







Languages
Pages
Legal


Pain Management ConsiderationsPain Management Considerationsfor Chemical Dependency Patientsfor Chemical Dependency Patients
Bill Dickinson, D.O., FASAM, FAAFPBill Dickinson, D.O., FASAM, FAAFP

ObjectivesObjectives
•• Discuss the risks of using opiate/opioid Discuss the risks of using opiate/opioid medications in these patientsmedications in these patients
•• Review options for pain control for these Review options for pain control for these patientspatients


Pain Specialist ViewPain Specialist View
•• Focus on providing adequate pain reliefFocus on providing adequate pain relief•• Allay patient concerns about addictionAllay patient concerns about addiction•• Addiction from medical care is rareAddiction from medical care is rare•• Under treatment of pain is more commonUnder treatment of pain is more common
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pg1483, Pain and Addiction, pg1483

Addiction Medicine ViewAddiction Medicine View
•• See failed pain management and addictionSee failed pain management and addiction•• See consequences of increased opioid See consequences of increased opioid
availability, both licit and illicitavailability, both licit and illicit•• Aware of pain patients selling medicationAware of pain patients selling medication•• Rarely see increased opioid use increasing Rarely see increased opioid use increasing
quality of lifequality of life
The American storyThe American story
•• 2.3 million Americans reported using heroin 2.3 million Americans reported using heroin ≥≥once (1998)once (1998)
•• 149,000 new users (1999) 149,000 new users (1999) –– 980,000 persons using at least weekly 980,000 persons using at least weekly
(1998)(1998)•• 810,000810,000––1 million chronic users of heroin1 million chronic users of heroin•• Only 170,000Only 170,000––200,000 receiving treatment200,000 receiving treatment
(National Household Survey on Drug Abuse, 1999; Office of National Drug Control Policy, 1997; SAMHSA, Office of Applied Studies, National
Household Survey on Drug Abuse, 2000 and 2001)


Addiction to prescription opioidsAddiction to prescription opioids
•• Prescription opioid drug abuse and misuse Prescription opioid drug abuse and misuse (eg, oxycodone, hydrocodone)(eg, oxycodone, hydrocodone)
•• Estimated to be 3 million Estimated to be 3 million (DAWN 2002)(DAWN 2002)
–– 1.9 million persons aged 1.9 million persons aged ≥≥12 had used 12 had used OxyContin nonOxyContin non--medically at least once in medically at least once in their lifetimetheir lifetime
–– (2002 National Survey on Drug Use and Health (NSDUH))(2002 National Survey on Drug Use and Health (NSDUH))

Abuse of prescription opioids: a Abuse of prescription opioids: a growing problemgrowing problem
Non-medical OxyContin use – 2002
Prescription drug monitoring: American Society of Interventional Pain Physicians, 2002
0200000400000600000800000100000012000001400000160000018000002000000
1997 2000 2001 2002

““Between 1999 and 2002Between 1999 and 2002…….opioid analgesic .opioid analgesic poisonings increased by 91.2%poisonings increased by 91.2%””Paulozzi et al; Pharmacoepidemiology and Drug Safety 2006; 15: 6Paulozzi et al; Pharmacoepidemiology and Drug Safety 2006; 15: 61818--627627

Unintentional OD: 2Unintentional OD: 2ndnd Leading Leading Cause of Accidental Death!Cause of Accidental Death!
CDC: 2007 ATLANTA CDC: 2007 ATLANTA -- Unintentional fatal drug Unintentional fatal drug overdoses in the United States nearly doubled from overdoses in the United States nearly doubled from 1999 to 20041999 to 2004

““Deaths from overdoses on methadone rose 390 Deaths from overdoses on methadone rose 390 percent between 1999 and 2004 and the rise is percent between 1999 and 2004 and the rise is continuingcontinuing””
Methadone Diversion, Abuse, Misuse National Drug Intelligence Methadone Diversion, Abuse, Misuse National Drug Intelligence Center 11/2007Center 11/2007

Key Informant Network, Dr. CiceroKey Informant Network, Dr. CiceroCoverage AreaCoverage Area

Conclusions Conclusions
Prescription drug abuse is Prescription drug abuse is widespread with 2/3 of widespread with 2/3 of
informants reporting abuse.informants reporting abuse.OxyContin and Hydrocodone abuse OxyContin and Hydrocodone abuse
are also the most prevalent are also the most prevalent drugs of abuse being observed in drugs of abuse being observed in
5050--60% of all ZIP codes.60% of all ZIP codes.Status of Key Informant Network, Theodore J. Cicero, PhD, 2005Status of Key Informant Network, Theodore J. Cicero, PhD, 2005

