




Languages
Pages
Legal


46Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1 47 Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 146Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1 47 Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1
Anju Bansal, Fouzia Siraj, Shabnam
Bhandari Grover 1, Amar Bhatnagar2,
Sunita Saxena
Department of Pathology, National Institute of Pathology (ICMR), Safdarjung Hospital Campus,
New Delhi,1Departments of Radiology and 2Cancer
Surgery, Safdarjung Hospital and Vardhman Mahavir Medical
College, New Delhi, India
Address for Correspondence: Dr. Anju Bansal, 3126, Sector‑D,
Pocket‑3, Vasant Kunj, New Delhi ‑ 110 070, India.
E‑mail: [email protected]
Mesenteric lymphangioma: A rare intraabdominal finding in a pregnant woman
Mesenteric cavernous lymphangioma is a rare benign tumor, not often described in literature. The etiopathogenesis of this tumor is largely unknown. Clinically, the presentation is variable and may be asymptomatic or present with subacute or acute abdomen. We describe here a case of 23-year-old pregnant woman with an asymptomatic abdominal mass which was incidentally detected after ultrasound examination during antenatal visit. The pregnancy was subsequently terminated and the patient underwent surgical excision of the tumor along with intestinal resection. The mass was pathologically diagnosed to be mesenteric cavernous lymphangioma.
Key words: Lymphangioma, mesenteric mass, pregnant woman
INTRODUCTION
Lymphangioma is a benign neoplasm which usually occurs in children, common sites being head, neck and axilla.[1] These are considered to be congenital lymphatic malformations rather than true lymphatic neoplasms. Lymphangioma occurring in small bowel mesentery in an adult is very rare accounting for approximately 1% of lymphangiomas. Preoperative diagnosis is often difficult due to the clinical course that is frequently silent. Radiological investigations are a useful diagnostic tool, but definitive diagnosis is confirmed only by histopathology after a complete surgical resection. Surgical excision of the tumor is essential to prevent life‑threatening complications and at times an extensive surgery involving adjacent organs may be required for complete resection.
CASE REPORT
A 23‑year‑old female presented with amenorrhea for 2 months. Pregnancy was suggested by a positive Gravindex test which is an agglutination inhibition test performed on a urine sample to detect pregnancy. The patient was further advised routine laboratory investigations and an ultrasound to confirm the pregnancy. Ultrasound abdomen showed a live fetus of 6 weeks maturity. In addition, a large non‑homogenous lesion measuring 10.6 × 4.8 cm with ill‑defined margins was seen in the infraumbilical region just below the abdominal wall. Ultrasound‑guided fine‑needle aspiration cytology (FNAC) was performed from the mass which revealed clusters of inflammatory cells and cyst macrophages in a background of proteinaceous material. A diagnosis of a benign cystic lesion was made. The patient was advised termination of pregnancy and surgical excision of the mass.
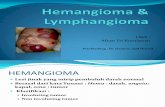
Preoperative CT and MRI evaluation was done. Contrast‑enhanced CT examination revealed a well‑marginated, spherical hypodense mass in the umbilical region. It was intraperitoneal in location and was encasing the mesenteric vessels (arrow) [Figure 1a]. The mass showed extension and streaking toward mesenteric surface of adjoining jejunal loops. The inferior limit of the tumor was at the pelvic brim. The mass measured approximately 8 × 10 × 15 cm in size. MR examination also confirmed the well‑defined lesion and encasement of mesenteric vessels. The pelvic organs were not involved [Figure 1b]. The patient underwent laparotomy with excision of the mesenteric mass and adjoining bowel loop which was sent for histopathological examination.
