






Languages
Pages
Legal


Pediatric Dentistry Pediatric Dentistry SeminarSeminar
Dr. Christine Bell, DMD, Cert.Ped.Dent, Dr. Christine Bell, DMD, Cert.Ped.Dent, FRCD(C)FRCD(C)
Pediatric Medical Residents Seminar SeriesPediatric Medical Residents Seminar Series
January 2013January 2013

ObjectivesObjectives
Provide a basic overview of pediatric Provide a basic overview of pediatric dentistrydentistry
Answer frequently asked questions Answer frequently asked questions raised by Family Medicine and Peds raised by Family Medicine and Peds Medicine ResidentsMedicine Residents

OverviewOverview
Normal Dental DevelopmentNormal Dental Development Abnormal Dental DevelopmentAbnormal Dental Development Early Childhood Caries Early Childhood Caries Common Pediatric DentistryCommon Pediatric Dentistry Recommendations for ParentsRecommendations for Parents When to Refer and For WhatWhen to Refer and For What Special Needs PatientsSpecial Needs Patients TraumaTrauma

Education: General Dentist Education: General Dentist and Specialistand Specialist
Undergraduate TrainingUndergraduate Training 3-4 years 3-4 years
Dental SchoolDental School 4 years4 years
General DentistGeneral Dentist
Specialty TrainingSpecialty Training 2-4 years depending on the specialty 2-4 years depending on the specialty
and the programand the program

Dental SpecialistsDental Specialists
EndodontistEndodontist Oral and Maxillofacial SurgeonOral and Maxillofacial Surgeon Orthodontist Orthodontist Pedodontist/Pediatric DentistPedodontist/Pediatric Dentist Periodontist Periodontist Prosthodontist Prosthodontist

When should the When should the first dental check first dental check
up be?up be?

The American & Canadian Academy of Pediatric The American & Canadian Academy of Pediatric Dentistry recommend a dental home be established Dentistry recommend a dental home be established as as early as 6 months of ageearly as 6 months of age oror 6 months after the 6 months after the eruption of the first tootheruption of the first tooth and definitely and definitely by 1 year of by 1 year of ageage
Age One

First Dental VisitFirst Dental Visit Comprehensive oral examination Comprehensive oral examination
acute care, preventive servicesacute care, preventive services assess for oral diseases and conditionsassess for oral diseases and conditions asses the need for fluoride asses the need for fluoride
Anticipatory guidance Anticipatory guidance teething, digit/pacifier habits, trauma, preventionteething, digit/pacifier habits, trauma, prevention
Oral hygiene instructionsOral hygiene instructions Dietary counselingDietary counseling
Prolonged breast/bottle feeding, sippy cup, juiceProlonged breast/bottle feeding, sippy cup, juice Caries- risk assessment Caries- risk assessment
determine individualized dental health plandetermine individualized dental health plan

Who can children see for Who can children see for dental exams/treatment?dental exams/treatment?
Family/General Dentist Family/General Dentist
Pediatric DentistPediatric Dentist Typically treats children from birth to Typically treats children from birth to
age 18age 18 Some offices stop seeing patients at an Some offices stop seeing patients at an
earlier age earlier age
Hospital Pediatric DentistHospital Pediatric Dentist

Alberta Children’s Alberta Children’s HospitalHospital

Alberta Children’s Hospital Alberta Children’s Hospital Pediatric Dental ClinicPediatric Dental Clinic
Patients are seen by referral onlyPatients are seen by referral only Referrals Referrals
Physicians/Medical SpecialistsPhysicians/Medical Specialists Community physicians/pediatricians Community physicians/pediatricians In-and Out-patient clinics/physiciansIn-and Out-patient clinics/physicians
Oncology, cardiology, nephrology, hematology, GIOncology, cardiology, nephrology, hematology, GI Perinatology, endocrinology, genetics, infectious Perinatology, endocrinology, genetics, infectious
diseasedisease Developmental Clinic, Neuromotor ClinicDevelopmental Clinic, Neuromotor Clinic Cleft Palate & Craniofacial Clinic, ENT, PlasticsCleft Palate & Craniofacial Clinic, ENT, Plastics Emergency DepartmentEmergency Department
Community general and pediatric dentistsCommunity general and pediatric dentists

ACH Dental Clinic ACH Dental Clinic PatientsPatients
Medically compromised and special needs Medically compromised and special needs patients from birth up to 18 yearspatients from birth up to 18 years Syndromes, autismSyndromes, autism Immune compromisedImmune compromised Bleeding disordersBleeding disorders Oncology, transplant patientsOncology, transplant patients Cardiac/vascular diseasesCardiac/vascular diseases Uncontrolled seizure disorders, etc…Uncontrolled seizure disorders, etc…
Children with craniofacial/structural anomaliesChildren with craniofacial/structural anomalies Genetic disorders, cleft lip and palate, craniofacial Genetic disorders, cleft lip and palate, craniofacial
anomalies velopharyngeal incompetency, sleep apneaanomalies velopharyngeal incompetency, sleep apnea Healthy patients under the age of 4 years with Healthy patients under the age of 4 years with
significant dental issuessignificant dental issues

Significant Dental IssuesSignificant Dental Issues
Urgent, extensive or special oral needsUrgent, extensive or special oral needs Early childhood cariesEarly childhood caries Dental/periodontal abscesses, facial cellulitisDental/periodontal abscesses, facial cellulitis Oral/dental traumaOral/dental trauma Oral surgery needs(surgical extraction, Oral surgery needs(surgical extraction,
frenectomy, gingivectomy, soft tissue biopsy)frenectomy, gingivectomy, soft tissue biopsy) Unusual/rare dental conditions (amelogenesis Unusual/rare dental conditions (amelogenesis
imperfecta, dentinogenisis imperfecta, imperfecta, dentinogenisis imperfecta, ectodermal dysplasia, cleidocranial ectodermal dysplasia, cleidocranial dysostosis etc)dysostosis etc)

Cleft Lip and Palate Cleft Lip and Palate InfantsInfants
Cleft lip and palate infants are Cleft lip and palate infants are referred to the ACH Dental Clinic for referred to the ACH Dental Clinic for consult by a Pediatric Dentist consult by a Pediatric Dentist certified in Nasoalveolar Molding certified in Nasoalveolar Molding (NAM) Therapy(NAM) Therapy