In terms of rate of growth, In terms of rate of growth, methadone,buprenorphine and morphine methadone,buprenorphine and morphine
are increasing at the greatest pace.are increasing at the greatest pace.It is rare for abuse of one drug to occur It is rare for abuse of one drug to occur
alone in any zip code; rather, the alone in any zip code; rather, the pattern is polypattern is poly--substance abuse.substance abuse.
Key Informant Network, T. Cicero, PhD, 2005Key Informant Network, T. Cicero, PhD, 2005
ConclusionsConclusions
ConclusionsConclusions
Approximately 87% of OxyContin and other Approximately 87% of OxyContin and other prescription drug abusers had past histories prescription drug abusers had past histories
of alcohol or opiate abuse, whereas the of alcohol or opiate abuse, whereas the remaining 13% of the individuals were remaining 13% of the individuals were
reported to have no history of alcohol or reported to have no history of alcohol or opiate abuse, at least to the extent known opiate abuse, at least to the extent known
by the informant.by the informant.Key Informant Network, T. Cicero, PhD, 2005Key Informant Network, T. Cicero, PhD, 2005

LikingLiking
Liking or drug reward is increased Liking or drug reward is increased dopaminergic activity in the mesolimbic dopaminergic activity in the mesolimbic pathway: the ventral tegmental area pathway: the ventral tegmental area (VTA), the nucleus accumbens (NA), and (VTA), the nucleus accumbens (NA), and basal forebrain. Reversible and adaptive.basal forebrain. Reversible and adaptive.
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd , Pain and Addiction, pg1395, Pain and Addiction, pg1395

WantingWanting
Wanting is an effect of dopamine release in the Wanting is an effect of dopamine release in the mesolimbic pathway which heightens and mesolimbic pathway which heightens and strengthens both learning and memory in the strengthens both learning and memory in the brain. Long lasting with permanent brain. Long lasting with permanent reorganization in synaptic connections. Explains reorganization in synaptic connections. Explains persistent use in spite of negative effects.persistent use in spite of negative effects.
Principles of Addiction Med, 3Principles of Addiction Med, 3rdrd, Pain and Addiction, pg 1395, Pain and Addiction, pg 1395

Nucleus Accumbens
Ventral TegmentalArea
PrefrontalCortex
Amygdala
Locus Coeruleus
Periaqueductal GrayArea
Arcuate Nucleus

Changes in the brain of an Changes in the brain of an addicted personaddicted person
•• Neurobiologic changes lead to:Neurobiologic changes lead to:–– Compulsive opioid use Compulsive opioid use
•• To feel or function normalTo feel or function normal•• To avoid painTo avoid pain•• To escape painTo escape pain
–– Loss of control over intakeLoss of control over intake–– Impaired social and occupational Impaired social and occupational
function function

The Natural Reward Mechanism is The Natural Reward Mechanism is ““HijackedHijacked””
Cami, Farre’, Drug Addiction, NEJM 349;10 9/4/2003 975-986

Physical Dependence with OpioidsPhysical Dependence with Opioids
““There existsThere exists…….outside .outside alkaloids and habit, a sense alkaloids and habit, a sense for opium, an intangible for opium, an intangible habit which lives on, despite habit which lives on, despite the recasting of the the recasting of the organism. The dead drug organism. The dead drug leaves a ghost behind. At leaves a ghost behind. At certain hours it haunts the certain hours it haunts the househouse””
--Jean Cocteau 1889Jean Cocteau 1889--19631963






Physical DependencePhysical Dependence
Endogenous Endogenous Endorphin SystemEndorphin SystemMu, Kappa, Delta Mu, Kappa, Delta ReceptorsReceptorsTolerance, Physical Tolerance, Physical Dependence, Dependence, Prolonged Withdrawal Prolonged Withdrawal SyndromeSyndrome
Endocrine basis?Endocrine basis?


Approach to Acute Pain TreatmentApproach to Acute Pain Treatment
•• Respect the disease of addictionRespect the disease of addiction•• Monitor for withdrawalMonitor for withdrawal•• Provide pain managementProvide pain management•• Document the treatment planDocument the treatment plan•• Monitor and adjustMonitor and adjust•• Taper opioids Taper opioids
Principles of Addiction Med 3Principles of Addiction Med 3rdrd, Pain and Addiction, pg 1408, Pain and Addiction, pg 1408

Respect the Disease of AddictionRespect the Disease of Addiction
•• Openly discuss all concernsOpenly discuss all concerns•• Involve the patient in decisionsInvolve the patient in decisions•• Facilitate, support the recovery processFacilitate, support the recovery process•• Educate staff and family about pain and Educate staff and family about pain and
addictive disordersaddictive disorders

Potential for WithdrawalPotential for Withdrawal
•• If the patient is dependent on If the patient is dependent on opiates/opioids, then a baseline opiates/opioids, then a baseline replacement is used.replacement is used.
•• 72 hour rule72 hour rule•• Possible withdrawal from other substancesPossible withdrawal from other substances

