





Languages
Pages
Legal

PANCREATIC SONOGRAPHIC anatomy
Dr.mohamed soliman
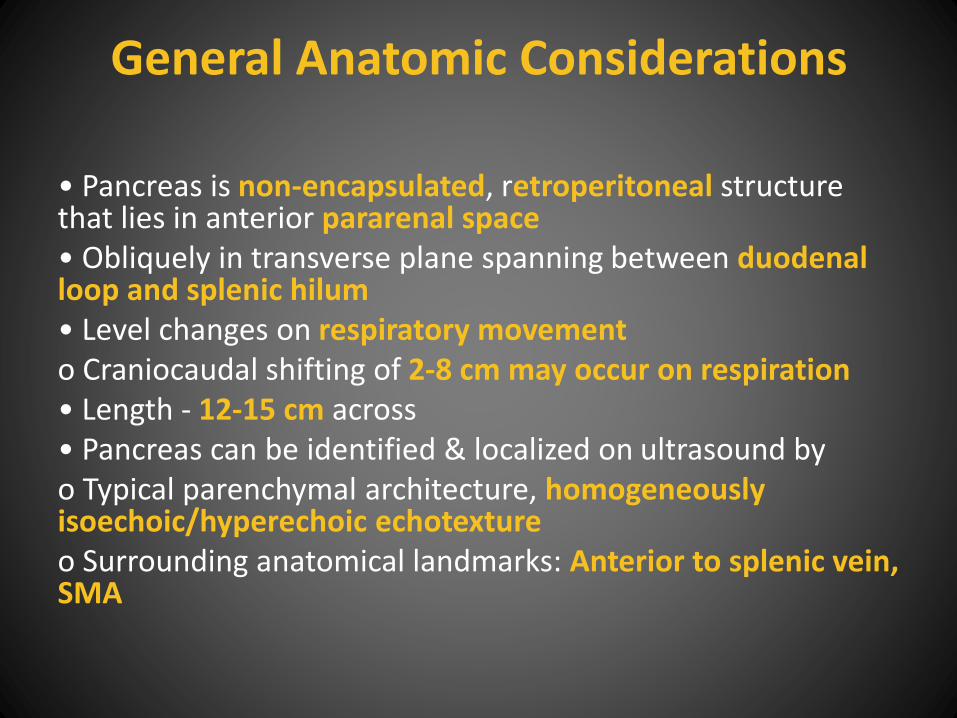
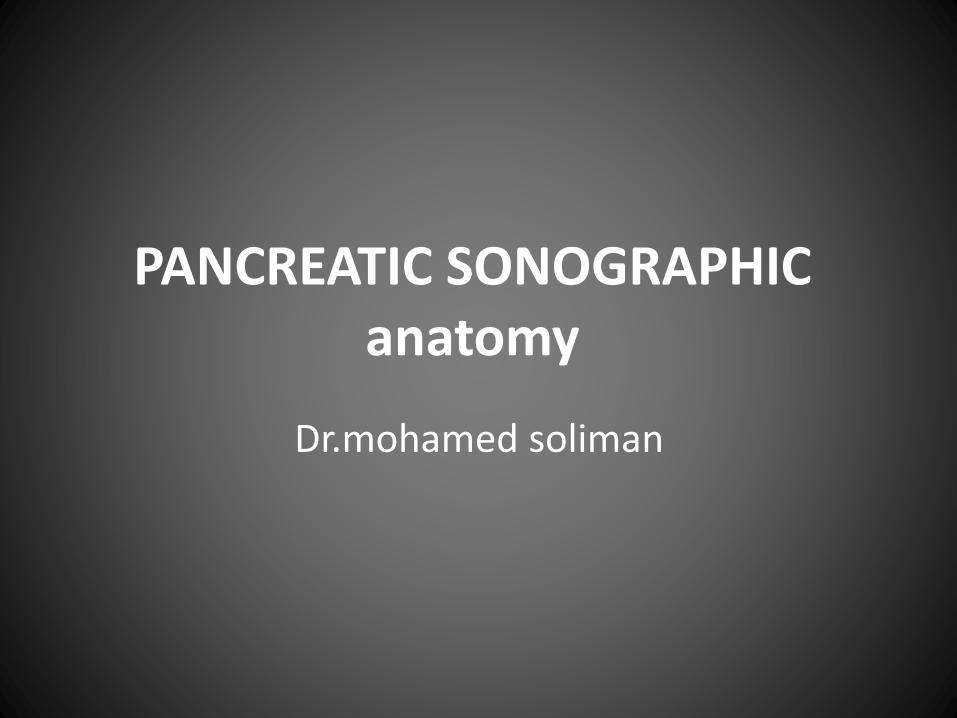
General Anatomic Considerations
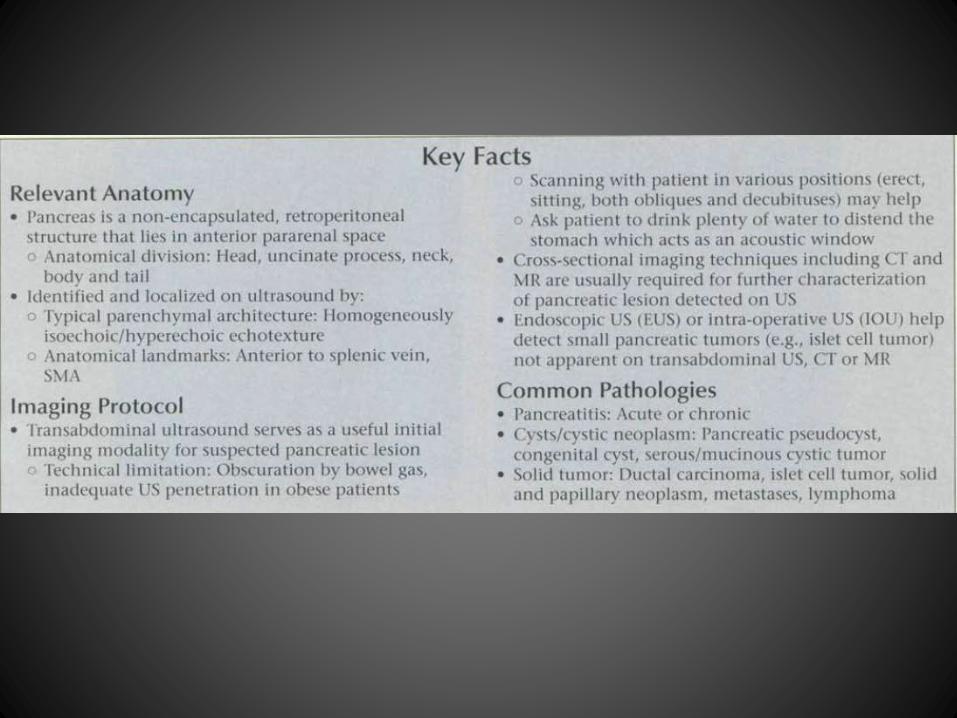
• Pancreas is non-encapsulated, retroperitoneal structure that lies in anterior pararenal space• Obliquely in transverse plane spanning between duodenal loop and splenic hilum• Level changes on respiratory movemento Craniocaudal shifting of 2-8 cm may occur on respiration• Length - 12-15 cm across• Pancreas can be identified & localized on ultrasound byo Typical parenchymal architecture, homogeneously isoechoic/hyperechoic echotextureo Surrounding anatomical landmarks: Anterior to splenic vein, SMA
Critical Anatomic Structures• Anatomical division
o Head: Parenchyma to the right of superior mesenteric vesselso Uncinate process: Represents medial extension of head• Lies posterior to superior mesenteric vesselso Neck: Narrow portion anterior to superior mesenteric vessels• Serves as dividing line between pancreatic head and bodyo Body: Parenchyma to left of superior mesenteric vessels• Constitute main bulk of pancreatic parenchymao Tail: Most distal portion of pancreatic parenchyma• No clear anatomic landmark separates tail from body
Critical Anatomic Structures• Histological division
o Functionally the pancreas comprised of exocrine and endocrine tissues
• 80% exocrine tissue; ductal and acinar cells
• 2% endocrine tissue; islet cell of Langerhans
• 18% fibrous stroma containing blood vessels,
nerves and lymphatics
Anatomic Relationships
• Pancreas is closely related to several important
structures/ organs
o Gastrointestinal tract & peritoneal spaces
• Anteriorly: Stomach, transverse colon and
root of transverse mesocolon, lesser sac
• Right: Duodenal loop (esp. second part of
