







Languages
Pages
Legal


6/10/2014
1
Chronic Kidney Disease -
General management and standard of care
Dr Nathalie Demoulin , Prof Michel Jadoul
Cliniques universitaires Saint-Luc
Université Catholique de Louvain
• Above all, clinical care !
• Pathophysiology is presented only to explain why a
practice is recommended
• The following topics will not be covered:
- diagnosis of the cause of CKD (frequently crucial)
- the methods to estimate GFR
What should and can be done when managing a CKD patient
Stage Description GFR
(mL/min./1,73m²)
Action
At increased risk >90
(with CKD risk factors)
Screening,
CKD risk reduction
1 Kidney damage
With normal or ↑ GFR
>90
Diagnosis and treatment,
Treatment of comorbid conditions,
Slowing progression,
CVD risk reduction
2 Kidney damage
With mild ↓ GFR
60-89 Estimating progression
3 Moderate ↓ GFR 30-59 Evaluating and treating
complications
4 Severe ↓ GFR 15-29 Preparation for kidney
replacement therapy
5 Kidney failure < 15
(or dialysis)
Replacement (if uremia present)
Management of CKD according to stage (KDOQI 2002)

6/10/2014
2
KDIGO CKD Guidelines 2012
Section 1: Definition and classification of CKD
Section 2: Definition, identification and prediction of CKD progression
Section 3: Management of progression and complications of CKD
Section 4: Other Complications of CKD: CVD, medication dosing,
patient safety, infections, hospitalizations, and caveats for
investigating complications of CKD
Section 5: Referral to specialists and models of care

6/10/2014
3
Definition and Classification
1.1. Definition of CKD: CKD is defined as abnormalities of
kidney structure or function for ≥3 months with
implications for health
- this definition specifically excludes simple renal cysts, …..
- If duration < 3 months -> could be CKD or AKI or both
Definition and Classification
Cause GFR Categories
(ml/min/1.73m2)
Albuminuria Categories
(ACR, mg/g)
Diabetes G1 ≥90
A1
<30
Hypertension G2 60-89
Glom Disease G3a 45-59
A2
30-299
Transplant G3b 30-44
Unknown G4 15-29
A3
≥300
etc G5 <15
Tigette OK
N to midly increased
Moderately increased
Severly increased
Staging of CKD (CGA staging)
6/10/2014
4
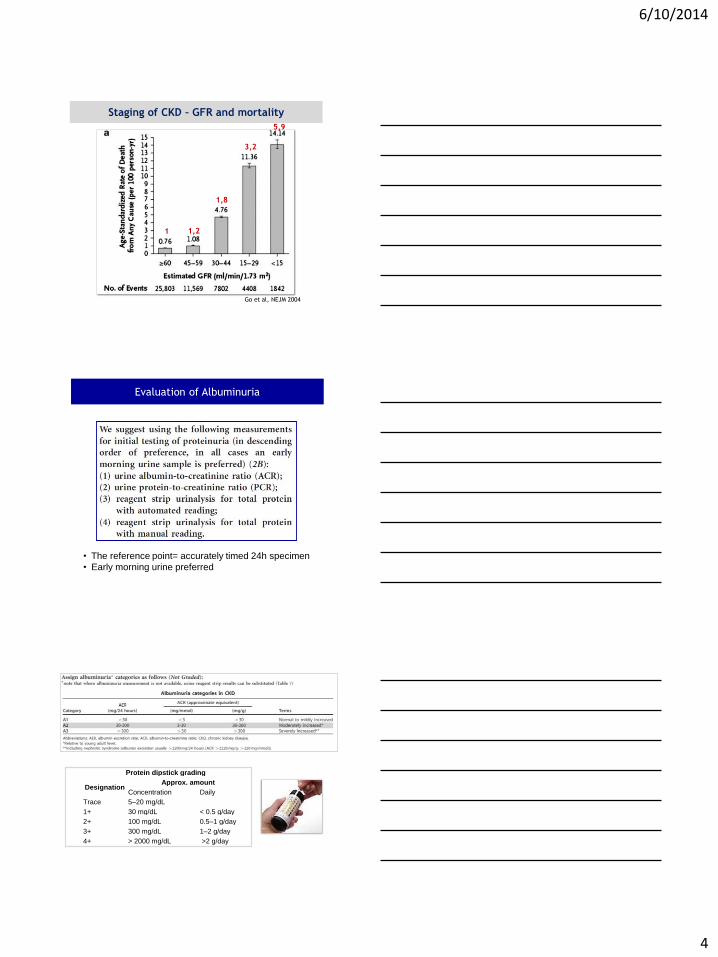
Go et al, NEJM 2004
Staging of CKD – GFR and mortality
5,9
3,2
1,8
1,2 1
• The reference point= accurately timed 24h specimen
• Early morning urine preferred
Evaluation of Albuminuria
Protein dipstick grading
Designation Approx. amount
Concentration Daily
Trace 5–20 mg/dL
1+ 30 mg/dL < 0.5 g/day
2+ 100 mg/dL 0.5–1 g/day
3+ 300 mg/dL 1–2 g/day
4+ > 2000 mg/dL >2 g/day

