







Languages
Pages
Legal

KEMENTERIAN PERHUBUNGANDIREKTORAT JENDERAL PERHUBUNGAN UDARA
PERATURAN DIREKTUR JENDERAL PERHUBUNGAN UDARA
NOMOR : KP 250 TAHUN 2017
TENTANG
PETUNJUK TEKNIS
PERATURAN KESELAMATAN PENERBANGAN SIPIL BAGIAN 67-01(STAFF INSTRUCTION PART 67-01) SUB BAGIAN I TENTANG
PROSEDUR PEMERIKSAAN KESEHATAN PENERBANGAN
(AVIATION MEDICAL EXAMINATION PROCEDURES}
DENGAN RAHMAT TUHAN YANG MAHA ESA
DIREKTUR JENDERAL PERHUBUNGAN UDARA,
Menimbang : a. bahwa dalam Peraturan Menteri Perhubungan NomorPM 69 Tahun 2017 tentang Peraturan Keselamatan
Penerbangan Sipil Bagian 67 (Civil Aviation SafetyRegulation Part 67) Tentang Sertifikasi dan Standar
Kesehatan Penerbangan (Medical Standard and
Certification) telah diatur mengenai pengujian kesehatanpersonel penerbangan;
b. bahwa dalam rangka memberikan panduan bagipenyelenggaraan pengujian kesehatan personelkesehatan perlu disusun suatu petunjuk teknis;
c. bahwa berdasarkan pertimbangan sebagaimanadimaksud pada butir a dan b, perlu menetapkanPeraturan Direktur Jenderal Perhubungan Udara
tentang Petunjuk Teknis Peraturan Keselamatan
Penerbangan Sipil Bagian 67-01 (Staff Instruction Part67-01) Volume I tentang Prosedur Pemeriksaan
Kesehatan Penerbangan (Aviation Medical ExaminationProcedures);
Mengingat : 1. Undang-Undang Republik Indonesia Nomor 1 Tahun
2009 tentang Penerbangan (Lembaran Negara RepublikIndonesia Tahun 2009 Nomor 1, Tambahan Lembaran
Negara Republik Indonesia Nomor 4956);
2. Peraturan Presiden Nomor 7 Tahun 2015 tentangOrganisasi Kementerian Negara (Lembaran NegaraRepublik IndonesiaTahun 2015 Nomor 5);
3. Peraturan Presiden Nomor 40 Tahun 2015 tentangKementrian Perhubungan (Lembaran Negara RepublikIndonesia Tahun 2015 Nomor 75);
4. Peraturan Menteri Perhubungan Nomor PM 1 Tahun
2014 Tentang Peraturan Keselamatan PenerbanganSipil Bagian 69 (Civil Aviation Safety Regulation Part 69)Tentang Lisensi, Rating, Pelatihan dan KecakapanPersonel Navigasi Penerbangan;
5. Peraturan Menteri Perhubungan Nomor PM 189 Tahun
2015 tentang Organisasi dan Tata Kerja Kementerian
Perhubungan (Berita Negara Republik Indonesia Tahun2015 Nomor 1844;
6. Peraturan Menteri Perhubungan Nomor PM 75 Tahun
2017 Tentang Peraturan Keselamatan PenerbanganSipil Bagian 65 (Civil Aviation Safety Regulation Part 65)Tentang Sertifikasi Ahli Perawatan Pesawat Udara
(Licensing ofAircraft Maintenance Engineer);7. Peraturan Menteri Perhubungan Nomor PM 59 Tahun
2017 Tentang Perubahan Kedua Atas Peraturan Menteri
Perhubungan Nomor KM 16 Tahun 2010 TentangPeraturan Keselamatan Penerbangan Sipil (PKPS)Bagian 63 Tentang Persyaratan Personel Pesawat Udara
Selain Penerbangan dan Personel Penunjang OperasiPesawat Udara;
8. Peraturan Menteri Perhubungan Nomor PM 50 Tahun
2016 Tentang Perubahan Keempat atas KeputusanMenteri Perhubungan Nomor KM 42 Tahun 2001
tentang Sertifikasi Penerbang dan Instruktur Terbang;
9. Peraturan Menteri Perhubungan Nomor PM 69 Tahun
2017 tentang Peraturan Keselamatan Penerbangan Sipil
Bagian 67 (Civil Aviation Safety Regulation Part 67)
Tentang Sertifikasi dan Standar Kesehatan
Penerbangan (Medical Standard and Certification)
MEMUTUSKAN
Menetapkan : PERATURAN DIREKTUR JENDERAL PERHUBUNGAN
UDARA TENTANG PETUNJUK TEKNIS PERATURAN
KESELAMATAN PENERBANGAN SIPIL BAGIAN 67-01
(STAFF INSTRUCTION PART 67-01) SUB BAGIAN I
TENTANG PROSEDUR PEMERIKSAAN KESEHATAN
PENERBANGAN (AVIATION MEDICAL EXAMINATION
PROCEDURES).
Pasal 1
Memberlakukan Petunjuk Teknis Peraturan Keselamatan
Penerbangan Sipil Bagian 67-01 (Staff Instruction Part 67-
01) Sub Bagian I Tentang Prosedur Pemeriksaan Kesehatan
Penerbangan (Aviation Medical Examination Procedures)
sebagaimana tercantum dalam Lampiran yang merupakanbagian tak terpisahkan dari Peraturan ini.
Pasal 2
Sejak berlakunya peraturan ini, BAB IV : Human Resources
Development For Aviation Medical Inspector pada Lampiran
Peraturan Direktur Jenderal Perhubungan Udara Nomor KP
620 Tahun 2015 Tentang Petunjuk Teknis HRD - 01.1
(Staff Instruction HRD-01.1) Pengembangan Sumber Daya
Manusia Personel Direktorat Kelaikan Udara dan
Pengoperasian Pesawat Udara dan Peraturan Direktur
Jenderal Perhubungan Udara Nomor KP 572 Tahun 2015
Tahun 2013 tentang Petunjuk Pelaksanaan Peraturan
Menteri Perhubungan Nomor 8 Tahun 2015 Tentang
Peraturan Keselamatan Penerbangan Sipil Bagian TentangStandar Kesehatan dan Sertifikasi Personel Penerbangandinyatakan tidak berlaku.
