







Languages
Pages
Legal

Sickle Cell AnemiaGregg Selke, Ph.D.
11/28/06

What is Sickle Cell Anemia (SCA)? First described in Chicago in
1910 by James Herrick as an inherited condition that results in a decrease in the ability of red blood cells to carry oxygen throughout the body
Sickle red blood cells become hard and irregularly shaped (resembling a sickle)
Become clogged in the small blood vessels and therefore do not deliver oxygen to the tissues.
Lack of tissue oxygenation can cause excruciating pain, damage to body organs and even death.
Mechanism Red blood cells (RBC)
Contain a special protein called haemoglobin (Hb)
Hb is the component that carries oxygen from the lungs to all parts of the body
Most people have only hemoglobin type – Hb A within RBC (normal genotype: Hb AA)
Sickle Cell: HbS S similar to A, but one structural change
Other types: HbC, HbD, and HbE
Mechanism -HbS When sickle haemoglobin (HbS) gives up its
oxygen to the tissues, HbS sticks together Forms long rods form inside RBC RBC become rigid, inflexible, and sickle-shaped Unable to squeeze through small blood vessels,
instead blocks small blood vessels Less oxygen to tissues of body
RBCs containing HbS have a shorter lifespan Normally 120 days Chronic state of anaemia

Genetics 2 copies of the
gene for Hb (each parent)
HbS –Recessive S=Sickle A=Normal

Sickle Cell Trait
Sickle haemoglobin (S) + Normal haemoglobin (A) in RBC Adequate amount of normal Hb (A) in red blood
cells RBC remain flexible Carrier Do Not have the symptoms of the sickle cell
disorders, with 2 exceptions1. Pain when Less Oxygen than usual (scuba
diving, activities at high altitude (12,000ft), under general anaesthesia)
2. Minute kidney problems

1. Sickle Cell Anemia Sickle haemoglobin (HbS) + Sickle haemoglobin
(HbS) Most Severe – No HbA
Three common types of Sickle Cell Disorders

Other Sickling DisordersOther types of Hb combine with sickle Hb
2. Hemoglobin S-C disease Sickle haemoglobin (HbS) + (HbC)
3. Hemoglobin S-Beta thalassemia Beta thalassaemia gene reduces the
amount of HbA that can be made Sickle haemoglobin (HbS) + reduced HbA Milder form of Sickle Cell Disorder than
sickle cell anemia

Some Genetic History The error in the hemoglobin gene results from a
genetic mutation that occurred many thousands of years ago in people in parts of Africa, the Mediterranean basin, the Middle East, and India.
A deadly form of malaria was very common at that
time Malaria epidemics caused the death of many In areas where malaria was a problem, children who
inherited one sickle hemoglobin gene and who, therefore, carried the sickle cell trait - had a survival advantage.
Unlike the children who had normal hemoglobin genes, they survived the malaria epidemics they grew up, had their own children, and passed on the gene- for sickle hemoglobin.
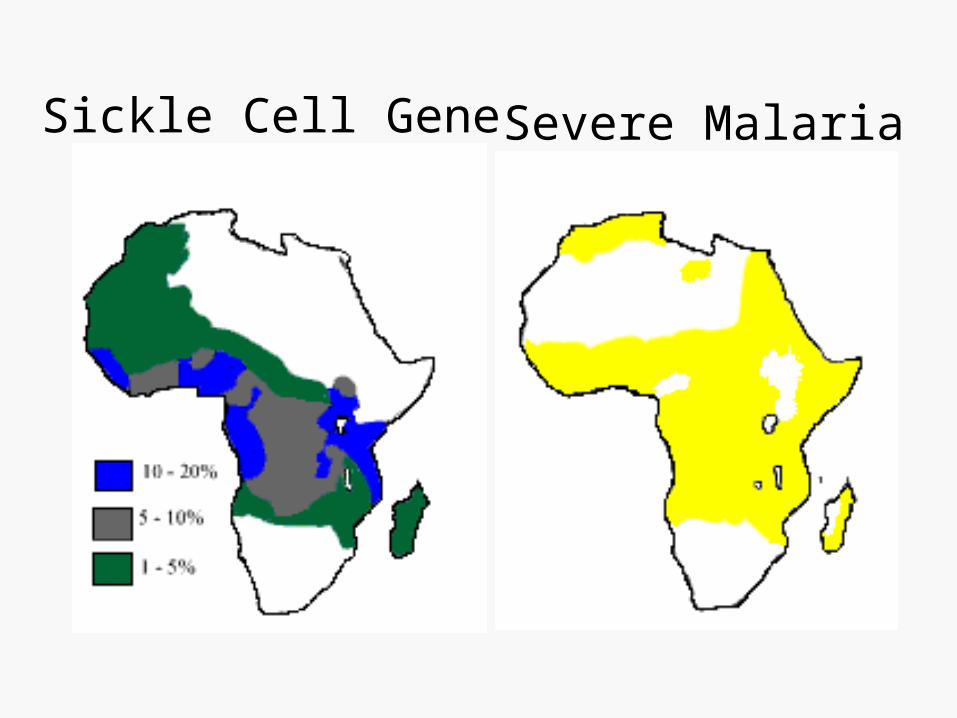
Sickle Cell Gene Severe Malaria

