Public health interventions creating an enabling environment for PHC, such as tobacco control legislation and regional cooperation in the control of malaria in endemic areas of the country

A clinic construction and upgrading programme involving more than 1,600 facilities, and ensuring geographical availability of services within 5 kilometres to more than 90% of the population.


Why “re-engineer” primary health care?


Health outcomes generally worse than they should have been, given the
financial investment
1. Life expectancy 53.5 (men) and 57.2 (women)
2. High infant mortality rate – 69 deaths in children under the age of 5 per 1,000 live births (and increasing! One of only 12 countries)
3. Number of women who die as a result of being pregnant – 160 per 100,000 live births. Up to 60% are avoidable
4. Number perinatal deaths – 31 per 1,000 births – up to 1/3rd are avoidable
5. TB cure rate - 65%
6. 50% women and 75% of men with hypertension / diabetes do not know that they have these conditions, only 14% treated properly

Problems with equity
Huge inequalities in health• Between men and women• Between urban and rural areas• Between districts• Between provinces
Content, coverage and quality of health care – still very much depends on where you live.





Why have our achievements been poor?
Service delivery: coverage, quality and focus of PHC
Lack of focus on priority problems
Poor quality in the delivery of PHC - patients wait a long time – and some are turned away, drugs run out, patients not treated with dignity and respect, shortage of staff
Focus on curative servicesFocus on primary careCoverage poor - inequitable Not enough focus on prevention
Governance and legislation
Establishment of DHS has stalled – staffing, amalgamation of old and new municipal systems. Provincialization in Gauteng!
Infrastructure, money and
people
Availability of staff - numbers of staff, inability to retain community service posts, high attrition rates
Suitability of staff - competence and orientation towards PHC – many health care workers not adequately prepared (Hospicentric)
Information Lack of really good information to enable good decision to be made and to monitor the performance of the PHC system

“..South Africa must overhaul its entire health system and move towards primary health
care.”
Minister of Health, Dr Aaron Motsoaledi; SA Parliament, Wednesday, Jan 26, 2011 6.03 pm
SAPA


So what is re-engineering?
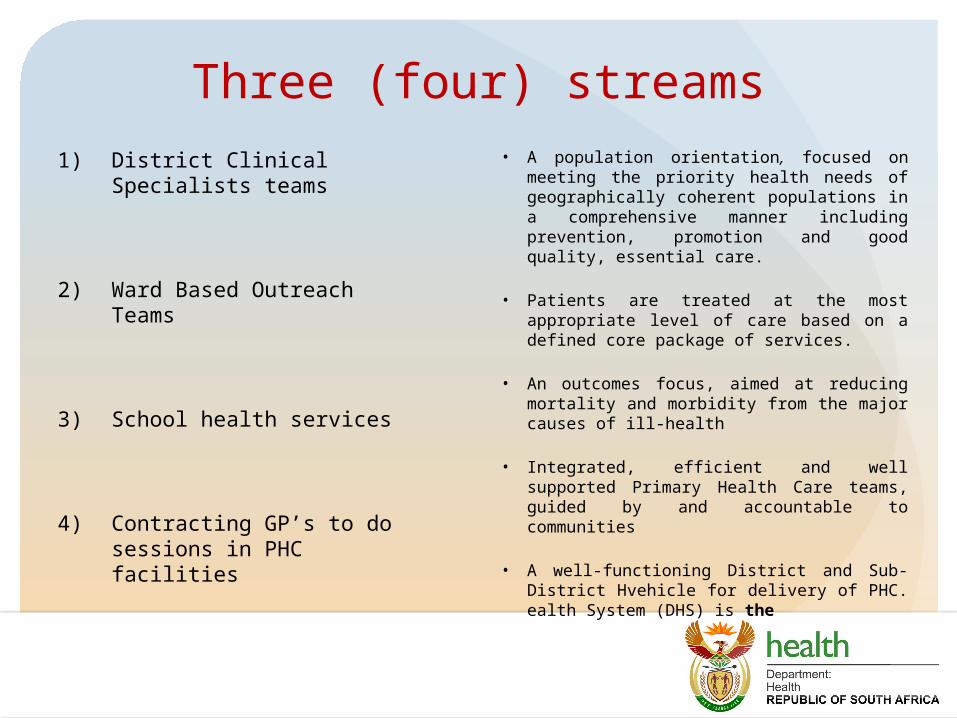
Three (four) streams1) District Clinical Specialists
teams
2) Ward Based Outreach Teams
3) School health services
4) Contracting GP’s to do sessions in PHC facilities
• A population orientation, focused on meeting the priority health needs of geographically coherent populations in a comprehensive manner including prevention, promotion and good quality, essential care.
• Patients are treated at the most appropriate level of care based on a defined core package of services.
• An outcomes focus, aimed at reducing mortality and morbidity from the major causes of ill-health
• Integrated, efficient and well supported Primary Health Care teams, guided by and accountable to communities
• A well-functioning District and Sub-District Hvehicle for delivery of PHC. ealth System (DHS) is the