Pasal 3
Direktur Navigasi Penerbangan dan Direktur Kelaikudaraan
dan Pengoperasian Pesawat Udara mengawasi PelaksanaanPeraturan ini.
Pasal 4
Peraturan ini mulai berlaku sejak tanggal ditetapkan.
Ditetapkan : Jakarta
Pada tanggal : 25 SEPTEMBER 2017
DIREKTUR JENDERAL PERHUBUNGAN UDARA
ttd
Dr. Ir. AGUS SANTOSO, M.Sc
Salinan sesuai aslinyaKEPALA BAGIAN HUKUM
^^MUU^ENDAH PURNAMA SART
Pembina /(IV/a)NIP. 19680704 199503 2 001
LAMPIRAN PERATURAN DIREKTUR JENDERAL PERHUBUNGAN UDARANOMOR : KP 250 Tahun 2017TANGGAL : 25 September 2017
STAFF INSTRUCTION
SI 67-01
Aviation Medical Examination Procedures
Sub Part I
Amandemen : 0
Tanggal : Juli 2017
REPUBLIC OF INDONESIA - MINISTRY OF TRANSPORTATIONSDIRECTORATE GENERAL OF CIVIL AVIATION
JAKARTA - INDONESIA
PURPOSE
REFERENCES
CANCELLATION
AMENDMENT
FOREWORD
This Staff Instruction prescribesresponsibilities, policies, and procedures tobeused by the Directorate of Airworthiness andAircraft Operations (DAAO) for the certification,licensing, technical administration, andsurveillance of organizations and individualismaccordance with CASR part 61 and part 63.This Staff Instruction may be made available tothe public so that they may better understandthe authority and responsibility of the DAAO.
This Staff Instruction is instructions only andshould beused in accordance with theapplicable regulations.
SI HRD-01.1 Amendment 2 date October 2015Chapter IV is canceled
Director General Regulation Number KP 5722015 on Staff Instruction of CASR 67 NumberPM 8 Year 2015 on Medical ExaminationStandar and Certification is canceled.
Amendment of this Staff Instruction will beapproved by The Director General of CivilAviation.
DIRECTOR GENERAL OF CIVILAVIATION
ttd
Dr. Ir. AGUS SANTOSO, M.Sc
Salinan sesuai aslinyaKEPALA BAGIAN HUKUM
_
ENDAH PURNAMA SARI
Pembina /(IV/a)NIP.P. 19680704 199503 2 001
SI 67-01 AVIATION MEDICAL EXAMINER PROCEDURES
SUB PART I
RECORD OF AMENDMENTS
NUMBERDATE
ENTEREDBY NUMBER
DATE
ENTEREDBY
Original 20 July 2017
TABLE OF CONTENT
FOREWORD 2
CHAPTER I. INTRODUCTION 6
1. The Chicago Convention 5
2. Standards and Recommended Practices are defined as follows: 63. Purpose g
CHAPTER II. PERSONNEL LICENSING SYSTEM 71. General 7
2. The conceptoflicensing 7
3. Different type oflicenses g
4. Issuance ofthe license or certificate g
5. Currency oflicenses g
CHAPTER III. PERSONNEL LICENSING LEGISLATION 101. Primary Legislation 10
2. International and National Regulations 103. Explanatory Documents H
CHAPTER IV. GENERAL PROVISIONS 12
1. MEDICAL PERSONNEL 12A. Chief Medical Officer (CMO) 12B. Aviation Medical Assessor (AMA) 13C. Aviation Medical Examiner (AME) 14D. Training For AMEs 152. Medical Board 17
CHAPTER V. AVIATION MEDICAL CENTER lg1. Aviation Medical Center igA. AMC Organization Responsibility lgB. Equipment Requirements lg2. Medical in confidenceity 20
CHAPTER VI. MEDICAL ASSESSMENTS 211. Venue 91
2. Authority 91
3. Medical Assessment Procedure 21A. Verification ofdeclaration 21B. Additional Medical Assessment 21C. Aeromedical Disposition 22
D- Denial ZZ22E. Deferal 23
CHAPTER VII. RECORDKEEPING 24
1. General 24
2. Forms 24
3. Explanatory Pamphlets 24
4. Documentation & Records 24
5. Maintenance of Training Records for Technical Staff 25
6. Content and Integrity of Records 25
A. Completeness 25
B. Integrity 25
C. Easy access for authorized personnel 25
7. Organization of Records 25
A. Filing/ File Handling Procedure 26
B. File Register 26
C. Filling system 26
D. Medical Record Officer 26
E. Contents of the File/Documents in the File 27
F. Archiving of Records 27
G. Instructions to Work on the File &Job 27
H. Safe Keeping Files 28
I. Medical Record Files 28
J. Papers in File &Their Maintenance 28
K. Library and Reference Documentation 29
8. Movement ofmedical files and medical assessment procedure 29Chapter VIII. LIST OF APPLICABLE FORM 31
Appendix A. TRAINING SUBJECT FOR BASIC TRAINING IN AVIATION MEDICINE 321. Aviation physiology 32
2. Clinical aviation medicine 323. Public Health 32
4. Regulatory medicine 33
5. Medical Assessment Procedure for Class 2 and Class 3 33
CHAPTER I. INTRODUCTION
1. The Chicago Convention
The convention on International Civil Aviation, which was signed inChicago on 7 December 1944, includes several articles which call foradoption of international regulations in all fields where uniformityfacilitates and improves air navigation. These regulations, known asStandards and Recommended Practices (SARPs) have been promulgated inAnnexes to the Convention which are amended from time to time whennecessary. Each Annex deals with a specific aspect of international civilaviation. Aviation medicine is included mainly in Annex 1 (PersonnelLicensing) and to some degree in Annex 2 (Rules of the Air), Annex 6(Operation of Aircraft) and Annex 9 (Facilitation). Issues involving Annex9, preparedness planning for a communicable disease of public healthconcern, are not considered in this manual.
