




Languages
Pages
Legal


Original ArticleJ Gastric Cancer 2015;15(4):262-269 http://dx.doi.org/10.5230/jgc.2015.15.4.262
Copyrights © 2015 by The Korean Gastric Cancer Association www.jgc-online.org
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Radical gastrectomy with lymph node dissection in patients
with gastric cancer has been associated with a high rate of post-
operative complications, ranging from 20% to 46%.1-4 Accumu-
lated surgical experience and recent advances in surgical instru-
ments and perioperative management have led to a reduction in
postoperative morbidity and mortality.5-9 However, despite these
advances, major complications, particularly in high-risk patients,
remain problematic.
Intraabdominal abscess is one of the most commonly re-
ported post-gastrectomy complications. The incidence of in-
traabdominal abscess, manifesting as complex fluid collection
on computed tomography (CT), abdominal pain, fever, and
leukocytosis, ranges from 0.6% to 17%.1,3,7,8,10 The abscess is
usually detected within several days of surgery, and immediate
intervention is possible if the patient is still hospitalized. How-
ever, there are patients who present to the emergency depart-
ment with delayed intraabdominal abscess after an uneventful
discharge. With the recent introduction of the enhanced recov-
ery after surgery pathway hospital stays are shorter, and fewer
pISSN : 2093-582X, eISSN : 2093-5641
Correspondence to: Young-Woo Kim
Gastric Cancer Branch, Research Institute and Hospital, National Cancer Center, 323 Ilsan-ro, Ilsandong-gu, Goyang 10408, KoreaTel: +82-31-920-1635, Fax: +82-31-920-0696E-mail: [email protected] November 11, 2015Revised December 11, 2015Accepted December 12, 2015*These authors contributed equally to this paper as co-first authors.
Nomogram Estimating the Probability of Intraabdominal Abscesses after Gastrectomy in Patients with Gastric Cancer
Bang Wool Eom*, Jungnam Joo1,*, Young-Woo Kim, Boram Park1, Hong Man Yoon, Keun Won Ryu, and Soo Jin Kim
Gastric Cancer Branch and 1Biometric Research Branch, Research Institute and Hospital, National Cancer Center, Goyang, Korea
Purpose: Intraabdominal abscess is one of the most common reasons for re-hospitalization after gastrectomy. This study aimed to de-velop a model for estimating the probability of intraabdominal abscesses that can be used during the postoperative period.Materials and Methods: We retrospectively reviewed the clinicopathological data of 1,564 patients who underwent gastrectomy for gas-tric cancer between 2010 and 2012. Twenty-six related markers were analyzed, and multivariate logistic regression analysis was used to develop the probability estimation model for intraabdominal abscess. Internal validation using a bootstrap approach was employed to correct for bias, and the model was then validated using an independent dataset comprising of patients who underwent gastrectomy between January 2008 and March 2010. Discrimination and calibration abilities were checked in both datasets. Results: The incidence of intraabdominal abscess in the development set was 7.80% (122/1,564). The surgical approach, operating time, pathologic N classification, body temperature, white blood cell count, C-reactive protein level, glucose level, and change in the hemoglobin level were significant predictors of intraabdominal abscess in the multivariate analysis. The probability estimation model that was developed on the basis of these results showed good discrimination and calibration abilities (concordance index=0.828, Hosmer-Lemeshow chi-statistic P=0.274). Finally, we combined both datasets to produce a nomogram that estimates the probability of intraab-dominal abscess. Conclusions: This nomogram can be useful for identifying patients at a high risk of intraabdominal abscess. Patients at a high risk may benefit from further evaluation or treatment before discharge.
Key Words: Stomach neoplasms; Postoperative complications; Abdominal abscess; Nomograms

Nomogram for Intra-Abdominal Abscesses
263
intraabdominal abscesses after discharge has been reported.11-14
Therefore, accurate identification of clinical findings indicative
of a higher probability of intraabdominal abscess, which could
prompt further evaluation and treatment before discharge, would
be helpful.
This study aimed to identify clinical and laboratory markers
associated with intraabdominal abscess in patients who have un-
dergone gastrectomy for gastric cancer and to develop a model
for estimating the probability of intraabdominal abscess based on
multivariate analysis.
Materials and Methods
1. Study cohort
The study cohort (development set) consisted of 1,564 pa-
tients who underwent curative gastrectomy for gastric cancer
in the National Cancer Center, Korea, from April 2010 to June
2012. We adopted all surgical approaches: open gastrectomy and
laparoscopic or robot-assisted gastrectomy, regardless of the
extent of the surgery (subtotal or total gastrectomy). In patients
with early gastric cancer, more than D1+ lymph node dissection
was performed, and in those with more advanced tumors, more
than D2 lymph node dissection was performed, in accordance
with the Japanese Gastric Cancer Association guideline.15
An independent cohort comprising of 1,508 patients who
underwent gastrectomy for gastric cancer from January 2008 to
March 2010 was used as a validation set to evaluate the perfor-
mance of the development model. The inclusion and exclusion
criteria for the validation set were the same as those for the de-
velopment set.