Nasoalveolar Molding Nasoalveolar Molding ApplianceAppliance
Consists of an intra-oral Consists of an intra-oral acrylic plate with extra-oral acrylic plate with extra-oral nasal stent.nasal stent.
Adjustments are made Adjustments are made weekly to the appliance to weekly to the appliance to guide tissues into a more guide tissues into a more desired position prior to desired position prior to initial lip closure procedureinitial lip closure procedure

NAM: ObjectivesNAM: Objectives Reduce the severity of Reduce the severity of
cleft deformitycleft deformity Approximate alveolar and Approximate alveolar and
lip segmentslip segments Decrease nasal base Decrease nasal base
widthwidth Shape nasal dome and Shape nasal dome and
alar cartilagealar cartilage Promote columella Promote columella
elongationelongation Allow one-stage lip and Allow one-stage lip and
nose repairnose repair No need for lip adhesion No need for lip adhesion
surgerysurgery

a c
b d

Behavior Management Behavior Management Options Options
ACH Dental ClinicACH Dental Clinic Non-pharmacologic techniquesNon-pharmacologic techniques
tell-show-dotell-show-do positive reinforcementpositive reinforcement voice controlvoice control distractiondistraction medical stabilizationmedical stabilization
Nitrous oxide inhalation sedationNitrous oxide inhalation sedation Oral conscious sedationOral conscious sedation Combination of oral and inhalation Combination of oral and inhalation
sedationsedation General anesthesiaGeneral anesthesia

2013 Pediatric Resident Seminar Series - Dr. Christine Bell
Dental Dental DevelopmentDevelopment

Basic Structure of a Basic Structure of a ToothTooth
Two “parts”Two “parts” CrownCrown RootRoot
Tooth StructureTooth Structure EnamelEnamel DentinDentin PulpPulp CementumCementum
Crown
Root

Dental DevelopmentDental Development
Two sets of teeth:Two sets of teeth: Primary DentitionPrimary Dentition
‘‘baby’ or ‘milk’ teethbaby’ or ‘milk’ teeth 20 teeth20 teeth
Secondary DentitionSecondary Dentition ‘‘adult’ or ‘permanent’ teethadult’ or ‘permanent’ teeth 32 teeth32 teeth

How are teeth How are teeth numbered?numbered?
Different tooth numbering systemsDifferent tooth numbering systems UniversalUniversal International (FDI)International (FDI) PalmerPalmer
Typically in Canada we use the Typically in Canada we use the International Tooth Numbering International Tooth Numbering System System

International Tooth International Tooth Numbering SystemNumbering System
Two digit numbering systemTwo digit numbering system First number is the quadrant numberFirst number is the quadrant number Second number is the position/number Second number is the position/number
of teeth from the midlineof teeth from the midline

Permanent TeethPermanent TeethQuadrant I Quadrant II
Quadrant IIIQuadrant IV

Primary TeethPrimary Teeth
Quadrant 5 Quadrant 6
Quadrant 7Quadrant 8
Right Left

Typical Eruption Sequence: Typical Eruption Sequence: Primary DentitionPrimary Dentition
First toothFirst tooth lower central incisor lower central incisor 6-10 months of age6-10 months of age
General trendsGeneral trends right and left erupt right and left erupt
around the same timearound the same time erupt in order from erupt in order from
front to back except front to back except the caninesthe canines
complete by 25 -33 complete by 25 -33 months of agemonths of age

Timing of Tooth EruptionTiming of Tooth Eruption
Primary Dentition
Permanent Dentition

Mixed Dentition StageMixed Dentition Stage
6 yrs – 14 yrs of age6 yrs – 14 yrs of age typically initiated with eruption of typically initiated with eruption of
the lower first permanent molarthe lower first permanent molar

What to do for What to do for teething?teething?

TeethingTeething
Massage the gums, have baby chew on cold Massage the gums, have baby chew on cold wash cloth, cold teething rings, give tylenol if wash cloth, cold teething rings, give tylenol if necessarynecessary We typically do not recommend oragel or baby We typically do not recommend oragel or baby
orageloragel Lidocaine or benzocaine contentLidocaine or benzocaine content
Studies have not confirmed strong association Studies have not confirmed strong association between tooth eruption and a range of teething between tooth eruption and a range of teething symptoms. symptoms. Study by King et.al. 1992 found HSV associated Study by King et.al. 1992 found HSV associated
with almost 50% of infants with teething difficultieswith almost 50% of infants with teething difficulties

Herpes Simplex VirusHerpes Simplex Virus
Everyone is exposed to itEveryone is exposed to it 1% present with primary herpetic 1% present with primary herpetic
gingivostomatitisgingivostomatitis Typically occurs in children <4 years of ageTypically occurs in children <4 years of age
7-18% end up with recurrent herpes 7-18% end up with recurrent herpes labialis (cold sores)labialis (cold sores)

Primary Outbreak of Primary Outbreak of Herpes Simplex Herpes Simplex
Primary Herpetic Primary Herpetic GingivostomatitisGingivostomatitis FeverFever MalaiseMalaise IrritabilityIrritability Not eating/drinking wellNot eating/drinking well Red inflamed, possibly Red inflamed, possibly
bleeding gingivableeding gingiva Herpetic ulcerations Herpetic ulcerations
intraorally, possibly extraorallyintraorally, possibly extraorally May not present with all May not present with all
signs/symptomssigns/symptoms Typically resolves within 14 daysTypically resolves within 14 days

Treatment of Primary Treatment of Primary Herpetic GingivostomatitisHerpetic Gingivostomatitis
Encourage fluidsEncourage fluids Treat fever (Tylenol)Treat fever (Tylenol) Encourage good hand hygieneEncourage good hand hygiene Educate family: viral, can Educate family: viral, can
spread/inoculate other sites (eyes, spread/inoculate other sites (eyes, herpetic whitlow), contagious (others herpetic whitlow), contagious (others can acquire)can acquire)
Antiviral meds of limited valueAntiviral meds of limited value typically prescribed if outbreak is severe or typically prescribed if outbreak is severe or
patient is immune compromised (acyclovir)patient is immune compromised (acyclovir)