Effective Pain ManagementEffective Pain Management
•• Consider nonConsider non--opioid treatmentopioid treatment•• Establish effective doseEstablish effective dose•• Avoid older agonistAvoid older agonist--antagonist opioidsantagonist opioids•• Use less rewarding opioids: slow release, Use less rewarding opioids: slow release,
PCA, continuous infusion (Less liking)PCA, continuous infusion (Less liking)

Monitor and AdjustMonitor and Adjust
•• Pain intensityPain intensity•• Ability to adhere to all other Ability to adhere to all other
medical/surgical treatmentmedical/surgical treatment•• ADLADL’’s s

TaperTaper
•• Opioids for painOpioids for pain•• Consider what is the usual course of pain Consider what is the usual course of pain
and opioid use in nonand opioid use in non--dependent patientsdependent patients•• Discuss treatment optionsDiscuss treatment options

Treatment PlanTreatment Plan
•• Pain controlPain control•• Interaction with other providersInteraction with other providers•• Recommendations and referrals for Recommendations and referrals for
treatmenttreatment

Universal Precautions in Pain MedicineUniversal Precautions in Pain Medicine
1.1. Make diagnosis Make diagnosis appropriate differentialappropriate differential
2.2. Psychosocial Psychosocial assessment with risk of assessment with risk of addictive disordersaddictive disorders
3.3. Informed consentInformed consent4.4. Treatment agreementTreatment agreement5.5. Pre or post intervention Pre or post intervention
assessment of pain level assessment of pain level and functionand function
6.6. Appropriate trial of opioid Appropriate trial of opioid therapy with or without therapy with or without adjunctive medicationadjunctive medication
7.7. Reassessment of pain Reassessment of pain scores and level of functionscores and level of function
8.8. Regularly assess the Regularly assess the ““4 A4 A’’ss””of pain medicineof pain medicine
9.9. Periodically review pain Periodically review pain diagnosis and comorbid diagnosis and comorbid conditions, including conditions, including addictive disordersaddictive disorders
10.10.DocumentationDocumentationGourlay, D, Heit, H. Pain Med. 2005;6:107-112

4 A4 A’’s of Treatment Outcomess of Treatment Outcomes1.1. Analgesia (level of pain relief)Analgesia (level of pain relief)2.2. Activities (psychological Activities (psychological
functioning/quality of life)functioning/quality of life)3.3. Adverse Effects (side effects)Adverse Effects (side effects)4.4. Aberrant drug taking behavior (Addiction)Aberrant drug taking behavior (Addiction)
Passik, SD, Weinreb, HJ. Adv Ther. 2000;17:70-83

Principles of PrescribingPrinciples of Prescribing
•• Single prescriber, single pharmacySingle prescriber, single pharmacy•• Patient and Prescriber sign agreementPatient and Prescriber sign agreement•• Use lowest effective doseUse lowest effective dose•• Caution on conditions that may potentiate Caution on conditions that may potentiate
adverse opioid effects: COPD, CHF, sleep apnea, adverse opioid effects: COPD, CHF, sleep apnea, elderly, hepatic and renal impairedelderly, hepatic and renal impaired
•• Assess function, monitor for misuse, random Assess function, monitor for misuse, random urine drug screensurine drug screens
Interagency Guideline on Opioid Dosing for CNCP, WA State AgencyInteragency Guideline on Opioid Dosing for CNCP, WA State Agency Med DirectorMed Director’’s Group, 03/2007s Group, 03/2007

Before the First PrescriptionBefore the First Prescription•• Is your paperwork in order?Is your paperwork in order?
–– Agreements signed?Agreements signed?–– One pharmacy selected / one prescriber One pharmacy selected / one prescriber
agreed upon?agreed upon?–– UDT sample collected?UDT sample collected?–– If appropriate, current doses confirmed?If appropriate, current doses confirmed?
•• Via pharmacy?Via pharmacy?•• Via past prescriber/prescribers office?Via past prescriber/prescribers office?
4/30/2009 41DL Gourlay MD - Wasser Pain Centre

Chronic Pain SyndromeChronic Pain Syndrome
•• Marked alteration of behavior, depression Marked alteration of behavior, depression and anxietyand anxiety
•• Marked restriction in daily activitiesMarked restriction in daily activities•• Excessive use of medication/medical srvsExcessive use of medication/medical srvs•• No clear relationship to organic disorderNo clear relationship to organic disorder•• History of multiple nonproductive tests, History of multiple nonproductive tests,
treatments, surgeriestreatments, surgeries

Approach to Chronic Pain: Approach to Chronic Pain: GoalsGoals
•• The reduction of painThe reduction of pain•• Improved painImproved pain--associated symptoms: associated symptoms:
sleep problems, depression/anxiety, sleep problems, depression/anxiety, physical functionphysical function
•• Decrease dependence on medicationDecrease dependence on medication
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, page 1413, Pain and Addiction, page 1413