duodenum)
Anatomic Relationships - Major vessels• Abdominal aorta: Posterior to body of pancreas
• Coeliac axis: Related to superior border of pancreas
• Common hepatic artery: Branch of coeliac axis, related to superior border of
pancreatic neck and head
• Gastroduodenal artery: Branch of coeliac axis, coursing inferiorly anterior to
pancreatic head
• Splenic artery: Branch of coeliac axis, towards the left in tortuous course along superior
border of pancreatic body and tail
• Superior mesenteric artery (SMA): Arises from abdominal aorta just caudal to
inferior border of pancreas, descends anterior to uncinate process
• Inferior vena cava: Posterior to head of pancreas
• Splenic vein: Coursing transversely from splenic hilum to portal vein confluence posterior
to pancreatic tail and body
• Superior mesenteric vein: Ascends to right of SMA anterior to uncinate process
• Portal vein: Confluence posterior to pancreatic neck, proximal portion above superior
margin of pancreatic head
Anatomic Relationships - Common bile duct
• Distal portion posterior to or embedded within
pancreatic head
• Forms common trunk with pancreatic duct in
80% to drain into ampulla of Vater
Imaging technique• Transabdominal ultrasound serves as a useful initial imaging modality for
suspected pancreatic lesion
• Advantages of USo Readily available o Relatively inexpensive imaging technique
o Does not involve ionizing radiation o Supplemented with Doppler US to identify abnormal flow (thrombosis, tumor encasement) or abnormal vascularity(tumor vascularity)
o Use as real time imaging guide for interventional procedures
• Disadvantages of USo Pancreas is retroperitoneal structure and considered "deep" intra abdominal organ for imaging with transabdominal ultrasound
o Limited US beam penetration in obese patient with thick subcutaneous and omental fat