Dental Dental Development Prior Development Prior
to Eruptionto Eruption

Dental DevelopmentDental Development
Initiation of all primary teeth occurs Initiation of all primary teeth occurs while IUwhile IU
Initiation of most permanent teeth Initiation of most permanent teeth occurs IU (with exception of the occurs IU (with exception of the premolars, 2premolars, 2ndnd and 3 and 3rdrd molars) molars)

Dental DevelopmentDental Development
All primary teeth begin to calcify at 4 All primary teeth begin to calcify at 4 months IUmonths IU
11stst permanent tooth to undergo permanent tooth to undergo calcification is the 1calcification is the 1stst permanent molar permanent molar (birth)(birth)
All permanent teeth with the exception of All permanent teeth with the exception of the wisdom teeth are calcified by 6-7 years the wisdom teeth are calcified by 6-7 years of ageof age

Dental DevelopmentDental Development
Complication or interruption of any Complication or interruption of any of the processes of development of the processes of development (initiation, histodifferentiation, (initiation, histodifferentiation, calcification or maturation) could calcification or maturation) could result in dental issuesresult in dental issues

2013 ACH Pediatric Resident Seminar Series - Dr. Christine Bell
Abnormal Dental Abnormal Dental DevelopmentDevelopment

Dental AnomaliesDental Anomalies Natal/Neonatal teethNatal/Neonatal teeth Extra/supernumerary teethExtra/supernumerary teeth Missing teethMissing teeth
Anodontia/oligodontiaAnodontia/oligodontia Malformed teethMalformed teeth
Microdont/macrodont/conical/twinning/Microdont/macrodont/conical/twinning/geninationgenination
Structural/mineralization anomaliesStructural/mineralization anomalies Hypocalcification/hypoplasia/fluorisis/Hypocalcification/hypoplasia/fluorisis/
amelogenesis imprefecta/dentinogenesis amelogenesis imprefecta/dentinogenesis imperfectaimperfecta

Natal/Neonatal TeethNatal/Neonatal Teeth
Natal teethNatal teeth teeth present at teeth present at
birth birth Neonatal teeth Neonatal teeth
Teeth/tooth erupt Teeth/tooth erupt during 1during 1stst month month following birthfollowing birth
Incidence 1:2500-Incidence 1:2500-3500 births3500 births
85% are 85% are mandibular incisorsmandibular incisors
90% are true 90% are true primary teethprimary teeth

TreatmentTreatment
Monitor vs extractionMonitor vs extraction
Indications for extractionIndications for extraction hyper-mobility hyper-mobility difficulties with breast feeding difficulties with breast feeding traumatic ulcerations on tongue (Riga traumatic ulcerations on tongue (Riga
Fede Disease)Fede Disease)

Dental AnomaliesDental Anomalies
Fused or Fused or geminated teethgeminated teeth
Hypoplastic toothHypoplastic tooth

Some dental development Some dental development issues may be linked to issues may be linked to genetics &/or medical genetics &/or medical
conditionsconditions Dentinogenesis imperfectaDentinogenesis imperfecta
Osteogenesis imperfectaOsteogenesis imperfecta
Oligodontia, conical teethOligodontia, conical teeth Ectodermal dysplasiaEctodermal dysplasia
Multiple supernumerary teethMultiple supernumerary teeth Cleidocranial dysostosisCleidocranial dysostosis

Dentinogenesis ImperfectaAmelogenesis Imperfecta

Ectodermal DysplasiaEctodermal Dysplasia
Conical teeth, severe oligodontia of the upper arch
Anodontia of lower arch

4 year old male with Ectodermal Dysplasia and severe oligodontia

2013 ACH Pediatric Resident Seminar Series - Dr. Christine Bell
Dental Caries Dental Caries (Cavities)(Cavities)

Dental Caries/CavitiesDental Caries/Cavities
The Centre for Disease Control & The Centre for Disease Control & Prevention reports Dental Caries as Prevention reports Dental Caries as being the being the ‘most prevalent ‘most prevalent infectious disease in our Nation’s infectious disease in our Nation’s children’children’
5x more common than asthma5x more common than asthma Estimated that >40 % of children Estimated that >40 % of children
have caries by kindergartenhave caries by kindergarten Preventable diseasePreventable disease

TIME
Fermentable Carbohydrate
Tooth
BacteriaCARIES
Etiology of Dental Caries Etiology of Dental Caries
MultifactorialMultifactorial

The Caries ProcessThe Caries Process

Streptococcus mutansStreptococcus mutans
Main bacteria responsible for Main bacteria responsible for causing tooth decaycausing tooth decay Part of natural oral floraPart of natural oral flora Can be acquired Can be acquired

Acquisition of Cariogenic Acquisition of Cariogenic BacteriaBacteria
Vertical TransmissionVertical Transmission Passing of bacteria from caregiver to childPassing of bacteria from caregiver to child Studies have shown the strain of S.mutans in the Studies have shown the strain of S.mutans in the
mouths of children are the same strain as that mouths of children are the same strain as that found in the mouths of their caregiversfound in the mouths of their caregivers
Horizontal transmissionHorizontal transmission Passing of bacteria from someone other than a Passing of bacteria from someone other than a
caregivercaregiver Studies have found that in the environment of Studies have found that in the environment of
daycares, the same strains of S.mutans are found daycares, the same strains of S.mutans are found among the childrenamong the children

Strategies to minimize Strategies to minimize transmission from primary transmission from primary
caregiverscaregivers improve caregivers oral hygiene and improve caregivers oral hygiene and
dental healthdental health do not share utensils or tooth brushesdo not share utensils or tooth brushes do not clean soother with your mouthdo not clean soother with your mouth Pre-chewing food is not recommendedPre-chewing food is not recommended
this is a practice in some culturesthis is a practice in some cultures

DemineralizationDemineralization
First stage of tooth decay First stage of tooth decay white spot lesion white spot lesion
Chalky white area usually following Chalky white area usually following curvature of the gum linecurvature of the gum line
demineralized enameldemineralized enamel
As the demineralization progresses, the surface layer becomes weaker and eventually collapses resulting in a cavity