Approach to Chronic PainApproach to Chronic Pain
•• Physical modalitiesPhysical modalities•• CognitiveCognitive--behavioral interventionsbehavioral interventions•• Invasive (interventionalist) treatmentsInvasive (interventionalist) treatments•• Medications, both nonMedications, both non--opioid and opioidopioid and opioid

Multidisciplinary Pain RehabilitationMultidisciplinary Pain Rehabilitation•• Education (for patient, family, support)Education (for patient, family, support)•• Reconditioning physical therapyReconditioning physical therapy•• MedicationMedication•• Nerve blocks, TensNerve blocks, Tens•• Biofeedback/relaxationBiofeedback/relaxation•• Psychotherapy (patient and family)Psychotherapy (patient and family)•• Treat psychiatric comorbidityTreat psychiatric comorbidity•• Chemical dependency treatmentChemical dependency treatment
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pg 1433, Pain and Addiction, pg 1433


Periodic ReviewPeriodic Review•• Urine drug testingUrine drug testing•• AnalgesiaAnalgesia•• Activities of Daily Living (ADLActivities of Daily Living (ADL’’s)s)•• Adverse effectsAdverse effects•• Aberrant BehaviorAberrant Behavior•• Patient affectPatient affect
Balancing Clinical and Risk Management for Chronic Pain Pts on OBalancing Clinical and Risk Management for Chronic Pain Pts on Opioids, AAFP CME Monographpioids, AAFP CME Monograph

Behavioral Predictors of MisuseBehavioral Predictors of Misuse
•• Illegal/Criminal: Forgery, theft, diversionIllegal/Criminal: Forgery, theft, diversion•• Dangerous: Aggressive/threatening, Dangerous: Aggressive/threatening,
overdoses, accidents(MVA) by intoxicationoverdoses, accidents(MVA) by intoxication•• Aberrant: Drug hoarding, request specific Aberrant: Drug hoarding, request specific
Rx, other sources, noncompliance, reports Rx, other sources, noncompliance, reports unintended mind/mood effects, resists unintended mind/mood effects, resists change, misses appts, not following change, misses appts, not following treatment plantreatment plan

Behavioral Predictors of MisuseBehavioral Predictors of Misuse
•• Use of medication in unapproved fashionUse of medication in unapproved fashion•• Uses other sources to obtain medication: Uses other sources to obtain medication:
Physicians, ED, illicitPhysicians, ED, illicit•• Use of other abused substancesUse of other abused substances•• Repeated requests for dose increases and/or Repeated requests for dose increases and/or
early refillsearly refills•• Work, family social deteriorationWork, family social deterioration•• Positive urine drug screen(s)Positive urine drug screen(s)
Balancing Clinical and Risk Management of Chronic Pain Pts on OpBalancing Clinical and Risk Management of Chronic Pain Pts on Opioids, AAFP CME Monographioids, AAFP CME Monograph

Brooner et al, Archives of General Psychiatry 1997Brooner et al, Archives of General Psychiatry 1997
Co-morbid substance disorder
Lifetime percentage
Current percentage
Cocaine dependence 65 40 Cocaine abuse 12 3 Cannabis abuse 15 2 Alcohol dependence 50 25 Alcohol abuse 13 2 Sedative-hypnotic abuse 13 2
How likely is my patient to have How likely is my patient to have another substance use disorder?another substance use disorder?
N=716

Prescribing ConcernsPrescribing Concerns
•• Federal LawFederal Law•• State LawState Law•• State Medical BoardsState Medical Boards•• Fear of Producing AddictionFear of Producing Addiction•• Fear of scrutinyFear of scrutiny•• Uncomfortable with addictsUncomfortable with addicts
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pgs 1466, 1479, Pain and Addiction, pgs 1466, 1479

Yellow Flags (exercise caution)Yellow Flags (exercise caution)
•• Multiple, unsanctioned dose increasesMultiple, unsanctioned dose increases•• Repeated lost or stolen medicationRepeated lost or stolen medication•• Early refillsEarly refills•• Double doctoringDouble doctoring•• UDT negative for prescribed medicationsUDT negative for prescribed medications
4/30/2009 54DL Gourlay MD - Wasser Pain Centre

Red Flags (stop prescribing)Red Flags (stop prescribing)
•• Use of illicit drugs i.e. cocaineUse of illicit drugs i.e. cocaine•• Tampering UDT specimenTampering UDT specimen•• Crushing/snorting oral medicationsCrushing/snorting oral medications•• Injecting oral medicationsInjecting oral medications•• Trafficking i.e. selling or giving controlled Trafficking i.e. selling or giving controlled
substances to someone without lawful substances to someone without lawful authorityauthority
4/30/2009 55DL Gourlay MD - Wasser Pain Centre

Sample Termination AgreementSample Termination Agreement
4/30/2009 56DL Gourlay MD - Wasser Pain Centre