o Often entire pancreatic parenchyma cannot be completely examined due to overlying bowel gas
o Operator-dependent imaging technique
Technical consideration in transabdominal US
o Examination should begin in transverse plane in midline below xiphisternum, using vascular landmarks to identify pancreas
• Longitudinal view for further evaluation particularly if lesion is detected
o Pancreatic body can usually be better delineated by transducer pressure to displace overlying bowel gaso If there is abundant bowel gas obscuring pancreatic parenchyma
• Scanning with patient in various positions including erect, sitting, both obliques and decubitus may help
• Ask patient to drink plenty of water to distend the stomach which acts as an acoustic window

Technical consideration in transabdominal US
o Using left kidney/spleen as acoustic window,
pancreatic tail can be visualized in left coronal view
o Head can be better assessed through right
lateral/decubitus approach in a coronal plane
o Place area of interest within the focal zone of
transducer
o Always examine the rest of the abdomen in detail
o Doppler US to aid assessment of patency and flow characteristics of vessels
• Special US techniques such as endoscopic US(EUS) or intra-operative US (IOU) are useful in detecting small pancreatic tumors (e.g., islet cell tumor) which are not apparent on transabdominal US, CT or MR
• Cross-sectional imaging techniques including CT and MR are usually required for further characterization of pancreatic lesion detected on US
• Advantages of CTo Fast scanning in era of multi-detector CT, thus more practical in critically ill patientso Shows calcifications better than other imaging modalitieso Less prQne to technical and interpretative errors