White Spot LesionsWhite Spot Lesions

The Caries ProcessThe Caries Process
Dental decay is associated with Dental decay is associated with frequencyfrequency and and durationduration of of exposure to cariogenic exposure to cariogenic substancessubstances
more frequent and longer duration of sugar in the more frequent and longer duration of sugar in the mouth produces a lower pH and longer exposure to mouth produces a lower pH and longer exposure to the change in pH (favoring demineralization)the change in pH (favoring demineralization)

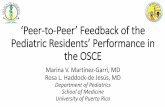
Stephan CurveStephan Curve
Minutes
7
6
5
10 20 30 400
pHCritical pH
Demineralization
Re-mineralization
- The average baseline oral pH is ~7
- pH of 5.5 is considered the critical pH
- The Stephan Curve shows changes in oral pH following exposure to a sucrose solution
- pH drops significantly below the critical pH on initial exposure
- takes ~20 minutes to recover to the critical pH and ~40 minutes to return to baseline
5.5

Early Childhood Caries Early Childhood Caries (ECC)(ECC)
May be referred to as:May be referred to as: Baby bottle decay/Baby bottle mouthBaby bottle decay/Baby bottle mouth Nursing bottle syndrome/Nursing cariesNursing bottle syndrome/Nursing caries Rampant cariesRampant caries

What is the impact of ECC What is the impact of ECC on a Child’s quality of life?on a Child’s quality of life?
Pre-school children do not necessarily Pre-school children do not necessarily complain of tooth pain complain of tooth pain they manifest the effects of pain by changing eating they manifest the effects of pain by changing eating
and sleeping patternsand sleeping patterns
Reported effects of untreated caries include:Reported effects of untreated caries include: Low percentile weights or failure to thriveLow percentile weights or failure to thrive Risk of delayed physical growth and developmentRisk of delayed physical growth and development Loss of school daysLoss of school days Diminished ability to learn: irritability, inability to Diminished ability to learn: irritability, inability to
concentrateconcentrate PainPain Risk of dental abscess, facial cellulitis and Risk of dental abscess, facial cellulitis and
potentially life threatening infections (Ludwig’s potentially life threatening infections (Ludwig’s angina, cavernous sinus thrombosis)angina, cavernous sinus thrombosis)
Hospitalizations and emergency room visitsHospitalizations and emergency room visits

Resolving Periorbital Resolving Periorbital Cellulitis Secondary to Cellulitis Secondary to Odontogenic InfectionOdontogenic Infection

We need to work together to We need to work together to help decrease the prevalence help decrease the prevalence
of this preventable diseaseof this preventable disease

Physician’s Role in Caries Physician’s Role in Caries PreventionPrevention
Early identification and referral of Early identification and referral of high risk childrenhigh risk children
Discuss caries prevention Discuss caries prevention information with familiesinformation with families

Caries Risk AssessmentCaries Risk Assessment
A systematic evaluation A systematic evaluation looks at the presence and intensity of looks at the presence and intensity of
etiologic disease factorsetiologic disease factors It is designed to provide an estimation It is designed to provide an estimation
of disease susceptibility of disease susceptibility aids in formulating preventative and aids in formulating preventative and
treatment strategiestreatment strategies

Caries Risk Screening Caries Risk Screening ToolTool
Caries-risk Assessment tool (CAT):Caries-risk Assessment tool (CAT): Check list Check list
Gather information from a primary caregiverGather information from a primary caregiver Conduct clinical evaluation of child’s mouthConduct clinical evaluation of child’s mouth
Can be used by dental and non-dental Can be used by dental and non-dental health care providers health care providers
American Academy of Pediatric Dentistry American Academy of Pediatric Dentistry website: website: www.aapd.org
Provides a current caries risk assessment formProvides a current caries risk assessment form

Risk Factors for Caries Risk Factors for Caries DevelopmentDevelopment
Primary caregiver or sibling with active cariesPrimary caregiver or sibling with active caries Low socioeconomic statusLow socioeconomic status Child has >3 between meal sugar containing Child has >3 between meal sugar containing
snacks/beverages per daysnacks/beverages per day Child is put to bed with bottle/cup containing Child is put to bed with bottle/cup containing
something other than watersomething other than water Not receiving optimally fluoridated drinking Not receiving optimally fluoridated drinking
water or fluoride supplementswater or fluoride supplements White spot lesions on teethWhite spot lesions on teeth Visible cavities or fillingsVisible cavities or fillings Visible plaque on teeth (poor oral hygiene)Visible plaque on teeth (poor oral hygiene) special health care needsspecial health care needs Recent immigrantRecent immigrant

Other Risk Factors for Other Risk Factors for Caries DevelopmentCaries Development
Breast or bottle feeding Breast or bottle feeding beyond 12 months of agebeyond 12 months of age
feeding throughout the feeding throughout the night or allowing baby to night or allowing baby to fall asleep for the night fall asleep for the night while feeding while feeding
Oral medications Oral medications (suspensions, inhalers)(suspensions, inhalers)
Nutritional supplements Nutritional supplements such as Pediasure or such as Pediasure or Nutren Junior etc.Nutren Junior etc.

Physician’s Role with Physician’s Role with Dental Caries PreventionDental Caries Prevention
Ask families if they have a dentist for their childAsk families if they have a dentist for their child are they seeing a dentist regularlyare they seeing a dentist regularly recommend first dental visit by age onerecommend first dental visit by age one
Review feeding habits Review feeding habits Prolonged breast/bottle/sippy cup use and feeding Prolonged breast/bottle/sippy cup use and feeding
throughout the night throughout the night juice, grazing habits, hidden sugarsjuice, grazing habits, hidden sugars
Discuss oral hygiene practicesDiscuss oral hygiene practices Brush 2x day by parentBrush 2x day by parent Start using fluoride toothpaste at age 3 (1/2 pea sized Start using fluoride toothpaste at age 3 (1/2 pea sized
amount)amount) <3 years of age; fluoride use is prescribed on an <3 years of age; fluoride use is prescribed on an
individual basis by the dentistindividual basis by the dentist Do not share tooth brushes Do not share tooth brushes