Patients generally received in-hospital postoperative care for
5 to 7 days after surgery, and laboratory tests were conducted
on postoperative days 1, 3, 5, and 7. After discharge, the pa-
tients visited the outpatient clinic within 1 month for short-term
evaluation. Regular follow-up was then performed for 5 years.
The last follow-up days were August 31, 2012, and December
31, 2013, in the development and validation sets, respectively.
This study was approved by the Institutional Review Board at
the National Cancer Center (No. NCCNCS-13-786).
2. Definition of intraabdominal abscess
An intraabdominal abscess was defined by the following
three conditions: 1) Appearance of an extra-luminal fluid col-
lection on a postoperative abdominal CT scan; 2) Absence of
any other infection focus on the abdominal CT scan; 3) Record
of treatments such as antibiotics and/or surgical, endoscopic, and
radiological intervention provided because of moderate or se-
vere complications, according to the Accordion Severity Grad-
ing System of Surgical Complications.16 Clinically insignificant
fluid collections not requiring treatment were excluded from the
analysis.
3. Clinicopathological variables
All clinical variables suspected to be associated with intraab-
dominal abscess, including age, sex, body mass index (BMI),
comorbidities, surgical approach, extent of gastrectomy, extent
of lymph node dissection, combined operation, operating time,
pathological stage, number of antibiotics used, and transfusion,
were analyzed in both cohorts, along with postoperative vital
signs, inflammation-related laboratory values (i.e., white blood
cell [WBC] count, segmented neutrophils, C-reactive protein
[CRP], total bilirubin [T. bil], glucose, serum amylase), and
change in hemoglobin level (HbD) from the preoperative period
to postoperative day 5 or 7. The highest values recorded during
the hospital period were used, and the tumor stage was defined
according to the American Joint Committee on Cancer staging
system, 7th edition.17
4. Statistical analysis
All continuous variables are presented as means±standard
deviation, and categorical variables are shown as proportions.
Distribution differences were tested using the chi-square test for
categorical variables and the t-test for continuous variables.
Logistic regression with intraabdominal abscess as an out-
come was carried out for both the univariate and multivariate
analyses. Univariate analyses were separately conducted for 26
potentially related factors, and all variables were then included
in the multivariate model. The final risk estimation model was
formulated on the basis of backward variable selection, with an
elimination criterion of P>0.05. Adjacent categories of certain
categorical variables, such as serum amylase, were grouped to-
gether when decreasing odds ratios were observed for increasing
values of related factors. The performance of the model was
then evaluated in terms of discrimination and calibration. For
discrimination, we examined the receiver operating character-
istics curve (ROC) and associated area under the ROC curve
(AUC), and to test calibration, we used the Hosmer-Lemeshow
(HL) chi-square statistic.

Eom BW, et al.
264
Internal validation using a bootstrap approach was then em-
ployed to correct biases.18 In this approach, random samples
of the same sample size were drawn from the original dataset
with replacement to form a bootstrap sample. The same model-
building technique was used on the bootstrap samples. This
bootstrap resampling procedure was repeated 2,000 times to ob-
tain the average bias, which provided a bias-corrected estimate
for performance measures. The risk estimation model was then
applied to the validation set to examine the performance of the
model on independent data. When the performance was accept-
able, the same procedure was performed for the entire dataset
(development and validation sets).19
Data analyses were performed using SAS ver. 9 (SAS Institute
Inc., Cary, NC, USA), and R software (ver. 2.12.1). All reported
P-values are two-sided.
Results
1. Clinicopathological characteristics in the
development and validation datasets
The incidence of intraabdominal abscess was 7.80%
(122/1,564) in the development set and 7.76% (117/1,508) in the
validation set. Among patients in the abscess group of the devel-
opment set, 65 patients (53.3%) were diagnosed with the abscess
during hospitalization and 43 patients (35.2%) presented to the
emergency department with abscess after discharge. Intraab-
dominal abscess was detected incidentally during prechemo-
therapy CT scans at 3 to 5 weeks postoperatively in 14 patients
(11.5%).
Patient characteristics and clinicopathological features were
compared between abscess and non-abscess groups in both
datasets (Supplement 1). In the development dataset, patients in
the abscess group were older and had higher BMI and prolonged
operating times, compared with the patients in the non-abscess
group. The abscess group had a greater number of male patients,
and the numbers of open surgeries, total gastrectomies, com-
bined operations, transfusions, and advanced pT and pN stages
were higher. Similar results were noted in the validation set, and
significant differences were observed for sex, incidence of hy-
pertension, extent of gastrectomy, combined operation, operat-
ing time, numbers of antibiotics used, transfusion, and pT.
In terms of postoperative vital signs and inflammation-relat-
ed laboratory data (Supplement 1), in the development set, fe-
ver; elevated heart rate, WBC count, segment neutrophil count,
and CRP; T. bil; glucose; and amylase levels; along with greater
values of HbD were associated with abscess, and the validation
set showed comparable results with the development set.