• Advantages of MRo No ionizing radiation is involvedo Does not require iodinated contrast agento Multiplanar capabilityo Allows easy evaluation of common bile duct and pancreatic duct using MRCP sequences
PATHOLOGY-BASED IMAGING ISSUES
• Two main categories to differentiate on imaging
include neoplasm (most commonly ductal pancreatic
carcinoma) and pancreatitis
o Ductal pancreatic carcinomas typically cause narrowing or obstruction of vessels and ducts, and extend dorsally to coeliac axis and SMA origins
o Acute pancreatitis causes fluid exudation and fat
infiltration, extends ventrally and laterally to mesentery and anterior pararenal space, less common cause for ductal obstruction
Differential diagnoses of cystic pancreatic mass
o Common• Pseudocyst• Mucinous cystic tumor• Serous cystadenoma• Necrotic pancreatic ductal carcinoma• Intraductal papillary mucinous tumor (IPMT)
o Uncommon• Simple/congenital cyst (e.g., Von Hippel Lindau syndrome, adult polycystic kidney disease)• Solid and papillary neoplasm of pancreas• Lymphangioma• Cystic metastases/lymphoma
Conditions to consider if dilated pancreatic duct is seen
o Chronic pancreatitis: Parenchymal or intraductal
calcification, atrophic pancreas
o Pancreatic ductal carcinoma: Common bile and
pancreatic ductal dilatation for most common
lesions in pancreatic head
o Periampullary tumor
o IPMT
o Obstructing distal common bile duct (CBD) stone
Embryologic Events• Embryologically, pancreas is developed from dorsal and ventral pancreatic budso Body-tail segment developed from dorsal pancreatic budo Head-uncinate segment developed from ventral pancreatic bud• During normal development, ventral bud migrates dorsally around fetal duodenum to merge with dorsal bud to form pancreatic substance and branching pancreatic and bile ducts