Lift the Lip



Look for…Look for…
Dental caries at any stage of progressionDental caries at any stage of progression Chipped or broken teethChipped or broken teeth Crooked/crowded teethCrooked/crowded teeth Discolored teethDiscolored teeth AbscessesAbscesses Poor oral hygienePoor oral hygiene Red inflamed gumsRed inflamed gums AnomaliesAnomalies

You may find…You may find…
White spot lesion
decay
abscess

Discolored tooth - indicates pulp necrosis Supernumerary tooth (“mesodens”)
Retained primary teeth
Stain/poor oral hygiene
1 2
3 4

Crossbite
Open bite Crowding
MalocclusionsMalocclusionsR L

Eruption CystsEruption Cysts May appear as a bluish-black or May appear as a bluish-black or
translucent, smooth, painless swelling translucent, smooth, painless swelling over an area of an unerupted toothover an area of an unerupted tooth
associated with an erupting primary or associated with an erupting primary or permanent toothpermanent tooth
no treatment necessaryno treatment necessary

Generalized Gingival Generalized Gingival HyperplasiaHyperplasia
Fibrous overgrowth Fibrous overgrowth of gingivaof gingiva CongenitalCongenital
Gingival fibromatosisGingival fibromatosis MucopolysaccharidosMucopolysaccharidos
es (Hunter, Hurler es (Hunter, Hurler syndrome, I-Cell syndrome, I-Cell disease)disease)
AcquiredAcquired Plaque induced/poor Plaque induced/poor
oral hygieneoral hygiene AML, aplastic anemiaAML, aplastic anemia Medication inducedMedication induced

Common Medications Common Medications Linked to Gingival Linked to Gingival
OvergrowthOvergrowth
CyclosporinCyclosporin Calcium Calcium
channel channel blockersblockers
Anti-seizure Anti-seizure medsmeds

GingivectomyGingivectomy

When to referWhen to refer Recommend they see a dentist if they do Recommend they see a dentist if they do
not have one and:not have one and: No sign of decayNo sign of decay No significant findingsNo significant findings Low risk for cariesLow risk for caries
Refer to a dentistRefer to a dentist Obvious decay or dental traumaObvious decay or dental trauma Significant findingsSignificant findings High risk for cariesHigh risk for caries

2013 ACH Pediatric Resident Seminar Series - Dr. Christine Bell
Oral HygieneOral Hygiene

Oral Hygiene Oral Hygiene RecommendationsRecommendations
Parents should brush their Parents should brush their children’s teeth until they are children’s teeth until they are about 8 yrs oldabout 8 yrs old
Always use a soft bristled Always use a soft bristled toothbrushtoothbrush
Floss teeth that are contacting Floss teeth that are contacting one anotherone another
Rule of 2’sRule of 2’s Brush 2x a day, for 2 minutes and Brush 2x a day, for 2 minutes and
visit the a dentist 2x a year for visit the a dentist 2x a year for regular check-upsregular check-ups

Oral Hygiene Oral Hygiene RecommendationsRecommendations
Prior to eruption of first tooth Prior to eruption of first tooth wipe gums with wet washcloth at least 1x daywipe gums with wet washcloth at least 1x day
Eruption of first toothEruption of first tooth Wipe tooth and gums with a wet washcloth 2x Wipe tooth and gums with a wet washcloth 2x
day or after every feedday or after every feed Be aware that feeding during the night or at Be aware that feeding during the night or at
bedtime can cause tooth decaybedtime can cause tooth decay Eruption of molarsEruption of molars
Use toothbrush with water or ‘safe to swallow’ Use toothbrush with water or ‘safe to swallow’ toothpaste 2x dailytoothpaste 2x daily

Recommendations:Recommendations:Fluoride UseFluoride Use
Under 3 years of ageUnder 3 years of age non-fluoridated toothpaste is non-fluoridated toothpaste is
recommendedrecommended fluoride recommendations based on fluoride recommendations based on
caries risk assessment caries risk assessment dentist develops an individualized dentist develops an individualized
caries prevention plan and caries prevention plan and recommendations for fluoride userecommendations for fluoride use

Recommendations: Recommendations: Oral Hygiene and Fluoride Oral Hygiene and Fluoride
UseUse Age 3-6 Age 3-6
Brushing 2x day using fluoride toothpaste Brushing 2x day using fluoride toothpaste (grain of rice sized to half the size of a pea (grain of rice sized to half the size of a pea amount of toothpaste)amount of toothpaste)
Flossing 1x day where teeth are Flossing 1x day where teeth are contactingcontacting
> 6 years of age> 6 years of age Brushing 2x day using fluoride toothpaste Brushing 2x day using fluoride toothpaste
(pea sized amount of toothpaste)(pea sized amount of toothpaste) Flossing 1x dayFlossing 1x day

Mechanism of Action of Mechanism of Action of FluorideFluoride
Topical and Post-eruptive Topical and Post-eruptive Increases the remineralization processIncreases the remineralization process
Catalyst for remineralization (Ca, PO4)Catalyst for remineralization (Ca, PO4) Prevents demineralizationPrevents demineralization
Decreases tooth solubilityDecreases tooth solubility Decreases bacterial acid productionDecreases bacterial acid production
Inhibits enolase, enzyme required in glycolysisInhibits enolase, enzyme required in glycolysis

Water FluoridationWater Fluoridation
Optimum water fluoride level Optimum water fluoride level 1 ppm (1.0mgF/L)1 ppm (1.0mgF/L) recommended range = 0.7-1.2 ppmrecommended range = 0.7-1.2 ppm

Fluoride Supplement Fluoride Supplement ScheduleSchedule
Fluoride concentration in community drinking H2OFluoride concentration in community drinking H2O
AgeAge < 0.3 ppm< 0.3 ppm 0.3-0.6 0.3-0.6 ppmppm
> 0.6 > 0.6 ppmppm
0-6 months0-6 months nonenone nonenone nonenone
6mo-3yr6mo-3yr 0.25mg/0.25mg/dayday
nonenone nonenone
3-6yr3-6yr 0.50mg/0.50mg/dayday
0.25mg/0.25mg/dayday
nonenone
6-16yr6-16yr 1.0mg/1.0mg/
dayday0.50mg/day0.50mg/day nonenone