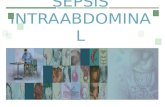
Grossly, a segment of small intestine with attached mesenteric mass was received [Figure 2a]. Intestine measured 40 cm in length. In the mesenteric fat there was a nodular mass measuring 10 × 6 × 5 cm. The outer surface was smooth and congested. Cut section was lobulated, grey white, soft with tiny
Abs
trac
t
Access this article online
Website: ***
DOI: 10.4103/2348-3113.139651
Quick response code:
Case Repor t

Figure 4: (a) Immunohistochemical staining showing the endothelial cells to be positive for CD31 (x200). (b)Immunohistochemical staining showing the endothelial cells to be positive for CD34 (x400)
Figure 1: (a) Contrast enhanced CT abdomen coronal reveals a hypodense, large spherical mass in the umbilical region which is encasing the mesenteric vessels (arrow). There is streaking and extension of disease into the mesenteric surface of adjoining jejunum. (b) MRI of lower abdomen and pelvis T1W showing a cystic lesion in the infraumbilical region. Pelvic organs are normal
Figure 2: (a) Gross image of segment of small intestine with attached mesenteric mass showing bosselation and congestion externally. (b) Cut section is grey white with foci of congestion
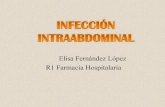
Figure 3: (a) Photomicrograph showing variable sized cavernous channels distended with proteinaceous material. Lymphoid follicles are interspersed within the septa (H and E, x100). (b) Higher magnification showing the lymphatic channels lined by flattened endothelial cells (H and E, x200)
a b
Bansal, et al.: Mesenteric lymphangioma in a pregnant woman
46Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1 47 Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 146Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1 47 Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1
cystic spaces [Figure 2b]. No attachment with the intestinal wall was seen. Multiple small lymph nodes were also isolated from the vicinity of the mass.
Microscopic examination showed a tumor composed of variable sized, interconnecting and cavernous channels separated by fibrous stroma and fat. Eosinophilic, proteinaceous material was noted in the lumen of these cystic spaces [Figure 3a]. A large number of lymphoid follicles and aggregates were dispersed in the stroma [Figure 3b]. Tumor was confined to the mesentery and not involving the adjacent small intestine. Sections from small intestine were essentially unremarkable. Four lymph nodes isolated showed sinusoidal dilatation.
Immunohistochemical staining with CD31 and CD34 highlighted the flat endothelial lining of the lymphatic channels [Figure 4a and b].
Final diagnosis of mesenteric cavernous lymphangioma was rendered. The post operative period was uneventful with the patient being discharged in a stable condition after 7 days.
DISCUSSION
Lymphangioma is a rare benign mass‑forming entity characterized by numerous thin‑walled lymphatic spaces. Although it can be encountered at any age, it usually manifests in the first few years
of life.[1] These are believed to arise from congenital malformation of lymphatic vessels leading to their sequestration during the embryonic period.[1‑3] However, other possible causes described are trauma, inflammation, surgery or radiation.[4,5] Majority of cases are seen in the head and neck region (75%) followed by axilla (25%). Other sites like abdominal or mediastinal cavity are rare, accounting for approximately 5% of lymphangiomas. [2] Among these, lymphangiomas of the small‑bowel mesentery have been described in less than 1% of cases.[1] Thus, the present case of a mesenteric lymphangioma in an adult female is quite rare.
Lymphangiomas are classified into three histologic types: Capillary (simple), cavernous, and cystic.[1] The capillary (simple) type usually originates in the skin and consists of uniform small thin‑walled lymphatic spaces. The cavernous type is composed of various sizes of dilated lymphatic spaces associated with lymphoid stroma and shows a connection with the adjacent normal lymphatic spaces. The cystic type consists of dilated lymphatic spaces of various sizes associated with collagen and smooth‑muscle bundles in the stroma but lacks connection to the adjacent normal lymphatic spaces. The present case was of cavernous type characterized by variable sized dilated lymphatic spaces having lymphoid infiltrate in the stroma.
Mesenteric lymphangiomas can remain asymptomatic or present with abdominal pain, vomiting, and constipation.[6] This can result in a diagnostic dilemma as these symptoms are common to many diseases of gastrointestinal tract. However, imaging modalities like ultrasonography, CT and MRI are useful tools for a proper diagnosis as was seen in our patient.[1,2,7] These tests are also used to estimate the size of the tumor and its infiltration into the surrounding
ba
ba
baba

Bansal, et al.: Mesenteric lymphangioma in a pregnant woman
48Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1 PB Oncology, Gastroenterology and Hepatology Reports| Jan-Jun 2015 | Vol 4 | Issue 1
tissues. Some diseases can be confused on imaging with mesenteric lymphangioma; these include hemangioma, cystic pancreatic tumor, gastrointestinal stromal tumor (GIST) and lymphangiosarcoma.