2. Development of the risk estimation model
Univariate and multivariate logistic regression analyses were
first performed using the development dataset (Table 1). The
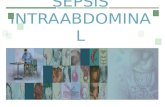
apparent discrimination and calibration performances were good,
with AUC=0.828 (95% confidence interval [CI], 0.788~0.868)
and HL chi-square test statistic=3.888 with P=0.274 (Fig. 1).
After bias correction with 2,000 cycles of bootstrap resampling,
the bias-corrected AUC was 0.801, and the HL chi-square test
statistic was 5.511 with P=0.138, which implied a good value.
The risk estimation model for probability of intraabdominal
abscess formulated using the development set was then applied
to the independent validation set. The AUC was 0.791 (95%
Table 1. Multivariate logistic regression analysis using the development set
Characteristic Subgroup Odds ratio (95% CI) P-value
Surgical approach Laparoscopy/robot
1
Open 1.76 (1.11~2.81) 0.017
Operating time (min) 1.01 (1.00~1.01) <0.001
pN 0 1
1 1.70 (0.94~3.09) 0.079
2, 3 1.75 (1.07~2.86) 0.026
Body temperature (oC)* <37.8 1
≥37.8 2.22 (1.44~3.42) <0.001
WBC (/μl)* <12 1
12~14.9 1.66 (1.04~2.63) 0.033
≥15 2.10 (1.18~3.74) 0.012
CRP (mg/dl)* <10 1
10~14.9 1.10 (0.50~2.41) 0.817
15~19.9 1.78 (0.83~3.82) 0.139
≥20 4.52 (2.18~9.36) <0.001
Glucose (mg/dl)* <150 1
150~199 1.18 (0.74~1.88) 0.493
≥200 2.34 (1.36~4.00) 0.002
Hemoglobin difference (g/dl)
<3 1
≥3 1.89 (1.23~2.90) 0.004
CI = confidence interval; WBC = white blood cell count; CRP = C-reactive protein. *The highest values for the vital signs and inflammatory markers were used in the analysis.

Nomogram for Intra-Abdominal Abscesses
265
CI, 0.751~0.832), and the HL chi-square result was 18.286 with
P=0.001. Although the calibration was slightly off, it showed
good discrimination, and the AUC was close to the value ex-
pected by internal validation.
3. Final model using the total dataset
Because the model development procedure was validated, we
used the total dataset (development and validation sets) to gen-
erate the final risk estimation model. The multivariate analysis
identified the extent of gastrectomy, operating time, transfusion,
pT, temperature, WBC count, segmented neutrophils, CRP and
amylase levels, and HbD as independent risk factors for intraab-
dominal abscess (Table 2).
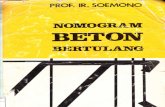
4. Development of the nomogram
We created a nomogram that estimates the risk of intraab-
dominal abscess on the basis of the final risk estimation model
(Fig. 2). Points are assigned for each factor, and the sum of the
points for all factors included in the model is obtained and cor-
responds to the estimated probability of the development of an
intraabdominal abscess after gastrectomy. Considering that the
incidence of intraabdominal abscess was approximately 7.8%
in this study, we calculated the sensitivity, specificity, positive
predictive value (PPV), and negative predictive value (NPV) for
each cut-off value between 6 and 9% in 0.5% increments (Table
3). For example, if a patient has an estimated probability of in-
traabdominal abscess of >7.5%, we can expect approximately
75.3% sensitivity, 74.3% specificity, 19.8% PPV, and 97.3% NPV
for postoperative intraabdominal abscess.
Discussion
Intraabdominal abscess is one of the most common reasons
for an early visit to the emergency department after gastrectomy.
A
0.0 0.2 0.4 0.6 0.8 1.0
1.0
0.8
0.6
0.4
0.2
Sensitiv
ity
1-Specificity
0.0
ActualPredicted
AUC=0.828 (95% CI, 0.788~0.868)Bias corrected AUC=0.801
Development data
1 2 3 4 5 6 7 8 9 10
45
40
35
30
25
20
15
10
5
Pro
babili
tyofdevelo
pin
gabscess
(%)
Decile of predicted risk based on model
0
Development data
�2=3.888 (P-value=0.274)
Bias corrected =5.511 (2
P-value=0.138)�
B
C
0.0 0.2 0.4 0.6 0.8 1.0
1.0
0.8
0.6
0.4
0.2
Sensitiv
ity
1-Specificity
0.0
AUC=0.791 (95% CI, 0.751~0.832)
Validation data
1 2 3 4 5 6 7 8 9 10
45
40
35
30
25
20
15
10
5
Pro
babili
tyofdevelo
pin
gabscess
(%)
Decile of predicted risk based on model
0
Validation dataD
�2=18.286 (P-value=0.001)
Fig. 1. Receiever-operator characteristic curve and calibration plots of the prediction model for the development dataset and the entire (development and validation) dataset. AUC = area under the receiver operating characteristics curve; CI = confidence interval.