Controlled Substances Act, 1970Controlled Substances Act, 1970
•• Federal lawFederal law•• Established USA system of drug controlEstablished USA system of drug control•• Reflects both control and availabilityReflects both control and availability•• Parallels international treatiesParallels international treaties•• Rules: Code of Federal Regulations (CFR)Rules: Code of Federal Regulations (CFR)•• DEADEA
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, page 1466, Pain and Addiction, page 1466

State Medical Board GuidelinesState Medical Board Guidelines
•• Evaluate each patient for addiction historyEvaluate each patient for addiction history•• Addiction medicine consultationAddiction medicine consultation•• Specialty consultationSpecialty consultation•• Extra care and attentionExtra care and attention•• Treatment plan includes misuse possibilityTreatment plan includes misuse possibility•• Vigilant to drug seeking behaviorsVigilant to drug seeking behaviors
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pg 1470, Pain and Addiction, pg 1470

Federation of State Medical BoardsFederation of State Medical Boards
•• 1998: Model Guidelines for the Use of 1998: Model Guidelines for the Use of Controlled Substances for the Treatment of PainControlled Substances for the Treatment of Pain
•• Cooperative effort: FSMB, the American Pain Cooperative effort: FSMB, the American Pain Society, the American Academy of Pain Society, the American Academy of Pain Medicine, the American Society of Law, Medicine, the American Society of Law, Medicine, and EthicsMedicine, and Ethics
•• No exclusion of addicts from pain controlNo exclusion of addicts from pain controlPrinciples of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pg 1471, Pain and Addiction, pg 1471

Guidelines for Rx with Abuse PotentialGuidelines for Rx with Abuse Potential
•• Clear rules and contractClear rules and contract•• Rx sufficient medication, titrate as neededRx sufficient medication, titrate as needed•• Adjunct medications and therapiesAdjunct medications and therapies•• One pharmacy, no lost or stolen RxOne pharmacy, no lost or stolen Rx•• Clean/sober monitoring by family/friendClean/sober monitoring by family/friend•• See patient more frequently if neededSee patient more frequently if needed•• Brings Rx to visit, random UABrings Rx to visit, random UA’’ss•• Document plan, changes, thoughts wellDocument plan, changes, thoughts well
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pg 1477, Pain and Addiction, pg 1477

Physicians and Rx Drug AbusePhysicians and Rx Drug AbuseThe 4 DThe 4 D’’ss
•• Dated: Not aware of current standardsDated: Not aware of current standards•• Duped: Easily manipulated by addictsDuped: Easily manipulated by addicts•• Disabled: Judgment impaired by their Disabled: Judgment impaired by their
illness or their own alcohol/drug problemillness or their own alcohol/drug problem•• Dishonest: Script doctorsDishonest: Script doctors
David Smith, MD (1980)David Smith, MD (1980)Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pgs 1489, Pain and Addiction, pgs 1489--14901490

PseudoaddictionPseudoaddiction
•• Drug seeking behaviors iatrogenically Drug seeking behaviors iatrogenically induced through inadequate tx of paininduced through inadequate tx of pain
•• Driven by patients need for pain reliefDriven by patients need for pain relief•• Patient escalates demands for pain reliefPatient escalates demands for pain relief•• Behavioral changes to show pain severityBehavioral changes to show pain severity•• Crisis of mistrust between patient and Dr.Crisis of mistrust between patient and Dr.•• Believe patientBelieve patient’’s pain report as valids pain report as valid
Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd, Pain and Addiction, pg1485, Pain and Addiction, pg1485

MethadoneMethadone
•• Long acting, 24Long acting, 24--36 hr 36 hr ½½ lifelife•• Accumulates because of the long Accumulates because of the long ½½ lifelife•• Good base for short term pain controlGood base for short term pain control•• Used in Opiate Substitution Therapy (OST) Used in Opiate Substitution Therapy (OST)
and in Chronic Pain programsand in Chronic Pain programs•• Sedative and other opioid interactionSedative and other opioid interaction

BuprenorphineBuprenorphine
Schedule III partial opioid agonistSchedule III partial opioid agonist(Agonist (Agonist –– Antagonist)Antagonist)

History of BuprenorphineHistory of Buprenorphine
•• 19801980’’ss……......Use in Europe......Use in Europe•• 19921992………………...US...US––11stst injectable, later injectable, later
research research •• Oct. 2000Oct. 2000…….Drug Abuse Treatment Act.Drug Abuse Treatment Act•• Oct. 2002Oct. 2002…….DEA releases.DEA releases•• Jan. 2003Jan. 2003…….Available by Rx, DEA waiver.Available by Rx, DEA waiver