2. Standards and Recommended Practices are defined as follows:
Standard - Any specification for physical characteristics, configuration,material, performance, personnel or procedure, the uniform application ofwhich is recognized as necessary for the safety or regularity ofinternational air navigation, and to which Contracting States will conformin accordance with the Convention.
Recommended Practice - Any specification for physical characteristicsconfiguration, material, performance, personnel or procedure, the uniformapplication of which is recognized as desirable in the interest of safetyregularity or efficiency of international air navigation, and to whichContracting States will endeavour to conform in accordance with theconvention. Although the purpose of SARPs is to provide provisions onlyfor international air navigation, they have greatly influenced nationalregulations governing domestic aviation in most Contracting States. ICAOalso originates guidance material which is intended to assist States in theimplementation of SARPs, but places no regulatory responsibility uponStates for compliance.
3. Purpose
The purpose of this SI is to prescribe personnel licensing proceduresCompliance by DGCA staff will ensure that all activities are efficient andremain within the confines of the relevant legislation. It is expected thatthis will be achieved if all staff fully comply with the procedures asdetailed in this SI. Full compliance with the SI procedures is thereforemandatory.
CHAPTER II. PERSONNEL LICENSING SYSTEM
1. General
Civil aviation includes different types ofoperations which for convenience,can be divided into three major categories.
Commercial air transport (airlines) - This category includes all operationsconducted with large and sophisticated aircraft which used to be pilotedby several crew members.In recent years the need for more efficiency hasproduced some dramatic technological changes which directly involveflight personnel. On modern aeroplanes, computers are handling thesystems and the pilot is becoming more and more of a systems managerand decision maker rather than a control operator.
Aerial work and small air transport - All professional flying except airlinesis included in this category. Typical operations are flying instruction, cropspraying, aerial surveying, small commuter operations, air taxi andcorporate flying. This category has not faced such important changes ashas airline transport. It must be noted that helicopters now perform asignificant part of these operations.
Private air transport and pleasure flight-The majority of the world's pilotsbelong to this category. The operations are not conducted forremuneration and generally involve small aircraft. In this category, gliderpilots form an important subgroup. During the last two decades, a newdimension has been added to this category with the fast-growingpopularity of the ultra light aircraft. The Aviation Medical Examiner, whenmaking an assessment, must be familiar with the various operatingenvironments.
2. The concept of licensing
DGCA have recognized the necessity to check the competency of personnelwho perform activities which, unless performed properly, could jeopardizeaviation safety. The recognition of this competency was generally made byissuing a license. This concept has remained valid throughout the years,and the whole of Annex 1 may be considered as an evolution of this basicidea.
The personnel licensing system on the following principles:
a. The license is the authorization which allows the holder to performspecific activities, which otherwise would be prohibited.
b. Alicense is issued bya DGCA when the applicant has demonstrated anacceptable degree of competency. The right to issue a license isresponsible to DGCA either directly or through a body with delegatedauthority.
c. There are different types of licenses. Each one grants specific privilegesto the holder. Ratings can be added to the license to extend the basicprivileges.
3. Different type of licenses
a. Pilot's Licenses
License is an authorization for a pilot issued by the DGCA to personswho meet the age, knowledge, skill and experience requirements ofCASR 61.
b. Licenses for flight crew members other than pilot.
License is authorization for a flight crew other than pilot issued by theDGCA to persons who meet the age, knowledge, skill and experiencerequirements of CASR 63.
c. License or certificate for Personnel Other Than Plight CrewMembers
1) Air traffic controllers.License is an authorization for an air traffic controller issued bythe DGCA to persons who meet the age, knowledge, skill andexperience requirements of CASR 69.
2) Flight Attendant.Certificate is a qualification for a flight attendant issued by theDGCA to persons who meet the age, knowledge, skill andexperience requirements of CASR 63.
d. Ratings
Rating isan authorization entered on or associated with a license andforming part thereof, stating special conditions, privileges or limitationspertaining to such license.
4. Issuance of the license or certificate
An applicant who seeks a Personnel license/cerficate must complete amulti-step process, which can be divided into three major parts:prerequisites, training and demonstration of competency. If a Licenses isassociated with a rating (usually is) Initial Issuance of that License shallbe coupled with issuance of at least one Rating which shall be endorsedon the License on the initial Issue of such License.
a. Prerequisites
Age - A minimum age is specified for each license.
Experience - Aminimum level of experience depending on the licenseis required for all personnel to be licensed. The unit of measurement ofexperience is flight hours for flight crew, on the job training (OJT)hours for Air Traffic Controllers (ATC) and years of duty for groundpersonnel.
Medical fitness- Most of the certificate require compliance with medicalfitness standards. Complete guidance on this matter is provided in thismanual.
b. Training
Training is obviously one of the most important parts of the licensingsystem. For several licenses, an applicant may choose to take anapproved training course instead of a regular course and thus beeligible for reduced experience requirements. It is expected that evenmore emphasis will be placed on training in the future.
c. Demonstration of competency
Each license has its specific skill and knowledge requirements, andeach applicant must demonstrate compliance with the requirementspursuant to the license he seeks. DGCA use a written examination,oral and a practical test to check the competency ofan applicant.
5. Currency of licenses
As outlined above, basically there are two different types of licensespracticed worldwide, can be found. Some Indonesia licensing system isexpiry type has a period of currency which is limited to a defined period.At each renewal, the holder must give evidence ofhis competency and hismedical fitness. Competency is usually judged by considering the recentflight experience and sometimes by an examination. The other type oflicense (continuous type) is not limited to a defined period of currency. Theholder is allowed to exercise license privileges as long as he holds acurrent Medical Assessment and complies with the regulations detailingthe actions necessary to ensure maintenance ofcompetency.
CHAPTER III. PERSONNEL LICENSING LEGISLATION
1. Primary Legislation
The Convention on International Civil Aviation, signed in Chicago in 1944,is the basis upon which all international civil aviation is regulated. As asignatory to the Convention, Indonesia has an obligation to comply, as faras it is possible, with the international standards of this Convention.
The Convention may be thought of as an international "Civil Aviation Act"and it obligates each signatory state to enact its own legislation along thelines of the Convention.