Eom BW, et al.
266
Some patients who are symptom-free at the time of discharge
develop abdominal pain or fever within several days after dis-
charge, and only then is an intraabdominal abscess detected. In
this study, we developed a nomogram to estimate the probability
of intraabdominal abscess on the basis of postoperative clinical
findings. A physician can use the nomogram to check the prob-
ability of intraabdominal abscess before discharging the patient,
and may choose to perform further evaluation or treatment if
the patient has a high probability of developing abscess.
There are several useful scoring systems for predicting clinical
outcomes, including the Sequential Organ Failure Assessment,
the Acute Physiology and Chronic Health Evaluation II scor-
ing system, the Simplified Acute Physiology Score II, and the
Physiological and Operative Severity Score for the enUmeration
of Mortality and Morbidity (POSSUM).20-23 Among these scoring
systems, POSSUM has been validated in various surgical fields,
and a nomogram based on POSSUM has been recently devel-
oped.24-27 However, these scoring systems are used to predict
general morbidity or mortality, whereas our nomogram is solely
focused on the risk of intraabdominal abscess after gastrectomy
in patients with gastric cancer.
Risk factors for post-gastrectomy complications have been
well reported, and include older age, male sex, presence of
comorbidities, advanced tumor stage, open surgical approach,
extended lymph node dissection, combined resection, and pro-
longed operating time.28-32 In terms of intraabdominal abscess
in particular, Lo et al.33 reported that the predisposing factors
include age, prolonged operating time, and combined organ
resection. While previous studies have identified risk factors ac-
cording to baseline or preoperative findings to predict complica-
tions in the early postoperative period, our study was performed
to estimate the probability of intraabdominal abscess in patients
who are ready for discharge. Therefore, we included not only
preoperative baseline factors but also postoperative vital signs
and laboratory findings in our analyses.
One of the potential benefits of our nomogram is the preven-
tion of delayed sepsis. Intraabdominal abscesses that are detected
in a timely fashion are readily treated with antibiotics, percuta-
neous drainage, or both.33 By contrast, delayed detection of an
abscess can result in sepsis or associated complications including
pseudoaneurysm, and the long-term sequelae may be irrevers-
ible. Because our nomogram predicts the probability of intraab-
dominal abscess, the physician can perform additional tests and
render necessary treatment before discharging the patient, and
delayed sepsis might be prevented. This could also contribute to
reduced hospital costs, which are high when patients are read-
mitted with postoperative infections.34-36 In one Swedish study,
the cost of readmission for small bowel obstruction was ap-
proximately equal to that of gastric cancer treatment.37 Another
potential benefit is the limitation of abdominal CT scanning to
only those patients with a high probability of abscess, which
would further contribute to the reduction of hospital costs.
Larger datasets provide better estimates of the effect of each
factor once a procedure for developing a risk estimation model
is validated by using acceptable performance. Therefore, we
evaluated models from both the development dataset and the to-
tal dataset, and found that there was some variation in significant
factors. In the model using the total dataset, surgical approach,
Table 2. Multivariate logistic regression using the total dataset
Characteristic Subgroup Odds ratio (95% CI) P-value
Extent of gastrectomy Subtotal 1
Total 1.60 (1.18~2.18) 0.003
Operating time (min) 1.00 (1.00~1.01) 0.005
Postoperative transfusion Absent 1
Present 2.25 (1.36~3.75) 0.002
pT 1 1
2, 3 1.53 (1.10~2.13) 0.011
4 1.93 (1.29~2.91) 0.002
Body temperature (oC)* <37.8 1
≥37.8 2.32 (1.72~3.13) <0.001
WBC (/μl)* <12 1
12~14.9 1.53 (1.06~2.21) 0.021
≥15 1.54 (1.07~2.22) 0.012
Seg neutrophil (%)* <75 1
75~84.9 1.79 (1.13~2.83) 0.013
≥85 2.72 (1.62~4.56) <0.001
CRP (mg/dl)* <10 1
10~14.9 1.57 (0.93~2.65) 0.095
15~19.9 2.85 (1.73~4.71) <0.001
≥20 5.40 (3.35~8.70) <0.001
Amylase (U/L)* 1~200 1
≥200 1.80 (1.31~2.47) <0.001
Hemoglobin difference (g/dl) <3 1
≥3 1.65 (1.22~2.23) 0.001
CI = confidence interval; WBC = white blood cell count; CRP = C-reactive protein. *The hightest values for the vital signs and inflam-matory markers were used in the analysis.

Nomogram for Intra-Abdominal Abscesses
267
pN, and glucose were replaced with the extent of gastrectomy,
pT, neutrophil count, amylase level, and transfusion. When we
performed internal validation by bootstrapping, we found that
significant risk factors were frequently matched with those in
the total dataset, and we therefore decided to develop our nomo-
gram on the basis of the total dataset. This method provided better
statistical accuracy for estimating the effects of each factor.