What is buprenorphine?What is buprenorphine?
•• PartialPartial µµ--opioid agonistopioid agonist•• High receptor affinity and receptor occupancyHigh receptor affinity and receptor occupancy::
–– 95% oc95% occcupupancyancy at 16 mg at 16 mg (Greenwald et al, 2003)(Greenwald et al, 2003)
–– Blockade or attenuated effect of the use of additional Blockade or attenuated effect of the use of additional opioidsopioids
•• Lower intrinsic activity than full agonistsLower intrinsic activity than full agonists::–– Favorable safety profile due to Favorable safety profile due to ““ceilingceiling”” effecteffect–– Lower street value Lower street value –– Lower abuse potentialLower abuse potential
(Walsh and Eissenberg, 2003)(Walsh and Eissenberg, 2003)
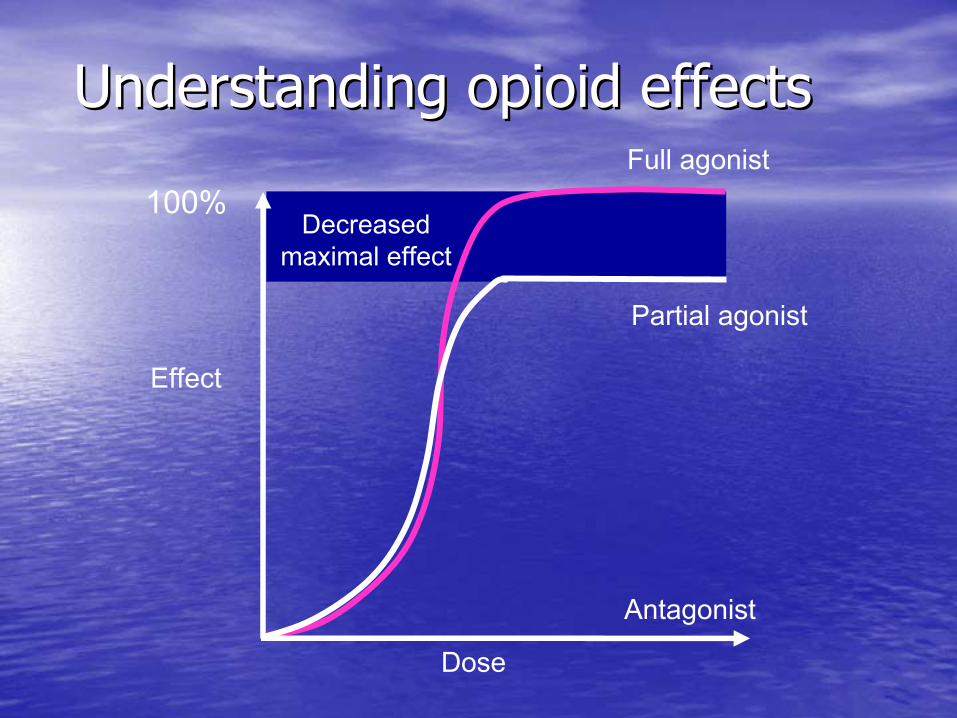
Effect
Dose
Partial agonist
Full agonist
Antagonist
100%
Understanding opioid effectsUnderstanding opioid effects
Decreased maximal effect

Agonist vs. AntagonistAgonist vs. Antagonist
•• AgonistAgonist AntagonistAntagonist
Stop cravingsStop cravings Cause withdrawalCause withdrawalStop withdrawalStop withdrawal Little or no effect fromLittle or no effect fromControl painControl pain other opiates/opioidsother opiates/opioidsNo euphoriaNo euphoria

PharmacologPharmacologic benefitsic benefits
•• Slow Slow receptor receptor dissociationdissociation::–– Longer duration of action Longer duration of action –– MMilder withdrawalilder withdrawal
•• Lower physical dependence liability than full Lower physical dependence liability than full agonistsagonists
•• Limited development of toleranceLimited development of tolerance
•• Ceiling effect on respiratory depressionCeiling effect on respiratory depression–– Increased safety against overdoseIncreased safety against overdose
Buprenorphine: Buprenorphine: Pharmacological AdvantagesPharmacological Advantages
Partial AgonistPartial Agonist•• high safety profile/ceiling effecthigh safety profile/ceiling effect•• low dependencelow dependence
Tight Receptor BindingTight Receptor Binding•• long duration of actionlong duration of action•• slow onset slow onset •• mild abstinencemild abstinence

Buprenorphine: a treatment built Buprenorphine: a treatment built on solid foundationson solid foundations
•• Extensively tested in 46 international Extensively tested in 46 international clinical trials:clinical trials:–– 5275 patients from France, Australia, 5275 patients from France, Australia,
England and the USEngland and the US
•• A Cochrane review of 13 studies A Cochrane review of 13 studies concluded concluded ““buprenorphine is an buprenorphine is an effective intervention for the effective intervention for the treatment of opioid dependencetreatment of opioid dependence””