The Law of the Republic of Indonesia Number 01 Year 2009 is, in effectIndonesia's "Civil Aviation Act" and, as such, is in compliance with theConvention. Article 18, reproduced here in full, provides for thecompetency of aviation personnel as follows:
Article 18
1) All aviation personnel shall have a certificate of competency.2) The certificate of competency mentioned in section (1) shall be
obtained through education and training.3) The requirements and procedures for obtaining a certificate of
competency mentioned in section (1) and section (2) shall be furtherregulated by government.
In summary, Article 18 says that aviation personnel must hold a'certificate of competency' which must be gained through education andtraining. In this context a certificate of competency can be a license,certificate, authorization or approval. Furthermore, the procedures forgaining such a license, certificate, authorization or approval shall be inaccordance with regulations, i.e. Civil Aviation Safety Regulations.
2. International and National Regulations
The Annex's to the Convention provide the standards with which nationalregulations should conform. Annex 1 prescribes the internationalstandards and recommended practices for personnel licensing. In respectof personnel licensing, Annex 1 can be thought of as "internationalregulations".
The further regulations prescribed by Article 18 are Civil Aviation SafetyRegulations (CASR). The national regulations for personnel licensing inIndonesia are CASR.
Part 61 Licensing of pilots and flight instructors.
Part 63 Licensing flight crew members other than pilot, flightoperation officers and certificate of flight attendant
Part 65 Licensing of Aircraft Maintenance Engineer
Part 67 Medical standards and certification.
10
Part 69 Air traffic services personnel licensing, rating, training andproficiency requirements.
3. Explanatory Documents
Annex'sto the Convention are supported by other documents containingexplanatory material. In respect of personnel licensing and aviationmedical, these include:
ICAO Doc 8984
ICAO Doc 9379
Manual of Civil Aviation Medicine
Manual of procedures for Establishment andManagement of a State's Personnel LicensingSystem.
In a similar way, state's issue explanatory material that offers guidance toassist their aviation industry's to comply with national regulations. InIndonesia, these publications are Advisory Circulars (AC's). Therelationship between international and national legislation is shown in theTable 1 below.
Table 1
INTERNATIONAL NATIONAL
Convention on InternationalCivil Aviation
Annex's to the Convention
ICAO Documents
The Law of the Republic ofIndonesia Number 01 Year2009
Civil Aviation Safety Regulations
Advisory Circulars and StaffInstructions
Table 1 showing relationship of international and national legislation.
11
CHAPTER IV. GENERAL PROVISIONS
1. MEDICAL PERSONNEL
A. Chief Medical Officer (CMO)
1) General
The Chief Medical Officer of the DGCA to be the 'accountable'responsible for national aeromedical safety.
Head of Aviation Medical Center as Chief Medical Officer
Responsible to:
Director General of Civil Aviation.
2) Qualifications & Experience
1) Have extensive experience in regulatory civil aviation medicine aswell as a thorough knowledge of medical requirements andmedical best practice
2) Have leadership qualities3) Have administrative skills and the ability to make decisions
concerning medical fitness of the applicants
3) Functions, Duties & Responsibilities
1) Responsible for using this aeromedical data, along with relevantinformation from the wider medical literature, to devise andimplement appropriate aeromedical policies.
2) Recommendation for Adoption of Annex 1 Standards for the Issueof Medical Assessments.
3) Developing 8b Amending of Medical Procedure.
4) Safe keeping of Medical Records 8b Maintaining confidentiality ofthe same.
5) Convening 8b conducting Medical Board to evaluate 8b establishAccredited Medical Conclusions.
6) Conduct of evaluations of the issuance requirements of individualin terms of medical investigations reports as per the establishedprocedure.
7) Recommendation of Appointment of AMEs.8) Recommendation for Withdrawal ofAuthority from AMEs9) Recommendation of Appointment of AMAs.10) Recommendation for Withdrawal ofAuthority from AMAs.11) Recommendation of Hospitals 8b Laboratories for Clinical
Investigations.12) Recommend to the DGCA for the purchase of equipment's,
periodicals, medical journals, medical books 8b ICAO Material forreference of Aviation Medical Examiners.
13) Recommend to the DGCA suspension, cancellation 8breinstatement of medical certificate.
12
14) Recommend the renewal of each AME at the end of tenure ofpresent arrangement after evaluating or AME doesn'tsatisfactorily complete the renewal requirement
B. Aviation Medical Assessor (AMA)
DGCA use the services of Aviation Medical Assessor to evaluate reportssubmitted to the DGCA by Aviation Medical Examiners.
Aviation Medical Assessor as a supervisor for the designated AviationMedical Examiners has basic/advanced training in the specialty ofaviation medicine and extensive experience in regulatory and clinical civilaviation medicine.
Evaluating medical reports submitted to the DGCA and making finalassessments in deferal and appeal cases, the Aviation Medical Assessorwill be in charge of Accredited Medical Conclusions.
An important duty of the Aviation Medical Assessor is the safeguarding ofmedical in confidenceity, although pertinent medical information may bepresented by the Aviation Medical Assessor to DGCA when justified byoperational concerns or when an Accredited Medical Conclusion is sought.
1) Qualifications & Experience
1) Minimum 5 (five) years experience as DGCA Aviation MedicalExaminer.
2) Have satisfactory completion training for Personnel LicensingProcedures
2) Functions, Duties &Responsibilities - Aviation Medical Assessor
1) Evaluation of Medical Asessment Reports, submitted by AMEs asper the applicable Medical Standards 8b Recommended Practices,8b determination of medical fitness of license holders for theIssue/ Renewal of Licenses.
2) Recommendation ofTraining requirements ofAMEs.3) Review and evaluate Medical Asessment Reports issued by
Aviation Medical Examiners and if there is any inconsistence,withdraw the Medical Certificate already issued by AME.
4) Submit pertinent Medical information to DGCA when justified byoperational concerns.
5) Evaluating the renewal requirements of individual in terms ofmedical investigations (Checks / Tests) and assessments carriedout by Aviation Medical Examiners as per the establishedprocedure.