Once we generated an acceptable risk prediction model, we
checked its discrimination and calibration abilities. Discrimina-
tion accounts for the probability of a model producing higher
risk estimates for patients who develop intraabdominal abscess
than it does for those who do not, and calibration determines
how closely the estimated probabilities match the observed
probabilities. We used the bootstrap approach for internal vali-
dation because bias occurs when discrimination and calibration
are calculated on the basis of a development dataset. The differ-
ence between performance measures in the model for the boot-
strap samples and the original dataset represents the bias indicating
over-fitting, and the bias-corrected measure indicates how well
the model will perform on an external independent dataset.
In producing our model, we defined all cases of fluid col-
lection as intraabdominal abscess, and there were some patients
who had both fluid collection (abscess) and anastomotic leakage.
In the development dataset, among 122 patients in the abscess
group, 17 (13.9%) had CT findings of probable anastomotic
leakage and 14 underwent further evaluations such as an en-
doscopy and upper gastrointestinal series, 3 (2.5%) of whom
had confirmed anastomotic leakage. Further, there were 8 of 16
patients without any suggestion of leakage on CT scan who were
diagnosed with leakage by other means. In total, there were 11
patients (11/122, 9.0%) in the abscess group of the development
dataset who had anastomotic leaks, suggesting that a more thor-
ough evaluation for this complication may be necessary.
The incidence of intraabdominal abscess after gastrectomy
Table 3. Sensitivity, specificity, PPV, and NPV of predicted probability using the nomogram for cut off points from 6% to 9% (increments of 0.5%)
Predicted probability (%)
Sensitivity (%)
Specificity (%)
PPV (%)
NPV (%)
6.0 78.7 69.5 17.9 97.5
6.5 77.0 71.3 18.5 97.3
7.0 76.2 72.8 19.1 97.3
7.5 75.3 74.3 19.8 97.3
8.0 74.1 75.9 20.6 97.2
8.5 73.2 77.4 21.4 97.2
9.0 72.4 78.5 22.1 97.1
PPV = positive predictive value; NPV = negative predictive value.
Points
Gastrectomy
OP time (min)
pT
Bodytemperature ( C)
WBC ( )�l
Seg neutrophil (%)
CRP (mg/dl)
Amylase (mg/dl)
Hb difference
Postoperativetransfuson
Total points
Linear predictor
Risk of abscess (%)
Subtotal Total
1 2 or 3 4
0 10 20 30 40 50 60 70 80 90 100
0900100 200 300 400 500 600 700 800
<37.8 >37.8
>12,000<12,000
<75 75~84.9 >85
<10 10~14.9 15~19.9 >20
<200 >200
<3 >3
No Yes
0 50 100 150 200 250 300 350
6 5 4 3 2 1 0 1 2
1 5 10 20 30 40 50 60 70 80
Fig. 2. A nomogram estimating the probability of developing intraab-dominal abscess after gastrectomy. OP = operative; WBC = white blood cell; CRP = C-reactive protein; Hb = hemoglobin.

Eom BW, et al.
268
in gastric cancer patients may be affected by various additional
factors, including surgeon, institution and tumor location. There-
fore, evaluating our nomogram by using patient data from other
institutions will be necessary. Additionally, the present study was
performed using retrospectively collected data, and there may be
selection, information, and measurement biases. However, we be-
lieve these biases had a weak influence on the results because all
variables were objective values, and there was little missing data.
In conclusion, we have developed a nomogram for estimating
the risk of intraabdominal abscess after gastrectomy in gastric
cancer patients. The availability of a calculated probability for
the development of intraabdominal abscess may help a physi-
cian decide whether further evaluation or treatment should be
ordered before a patient is discharged. Additional external vali-
dation using a multicenter dataset will be useful to generalize the
utility of the nomogram.
Acknowledgments
The authors thank Kyoung Rae Kim, Youngsook Kim, Eunju
Yoo, Soosie Kim, Suhee Kim, Hyun Jung Park, and Deok Hee
Kim for data collection and management.
This work was supported by a grant from the National Can-
cer Center (No. NCC-1410130-1).
Conflicts of Interest
No potential conflict of interest relevant to this article was
reported.
Electronic Supplementary Material
The online version of this article (doi: 10.5230/jgc.2015.15.
4.262) contains supplementary materials.
References
1. Bonenkamp JJ, Songun I, Hermans J, Sasako M, Welvaart K, Plukker JT, et al. Randomised comparison of morbidity after D1 and D2 dissection for gastric cancer in 996 Dutch patients. Lancet 1995;345:745-748.
2. Cuschieri A, Fayers P, Fielding J, Craven J, Bancewicz J, Joy-paul V, et al; The Surgical Cooperative Group. Postoperative morbidity and mortality after D1 and D2 resections for gastric
cancer: preliminary results of the MRC randomised controlled surgical trial. Lancet 1996;347:995-999.