Buprenorphine retains more Buprenorphine retains more patients than methadone in patients than methadone in detoxdetox
30
20
6
0
5
10
15
20
25
30
35
Treatment
% re
tent
ion Buprenorphine 8 mg
Methadone 60 mg
Methadone 20 mg
Johnson et al, 1992
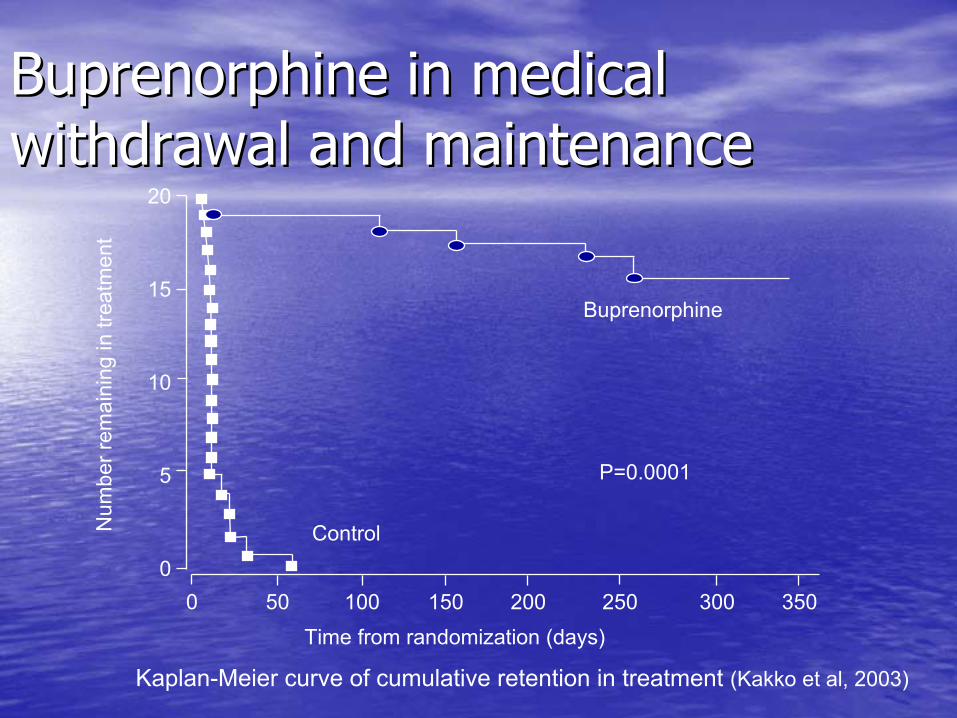
Buprenorphine in medical Buprenorphine in medical withdrawal and maintenancewithdrawal and maintenance
Kaplan-Meier curve of cumulative retention in treatment (Kakko et al, 2003)
Num
ber r
emai
ning
in tr
eatm
ent
Control
Buprenorphine
Time from randomization (days)
P=0.0001
15
20
10
5
00 25020015010050 300 350

Ideal in maintenanceIdeal in maintenance•• Increases retention compared with placeboIncreases retention compared with placebo•• Comparable efficacy to methadone when used Comparable efficacy to methadone when used
in clinically equivalent dosesin clinically equivalent doses•• ““CeilingCeiling”” level of receptor activation increases level of receptor activation increases
safetysafety•• Blocks or attenuates effects of other opioidsBlocks or attenuates effects of other opioids
Reduces concomitant opiReduces concomitant opioidoid useuse
•• NOT A CURE NOT A CURE –– enables participation in a enables participation in a comprehensive program of rehabilitationcomprehensive program of rehabilitation

More patients retained with More patients retained with buprenorphine in maintenancebuprenorphine in maintenance
42
32
20
05
1015202530354045
In treatment at 17 weeks
% re
tent
ion
Buprenorphine 8 mgMethadone 60 mgMethadone 20 mg
Johnson et al, 1992
* p<0.4 methadone 20 mg
*

13 consecutive opiate13 consecutive opiate--free free urinesurines
7
1316
25
0
5
10
15
20
25
30
Buprenorphine dose
% w
ith 1
3 co
nsec
utiv
opia
te-fr
ee s
ampl
es
1 mg4 mg8 mg16 mg
Ling et al, 1998

Mean opioid craving Mean opioid craving –– 1616--week week completerscompleters
15
20
25
30
35
40
45
50
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Week of study
Mea
n cr
avin
g sc
ore
1 mg buprenorphine4 mg buprenorphine
8 mg buprenorphine16 mg buprenorphine
Ling et al, 1998

Buprenorphine: Buprenorphine: Pharmacological AdvantagesPharmacological Advantages
Partial AgonistPartial Agonist•• high safety profile/ceiling effecthigh safety profile/ceiling effect•• low dependencelow dependence
Tight Receptor BindingTight Receptor Binding•• long duration of actionlong duration of action•• slow onset slow onset •• mild abstinencemild abstinence