6/10/2014
5
Relationship between categories of
albuminuria and proteinuria
Cause GFR Categories
(ml/min/1.73m2)
Albuminuria Categories
(ACR, mg/g)
Diabetes G1 ≥90
A1
<30
Hypertension G2 60-89
Glom Disease G3a 45-59
A2
30-299
Transplant G3b 30-44
Unknown G4 15-29
A3
≥300
etc G5 <15
N to midly increased
Dipstick neg to trace
Moderately increased
Dipstick trace to +
Severely increased
Dipstick > +
Staging of CKD (CGA staging)
Prognostic value of GFR and albuminuria:
Cohorts and Subjects of CKD Consortium
• Community based populations – With ACR data, 14 studies, n=105,872
– With dipstick data, 10 studies, n=1,239,447
• Populations at increased CVD risk (HTN, diab, CV) – 10 studies, n=266,975
• CKD cohorts – 14 studies, n= 21,688
45 cohorts in total, >1.5 million subjects
Collaborative meta-analysis
Major publications: Lancet, KI, JAMA

6/10/2014
6
Prognostic value of GFR and albuminuria:
Cohorts and Subjects of CKD Consortium
• Community based populations – With ACR data, 14 studies, n=105,872
– With dipstick data, 10 studies, n=1,239,447
• Populations at increased CVD risk (HTN, diab, CV) – 10 studies, n=266,975
• CKD cohorts – 14 studies, n= 21,688
45 cohorts in total, >1.5 million subjects
Collaborative meta-analysis
Major publications: Lancet, KI, JAMA
Matsushita et al, Lancet 2010
Predictive ability of albuminuria at all categories of GFR:
Meta-analysis from General Population Cohorts -
CKD Prognosis Consortium
Levey, KI 2011
ACR>=300
ACR 30-299
ACR <30
Predictive ability of albuminuria at all categories of GFR:
General Population Cohorts
ACR>=300
ACR 30-299
ACR <30
Levey, KI 2011

6/10/2014
7
Adjusted relative risk of renal and cardiovascular outcomes
for GP cohorts with ACR
Levey et al, Kidney Int 2011
KDIGO CKD Guidelines 2012
Section 1: Definition and classification of CKD
Section 2: Definition, identification and prediction of CKD progression
Section 3: Management of progression and complications of CKD
Section 4: Other Complications of CKD: CVD, medication dosing,
patient safety, infections, hospitalizations, and caveats for
investigating complications of CKD
Section 5: Referral to specialists and models of care
6/10/2014
8
Definition of CKD progression
• Decline in GFR category (G1-G4)
accompanied by ≥ 25% drop in eGFR from baseline
• Rapid progression defined as sustained decline in
eGFR > 5ml/min/1,73m2/year
• Cause of CKD
• Level of GFR
• Level of albuminuria
• Age
• Gender
• Elevated BP
• Hyperglycemia
• Dyslipidemia
• Smoking
• Obesity
• History of CVD
• Ongoing exposure to nephrotoxic agents
Predictors of progression of CKD
Anemia, acidosis, bone metabolism, hyperuricemia….
Minimising CKD progression (and CV risk) – BP control