6) Evaluate and discuss with the Aviation Medical Examiners thecomposition of the Medical Board of any abnormalities andborderline cases for the:
a) Initial Medical assessments ofa license applicant,b) Medical assessment of a person whose license had been
suspended on medical grounds 8b qualifies forreinstatement.
c) Medical assessments of a holder of a lapsed license whomay not qualify for a routing Medical assessment due tothe period of lapse.
13
d) Medical assessment of a holder of a lapsed license whohad been grounded for indiscipline/ incompetence / courtcase.
7) In consultation with the Aviation Medical Examiners, devisemethods to ensure confidentiality in pathological examinationsrecord safekeeping.
8) Coordinate and conduct periodic meetings with AMEs.9) Supervision of the medical examination facility, and suggest to
make improvement of equipment, procedures and etc.10) Establish a working relationship with the relevant Aviation
Medical Examiners if one or several medical conditions of alicense holder are found to decrease medical fitness over a period,and notice to DGCA.
11) Provide further details/clarifications/explanations on medicalassessment conducted to the DGCA on own initiation or onrequest as 8b when necessary.
12) Attend local or overseas training programs or familiarization visitsorganized by DGCA.
13) Conduct minimum of one evaluation/competency assessment oneach Designated Aviation Medical Examiner Representative(DAMER) once every one year prior to renewal of authorizationand ensure that the DAMER meet applicable standards of goodmedical practice and aero medical risk assessment.
14) Maintain surveillance on all DAMER whenever possible while theyconduct medical assessment not less than one inspection/surveillance per year per DAMER.
15) Submit surveillance plan to DGCA before the beginning of theyear for approval.
C. Aviation Medical Examiner (AME)
1) General
The DGCA has medical personnel or designated, in sufficient numbers,Aviation Medical Examiners, within Indonesia, qualified and fullyregistered medical practitioner permit in the practice of medicine.
Aviation Medical Examiners will conduct detailed medical assessmentsand refer to the designated Medical Examination Facility to conductlaboratory tests.
Aviation Medical Examiner shall coordinate the results of theexamination and submit a signed report to the DGCA with appropriatecomments and recommendation.
2) Qualification of Aviation Medical Examiners.
1) Medical doctor degree or Aviation Medical Specialist2) Have satisfactory completion of Flight Surgeon Training for
medical doctor degree.3) Have satisfactory completion Training of Aviation Medical
Examinations Procedure.
14
3) Functions, Duties & Responsibilities - Aviation Medical Examiner
1) Conduct medical assessments for the issue and renewal of amedical certificate of all categories in compliance with the CASRof Indonesia and Requirements issued by the DGCA.
2) Conduct medical assessments in accordance with SI 67-02Aviation Medical Examination Manual.
3) In consultation with and approval of the DGCA, AME shall takenecessary steps to seek accredited medical conclusion as andwhen necessary.
4) As a member of Medical Board.5) Review / evaluate results of previous medical assessments of
personnel licenses holders and monitor and analyze the medicalcondition of license holders.
6) Propose development of new procedures and practices, whichcould be implemented in order to maintain highest standards andquality.
7) Recommend purchase of new equipment as and when necessary.8) Recommend purchase of periodicals, medical journals and
medical books for reference by the AMEs.9) Sign the Medical Certificate10) Submit Medical Assessment Report to AMA at the earliest
possible but not later than one week from the date of the medicalassessment.
11) Attend training Programs or familiarization visits offered bv theDGCA.
D. Training For AMEs
DGCA shall designate medical examiners, qualified in the practice ofmedicine, to conduct medical assessment of fitness of applicants for theissue or renewal of the licences or ratings specified in Chapters VI of thisStaff Instruction.
• Aviation Medical Examiners is designated to conduct Class 2 and 3medical assessment shall receive Basic Training in AviationMedicine or Flight Surgeon Training and demonstrated adequatecompetency in aviation medicine.
• Aviation Medical Examiners is designated to conduct Class 1, 2 and3 medical assessment shall receive Basic and Advance Training inAviation Medicince and demonstrated adequate competency inaviation medicine.
• Medical examiners shall have practical knowledge and experience ofthe conditions in which the holders of licences and ratings carrv outtheir duties. J
15
1) Basic Training in Aviation Medicine or Flight Surgeon Training.
Aviation Medical Examiners shall receive basic training in aviationmedicine at training organization recognized by DGCA. The trainingsubject shall include :
1. Aviation Physiology2. Clinical Aviation Medicine3. Public Health
4. Regulatory Medicine5. Class 2 and 3 Medical Assessment Procedures
The details of training subject described in Appendix A of this StaffInstruction.
In order to achieve competency, aviation medical examiner mustcomplete practical knowledge and experience including flightexperience and on the job training.
2) Advanced Training in Aviation Medicine
Advance training in aviation medicine will include training subject forclass 1 medical assessment procedure, to attend the advance trainingthe AME shall satisfactory completions of basic training and havemedical assessment experience at least 2 years.
3) Refresher Training in Aviation Medicine
The Aviation Medical Examiner should receive refresher classroomtraining every 60 months. Generally, refresher should contain a reviewof the training subject on basic and advance training along with adiscussions of any new requirements or procedures that have beenestablished.
The Aviation Medical Examiners may attend aviation medical seminarsor workshops to maintain their competency.
4) Evaluation of Aviation Medical Examiner
The medical assessments may be conduct by either DGCA AviationMedical Examiners or Designated Aviation Medical ExaminerRepresentatives (DAMER).
Staff Instructions 183-05 contain procedures for DAMERadministrations.
1) Letter of Designations.After the completion of Basic Training AME is required to conductpractical knowledge and experience found satisfactory by an AMA.
The AMA will evaluate medical examiner qualifications to ensurethe prospective medical examiner meet the qualificationrequirement as stated in paragraph 3(b) of this chapter.
After the prospective medical examiner meet the qualificationrequirement, AMA will conduct the Competency Test using AMCForm No. 67-05 that include :
16
• Demonstration of medical assessment preperation.• Demonstration of medical assessment
• Demonstration of medical assesment report submission
Letter of Designation may be issued by Director General if theprospective medical examiner passed the competency test.
2) Conditions for Renewal of Letter of Designation.a) At least Ten (10) Medical Examination per year.b) Participate on Medical Board.c) Recommended by AMA.