Pharmacodynamic drug interactionsPharmacodynamic drug interactions
•• CNS depressants and sedatives (eg, CNS depressants and sedatives (eg, benzodiazepinesbenzodiazepines):):–– All oAll opioids pioids have additive sedative effects when used have additive sedative effects when used
in combination with other sedativesin combination with other sedatives•• Increased potential for respiratory depression, Increased potential for respiratory depression,
heavy sedation, coma, and deathheavy sedation, coma, and death
•• Despite favorable safety, use caution with Despite favorable safety, use caution with concomitant psychotropics (eg, concomitant psychotropics (eg, benzodiazepines)benzodiazepines)

Bup 0 mg
Bup 2 mg
Bup 16 mg
Bup 32 mg0 -
4 -
MRI
Bindingpotential(Bmax/Kd)
Effects of buprenorphine on Effects of buprenorphine on µµ--opioid opioid receptor availabilityreceptor availability
D Nutt. Personal communication

0 1 2 4 8 16 3210
11
12
13
14
15
16
17
Bre
aths
/Min
ute
PL Buprenorphine (mg, sl)
Human respiratory rate
Adapted from Walsh et al., 1994
Ceiling effect on respiratory Ceiling effect on respiratory depressiondepression

For how long does For how long does buprenorphine work? buprenorphine work? •• DDuration of action is dose related:uration of action is dose related:
–– 44––8mg: 8mg: 44––12 h12 h–– >8>8––16mg: 16mg: ~~24 h24 h–– >16>16––32mg: 32mg: 22––3 days3 days
(or 2(or 2––3 x maintenance dose)3 x maintenance dose)
•• Elimination Elimination half life half life ~24~24––36 h36 h
•• Steady state equilibrium achieved after 3Steady state equilibrium achieved after 3––7 days7 days
Note: high individual variabilityNote: high individual variability

Buprenorphine: Considerations for Buprenorphine: Considerations for Pain ManagementPain ManagementRolley E Johnson et al. Journal of Pain and Symptom Management,Rolley E Johnson et al. Journal of Pain and Symptom Management, Vol 29, No 3, March Vol 29, No 3, March 2005, pp2972005, pp297--326326

Open label study 95 consecutive patients on long term Open label study 95 consecutive patients on long term opioid therapy (LTOA) failing treatment based on:opioid therapy (LTOA) failing treatment based on:
Increased painIncreased painDecreased Functional CapacityDecreased Functional CapacityEmergence of opioid addiction (8%)Emergence of opioid addiction (8%)
Induced on buprenorphine 4Induced on buprenorphine 4--16mg (8mg mean dose)16mg (8mg mean dose)86% Experienced moderate to substantial pain relief86% Experienced moderate to substantial pain relief
Mood and function improvedMood and function improved
8% Discontinued due to side effects or increased pain8% Discontinued due to side effects or increased pain

Who can train you to become Who can train you to become certified?certified?•• Accredited buprenorphine training courses Accredited buprenorphine training courses
can be conducted only bycan be conducted only by::–– ASAM (American Society of Addiction ASAM (American Society of Addiction
Medicine)Medicine)–– AAAP (American Academy of Addiction AAAP (American Academy of Addiction
Psychiatry)Psychiatry)–– AMA (American Medical Association)AMA (American Medical Association)–– AOA (American Osteopathic Association)AOA (American Osteopathic Association)–– APA (American Psychiatric Association)APA (American Psychiatric Association)–– OOthers designated by the Secretary of HHSthers designated by the Secretary of HHS

How Can I Prescribe How Can I Prescribe Buprenorphine?Buprenorphine?
AAAP CD ROM CourseAAAP CD ROM CourseASAM Course ASAM Course www.buprenorphinecme.comwww.buprenorphinecme.comApply for DEA WaiverApply for DEA Waiver
Posting on SAMHSA website optionalPosting on SAMHSA website optional
Buprenorphine Mentoring ProgramBuprenorphine Mentoring Programwww.pcssmentor.orgwww.pcssmentor.org

ReferencesReferences
•• Principles of Addiction Medicine, 3Principles of Addiction Medicine, 3rdrd Ed., Allan Graham, Ed., Allan Graham, MD, etal, American Society Addiction Medicine, 2003MD, etal, American Society Addiction Medicine, 2003
•• Advances in Pain Management, vol 2 number 2, 2008, Advances in Pain Management, vol 2 number 2, 2008, Remedica publishingRemedica publishing
•• Urine Drug Testing in Primary Care, Douglas Gourlay, Urine Drug Testing in Primary Care, Douglas Gourlay, MD, and Howard Heit, MD, PharmaCom Group, Inc., MD, and Howard Heit, MD, PharmaCom Group, Inc., 20032003
•• Balancing Clinical and Risk Management Considerations Balancing Clinical and Risk Management Considerations for Chronic Pain Patients on Opioid Therapy, AAFP CME for Chronic Pain Patients on Opioid Therapy, AAFP CME Monograph, 2008Monograph, 2008
Top Related