Although mesenteric lymphangioma is a benign lesion, it often has life‑threatening complications such as secondary infection, rupture with hemorrhage and volvulus or intestinal obstruction.[1,2,8] Surgical excision is the treatment of choice and in some instances extended surgery may be required for complete excision of the mass and to prevent recurrences.[9] In the present case also, a part of small intestine was excised as the tumor was in its close proximity. The only medication known to be effective against lymphangioma is OK432, a sclerotherapeutic agent consisting of an injectable, lyophilized incubation mixture of group A Streptococcus pyogenes.[10] The tumor can be reduced in size by injecting OK432 into the cysts, and may also be useful in cases with difficult complete resections. In a series of patients of lymphangiomas, OK432 was used for reduction of the mass with minimal side effects and favorable outcome.[11]
The coexistence of mesenteric lymphangiomas with pregnancy is very rare and to the best of our knowledge only three cases have been reported in English literature, all of whom had a favorable outcome. The clinical and management details of the cases are summarized in Table 1.[12‑14]
CONCLUSION
Mesenteric lymphangioma in adults is a rare disease which may remain asymptomatic or present with life‑threatening complications. Preoperative diagnostic tools are ultrasound and abdominal CT or MRI. Mesenteric lymphangioma should be considered in the
differential diagnoses of patients found to have intra‑abdominal cystic masses on imaging. Complete surgical resection is the ideal modality of treatment and definitive diagnosis is confirmed by histopathology.
REFERENCES1. Chen CW, Hsu SD, Lin CH, Cheng MF, Yu JC. Cystic lymphangioma of
the jejunal mesentery in an adult: A case report. World J Gastroenterol 2005;11:5084‑6.
2. Jang JH, Lee SL, Ku YM, An CH, Chang ED. Small bowel volvulus induced by mesenteric lymphangioma in an adult: A case report. Korean J Radiol 2009;10:319‑22.
3. Campbell WJ, Irwin ST, Biggart JD. Benign lymphangioma of the jejunal mesentery: An unusual cause of small bowel obstruction. Gut 1991;32:1568.
4. Hardin WJ, Hardy JD. Mesenteric cysts. Am J Surg 1970;119:640‑5.5. Roisman I, Manny J, Fields S, Shiloni E.Intra‑abdominal lymphangioma.
Br J Surg 1989;76:485‑9.6. Allen JG, Riall TS, Cameron JL, Askin FB, Hruban RH, Campbell KA.
Abdominal lymphangiomas in adults. J Gastrointest Surg 2006;10:746‑51.
7. Pui MH, Li ZP, Chen W, Chen JH. Lymphangioma: Imaging diagnosis. Australas Radiol 1997;41:324‑8.
8. Chung JC, Song OP. Cystic lymphangioma of the jejunal mesentery presenting with acute abdomen in an adult. Can J Surg 2009;52:E286‑8.
9. Losanoff JE, Kjossev KT. Mesenteric cystic lymphangioma: Unusual cause of intra‑abdominal catastrophe in an adult. Int J Clin Pract 2005;59:986‑7.
10. Tokuhara K, Hamada Y, Watanabe K, Tanano A, Takada K, Sato M, et al. A case of huge mesenteric lymphangioma managed by laparoscopy‑assisted subtotal resection with sclerosing therapy. JSPS 2003;39:90‑5.
11. Rebuffini E, Zuccarino L, Grecchi E, Carinci F, Merulla VE.Picibanil (OK‑432) in the treatment of head and neck lymphangiomas in children. Dent Res J (Isfahan) 2012;9 (Suppl 2) :S192‑6.
12. O’driscoll RG, Salerno JG, Quartrell AC, Fletcher HS. A mesenteric cyst in pregnancy. Am J ObstetGynecol 1977;129:588‑90.
13. Cipriano L, Palazzetti PL, Alò P, Serpieri DE, Torcia F, Pachì A. Abdominal cystic lymphangioma in a woman at 14 weeks’ gestation: Case report. Eur J GynaecolOncol 2000;21:391‑2.
14. Torashima Y, Yamaguchi J, Taniguchi K, Fujioka H, Shimokawa I, Izawa K, et al. Surgery for ileal mesenteric lymphangioma during pregnancy: Case report and review of the literature. J Gastrointest Surg 2004;8:616‑20.
Table 1: Details of previously reported cases of mesenteric lymphangioma in pregnant women
Case Year Age (years)
Gestational age
(weaks)
Lesion size (cm)
Treatment
1 1977 31 8 20 Tumorectomy2 2000 34 14 35 Intestinal resection3 2004 31 25 15 Intestinal resection4 Present
case23 8 15 Intestinal resection
How to cite this article: Bansal A, Siraj F, Grover SB, Bhatnagar A, Saxena S. Mesenteric lymphangioma:Arareintraabdominalfindingin a pregnant woman. Onc Gas Hep Rep 2015;4:46‑8.Source of Support: Nil, Conflict of Interest: None declared.
Top Related