3) Record KeepingThe documents of AME shall be keep and maintain at AMC asfollow:
a) A copy of Medical Doctor Degree or Aviation MedicalSpecialist Diploma
b) A copy of basic or advance aviation medical trainingcertificate.
c) A copy of Aviation Medical Examination ProcedureTraining Certificate
d) AMC Form No. 67-05e) A Copy of Letter of Designation
2. Medical Board
Medical board will convened for a case of deferal, appeal from anapplicant or any case which considered necessary to be discussed.
The chief medical officers appoint the Medical Board which consist ofAME(s) and AMA(s). Regardless of the composition the number ofmember of Medical Board shall be an odd number and lead by an AMA.Chief medical officer may obtain external expertise or resources (e.g.Flight Operation Expert) to join the medical board if it is deemednecessary.
Result from medical board will be considered as an accredited medicalconclusion. It then may be used as a basis for:
• Issuing or denying medical certificate in accordance withaccredited medical conclusion.
• Recommendation to perform special medical test through theissuance of Letter of Authorization (LoA)
17
CHAPTER V. AVIATION MEDICAL CENTER
1. Aviation Medical Center
Aviation Medical Center (AMC) or Balai Kesehatan Penerbangan is theestablished facility by DGCA within its premises, for the proper conduct ofaviation medical assessments & safe keeping of relevant documents 8bapparatus used for the purpose, which is functioning as a fully-fledgedclinic.
Also Designation of Aviation Medical Examiners (AME) has been done fromtime to time starting from two practitioners, from well experiencedPhysicians in the practice of aviation medicine appointed by DGCA toconduct examinations to determine medical fitness of Aviation licenseholders. Such physicians duly empowered to act on behalfof the DGCA, 8bthey shall be known as the Aviation Medical Examiners (AME) of AviationMedical Center (AMC) of DGCA. Specialized tests are carried out indesignated hospitals and the investigations reviewed prior to issue oflicense.
In addition there is a Medical Assistant for record management and assistthe Aviation Medical Examiners Aviation Medical assessments.
A. AMC Organization Responsibility
The organization employer of designated to conduct the examination foraviation medical is responsible for the following:
1) The designated organizations shall conduct the medicalexamination in compliance with the aviation medical certificatefor aviation personnel, and under supervision of the DGCA.
2) The organization shall be maintaining a designated personalcurrency, proficiency and training as a person.
3) The organization providing the equipement element of the medicalassessment.
4) The designated organizations shall compile a summary report forall applicants who fail the test every 6 months. The report shouldbe submitted to the DGCA.
5) The managements or superior of the organizations may notinterfere or influence to the judgment of the examiners and maynot order the examiners to produce a false record.
B. Equipment Requirements
For the conduct of the medical assessment, AMC shall have adequatefacilities for performing the required examinations and possess thefollowing equipment prior to conducting any DGCA examinations.History or current findings may indicate a need for special evaluations.AMCs shall certify at the time of designation, re-designation, or uponrequest that they possess (and maintain as necessary) the equipmentspecified.
18
Aviation medical Center must becompleted equipment element ofmedical assessment, as follows:
1) Standard Snellen Test.
Types for visual acuity (both near and distant) and appropriateeye lane. Near Vision Acuity Test Card may be used for near andintermediate vision testing. Metal, opaque plastic, or cardboardocclude.
2) Eye Muscle Test-Light.May be a spot of light 0.5cm in diameter, a regular muscle-testlight, or an ophthalmoscope.
3) Maddox Rod.May be hand-type.
4) Horizontal Prism Bar.Risley or hand prism are acceptable alternatives.
5) Other vision test equipment that is acceptable as a replacementfor 1 through 4 above include any commercially available visualacuities and heterophobia testing devices.
6) Color Vision Test Apparatus.Pseudoisochromatic plates, American Optical Company (AOC)1965 edition; AOC-HRR, 2nd edition; Dvorine, 2nd edition:Ishihara, Concise 38-plate editions;
7) AWall Target consisting of a 50-inch square surface with a mattefinish (may be black felt or dull finish paper) and a 2-ram whitetest object (may be a pin) in a suitable handle of the same color asthe background.
8) Note: this is not necessary if an ME chooses the acceptable optionofperforming field ofvision testing by direct confrontation.
Standard physician diagnostic instruments and aids includingthose necessary to perform urine testing for albumin and glucoseand those to measure height and weight.
9) Electrocardiographic equipment.
Senior Examiners must have access to digital electrocardiographicequipment with electronic transmission capability.
10) Audiometric equipment.
All Examiners must have access to audiometric equipment or acapability of referring applicants to other medical facilities foraudiometric testing
19
2. Medical in confideneeity
Medical in confidenceity shall be respected at all times. The DGCA shallensure that all oral or written reports and electronically stored informationon medical matters of license holders/applicants are made available toAME 8b to AMA, in order to be used by the DGCA for completion of amedical assessment.
Examining a healthy person may seem an easy task but also a ratherfutile thing to do, for what can you expects to find where nothing iswrong? In reality the periodic examination of airmen is both difficult anddemanding, but may also be quite rewarding when performed withinterest, care and thoroughness. A license holder is legally obliged toundergo regular health examinations, performed by an AuthorisedAviation Medical Examiner (AME).The airman may appear to be in perfecthealth, and more often than not will he himself believe this to be the case.At the same time he may reasonably fear that if something is wrong afterall then this might cost him his medical certificate, i.e. his livelihood. Thissituation may lead the airman to feel nervous and tense at theexamination, but almost invariably he will try to present himself asperfectly healthy. Fortunately most examinations will confirm that he isindeed in good health and fit for flying. But even if he is experiencing amental or physical problem he may, consciously or subconsciouslyrepress it, and in either case the AME may not receive the usual help fromhis examinee to guide him towards the site of any problem. To find a signof early disease or malfunction under these circumstances takes skillexperience and the utmost thoroughness.