Fluoride SupplementsFluoride Supplements
Very rarely do we Rx systemic Very rarely do we Rx systemic fluoride supplementsfluoride supplements
Consider Consider all all sources of fluoridesources of fluoride Young children with incipient decay Young children with incipient decay
(white spot lesions) may benefit from (white spot lesions) may benefit from application of fluoride varnishapplication of fluoride varnish

Dental FluorosisDental Fluorosis
Ingestion of too much Ingestion of too much fluoride during the fluoride during the mineralization stage mineralization stage in tooth development in tooth development may cause fluorosismay cause fluorosis

2013 ACH Pediatric Residency Seminar Series - Dr. Christine Bell
Common Pediatric Common Pediatric DentistryDentistry

Common Pediatric Common Pediatric Dentistry Dentistry
PreventionPrevention Routine dental exams, cleanings, Routine dental exams, cleanings,
fluoride applicationfluoride application Sealants (recommended on molars with Sealants (recommended on molars with
deep grooves)deep grooves)

Common Pediatric Common Pediatric Dentistry Dentistry
RestorationsRestorations Composite restorations (white fillings)Composite restorations (white fillings) Amalgam restorations (silver fillings)Amalgam restorations (silver fillings) Stainless steel crownsStainless steel crowns Nerve treatments Nerve treatments
(pulpotomies/pulpectomies/root canal (pulpotomies/pulpectomies/root canal treatments)treatments)

Common Pediatric Common Pediatric Dentistry TreatmentDentistry Treatment
ExtractionsExtractions SpacemaintenanceSpacemaintenance Guidance/monitoring of occlusionGuidance/monitoring of occlusion

Why fix a baby tooth? They Why fix a baby tooth? They just fall out, don’t they?just fall out, don’t they?
Primary teeth are important: Primary teeth are important: ChewingChewing SpeakingSpeaking EstheticsEsthetics Hold space for the adult teethHold space for the adult teeth Gives face shape and formGives face shape and form
If not restored, decay will continue to If not restored, decay will continue to worsen and eventually lead to pain, worsen and eventually lead to pain, discomfort and infectiondiscomfort and infection

Special Needs and Special Needs and Medically Compromised Medically Compromised
ChildrenChildren

Special Needs and Special Needs and Medically Compromised Medically Compromised
ChildrenChildren
Unique medical and dental needsUnique medical and dental needs May not be the most cooperative May not be the most cooperative
dental patientsdental patients Best seen by a Pediatric DentistBest seen by a Pediatric Dentist
Private practice Pediatric DentistPrivate practice Pediatric Dentist Hospital based Pediatric Dentist Hospital based Pediatric Dentist

Children with Special Children with Special Health Care NeedsHealth Care Needs
Typically have one or more risk factors Typically have one or more risk factors predisposing them to dental diseasepredisposing them to dental disease Delayed first dental visitDelayed first dental visit
Complex medical needsComplex medical needs Parents overwhelmed with medical issuesParents overwhelmed with medical issues
Limited cooperation for home oral hygieneLimited cooperation for home oral hygiene Mental and/or physical disability complicates Mental and/or physical disability complicates
oral hygiene processoral hygiene process Perioral sensitivityPerioral sensitivity Behavior issuesBehavior issues

Possible Risk Factors of Possible Risk Factors of Children with Special Children with Special
Health Care NeedsHealth Care Needs DietaryDietary
Need for frequent high calorie feedings, Need for frequent high calorie feedings, night feedingsnight feedings
Tube feedingTube feeding Behavior reinforcing therapy with sweet Behavior reinforcing therapy with sweet
treatstreats Greater exposure to medicationsGreater exposure to medications
Xerostomia is common side effect of many Xerostomia is common side effect of many medicationsmedications
Suspensions contain sugarSuspensions contain sugar Oral steroids/inhalers linked to tooth decayOral steroids/inhalers linked to tooth decay

Possible Risk Factors of Possible Risk Factors of Children with Special Children with Special
Health Care NeedsHealth Care Needs Oral motor dysfunction/parafunctionOral motor dysfunction/parafunction
Chewing, swallowing problemsChewing, swallowing problems Grinding/clenchingGrinding/clenching Self biting (lip, cheek)Self biting (lip, cheek) Chewing objectsChewing objects Pouching of foodPouching of food
Gastro-esophageal reflux, frequent vomitingGastro-esophageal reflux, frequent vomiting Greater susceptibilityGreater susceptibility
Periodontal disease (Down Syndrome)Periodontal disease (Down Syndrome) Trauma (CP, seizure disorder)Trauma (CP, seizure disorder) Neglect and abuseNeglect and abuse

Tube Fed ChildrenTube Fed Children
Oral aversionsOral aversions Uncooperative for tooth brushingUncooperative for tooth brushing
Aspiration riskAspiration risk Parents afraid to brush teeth as worried Parents afraid to brush teeth as worried
about secretionsabout secretions No oral feedsNo oral feeds
Parents incorrectly think they are not Parents incorrectly think they are not eating so no need to brush teetheating so no need to brush teeth
May take tastes, usually sweet May take tastes, usually sweet foods/drinksfoods/drinks

Common Oral Findings with Common Oral Findings with Tube Fed ChildrenTube Fed Children
Significant calculus build-upSignificant calculus build-up GingivitisGingivitis Periodontal diseasePeriodontal disease
Possible GERDPossible GERD Acid erosion of teethAcid erosion of teeth

Calculus: 2 year old G-Tube Calculus: 2 year old G-Tube fed patientfed patient

Gastro-esophageal Reflux Gastro-esophageal Reflux (GERD)(GERD)
Enamel erosion Enamel erosion due to acid refluxdue to acid reflux
Role of physicianRole of physician AwarenessAwareness ReferralReferral
Importance of Importance of early detection, early detection, prevention and prevention and rehabilitationrehabilitation

Cardiac PatientsCardiac Patients
Some are at risk of Bacterial Some are at risk of Bacterial EndocarditisEndocarditis Prophylactic antibiotic coverage may be Prophylactic antibiotic coverage may be
indicated prior to dental treatmentindicated prior to dental treatment Prior to open heart surgery patients Prior to open heart surgery patients
require dental clearance letterrequire dental clearance letter Cardiac surgery may be cancelled if Cardiac surgery may be cancelled if
unable to complete dental work before unable to complete dental work before scheduled surgeryscheduled surgery