6/10/2014
9
ACR <30mg/g 30-300 mg/g > 300 mg/g
Diabetic ≤ 140/90 mmHg
(1B)
≤ 130/80 mmHg
(2D)
≤ 130/80 mmHg
(2D)
Non
diabetic
≤ 140/90 mmHg
(1B)
≤ 130/80 mmHg
(2D)
≤ 130/80 mmHg
(2D)
Minimising CKD progression (and CV risk) – BP control
Minimising CKD progression
Lewis et al. NEJM 1993; 329, 1456-1462
Captopril protects against deterioration in renal function in insulin-
dependent diabetic nephropathy independently of BP control

6/10/2014
10
20
Lewis et al. N Engl J Med 2001; 345: 851-860
Irbesartan
Amlodipine
Placebo
The angiotensin-II-receptor blocker irbesartan is effective in protecting against
progression in type 2 diabetes nephropathy, independently of BP control
1715 patients, Target BP ≤ 135/58 mmHg
Lewis et al. N Engl J Med 2001; 345: 851-860
Mean BP + 3,3 mmHg in placebo vs amlodipine and irbesartan (p=0,001)

6/10/2014
11
ACEi and ARBs are beneficial agents in CKD
• Hemodynamic/antihypertensive actions – ↓ capillary hypertension by ↓ perfusion pressure and efferent
arteriole relaxation
• Anti-inflammatory/anti-fibrotic actions
Turner et al, Kidney Int 2012
Heeg et al, Kidney Int 1989
The anti-proteinuric effect of lisinopril is dose and time related,
and strongly dependent on dietary sodium restriction
Salt intake 50 and 200 mmol/day

6/10/2014
12
Salt restriction or diuretics :
similar potentiation of ACE-I effect
Buter et al, Nephrol Dial Transplant 1998
low= sodium 50 mmol/d high= sodium 200 mmol/d
Addition of HCT -> ↓ 10% BP ↓ 40% proteinuria
The optimal clinical use of diuretics
• eGFR > 30 : thiazide ( Chlortalidone, « Co…. », « Plus »)
• eGFR < 30 or poor response to thiazide: loop diuretic
(furosemide / bumetanide)
– works for max 6-8h, thus if still poor response , give 2-3 times a day
(8am, 12am and 5pm)
– ! tolerance : cramps (volume –related (not K, Ca, Mg)),
pollakiuria ( prostate…)
– adapt timing of administration to daily activities
24
Estimating salt intake from 24 h urine sample?
• Prerequisite 1) Volume IN = Volume OUT (steady state)
• Thus not valid if diarrhea or vomiting, ileostomia or
intense sweating or recent start or change of dosage or
variable adherence to diuretics
• Prerequisite 2) Na IN = Cl IN
• Thus not valid if Vichy water or NaHCO3 taken orally
• 100 mmol Na = roughly 6g de salt
• Prerequisite 3) 24h urine collection is complete
• Estimated from creatininuria (10-25 mg/kg (depending
on age, gender, ethnicity))
25