It is important that the aviation medical assessment is performed in a waythat encourages the airman to discuss freely and openly whateverproblems, medical or otherwise, he may have, but the situation is notideal for developing the usual doctor-patient relationship between AMEand airman. An airman is not a patient and so has little encouragement toconfide more than is required by the regulations. On the other hand theAME gains little without the airman's confidence as most information ofvalue is voluntary. There is no specific route for the AME to follow in orderto ensure an aviation medical assessment of quality, but some importantfactors are:
20
CHAPTER VI. MEDICAL ASSESSMENTS
1. Venue
Unless otherwise exempt by writing by the DGCA every Medicalassessments except certain laboratory tests conducted for the purpose ofissuance or renewal of Licenses shall be conducted at the Civil AviationMedical Center established &maintained within the DGCA premises
2. Authority
Conduct of Medical assessment for the issue of Medical Assessments shallbe only performed by AME who has been duly delegated the test &whoholds a valid authorization.
3. Medical Assessment Procedure
A. Verification of declarationAn applicant for a medical assessment must furnish adequate proof ofhis or her identity as a prerequisite for an assessment. Thedocumentation required to verify identity will vary from State to Stateand is particularly important when the medical examiner does notpersonally know the applicant. In case of a renewal, the currentlicence and last issued medical assessment report should be reviewedby the medical examiner at each examination.
The actual assessment commences with the identified applicantproviding the medical examiner with a declaration statement ofmedical facts concerning personal, familial and hereditary history. Areliable assessment requires that statement to be complete andaccurate, and the applicant should be advised that any false ormisleading information in the statement could have far-reachingconsequences. The Declaration Statement include in AMC Form No.67-01, Application For Aviations Medical Assesment.
Any false declaration will consequence that the Aviation MedicalExaminer will not conduct the medical assessment before theapplicant provide the correct declaration statements.
Any false declaration found after the medical certificate has beenissued, Directore General will issue a warning letter to the licenseholder and the medical may be withdrawed.
B. Additional Medical Assessment
Additional medical assessment is required for the following conditions:
1) ^ere the DGCA has reasonable doubt about the continuing fitnessof the holder of a medical certificate. Additional medical assessmentconduct in accordance with SI 67-02.
21
2) Class 1 Medical Assessments for Pilots over the Age of 60 years upto 65 years operating in Multi Crew Environment. AdditionalMedical Examination Procedure for Pilot over 60 years of Age aredescribed in DG Decree No. SKEP/30/II/2009 as amended by DGDecree No. KP 344 Year 2013.
C. Aeromedical Disposition
After reviewing the medical history and completing the medicalassesment in accordance with Part II of this Staff Instruction, theaviation medical examiner, either:
1) issue a Medical Certificate (AMC Form No. 67-03) if the applicant isfound fit in all respects;
2) deny the application if the applicant is found unfit; or3) defer the action to the DGCA if the applicant does not meet all the
medical criteria to be assessed as fit, but his or her condition is notconsidered by the aviation medical examiner to be detrimental toflight safety.
Whatever the outcome, AMC Form No. 67-02, Medical AssesmentReport should also be produced and sent to the DGCA for evaluationby the Aviation Medical Assessor (AMA) and for recording and auditingpurposes.
Audit is performed by randomly reviewed medical report submitted bymedical examiner. Upon finding of any discrepancies medical assessormay conduct further review on the result of medical assessment thatmay lead to the recommendation of reassessment of the applicant, orsuspension or revocation of the medical examiner authorization.
The reports are required to be evaluated by an aviation medicalassessor whenever an aeromedical decision needs to be made thataffects the medical fitness of the applicant, in addition, a sample ofother reports should be evaluated by the aviation medical assessor(s)for auditing purposes.
D. Denial
The Aviation Medical Examiner is therefore primarily responsible fordeciding whether or not an applicant is within the Requirements. Anyapplicant who presents for examination must be examined unless theimmediate history (epilepsy and psychosis for example) obviouslyprecludes any kind of certification. If full examination indicates that anapplicant does not clearly meet the requirements, the AME may advisehim of the area of concern and issue Denial Letter (AMC Form No.67-08) will be forwarded without delay to the applicant.
Ifan application for a medical assessment is found unfit, the applicantmay accept the decision or appeal the decision.
22
An appeal request should be addressed to the CMO, with suitablesupporting data. The CMO will then review the case, which could relyon expert opinion from medical examiner or by convening a medicalreview board (consisting of relevant specialists) to provide expertadvice.
Result of the review above shall then be assessed by Aviation MedicalAssessor, for the final aeromedical decision which will be then issuedby the CMO. who should have autonomy in making this decision.
E. Deferal
After conducting amedical assessments if the AME is not in oppositionto determine that one or more medical condition/s of the applicant donot confirm to standard specified in CASR 67 numerically orotherwise, AME shall defer the issue appropriate Medical Certificate.Inis decision shall be notified to the applicant.Any case deferred to the medical board must be reconsidered againstall applicable requirements appropriate to the class of assessment Iffurther investigation or opinion is required the applicant should beadvised of this need and how it may be achieved. On occasion it maybe necessary for the AMC to direct the applicant to a specific medicalspecialist for a further opinion. In all such cases relevantdocumentation must be provided to the specialist.
Upon completion of their review the medical board should make anassessment. In most cases the medical board will have sufficientadditional expertise and operational experience to make a decisionHowever, some cases require careful consideration of complex studies'lor example coronary angiograms In such cases it may beadvantageous for the DGCA to bring together several DGCA acceptedcardiologists in order to gain consensus concerning interpretation ofthis data. The assessments can then be demonstrated as having beengiven full consideration:
l\ Th6 Tr^1 d,ef?,Cien7 in relati0n t0 the operating environment;I) The ability, skill and experience of the applicant in the relevantoperating environment;
3) Aspecial medical test, ifappropriate; and4) The requirement for application of any limitations, conditions or
variations to the medical certificate and license. Where the issueol a certificate will require more than one limitation, condition orvariation, the additive and interactive effects upon flight safetvmust be considered by the AMC before a certificate can be issued
Medical board will then produce an accredited medical conclusion.
23
CHAPTER VII. RECORD KEEPING
1. General
Maintenance of records of an organization in a systematic manner is a keyto achieve highlevel of efficiency, regularity, productivity and transparencyof the work that it has performed. In a public enterprise such as theDGCA, records shall be maintained in a systematic manner not only toachieve the above objectives but also to keep track of the workperformed and also to take legal action of the persons/organizationsbeing regulated, whose duties and functions have bearing on either safetyor security.
