







Languages
Pages
Legal


Pre-malignant Lesions
of
Female Genital Tract
Jed Delmore, MD, FACS, FACOG
Professor, Obstetrics and Gynecology
University of Kansas School of Medicine, Wichita

Disclosure

Documented Premalignant Lesions
• Vulva: Yes
– VIN
• Vagina: Yes
– VAIN
• Cervix: Yes
– CIN
• Endometrium: Yes
– For Type I cancers, EIN
• Fallopian Tube: Yes
– STIC
• Ovary: Probably not, or No

Principles
• Rule out invasive disease
• Define extent of disease
• Do more good than harm
Treatment Selection
• Risk of progression if untreated?
• Success of treatment?
• Toxicity/complications of therapy?
• Extent or size of lesion?
• Presence or absence of symptoms?

Case #1
45 year old renal transplant patient, smokes 2
ppd. Complains of vulvar pruritis.
Exam demonstrates-

Diagnosis?

Diagnosis?

Vulvar Intraepithelial Neoplasia
• VIN I: does not exist
• VIN: Encompasses VIN 2 & 3
– VIN- Usual Type (warty, basaloid, mixed)
• Associated with invasive squamous carcinoma of
warty or basaloid type
– VIN-Differentiated type
• More common in older women, with lichen
sclerosus.
• Associated with keratinizing squamous carcinoma.
• Not HPV related
Sideri M, et al Squamous Vulvar Intraepithelial Neoplasia 2004 Modified Terminology, ISSVD Vulvar Oncology Subcommittee.J Reprod Med 2005;50:807-10.
Treatment Options
• Observation- In the face of repeated recurrences, or
something else will do her in first.
• Excision- Primary closure or skin graft
• Laser vaporization- Multiple lesions, large, or at the
introitus
• Topical therapy ( 5-FU), Imiquimod
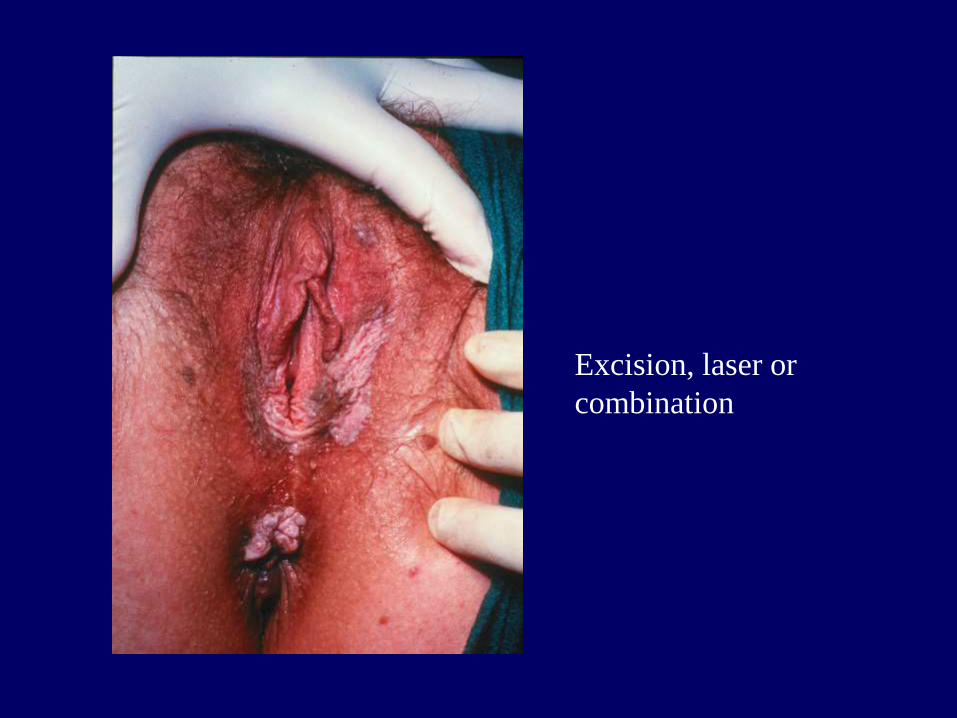
Excision, laser or
combination

Laser or excision and graft



What if the biopsy showed this?

Diagnosis?

Case #1
45 year old renal transplant patient, smokes 2
ppd. Complains of vulvar pruritis.
Exam demonstrates- Hypo and hyper
pigmented vulvar lesions.
Bx = VIN/CIS with probable early invasion.
Treatment Options??

Case # 2
77 year old with vulvar pruritis and multiple
treatments for yeast infection.
Exam =

Diagnosis?

Diagnosis?

Case # 2
77 year old with vulvar pruritis and multiple
treatments for yeast infection.
Exam = Erythematous, excoriated epithelium
with “cake frosting” coating.
Vulvar Biopsy = Paget’s disease of the vulva
Workup and treatment??

Treatment Options
• Excision- Primary
• Laser vaporization- Poor choice due to
gland involvement
• Topical therapy ( 5-FU)-Rarely


Case # 3
38 year old G3P3, Reports a vaginal hysterectomy
for a precancerous condition three years ago.
Pap = HSIL
Colposcopy = Thickened, acetowhite epithelium at
the vaginal apex.

Now what??

VAIN II-III

Treatment Options?

Treatment Options
• Excision- I wouldn’t unless I suspected invasion.
• Laser vaporization- Yep
• Topical therapy ( 5-FU), Imiquimod- Last
resort

Case # 4
32 year old G2P2 with HSIL Pap.
Colposcopy = Acetowhite epithelium with
punctuation. Large transformation zone.
ECC and Cervical Biopsies performed.
What is a Transformation Zone??

Squamocolumnar Junction

Transformation Zone

Transformation Zone

Acetowhite Epithelium

Mosaicism

Punctation

Atypical Vasculature

Case # 4
32 year old G2P2 with HSIL Pap.
Colposcopy = Acetowhite epithelium with
punctuation. Large transformation zone.
ECC-neg, CxBx-CIN III
Treatment Options??

Treatment Options ??
• Observation ?
• Excision ?
• Laser vaporization, Cryotherapy ?
• Hysterectomy ?

Treatment of CIN 2,3
• LEEP, or conization may be used whenever
treatment is appropriate.
• Cryotherapy of Laser vaporization should be used
only after rigorously excluding invasive cancer.
• Hysterectomy is unacceptable as primary therapy
for CIN 2+
ACOG Practice Bulletin 140, December, 2013

Case # 4
32 year old G2P2 with HSIL Pap.
Colposcopy = Acetowhite epithelium with
punctuation. Large transformation zone.
What if the biopsy had shown
adenocarcinoma in situ of the cervix?

The End

Pretend the cervix is gone.
Diagnosis?

Diagnosis?
Slide # 1

Slide #2
Diagnosis ?

VAIN Treatment Outcome

VIN Therapy
Top Related