As populations migrated, the sickle cell-mutation spread to other Mediterranean areas, further into the Middle East and eventually into the Western Hemisphere.
In the United States and other countries where malaria is not a problem, the sickle hemoglobin gene no longer provides a survival advantage.
Instead, it may be a serious threat to the carrier's children, who may inherit two abnormal sickle hemoglobin genes and have sickle cell anemia.
History
Most common in Africans and African Americans.
East Asia, Southern Italy, Saudi Arabia, India, Egypt, South and Central American, Cuba, the Caribbean, Greece, and Iran, and Eastern Jews have also been found to have a form of this illness.
Who is at risk?

Prevalence More than 2.5 million Americans
have the trait 70,000 or more Americans have
sickle cell disease About 1,000 babies are born with
the disease each year in America In Nigeria, 1/3 population of U.S., 45,000-90,000
babies with sickle cell disease are born each year

Among African - Americans 1 in 12 have Sickle Cell Trait (Hb SA) 1 in 600 have Sickle Cell Anemia (Hb SS) 1 in 1500 have Sickle C Disease (Hb SC) 1 in 350 have Sickle Cell Disease (Hb SS, SC,
S-Beta-Thal)
Among Latinos 1 in 172 have Sickle Cell Trait (Hb AS) 1 in 1,000 have Sickle Cell Disease (Hb SS, SC,
S-Beta-Thal)

Screening1. Haemoglobin Electrophoresis
Simple Blood test Routine screening in high risk groups
• During pregnancy• Before anaesthesia
2. Prenatal Testing Amniocentesis
16 and 18 weeks of the pregnancy small risk of causing a miscarriage (1 in 100)
Chorionic villus sampling (CVS) 9th or 10th week of pregnancy very small amount of material from the developing
placenta slightly higher chance of miscarriage

Early Symptoms and Complications
Typically appear during infant's first year 1st symptom: dactylitis and fever (6 mo-2
yrs) Pain in the chest, abdomen, limbs and
joints Enlargement of the heart, liver and spleen
nosebleeds Frequent upper respiratory infections Chronic anemia as children grow older
Over time Sickle Cell sufferers can experience damage to organs such as liver, kidney, lungs, heart and spleen
Can result in death

Medical Complications
1. pain episodes 2. strokes 3. increased
infections4. leg ulcers 5. bone damage 6. yellow eyes or
jaundice 7. early gallstones 8. lung blockage
9. kidney damage and loss of body water in urine 10.painful erections in men
(priapism) 11.blood blockage in the
spleen or liver (sequestration)
12.eye damage 13.low red blood cell counts
(anemia) 14.delayed growth