Ward –based outreach teams: using the principles of COPC


Maternal Neonatal Child Health
HIV & TB Chronic Non –communicable Diseases
Violence & Injury
HOUSEHOLDS
Screening, assessment & referral
Pregnant women, newborn & infants
HIV Testing, regular CD4, early HAART, TB symptoms
Screen for hypertension, diabetes
Substance abuse, domestic violence
Information & education
Feeding, hand washing, Oral Rehydration Therapy (ORT)
Diet, exercise, lifestyle
Psychosocial support
Integrated approach to adherence support
Victim support
Basic home treatment
ORT, worms, refer pneumonia, Vitamin A
Foot care First aid
COMMUNITY, SCHOOLS & EARLY LEARNING CENTRES
Assessments, campaigns, & screening
Immunisation, water and sanitation, nutrition, food security
Condom distribution, youth programmes
Diet, exercise Pedestrian safety
Comprehensive CHW roles

School health services

School health programme Launched in 2012 in Refiloe in Cullinan near Tshwane.
The Integrated School Health Programme will offer the following services:
• Eyesight, hearing and oral hygiene
• Immunisation (for foundation and intermediate phases)
• Deworming (for foundation and intermediate phases)
• Treatment of minor conditions especially skin conditions (all phases)
• Counselling on sexual and reproductive health issues and offer of services via mobile health units (all senior and FET learners, and intermediate learners where required)
• Prevention of drug and alcohol use and abuse.
• Individually assess every learner once during each of the four educational phases.

Progress• 29 000 schools in the country
• Not possible to have a school health nurse in every school in the short to medium term.
• Focus on schools in quintiles 1 and 2 (the poorest schools)
• Prioritise a selected range of services.
• As more resources become available the package of services will be expanded to the full range of school health services as outlined in the revised policy.
• Option to run outreach services from district / sub-district with mobile units

Contracting of doctors to work in primary health care facilities
• National Technical Task Team (with NHI managers)
• Idea of contracting in and contracting out discussed in 2012. Opted for contracting in (for now) so that the image of the public sector – and service delivery improves.
• Advert for GP’s - 2013.
• Initially in NHI pilot districts

Some details
• GP’s are contracted by NDoH
• SLA with district. Currently just covers delivery of service but would like to move towards performance based contract.
• Currently paid an hourly rate – R355 – regardless of level of experience
• Also paid for travel and kilometres (to ensure that rural areas covered.
Pillars of capacity building (slides provided by Dr R Cooke)

Why is this important for DCST’s
• All these initiatives are changing the context in which DCST’s are working.
• Collectively, they ALL aim to improve maternal and child health outcomes.
• Therefore, important to consider how to ensure that efforts are not duplicated and that collaboration is maximised
• Ensure that synergies explored.
Top Related