Practical Implications• Failure or anomalies of rotation or fusion may result in congenital lesions such as annular pancreas, pancreas divisum, agenesis of dorsal pancreas• Ventral (head-uncinate) and dorsal (body-tail) segments may have different echotexture that may be misinterpreted as pathology• Pancreatic ductal obstruction of either dorsal or ventral buds may lead to dilatation of involved portion with sparing of uninvolved segments
Clinical Importance
• Ductal pancreatic carcinoma: Usually presents late with poor overall prognosis, surgically not operable in most cases
• Serous cystadenoma: No malignant potential, microcystic/macrocystic in appearances
• Mucinous cystic pancreatic tumor: Regarded as pre-malignant lesion, predominantly cystic with septations +/- solid component
• Islet cell tumor: Hypervascular primary tumor and liver metastases, most commono Insulinoma, functional tumors small at presentationo Non-functional tumors large at diagnosis
• Solid and papillary neoplasm, metastases, lymphoma; rare lesions
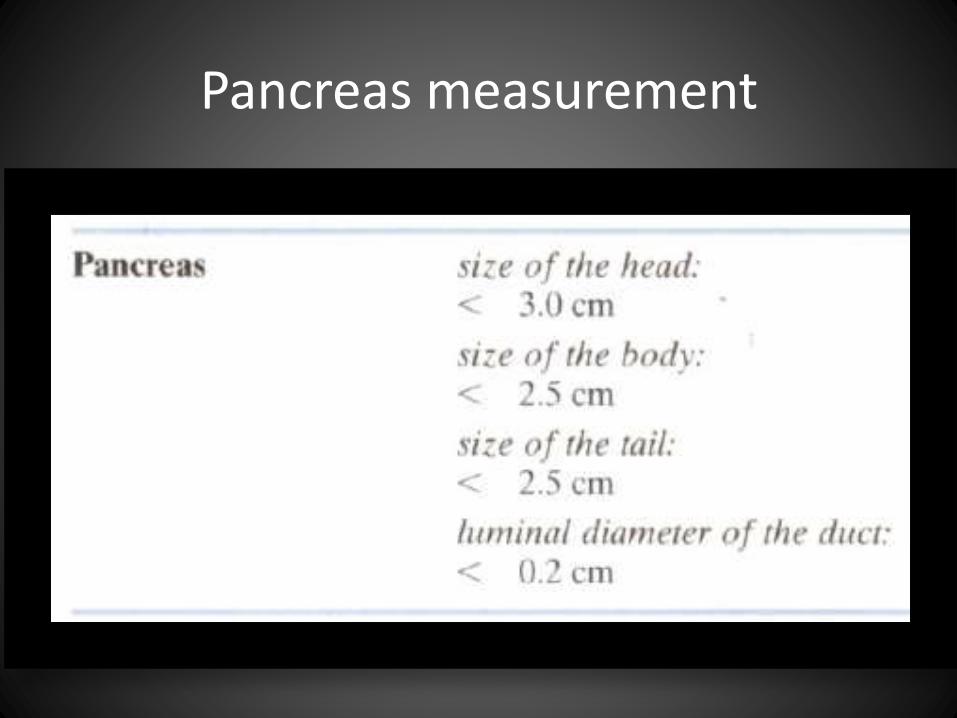
Pancreas measurement
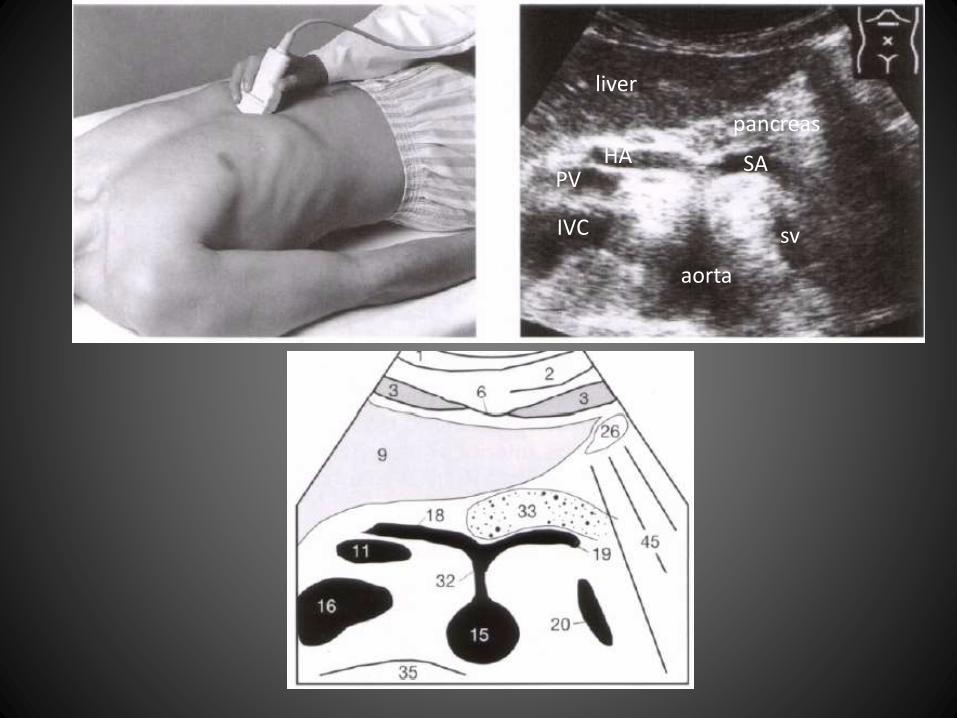
liver
aorta
HA SA
IVC
pancreas
sv
PV
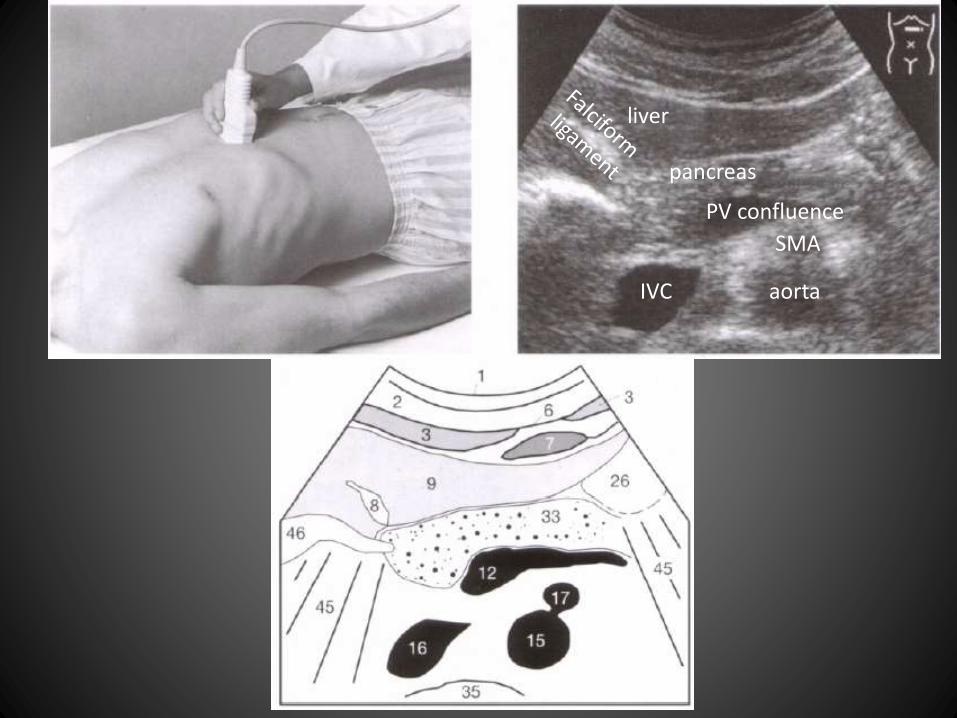
liver
pancreas
PV confluence
aorta
SMA
IVC
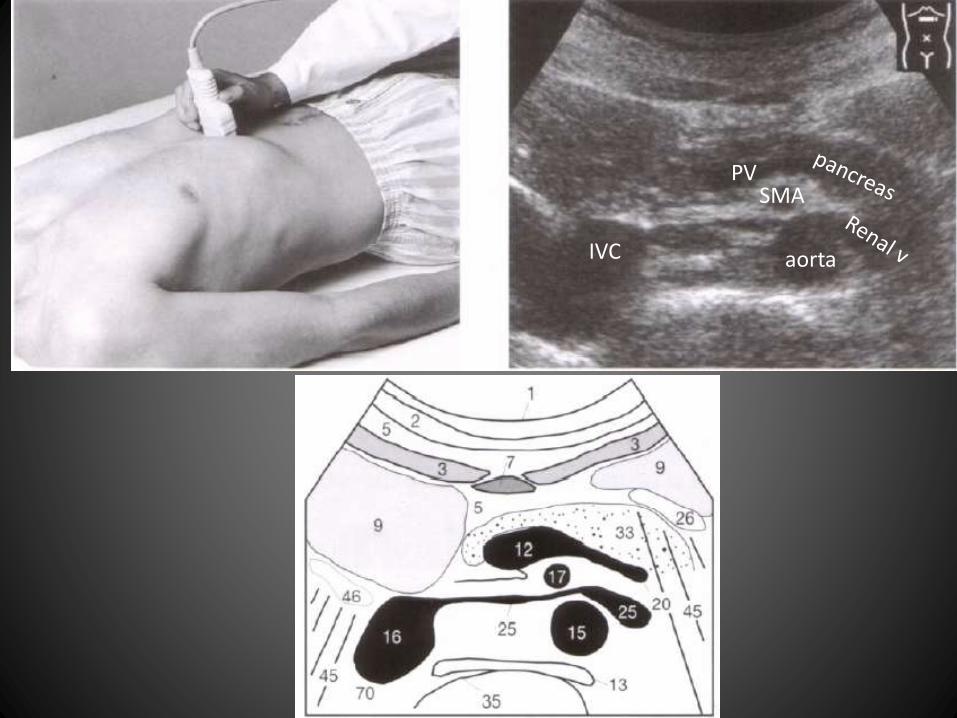
PVSMA
aortaIVC
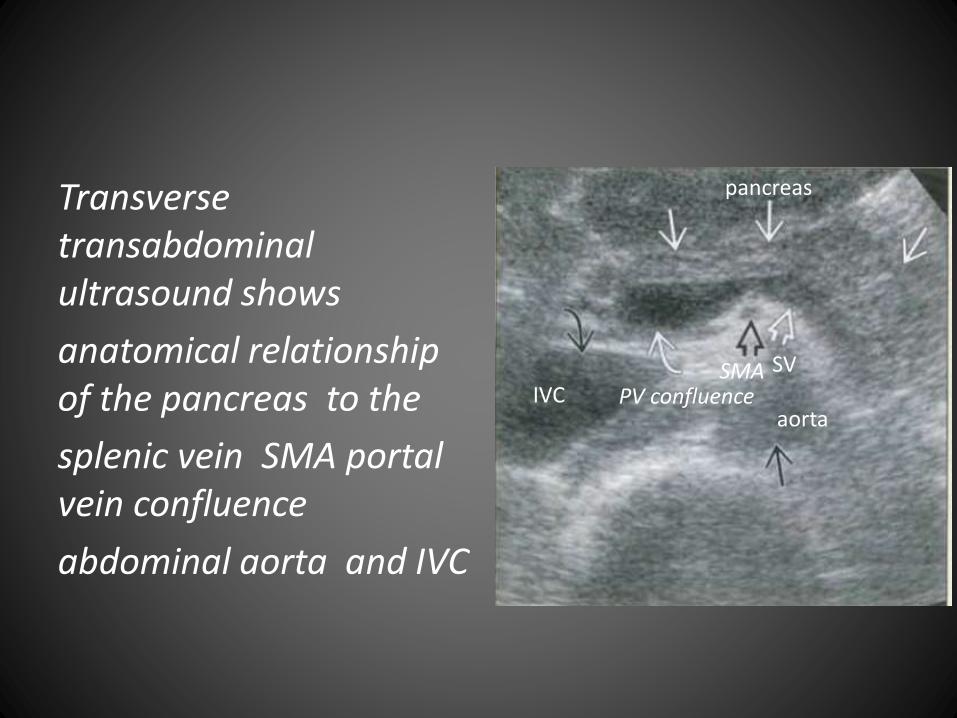
Transverse transabdominalultrasound shows
anatomical relationship of the pancreas to the
splenic vein SMA portal vein confluence
abdominal aorta and IVC
pancreas
SVSMAPV confluence
aortaIVC
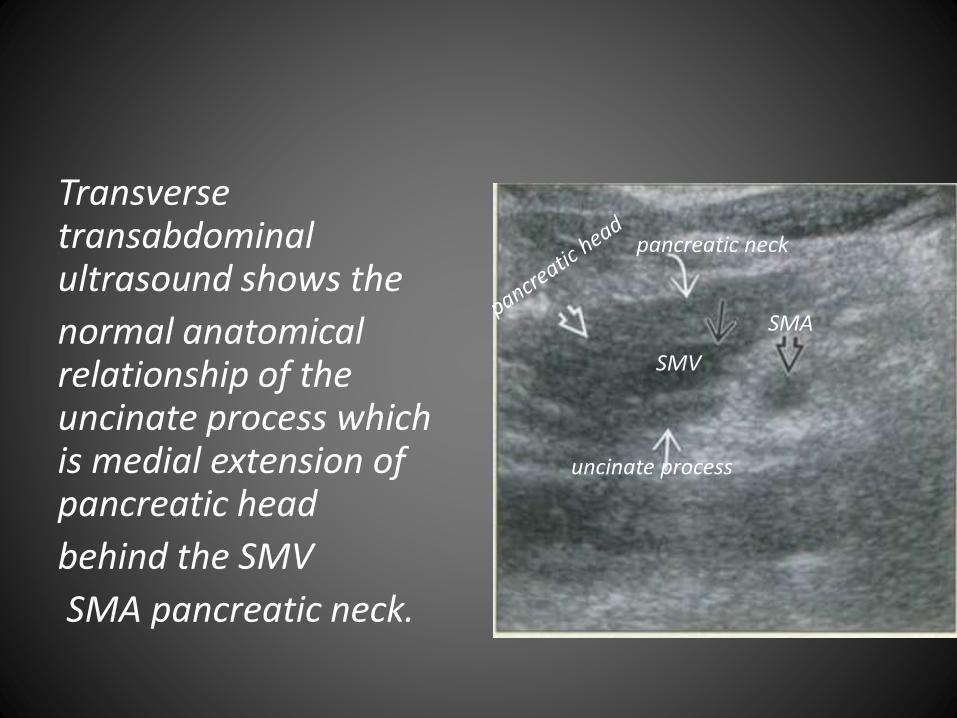
Transverse transabdominalultrasound shows the
normal anatomical relationship of the uncinate process which is medial extension of pancreatic head
behind the SMV
SMA pancreatic neck.
uncinate process
SMV
SMA
pancreatic neck
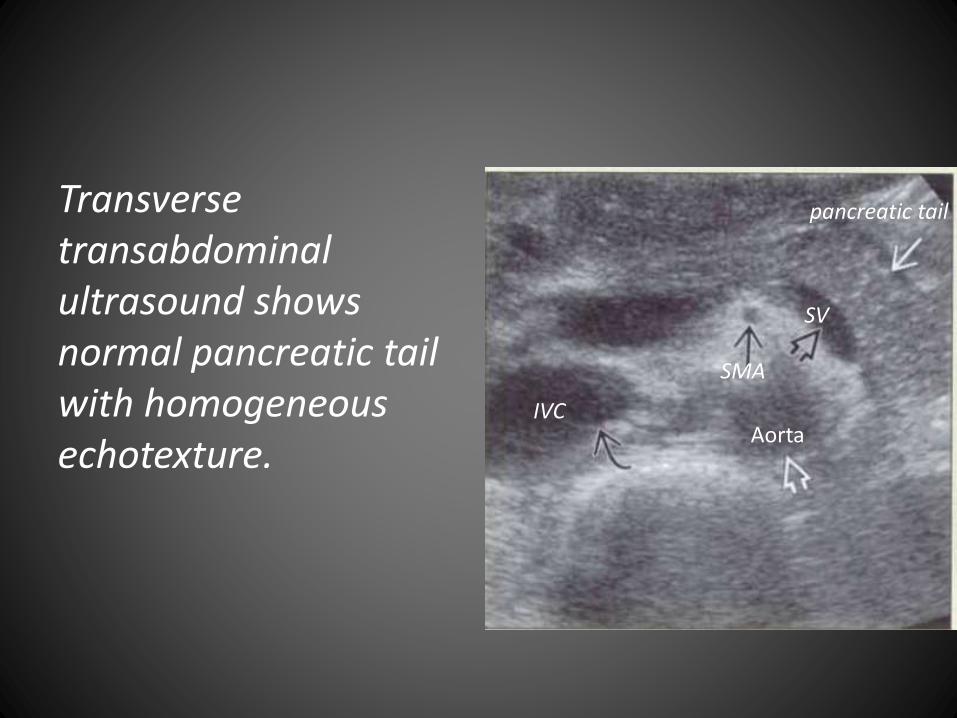
Transverse transabdominalultrasound shows normal pancreatic tail with homogeneous echotexture.