Infectious complications Prominent early in life Leading cause of morbidity and mortality Great improvement in the prognosis related to newborn
screening for sickle cell disease, vaccination for childhood illnesses, the use of prophylactic antibiotics, and aggressive diagnosis and treatment of febrile events
Acute splenic sequestration Episodes of rapid increase in splenic size and decrease
in hemoglobin Potential source of morbidity and mortality early in life
for children with sickle cell anemia and at any age for those with Hb SC disease and sickle thalassemia
Serious Complications
Strokes Up to 15% of children may have overt or silent strokes
during childhood Chronic transfusion therapy reduces the recurrence
rate of overt stroke which may approach 75% without intervention
Bone disease Early risk is primarily from osteomyelitis
Infectious usually painful inflammatory disease of bone often of bacterial origin and may result in bone tissue death
Avascular necrosis of the femur and humerus Death of bone tissue due to disrupted blood
supply Marked by severe pain in the affected region and
by weakened bone that may flatten and collapse
Serious Complications
Serious Complications Leg ulcers
Seen in patients older than 10 years of age Resistant to therapy and cause significant morbidity
Ophthalmic complications Proliferative retinopathy, vitreous hemorrhage, & retinal
detachment
Priapism Distressing complication that occurs at all ages Difficult to treat Causes a high incidence of impotence
Chronic Anemia Associated with fatigue, irritability, jaundice, pain, delayed
puberty, leg sores, eye problems, gum disease

Serious Complications: PAINRecurrent Pain Episodes or Sickling
Crises Occur at any age but appear to be
particularly frequent during late adolescence and early adult life Unpredictable Red Blood Cells get stuck in the small veins
and prevent normal blood flow Characterized by severe severe pain in the back,
chest, abdomen, extremities, and head Highly disruptive to life Most common reasons for individuals to seek
health care

1. Fever 2. Chest pain 3. Shortness of
Breath 4. Increasing
tiredness 5. Abdominal
swelling 6. Unusual headache
Danger Signs of a Crisis
7. Any sudden weakness orloss of feeling
8. Pain that will not go away with home treatment
9. Priapism (painful erection that will not go down)
10.Sudden vision changeSEEK URGENT HOSPITAL TREATMENT IF IN CRISIS

Crises During a crisis
severe pain in the fingers, toes, arms, joints,legs, back, abdomen, and bones.
Decrease in oxygen to the chest and lungs May lead to acute chest syndrome
Damage to the lungs Severe pain and fever Lungs' airways narrow, further reducing
O2 Leads to an increased risk of potentially
fatal infections

Infections Thirst and dehydration caused by not
drinking enough even if thirst is not felt Over-exertion Over-excitement Cold weather and cold drinks and
swimming Bangs, bumps, bruises and strains Stress triggers pain in adults, but does
not seem to do so in children.
Triggers of Pain

Children and families can often tell when a severe sickle pain is coming on by
Thirst Eyes turning yellow (jaundice), Sufferer being more irritable or tired
than usual.
Predicting Pain

Alleviating Pain
Warmth: increases blood flow Massaging and rubbing Heat from hot water bottles and deep heat creams Bandaging to support the painful region Resting the body Cognitive Behavioral Therapy Getting the sufferer to relax
deep breathing exercises distracting the attention by other psychological methods.
Pain-killing medicines (analgesics): paracetamol, codeine non-steroidal anti-inflammatory, morphine if necessary

1. Taking the folic acid (folate) daily to help make new red cells
2. Daily penicillin until age six to prevent serious infection
3. Drinking plenty of water daily (8-10 glasses for adults)
4. Avoiding too hot or too cold temperatures 5. Avoiding over exertion and stress 6. Getting plenty of rest 7. Getting regular check-ups from knowledgeable
health care providers
Daily Preventative Measures

Treating Complications
Pain-killing drugs and oral and intravenous fluids To reduce pain and prevent complications.
Transfusions Correct anemia Treat spleen enlargement in children before the
condition becomes life-threatening Regular transfusion therapy also can help prevent
recurring strokes in children at high risk of crippling nervous system complications.
Psychosocial Issues Require regular medical attention
Especially before and after operations, dental extraction and during pregnancy.
Adherence to medical regimen Vitamins, antibiotics, fluid intake, activity level
Schools must be involved Family planning Suitable types of employment Air travel
Increased fluids, pain killers or oxygen may be recommended