3. Sano T, Sasako M, Yamamoto S, Nashimoto A, Kurita A, Hi-ratsuka M, et al. Gastric cancer surgery: morbidity and mor-tality results from a prospective randomized controlled trial comparing D2 and extended para-aortic lymphadenectomy: Japan Clinical Oncology Group study 9501. J Clin Oncol 2004;22:2767-2773.
4. Zilberstein B, Martins BC, Jacob CE, Bresciani C, Lopasso FP, de Cleva R, et al. Complications of gastrectomy with lymphad-enectomy in gastric cancer. Gastric Cancer 2004;7:254-259.
5. Ryu KW, Kim YW, Lee JH, Nam BH, Kook MC, Choi IJ, et al. Surgical complications and the risk factors of laparoscopy-assisted distal gastrectomy in early gastric cancer. Ann Surg Oncol 2008;15:1625-1631.
6. Ahn CW, Hur H, Han SU, Cho YK. Comparison of intracorpo-real reconstruction after laparoscopic distal gastrectomy with extracorporeal reconstruction in the view of learning curve. J Gastric Cancer 2013;13:34-43.
7. Kim KM, An JY, Kim HI, Cheong JH, Hyung WJ, Noh SH. Major early complications following open, laparoscopic and robotic gastrectomy. Br J Surg 2012;99:1681-1687.
8. Kim HH, Hyung WJ, Cho GS, Kim MC, Han SU, Kim W, et al. Morbidity and mortality of laparoscopic gastrectomy versus open gastrectomy for gastric cancer: an interim report: a phase III multicenter, prospective, randomized Trial (KLASS Trial). Ann Surg 2010;251:417-420.
9. Kim YW, Yoon HM, Eom BW, Park JY. History of minimally invasive surgery for gastric cancer in Korea. J Gastric Cancer 2012;12:13-17.
10. Wu CW, Hsiung CA, Lo SS, Hsieh MC, Shia LT, Whang-Peng J. Randomized clinical trial of morbidity after D1 and D3 sur-gery for gastric cancer. Br J Surg 2004;91:283-287.
11. Tang J, Humes DJ, Gemmil E, Welch NT, Parsons SL, Cat-ton JA. Reduction in length of stay for patients undergoing oesophageal and gastric resections with implementation of en-hanced recovery packages. Ann R Coll Surg Engl 2013;95:323-328.
12. Grantcharov TP, Kehlet H. Laparoscopic gastric surgery in an enhanced recovery programme. Br J Surg 2010;97:1547-1551.
13. So JB, Lim ZL, Lin HA, Ti TK. Reduction of hospital stay and cost after the implementation of a clinical pathway for radical gastrectomy for gastric cancer. Gastric Cancer 2008;11:81-85.
14. Choi JW, Xuan Y, Hur H, Byun CS, Han SU, Cho YK. Out-

Nomogram for Intra-Abdominal Abscesses
269
comes of critical pathway in laparoscopic and open surgical treatments for gastric cancer patients: patients selection for fast-track program through retrospective analysis. J Gastric Cancer 2013;13:98-105.
15. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer 2011;14:113-123.
16. Strasberg SM, Linehan DC, Hawkins WG. The accordion severity grading system of surgical complications. Ann Surg 2009;250:177-186.
17. Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A, eds. AJCC Cancer Staging Handbook. 7th ed. New York: Springer-Verlag, 2010.
18. Harrell FE Jr, Lee KL, Mark DB. Multivariable prognostic models: issues in developing models, evaluating assumptions and adequacy, and measuring and reducing errors. Stat Med 1996;15:361-387.
19. Simon R. Diagnostic and prognostic prediction using gene expression profiles in high-dimensional microarray data. Br J Cancer 2003;89:1599-1604.
20. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonça A, Bruining H, et al; On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. The SOFA (Sepsis-related Organ Failure Assess-ment) score to describe organ dysfunction/failure. Intensive Care Med 1996;22:707-710.
21. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med 1985;13:818-829.
22. Le Gall JR, Lemeshow S, Saulnier F. A new Simplified Acute Physiology Score (SAPS II) based on a European/North Amer-ican multicenter study. JAMA 1993;270:2957-2963.
23. Copeland GP, Jones D, Walters M. POSSUM: a scoring system for surgical audit. Br J Surg 1991;78:355-360.
24. Wijesinghe LD, Mahmood T, Scott DJ, Berridge DC, Kent PJ, Kester RC. Comparison of POSSUM and the Portsmouth pre-dictor equation for predicting death following vascular surgery. Br J Surg 1998;85:209-212.
25. Sagar PM, Hartley MN, MacFie J, Taylor BA, Copeland GP. Comparison of individual surgeon's performance. Risk-adjust-ed analysis with POSSUM scoring system. Dis Colon Rectum 1996;39:654-658.
26. Neary B, Whitman B, Foy C, Heather BP, Earnshaw JJ. Value of POSSUM physiology scoring to assess outcome after intra-
arterial thrombolysis for acute leg ischaemia (short note). Br J Surg 2001;88:1344-1345.