Transplant PatientsTransplant Patients
Will be immune suppressed Will be immune suppressed Should have all dental treatment Should have all dental treatment
completed prior to transplantcompleted prior to transplant bone marrow or organ transplant bone marrow or organ transplant
may be postponed if oral health is may be postponed if oral health is not satisfactorynot satisfactory

Immune Compromised Immune Compromised Patients and Oncology Patients and Oncology
PatientsPatients
Issues with low counts (CBC)Issues with low counts (CBC) Issues with low plateletsIssues with low platelets Unable to deal with infectionUnable to deal with infection
Septicemia/BacteremiaSepticemia/Bacteremia Delayed healingDelayed healing Other serious complicationsOther serious complications

Prior to Dental WorkPrior to Dental Work
Consult specialist teamConsult specialist team Proper timing for safe dental treatmentProper timing for safe dental treatment
Blood work, medications/antibiotics, Blood work, medications/antibiotics, transfusion etc may be necessary transfusion etc may be necessary pre and post dental treatmentpre and post dental treatment
Dental work, dental cleanings etc Dental work, dental cleanings etc may need to be postponed until may need to be postponed until health of patient is more idealhealth of patient is more ideal

Absolute Neutrophil Count Absolute Neutrophil Count (ANC) and Dental (ANC) and Dental
TreatmentTreatment ANC >1000/mm3 ANC >1000/mm3
No antibiotic prophylaxis necessary No antibiotic prophylaxis necessary unless infection presentunless infection present
ANC of 500-1000/mm3ANC of 500-1000/mm3 Antibiotics indicated, may defer Antibiotics indicated, may defer
treatmenttreatment ANC <500/mm3ANC <500/mm3
Defer elective dental treatmentDefer elective dental treatment

Platelet Count and Dental Platelet Count and Dental TreatmentTreatment
>75, 000>75, 000 no additional support except aggressive no additional support except aggressive
local measureslocal measures 40, 000-75,00040, 000-75,000
consider platelet transfusion prior to consider platelet transfusion prior to and 24 hrs post dental treatmentand 24 hrs post dental treatment
<40, 000<40, 000 defer caredefer care

Considerations: Bleeding Considerations: Bleeding DisordersDisorders
May need factors, transfusions etcMay need factors, transfusions etc Early detection and early treatment Early detection and early treatment
allows for minor procedures and less allows for minor procedures and less bleeding issues/complicationsbleeding issues/complications

2013 ACH Pediatric Resident Seminar Series - Dr. Christine Bell
Antibiotics in Antibiotics in DentistryDentistry

Antibiotic ProphylaxisAntibiotic Prophylaxis
May be indicated for some patients:May be indicated for some patients: Cardiac conditions at risk for sub-acute Cardiac conditions at risk for sub-acute
bacterial endocarditisbacterial endocarditis Immune compromised patientsImmune compromised patients Patients with VA (ventricular-arterial) Patients with VA (ventricular-arterial)
shunts, indwelling vascular catheters shunts, indwelling vascular catheters (central line, chemo-port)(central line, chemo-port)
Some orthopedic patients (VEPTR, joint Some orthopedic patients (VEPTR, joint replacements)replacements)

Antibiotic CoverageAntibiotic Coverage
Cardiac and Immune Compromised Cardiac and Immune Compromised Patients:Patients: Follow American Heart Association Follow American Heart Association
Guidelines – reviewed/revised 2007Guidelines – reviewed/revised 2007 Amoxicillin: 50mg/kg (max 2g) 1 hr prior to Amoxicillin: 50mg/kg (max 2g) 1 hr prior to
dental proceduredental procedure Clindamycin: 20mg/kg (600mgs) 1 hr priorClindamycin: 20mg/kg (600mgs) 1 hr prior
Orthopedic Patients:Orthopedic Patients: Follow the American Academy of Follow the American Academy of
Orthopedic Surgeons GuidelinesOrthopedic Surgeons Guidelines 50mg/kg Keflex 1 hr prior; amoxicillin or 50mg/kg Keflex 1 hr prior; amoxicillin or
clindamycin could be given insteadclindamycin could be given instead

Reason for coverageReason for coverage
Dental procedures may cause a Dental procedures may cause a transient bacteremia transient bacteremia Prevent seeding of bacteria in Prevent seeding of bacteria in
susceptible areasusceptible area Vulnerable areas of the heartVulnerable areas of the heart Certain implanted hardware (VEPTR)Certain implanted hardware (VEPTR) Central lines, etcCentral lines, etc
Those with compromised immune Those with compromised immune systems may be unable to handle a systems may be unable to handle a transient bacteremiatransient bacteremia

Potential Oral Source of Potential Oral Source of BacteremiaBacteremia
Routine tooth brushing or chewingRoutine tooth brushing or chewing Poor oral/dental hygienePoor oral/dental hygiene Periodontal or dental infectionsPeriodontal or dental infections Oral/dental procedures associated Oral/dental procedures associated
with bleedingwith bleeding

Immune CompromisedImmune Compromised Includes but not limited to:Includes but not limited to:
Chemotherapy, radiation, bone marrow transplantChemotherapy, radiation, bone marrow transplant HIV, diabetesHIV, diabetes NeutropeniaNeutropenia Chronic steroid useChronic steroid use Hemodialysis Hemodialysis Status post splenectomyStatus post splenectomy Organ transplantOrgan transplant
Consultation with medical specialist Consultation with medical specialist indicatedindicated
Standard AHA prophylactic regimen Standard AHA prophylactic regimen recommendedrecommended

Hemodialysis: Coverage is Hemodialysis: Coverage is two foldtwo fold
Immune suppressed Immune suppressed At risk of infective endocarditis even At risk of infective endocarditis even
in the absence of a structural in the absence of a structural cardiac defectcardiac defect Altered host defenceAltered host defence Altered cardiac output and mechanical Altered cardiac output and mechanical
stressesstresses Bacterial seeding and growth on shuntsBacterial seeding and growth on shunts