pancreatic tail
SV
SMA
IVCAorta
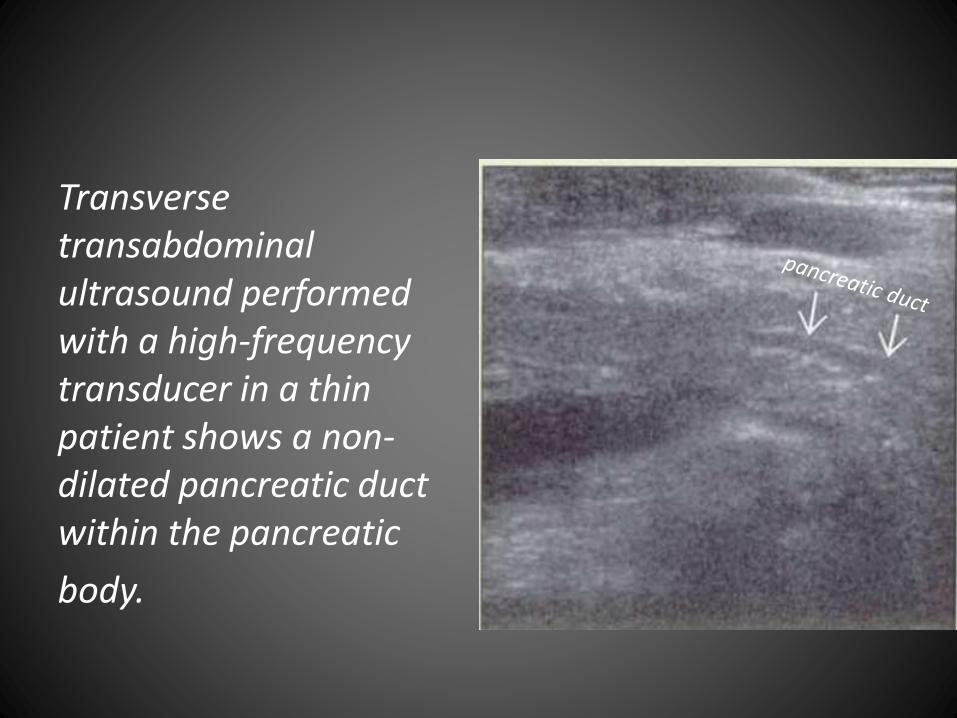
Transverse transabdominalultrasound performed with a high-frequency transducer in a thin patient shows a non-dilated pancreatic duct within the pancreatic
body.
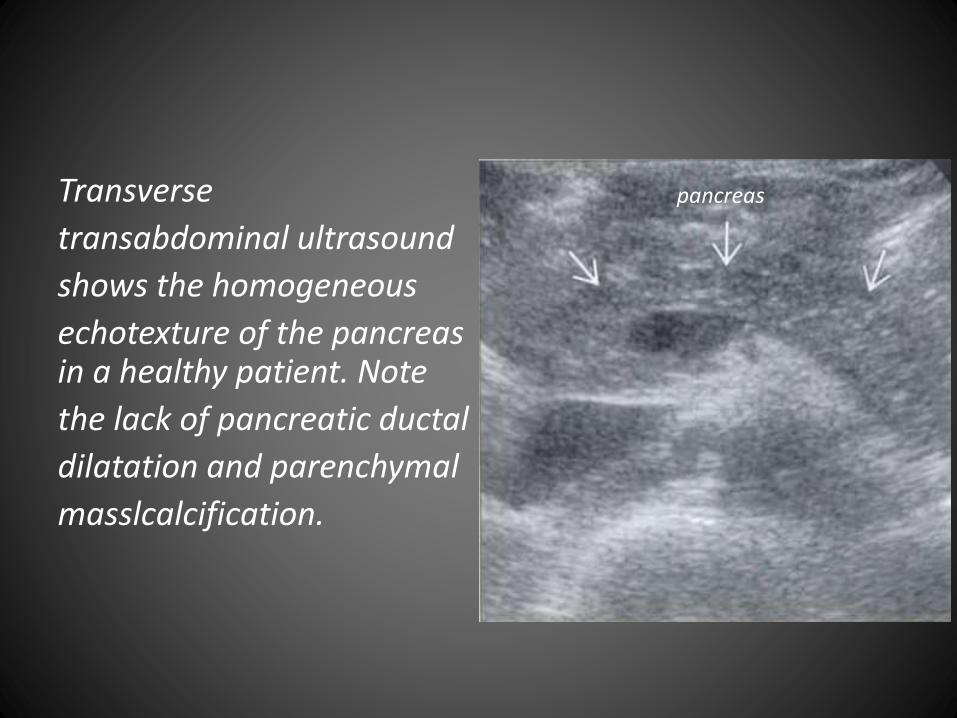
Transverse
transabdominal ultrasound
shows the homogeneous
echotexture of the pancreas in a healthy patient. Note
the lack of pancreatic ductal
dilatation and parenchymal
masslcalcification.
