






Languages
Pages
Legal


November 30, 2018
Primary Care Pathways
Julia Carter, MD, FCFPDigestive Health SCN Core Committee member
Co-chair, Primary Care Pathways Working Group

Presenter Disclosure
• Presenter: Dr. Julia Carter
• Relationships that may introduce potential bias
and/or conflict of interest:
• Grants/Research Support: N/A
• Speakers Bureau/Honoraria: AHS – Digestive Health SCN
• Consulting Fees: N/A
• Other: N/A

Disclosure of Commercial
Support• This program has received financial support from in the form of
an education grant from:
• Merck Canada, University of Calgary Department of Medicine, Alberta
Health Services, Alberta Innovates, Alberta Netcare, College of
Licensed Practical Nurses of Alberta, BrightSquid,, Health Quality
Council of Alberta, Boehringer-Ingelheim, and the Institute of Health
Economics.
• This program has received NO COMMERCIAL in-kind support.
• Potential for conflict(s) of interest:– Dr. Julia Carter has not received payment from the APCC planning
committee. Funds from sponsors are pooled to off-set conference costs.

Mitigating Potential Bias
• The planning committee developed the conference
objectives which do not include the discussion of our
sponsor’s products or services.
• Sponsorship funds are pooled and are evenly distributed
throughout the conference. They do not fund specific
speakers.
• The committee has reviewed the content of the
presentations and ensured that content presented is
evidence-based and free of undue influence.

Can Enhanced Primary Care
Pathways Improve Patient Care
and Referral Processes in Alberta?

The problem: Access to
digestive health care

• Untenable wait times
– 24 months+ in Calgary
• Appropriateness
• Frustrating for primary care
providers, specialists, and
PATIENTS
Calgary Digestive Health
Pathways background

The proposed solution:
Pathways

• Primary care pathways for low-risk,
high-demand indications
• Telephone advice (Specialist Link) -
same-day phone consultation
• Electronic advice (Advice Request) -
non-urgent consultation through Netcare
• QuRE
Primary-Specialty Care
Integration

Quality Referral Evolutionhttps://albertahealthservices.ca/assets/info/hp/arp/if-hp-arp-qure-digital-checklist.pdf

• Build capacity to manage common,
low-risk conditions in the Medical
Home – rather than referring to
specialty care
Why pathways?

• Agreement on “pathway conditions” – that
can be managed in the Medical Home
• Co-development by GI and primary care
• Knowledge translation
Pathway development

• Evidence-based algorithm to guide
diagnosis and management of common,
low-risk health conditions
• Local resources (e.g. PCN supports,
Alberta Healthy Living Program)
• References
• Patient information resources
Pathway components

• Irritable bowel syndrome
• Chronic constipation
• Dyspepsia
• GERD
• H. pylori
• NAFLD
• Chronic diarrhea
• More to come…
GI “pathway conditions”

• Endocrinology
• General Neurology
• Respirology
• Rheumatology
• Others
Other specialties

• Implementation through Central Access
Triage
• Referral “closed” – sent back for further
investigation/management within
Medical Home
• Expedited consultation if no resolution
after pathway completion
Calgary Process



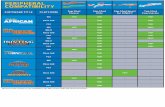
1. Who should be tested for H. pylori?
Patients with dyspepsia symptoms
Patients with history of peptic ulcer/upper GI bleed who are
contemplating use of NSAIDs or antiplatelets
Patients with first degree relative with history of gastric cancer
2. Alarm features Dyspepsia symptoms plus VBAD (V =vomiting, B =bleeding or
anemia, A =abdominal mass, D =dysphagia) or melena
Dyspepsia symptoms plus first degree relative with history of gastric
cancer
3. Diagnosis HpSAT or UBT
Before testing, patient must be off antibiotics x4
weeks and off PPI at least 3 days
4. Treatment Round 1: CLAMET Quad or BMT Quad
Round 2 (if needed): CLAMET Quad or BMT Quad
Round 3 (if needed): Levo Amox
Round 4 (if needed or refer to GI): Rif-Amox
5. Confirm eradication HpSAT or UBT at least 4 weeks after finishing
treatment
6. Treatment failure Proceed to next round of treatment
Option to refer to GI after 3 failed
treatment attempts
Treat according to
dyspepsia pathway
Yes, no symptoms = DONE
Yes, continued
symptoms
7. Refer for
gastroscopy
No
Positive
No
Negative
Yes

• For patients
– Comprehensive, evidence-based care within
the patient medical home
– Local resources
– Patient information sheets
What do pathways do?