27. Williams DJ, Walker JD. A nomogram to calculate the Physi-ological and Operative Severity Score for the enUmeration of Mortality and morbidity (POSSUM). Br J Surg 2014;101:239-245.
28. Hartgrink HH, van de Velde CJ, Putter H, Bonenkamp JJ, Klein Kranenbarg E, Songun I, et al. Extended lymph node dissection for gastric cancer: who may benefit? Final results of the randomized Dutch gastric cancer group trial. J Clin Oncol 2004;22:2069-2077.
29. Park DJ, Lee HJ, Kim HH, Yang HK, Lee KU, Choe KJ. Pre-dictors of operative morbidity and mortality in gastric cancer surgery. Br J Surg 2005;92:1099-1102.
30. Seo SH, Hur H, An CW, Yi X, Kim JY, Han SU, et al. Operative risk factors in gastric cancer surgery for elderly patients. J Gas-tric Cancer 2011;11:116-121.
31. Lee JH, Park do J, Kim HH, Lee HJ, Yang HK. Comparison of complications after laparoscopy-assisted distal gastrectomy and open distal gastrectomy for gastric cancer using the Clavien-Dindo classification. Surg Endosc 2012;26:1287-1295.
32. Bozzetti F, Marubini E, Bonfanti G, Miceli R, Piano C, Crose N, et al; The Italian Gastrointestinal Tumor Study Group. Total versus subtotal gastrectomy: surgical morbidity and mortal-ity rates in a multicenter Italian randomized trial. Ann Surg 1997;226:613-620.
33. Lo CH, Chen JH, Wu CW, Lo SS, Hsieh MC, Lui WY. Risk factors and management of intra-abdominal infection after extended radical gastrectomy. Am J Surg 2008;196:741-745.
34. Miletic KG, Taylor TN, Martin ET, Vaidya R, Kaye KS. Re-admissions after diagnosis of surgical site infection following knee and hip arthroplasty. Infect Control Hosp Epidemiol 2014;35:152-157.
35. Avritscher EB, Cooksley CD, Rolston KV, Swint JM, Delclos GL, Franzini L, et al. Serious postoperative infections follow-ing resection of common solid tumors: outcomes, costs, and impact of hospital surgical volume. Support Care Cancer 2014;22:527-535.
36. Keller DS, Swendseid B, Khorgami Z, Champagne BJ, Reyn-olds HL Jr, Stein SL, et al. Predicting the unpredictable: com-paring readmitted versus non-readmitted colorectal surgery patients. Am J Surg 2014;207:346-351; discussion 350-351.
37. Tingstedt B, Isaksson J, Andersson R. Long-term follow-up and cost analysis following surgery for small bowel obstruction caused by intra-abdominal adhesions. Br J Surg 2007;94:743-748.

Supplement 1. Patient characteristics, clinicopathological features, postoperative vital signs, and inflammation-related laboratory findings in the development and validation datasets
Characteristic Subgroup
Development set (n = 1564) Validation set (n = 1508) No abscess
(%) Abscess (%)
P Non-abscess
(%) Abscess
(%) P ( n = 1442 ) (n = 122) (n = 1391) (n = 117)
Age (mean ± SD)
58.5±12.0 61.5±11.3 0.009 58.2±11.9 60.4±12.0 0.055
Sex Male 942 (65.3) 99 (81.1) <0.001 906 (65.1) 94 (80.3) 0.001
Female 500 (34.7) 23 (18.8) 485 (34.9) 23 (19.7)
BMI (kg/m2) (mean ± SD)
23.7±3.1 24.4±3.5 0.013 23.6±3.2 23.8±3.0 0.462
Diabetes mellitus Absent 1234 (85.6) 101 (82.8) 0.403 1226 (88.1) 101 (86.3) 0.562
Present 208 (14.4) 21 (17.2) 165 (11.9) 16 (13.7)
Hypertension Absent 974 (67.5) 75 (61.5) 0.171 1011 (72.7) 73 (62.4) 0.017
Present 468 (32.5) 47 (38.5) 380 (27.3) 44 (37.6)
Heart disease Absent 1332 (92.3) 109 (89.3) 0.233 1347 (96.8) 113 (96.6) 0.784
Present 110 (7.6) 13 (10.7) 44 (3.2) 4 (3.4)
Liver disease Absent 1364 (94.6) 118 (96.7) 0.311 1242 (89.3) 104 (88.9) 0.893
Present 78 (5.4) 4 (3.2) 149 (10.7) 13 (11.1)
Pulmonary disease
Absent 1407 (97.6) 116 (95.1) 0.128 1370 (98.5) 115 (98.3) 0.698
Present 35 (2.4) 6 (4.9) 21 (1.5) 2 (1.7)
Surgical approach Open 661 (45.8) 84 (68.9) <0.001 802 (57.7) 81 (69.2) 0.015
Laparoscopy 781 (54.2) 38 (31.1)
589 (42.3) 36 (30.8)
/Robot
Extent of gastrectomy
Subtotal 1065 (73.9) 76 (62.3) 0.006 1029 (74.0) 50 (42.7) <0.00
1
Total 377 (26.1) 46 (37.7) 362 (26.0) 67 (57.3)
LN dissection D1+ 127 (8.8) 6 (4.9) 0.139 88 (6.3) 4 (3.4) 0.207
D2 1315 (91.2) 116 (95.1) 1303 (93.7) 113 (96.6)
Combined operation
Absent 1305 (90.5) 95 (77.9) <0.001 1344 (96.6) 99 (84.6) <0.00
1
Present 137 (9.5) 27 (22.1) 47 (3.4) 18 (15.4)
Operating time (mean ± SD) 177.3±64.1 214.4±84.8 <0.001 187.1±71.8 212.9±102.