pancreas
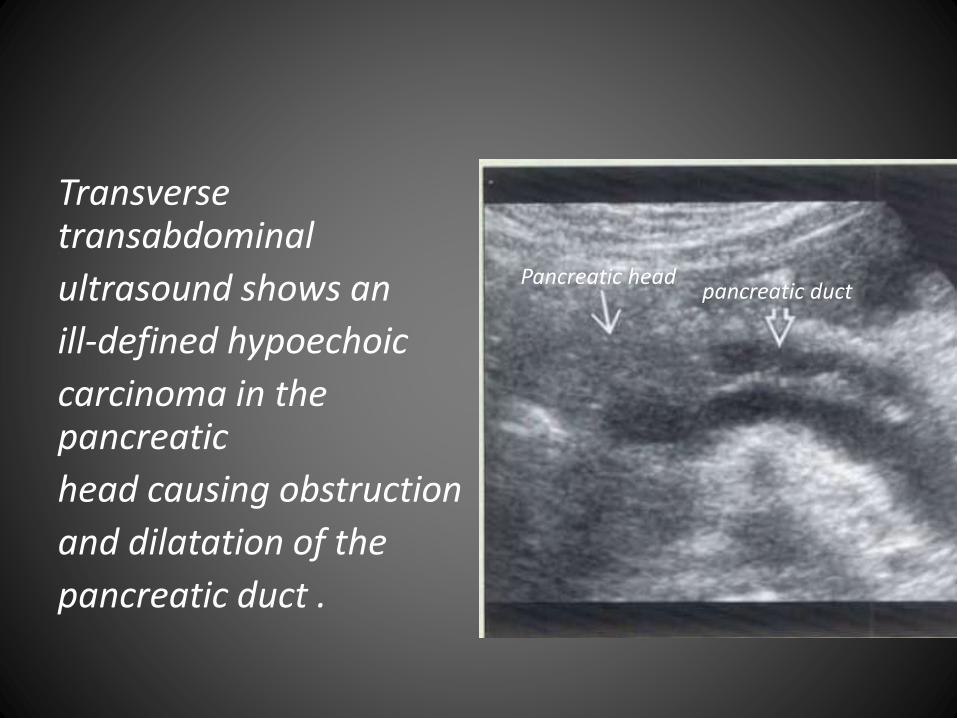
Transverse transabdominal
ultrasound shows an
ill-defined hypoechoic
carcinoma in the pancreatic
head causing obstruction
and dilatation of the
pancreatic duct .
Pancreatic headpancreatic duct
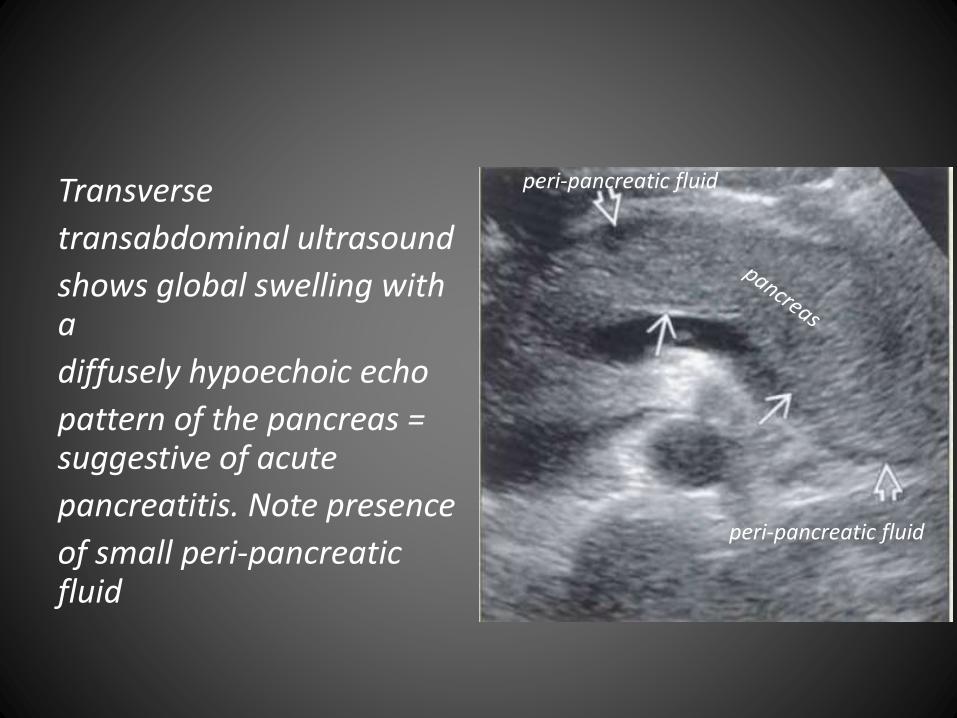
Transverse
transabdominal ultrasound
shows global swelling with a
diffusely hypoechoic echo
pattern of the pancreas = suggestive of acute
pancreatitis. Note presence
of small peri-pancreatic fluid
peri-pancreatic fluid
peri-pancreatic fluid
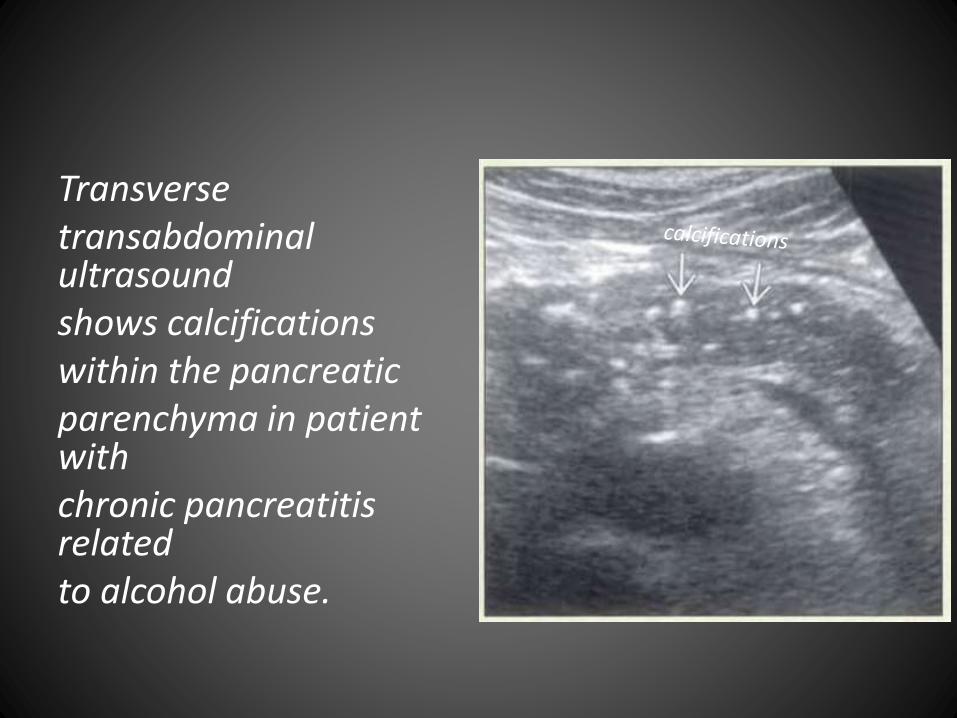
Transversetransabdominalultrasoundshows calcifications within the pancreaticparenchyma in patient withchronic pancreatitis relatedto alcohol abuse.