• For patients
– Decrease unnecessary investigations/
endoscopy
– Decrease time off work/travel for specialist
consultation that may not change
outcome/management
What do pathways do?

• For primary care providers
– Enhance supports in diagnosis and
management
– Suggest local resources
– Provide references
– Minimize unnecessary consultations
– Facilitate necessary consultations
(expedited)
What do pathways do?

• For specialists
– Reduce referrals for conditions that can be
managed within the medical home
– Create capacity for more timely consultation
with patients at higher risk
– Good quality referrals with comprehensive
work-up (and without unnecessary testing)
– Alarm features identified
What do pathways do?

– To identify “alarm” features and highlight
them on the referral letter
– To reassure patients without “alarm” features
that they don’t need referral and provide
them with resources
– To guide management while awaiting, or
instead of GI consultation
– Example: NAFLD
Pathways can be used
pre-emptively:

Outcomes of pathway
implementation

• Prospective review (2015-2017)
• 2,240 referrals returned to primary care
– 15% re-referred to GI for endoscopy
– 70% were completely normal
– Only 2% had a clinically significant finding
(e.g. esophagitis)
Outcomes - safety

• 98% reduction in non-urgent GI wait list
(Jan 2016-Dec 2017)
• August 2017-2018, 86% drop in referrals
for NAFLD
Outcomes - access

Outcomes - adoption
105
128
412
308
355
329340
297
0
50
100
150
200
250
300
350
400
450
Nov-17 Dec-17 Jan-18 Feb-18 Mar-18 Apr-18 May-18 Jun-18
GI/Hepatology Pathway DownloadsNovember 2017-June 2018
NAFLD pathway
introduced

• 2018 survey of Calgary family
physicians (n= 625)
• 55% were aware of pathways
• 78% of these reported pathways
changed their clinical practice
Outcomes – awareness/impact

• 1,722 calls to GI
• Average system savings of $133/call
(avoided consultations and ER visits)
• 89% of family physicians are aware of
Specialist Link
• 73% of these report it changed their
practice
Specialist Link

GI Access Challenges -
Alberta

• Edmonton
12-24 months
• Central and South
9-12 months
• Calgary (CAT)
24+ months
Wait times for routine GI
consultation

• Improve access through spread of GI
Primary Care Pathways across Alberta
DHSCN Pathways Goal

Clear Adaptable

Safe Local

• Validation (content & format)
• – primary care, specialists and allied health
• Spread
– Knowledge translation to primary care
providers and allied health professionals
– Collaborative implementation between GI
and primary care
• Evaluation
How?

• Zonal differences
• Rural/remote
• Varying triage processes
• Variable need for formal phone advice
system
Locally appropriate

ACFP e-panel survey input
87%
2%11%
Do you see a role for using clinical pathways BEFORE you consider a specialist referral?
Yes No Maybe

• “determine if a specialist referral is even
necessary”
• “help assure the patient”
• “prevents wasted time for the physician
and the specialist”
ACFP survey input

0
5
10
15
20
25
30
Co-developedwith familyphysicians
Brief Recommendedas best practice
Very visual Comprehensive Not useful at all
Which factors would increase the likelihood of youusing clinical care pathways?
ACFP survey input

• Central repository
• Easy access at point of care
– EMR?
• Potentially time-consuming
• Need for patient information resources
Primary care input

• Create capacity/more timely care for
higher risk patients
• “Can I/when can I decline a referral?”
• Triage processes vary – challenges for
community specialists
Specialist input

• Quality/timely care is the key
• Self-management resources
• Strong communication between providers
• Satisfaction surveys to come
Patient input

Evaluation plan
• Inappropriate specialty consultations and endoscopy procedures avoided
• Family physician & specialist satisfaction survey
• Improved system integration
• Inpatient admissions and ED visits for pathway conditions
• Improved access to GI for sick/urgent patients
• Patient Experience survey
• Specialty care wait time
• Continuity of care
Enhanced Patient
Experience
Improved Patient
Outcomes
Value for Investment
Improved Provider
Satisfaction

• Primary care and specialist champions
working together
• Primary care teams – dieticians,
pharmacists, CDMs, BHCs
• PCN leadership, improvement facilitators
• PHCIN, AMA, AIM, TOP
Partnerships

• Primary care pathways can improve
patient care and referral processes
– Improved care of pathway conditions in the
patient’s Medical Home
– Proven safety
– Decreased unnecessary referrals &
endoscopy
– Improved triage processes
Summary

Thank you!
November 30, 2018
Top Related