Child should be encouraged to participate in sports, but not pushed passed their limitations If they are in pain or feel tired they should be
allowed to rest and keep warm. They should have access to drinks. Strenuous exercise, dehydration and cold can
induce a crisis. Strenuous outdoor activities should be avoided in
cold or wet weather Should only swim if the water is warm and care is
taken to keep warm when leaving the water If develops a crisis despite these precautions he or
she should avoid swimming all together
Psychosocial Issues
Child Specific Issues: Coping with Pain Pain happens more often
On an average of one third of all days Lasts longer
Generally all day, even if not continuously all day
Associated with great tiredness about half the time
Causes them to spend significant time in bed On average the time spent wholly or partly in
bed adds up to about a week of every school term.
Psychosocial Issues
Variability and Unpredictability Some are mildly affected and largely free from
pain, while others have frequent and severe pain Most children go through good and bad patches Doctors cannot predict who will be severely
affected.
No easily overt detectable signs of sickle pain So children known to have sickle cell disorder
who say they are in pain must be trusted If they can rely on the adults around them to
take them seriously, they are less likely to take advantage of their condition to seek attention or avoid distasteful tasks.
Psychosocial Issues

To reduce risk of crisis, children are encouraged to drink much more than normal and more frequently May require about 1/4 litre of liquid every 60 -
90 minutes. Child will need to go to the toilet more
frequently May increase risk of Enuresis
Boys at risk for priapism May be too embarrassed to mention to parents Severe sickling can lead to impotence
Psychosocial Issues

Hydroxyurea The first effective drug treatment for adults with
severe sickle cell anemia reported in early 1995 Daily doses of the anticancer drug,
hydroxyurea, reduced the frequency of painful crises, acute chest syndrome, needed fewer blood transfusions
Increases production of fetal hemoglobin in the blood Fetal hemoglobin seems to prevent sickling
of red cells cells containing fetal hemoglobin tend to
survive longer in the bloodstream
Developing Treatments

Bone marrow transplantation Shown to provide a cure for
severely affected children with sickle cell disease
Only about 18 percent of children with sickle cell anemia are likely to have a matched sibling.
Developing Treatments

The Ultimate Cure? Gene Therapy
1. Correcting the “defective gene” and inserting it into the bone marrow
2. Turning off the defective gene and simultaneously reactivating another gene that turns on production of fetal hemoglobin.
No real cure for Sickle Cell Anemia at this time.
“In the past 30 years, the life expectancy of people with sickle cell anemia has increased. Many patients with sickle cell anemia now live into their mid-forties and beyond.”

Websiteshttp://www.sicklecellsociety.org/ : Another Great Siteinformation, Counselling and Caring for those with Sickle Cell Disorders and their families: UK based
http://www.sicklecelldisease.org/: Sickle Cell Disease Association of America
The Human Genome Project Sickle Cell Education Site at http://www.massinteraction.org/html/genome/
http://www.ascaa.org/ American Sickle Cell Anemia AssociationASCAA was founded in 1971 and is the oldest sickle cell research, education, and social services organization in the United States.
http://www.ncd.gov/
http://www.painfoundation.org/

Sites for Kidshttp://www.sicklecellsociety.org/sicklescene/pshomf.htm
Planet Sickle Cell Society (UK based)-Youth support, Poetry, Pen-Pals, Information, Message
Board
http://www.starbright.org/The STARBRIGHT Foundation is dedicated to the development of projects that empower seriousl ill children to combat the medical and emotional challenges they face on a daily basis.
Coloring Books on Sickle Cell from Emory:http://www.emory.edu/PEDS/SICKLE/bbc/index.htmhttp://www.emory.edu/PEDS/SICKLE/chelate/index.htm

Support Group Information:
Florida, Jacksonville: Sickle Cell Support Groups (904) 549-4472
Georgia, Atlanta: Parent SC Support Group (404) 616-4395
Top Related