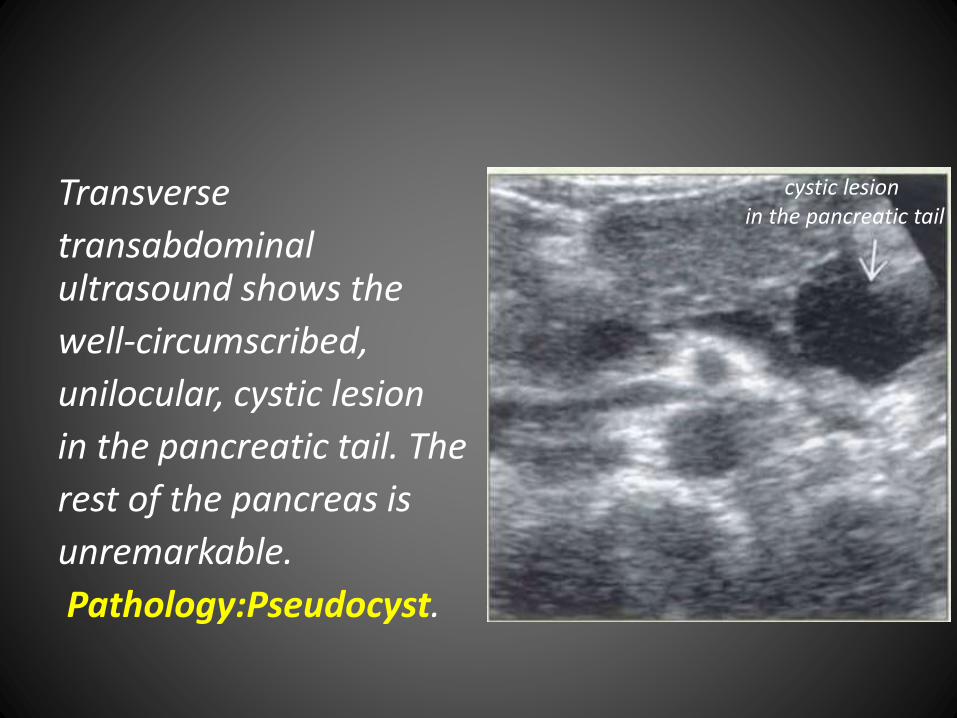
Transverse
transabdominalultrasound shows the
well-circumscribed,
unilocular, cystic lesion
in the pancreatic tail. The
rest of the pancreas is
unremarkable.
Pathology:Pseudocyst.
cystic lesion in the pancreatic tail
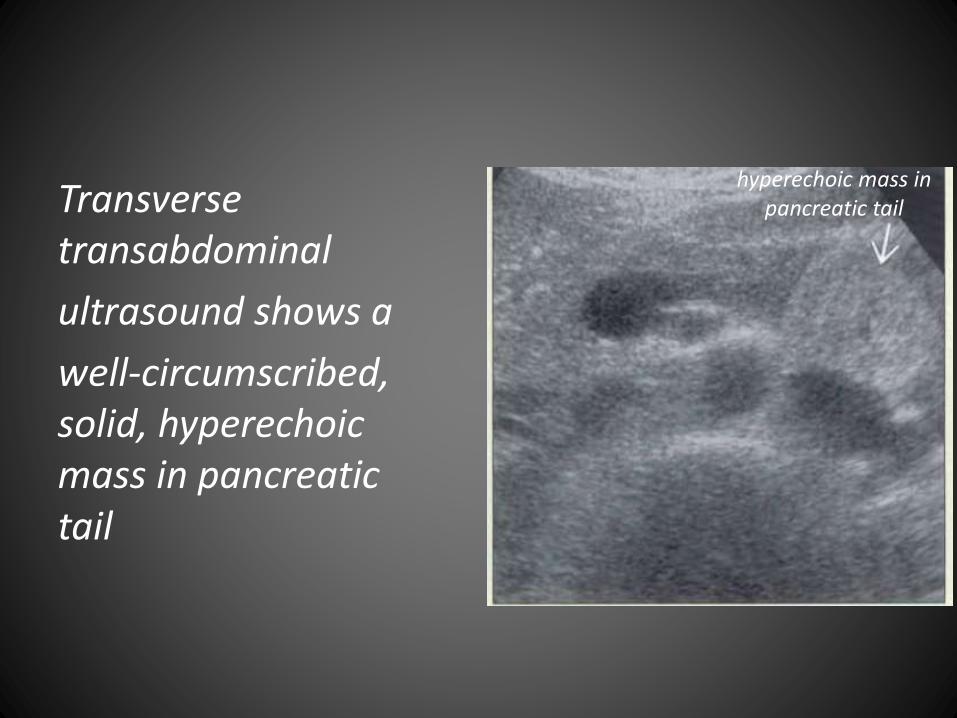
Transverse transabdominal
ultrasound shows a
well-circumscribed, solid, hyperechoicmass in pancreatic tail
hyperechoic mass inpancreatic tail
Top Related