4 0.009
Number of Antibiotics
1–2 1434 (99.4) 120 (98.4) 0.18 145 (10.4) 20 (17.1) 0.026
usage ≥3 8 (0.6) 2 (1.6) 1246 (89.6) 97 (82.9)
Postoperative transfusion
Absent 1402 (97.2) 111 (91.0) 0.001 1332 (95.8) 97 (82.9) <0.00
1
Present 40 (2.8) 11 (9.0) 59 (4.2) 20 (17.1)
pT 1 915 (63.5) 52 (42.6) <0.001 742 (53.3) 45 (38.5) 0.001
2,3 381 (26.4) 43 (35.2) 469 (33.7) 45 (38.5)
4 146 (10.1) 27 (22.1) 180 (12.9) 27 (23.1)
pN 0 994 (68.9) 61 (50.0) <0.001 893 (64.2) 67 (57.3) 0.084

1 167 (11.6) 20 (16.4) 173 (12.4) 12 (10.3)
2,3 281 (19.5) 41 (33.6) 325 (23.4) 38 (32.5) *Body temperature (°C)
<37.8 1106 (76.7) 51 (41.8) <0.001 1042 (74.9) 49 (41.9) <0.00
1
≥37.8 336 (23.3) 71 (58.2) 349 (25.1) 68 (58.1)
*Pulse rate <100 1035 (71.8) 62 (50.8) <0.001 1044 (75.1) 48 (41.0) <0.00
1
100–119 338 (23.4) 41 (33.6) 299 (21.5) 55 (47.0)
≥120 69 (4.8) 19 (15.6) 48 (3.5) 14 (12.0)
*WBC (/㎕) <12 990 (68.7) 51 (41.8) <0.001 385 (27.7) 16 (13.7) 0.002
12–14.9 334 (23.2) 43 (35.2) 430 (30.9) 36 (30.8)
≥15 118 (8.2) 28 (23.0) 576 (41.4) 65 (55.6)
*Seg neutrophil (%)
<75 393 (27.3) 15 (12.3) <0.001 351 (25.2) 10 (8.5) <0.00
1
75–84.9 884 (61.3) 68 (55.7) 879 (63.2) 67 (57.3)
≥85 165 (11.4) 39 (32.0) 161 (11.6) 40 (34.2)
*CRP (mg/dL) <10 479 (33.2) 11 (9.0) <0.001 576 (41.4) 14 (12.0) <0.00
1
10–14.9 430 (29.8) 20 (16.4) 357 (25.7) 19 (16.2)
15–19.9 300 (20.8) 26 (21.3) 258 (18.5) 34 (29.1)
≥20 233 (16.2) 65 (53.3) 200 (14.4) 50 (42.7)
*T. bil (mg/dL) <1.2 834 (57.8) 51 (41.8) <0.001 813 (58.4) 60 (51.3) 0.196
1.2–2.9 584 (40.5) 64 (52.5) 545 (39.2) 52 (44.4)
≥3 24 (1.7) 7 (5.7) 33 (2.4) 5 (4.2)
*Glucose (mg/dL) <150 834 (57.8) 49 (40.2) <0.001 413 (29.7) 23 (19.7) 0.003
150–199 450 (31.2) 41 (33.6) 755 (54.3) 62 (53.0)
≥200 158 (11.0) 32 (26.2) 223 (16.0) 32 (27.4)
*Amylase (U/) <100 800 (55.5) 52 (42.6) <0.001 629 (45.2) 31 (26.5) <0.00
1
101–200 440 (30.5) 36 (29.5) 461 (33.1) 34 (29.1)
>201 202 (14.0) 34 (27.9) 301 (21.6) 52 (44.4)
Hemoglobin difference
<3 1135 (87.7) 61 (50.0) <0.001 884 (63.6) 54 (46.2) <0.00
1
(g/dL) ≥3 307 (21.3) 61 (50.0) 507 (36.5) 63 (53.8)
SD, standard deviation; BMI, body mass index; LN, lymph node; WBC, white blood cell count; CRP, C-reactive protein; T. bil, total bilirubin. * The highest values for the vital signs and inflammatory markers were used in the analysis.
Top Related