Peritoneal DialysisPeritoneal Dialysis
Lower risk for infection of catheter Lower risk for infection of catheter from transient bacteremiafrom transient bacteremia
Have altered host defencesHave altered host defences Antibiotic prophylaxis may be Antibiotic prophylaxis may be
recommended; consultation is recommended; consultation is indicatedindicated

Considerations when Considerations when Prescribing Prophylactic Prescribing Prophylactic
AntibioticsAntibiotics Patients already receiving antibioticsPatients already receiving antibiotics
select drug of different class, orselect drug of different class, or delay procedure 10-14 days after delay procedure 10-14 days after
completion of the antibioticcompletion of the antibiotic Need for multiple visitsNeed for multiple visits
wait 10-14 days between appointmentswait 10-14 days between appointments Unanticipated bleedingUnanticipated bleeding
effective prophylaxis up to 2 hrs post-opeffective prophylaxis up to 2 hrs post-op

Antibiotics and Dental Antibiotics and Dental InfectionsInfections
Dental abscessDental abscess Antibiotics typically if systemically involved Antibiotics typically if systemically involved Pen VK, Amoxicillin, ClindamycinPen VK, Amoxicillin, Clindamycin
Facial cellulitisFacial cellulitis Mild-Moderate: PO antibiotics (eg. Mild-Moderate: PO antibiotics (eg.
Clindamycin)Clindamycin) Moderate-severe: IV antibiotics (eg. Moderate-severe: IV antibiotics (eg.
Clindamycin or Flagyl/ancef) Clindamycin or Flagyl/ancef)

Dental InfectionsDental Infections
Dental treatment necessary Dental treatment necessary primary tooth: extractionprimary tooth: extraction permanent tooth: extraction vs root canal permanent tooth: extraction vs root canal
treatmenttreatment
Dental infections will return if tooth Dental infections will return if tooth is not treated appropriatelyis not treated appropriately

Seek the most up-to-date Seek the most up-to-date information for antibiotic information for antibiotic
recommendationsrecommendations It is possible that these current It is possible that these current
recommendations may change as the result of recommendations may change as the result of more advanced research and of the ongoing more advanced research and of the ongoing clinical guidelines development of professional clinical guidelines development of professional associations and academiesassociations and academies
Therefore, clinicians are encouraged to Therefore, clinicians are encouraged to consider the recommendations in the context of consider the recommendations in the context of their specific clinical situation and consult, their specific clinical situation and consult, where appropriate, other sources of clinical, where appropriate, other sources of clinical, scientific, or regulatory information prior to scientific, or regulatory information prior to making a treatment decision and seek most-up-making a treatment decision and seek most-up-to-date informationto-date information

2013 ACH Pediatric Resident Seminar Series - Dr. Christine Bell
Dental TraumaDental Trauma

Dental TraumaDental Trauma FracturesFractures
Ellis Class I:Ellis Class I: enamel onlyenamel only patient usually not sensitivepatient usually not sensitive
Ellis Class II:Ellis Class II: enamel and dentin enamel and dentin usually sensitive to hot/cold usually sensitive to hot/cold
and airand air Ellis Class III:Ellis Class III:
enamel, dentin and pulp enamel, dentin and pulp you see red and they are in you see red and they are in
painpain Root fracturesRoot fractures Alveolar fracturesAlveolar fractures

Pulp ExposuresPulp Exposures
Pinpoint pulp exposure
Frank pulp exposure

Displacement InjuriesDisplacement Injuries Concussion (A) Concussion (A)
no mobility, no displacementno mobility, no displacement
Subluxation (B) Subluxation (B) loose but not displacedloose but not displaced
Extrusion (C) Extrusion (C) displaced away from the displaced away from the
gumsgums ie. the tooth looks longerie. the tooth looks longer
Lateral Luxation (D) Lateral Luxation (D) displaced forward or displaced forward or
backwardbackward May be accompanied by May be accompanied by
alveolar fracturealveolar fracture
Intrusion (E) Intrusion (E) displaced into the gumsdisplaced into the gums ie. the tooth looks shorterie. the tooth looks shorter
Avulsion (F) Avulsion (F) tooth completely out of the tooth completely out of the
socketsocket

1 2
3 4


Dental trauma that shouldn’t Dental trauma that shouldn’t wait till tomorrow for wait till tomorrow for
treatmenttreatment Patient cannot close teeth all the way Patient cannot close teeth all the way togethertogether
Fractures involving pulpFractures involving pulp Mobility greater than 3mmMobility greater than 3mm Intruded teethIntruded teeth Extruded teethExtruded teeth Avulsions Avulsions
This is a true dental emergencyThis is a true dental emergency survival is dependant on time out of the mouthsurvival is dependant on time out of the mouth immediately place tooth in milk immediately place tooth in milk ideally, place tooth back in the socket (permanent ideally, place tooth back in the socket (permanent
teeth)teeth) DO NOTDO NOT replant primary teeth replant primary teeth


Intrusion
Intrusion
Lateral luxation
What do you think?

Complete IntrusionComplete Intrusion
Looks like an avulsionLooks like an avulsion Palpate buccal gingivaPalpate buccal gingiva
may feel a bumpmay feel a bump
Radiograph to confirm Radiograph to confirm diagnosisdiagnosis

Where could the missing Where could the missing tooth or tooth fragment be?tooth or tooth fragment be?1)1) lost extra-orallylost extra-orally
2)2) ingestedingested
3)3) aspiratedaspirated
4)4) tissue inclusiontissue inclusion


Alberta Children’s Alberta Children’s HospitalHospital
Dental traumaDental trauma Pediatric Dentist is on call 24/7 at ACHPediatric Dentist is on call 24/7 at ACH
Facial cellulitis/odontogenic Facial cellulitis/odontogenic infectionsinfections Emergency department physicians may Emergency department physicians may
Rx antibiotics (IV/ PO). Patients are Rx antibiotics (IV/ PO). Patients are instructed to follow up with their instructed to follow up with their dentist, or referred to a dentist dentist, or referred to a dentist (possibly the one on call)(possibly the one on call)

2013 ACH Pediatric Resident Seminar Series - Dr. Christine Bell
Questions?Questions?
Thank you !Thank you !
Top Related