6/10/2014
13
ACE-I, ARB : should we stop them if creatinine rises?
No if creatinine < 3 mg/dl and rising by less than < 30 %
Treatment is associated +++ with preservation of GFR
(if creatinine rises +++ (double or triple): look for renal artery
stenosis or stenoses)
Bakris et al. Arch Int Med 2000; 160: 685-693
Example of a patient with diabetic nephropathy patient already
under Irbesartan: loop diuretic increased progressively
Hyperkalemia with ACE inhibitors /
angiotensin II receptor antagonist / aliskiren (I)
Is it true hyperkalemia? (to avoid stopping valuable drug because of a laboratory error)
• Time between blood sampling and analysis?
• Hemolysis?
• Confirmed (precautions), severe? (> 5.8 mmol/l)
Dietary ? • Salt substitute
• (Dried) fruit, bananas, chocolate, instant coffee,....
28

6/10/2014
14
Correct any acidosis (Vichy 1-2 glasses/d)
ACE inhibitor + angiotensin II receptor or aliskiren:
stop or reduce 1 of the 2
ACE inhibitor (angiotensin II receptor ) + spironolactone:
stop or reduce spironolactone
ACE inhibitor or angiotensin II receptor or aliskiren monotherapy:
dose - add Furosemide
If persistence, add calcium kayexalate 15 g/2 days per os
29
Hyperkalemia with ACE inhibitors /
angiotensin II receptor antagonist / aliskiren (I)
Dual RAAS blockade in CKD ?
Similar results in « Altitude » with Aliskiren + ACEI or A2RB

6/10/2014
15
Dual RAAS blockade ?
Nephro-protection : reducing proteinuria
with medium to long-term renoprotective effect
(dialysis later ... or never)
Nephro-risk: acute worsening of renal failure
and hyperK if intercurrent disease
(gastroenteritis ++, …)
So block RAAS : YES but usually single agent (ACEi
or ARB) + possibly microdose « cardio »
spironolactone
Association ACE inhibitor + ARB : only if heavy
proteinuria (« glomerular), close, careful
nephrology follow-up in reliable patients
32
Rationale:
If BP and proteinuria are well controlled, the slope of CKD
progression will not change much with lower protein intake
In > 65 y old patients, potential for malnutrition !
Protein intake
Glycemic control
6/10/2014
16
Lifestyle measures
KDIGO CKD Guidelines 2012
Section 1: Definition and classification of CKD
Section 2: Definition, identification and prediction of CKD progression
Section 3: Management of progression and complications of CKD
Section 4: Other Complications of CKD: CVD, medication dosing,
patient safety, infections, hospitalizations, and caveats for
investigating complications of CKD
Section 5: Referral to specialists and models of care
• Strong and independent associations between GFR and albuminuria
categories and risk of CVD in people with CKD
• Cardiovascular risk in CKD is multifactorial
• Cardiovascular disease is more frequent and severe, often not
recognised and undertreated in patients with CKD
• Patients with CKD should be viewed amongst the highest risk
groups for CVD
• To prevent progression of CKD is to prevent CVD

6/10/2014
17
The burden of cardiovascular disease:
Causes of death per CKD stage (Canadian data)
Gansevoort et al, Lancet 2013
Classical CV risk factors
Not modifiable Modifiable but no proven benefit
Modifiable with clinical benefit
Older age Uric acid Smoking
Male gender Homocysteine Obesity
Ethnicity Hypertension
Lp (a) Diabetes
HDL cholesterol LDL cholesterol
Physical activity
37
38

6/10/2014
18
Lipid control and antiplatelet therapy
• No specific lipid targets are established in CKD patients
-> treat in accordance with guidelines for other high-
risk populations
• Antiplatelet therapy should be offered to high risk
patients unless bleeding risk outweighs CV benefits.
Gansevoort et al, Lancet 2013
• Even if cause of CKD not treatable, much can and should
be done for any CKD patient
• Treat BP to target and aggressively substantial
albuminuria; both interventions delay CKD progression
• Underuse of salt restriction/diuretics !!
• Manage aggressively classical CV risk factors
Chronic Kidney Disease -
General management and standard of care
Top Related