Record system of DGCA has been developed with a view to achieving auniform record management procedure within the DGCA.
Record system is the definitive reference for all DGCA records systemprocedures All DGCA employees during the tenure of their official dutiesshall abide by the procedures explained in this procedure with regard tohandling and management of the DGCA records. Any deviation is possibleonly on a special approval from the Director General.
2. Forms
Form is a designed documentwhich facilitates the administrative functionof making application, processing the application, recording data andissuing the license.
3. Explanatory Pamphlets
An explanatory pamphlet is a document which provides an applicant withthe requirements for a particular license, and gives him /her reference toall pertinent approved documents. These pamphlets contain all thenecessary guidelines in one document without the need to refer to otherexplanatory documents. Because a pamphlet, as described above, is asmall and contain only material relevant to a particular license, it will beeasy to assimilate by the public and convenient to publish and amend bythe issuing authority. However, it is important to note that a pamphletgives a detailed explanation as to the requirements for a license and thenecessary administrative steps to facilitate easy application.
4. Documentation & Records
Each license holder should have a personal file on which is placed allcorrespondence, applications, assessments, examination results and alllicensing documentation. An indexregister system showing the file detailspurposes.
The record held by a DGCA licensing system included a medical registry ofcertificate, complemented by individual files which contained a summary
24
of all medical assessment action taken and all the personal records of theapplicant.
The record system is fully or partially paper based and secure forconfidential data. Such a purely manual system is adequate for DGCAwith a limited number of medical certificate. However, as the number ofactive certificate grows beyond a few thousand, a computerized systembecomes necessary either to complement or replace the paper-basedrecords
5. Maintenance of Training Records for Technical Staff
It is considered mandatory thatall PEL staff undergoes trainingprogrammes as per training plan and all records pertaining to individualtraining shall be recorded. Therefore each PEL Staff including AMA andAME (authorized to conduct licensing tasks should have a personal file onwhich contains all certificates received for training).
When trainings is conducted for PEL staff, printed copy of trainingmaterials, course notes& electronic copies will be forwarded to the actionofficer who handles the subject of "PEL Staff Training" and all documentsshould be filed.
6. Content and Integrity of Records
!£*££?* maintains records that support every licencing action takenbythe DGCA for each applicant or license holder. The main characteristics ofa record keeping system are:
A.Completeness
The records kept by each medical facility should be sufficient to providedocumentary evidence each medical assessment action and allow thereconstruct the history of each certificate of issued.
B.Integrity
It is important to maintain the integrity of records that is not removedor altered. This usually requires that each record entered in the file beproperly minute and that proper procedures exist to control that hasaccess to the files. This applies to both paper and computerized records.
C.Easy access for authorized personnel
The information contained in the medical records should be easilyaccessible to the staff of licensing section. This is a requirement whichconflicts with those necessary to maintain the integrity of the recordsand the proper compromise have to be made.
7. Organization of Records
The records held by the each medical facility maintained for each medicalrecord complemented by individual files which contained a summary ofmedical assessment action taken and all the personal records of theapplicant.
25
It is also important to maintain a backup system of the records to ensurecontinuity in case of a major disaster. When the records are computerizedit is easy to make backup thedata on a regular basis and to keep thebackup in an offsite storage that offers the required level of security forconfidential data. J
Nevertheless, it would be necessary to keep a backup of the essentialinformation such as medical certificate Registry, with the details of allmedical certificate issued.
A. Filing/ File Handling Procedure
Each certificate holder should have a personal file on which contains allcorrespondence, applications, examination results and all otherlicensing documentation.
B.File Register
Update the appropriate file register when creating a new file, enter thefile number, and subject of the file.
C. Filling system
All Action Officers are responsible for file handling.D. Medical Record Officer
Medical Record Officer is the person whom with the file is physicallykept under locked 8b key. H y y
Responsibilities of the Medical Record Officer:
1) Safe Keeping of the file with its contents properly numbered pagesand minute sheets in chorological order.
2) Medical Record Officer should be well worse and conversant withthe contents and records checklists etc.
3) Taking actions within the guidelines provided by the action officerthough the file pertaining to each and every subject Anydocuments and file are or any ambiguities shall be submittedimmediately to the immediate supervisor in- charge of the subject
4) This process of action shall be in a minute made on a designatedminute sheet as per guidance and instructions given withrequired to the subject matter.
5) In case when there's a requirements for taking actionconcurrently while another action being process in the same fileresubmitting the file or record and pending task shall be theresult of other Medical Record Officer immediately after thesecond task.
6) Taking action on the job task and submitting of file to thesupervising offers and pursue the matter.
7) No unattended matter/job/letter/instruction/minute shall befound in a file.
8) No record for more than one day for any reason
26
E.Contents of the File /Documents in the File
Contents /documents are a structured unit of information pertainingto facts, qualifications, decisions and actions taken by DGCA officialsIt is printed or written on paper. It becomes a record if it containsinformation that can be used as evidence of DGCA activity and theprogressive history of the applicant/file.
After the medical certificate has been issued and receive by theapplicant, the Medical Record Officer shall:A. Record the medical assesment data in the Aviation Personel
Medical Record consist ofthe following document as required •i. AMC Form No. 67-01
ii. AMC Form No. 67-02iii. Copy of AMC Form No. 67-03iv. Physical Test Resultv. Laboratory Test Result
vi. Radiology Test Resultvii. Cardiology Test Result
viii. Opthalmology Test Resultix. Audiometry Test Resultx. Dental Test Result
xi. EEG Test Result
B. Keep the Aviation Personel Medical Record in Medical RecordRoom.
F. Archiving of Records
Paper files are to be retained at least 5 years and inactive records willbe kept for at least 5 years before they are destroyed. Inactive recordswill be kept at archiving room.
G.Instructions to Work on the File & Job
1) Identify the job.2) After opening the file the pending job has to be evaluated against
the relevant check list
3) Each item of the check list has to be scrutinized, evaluated andendorsed either yes or no as per the records, evident &subjectknowledge. Also it is advisable to make use of the remarkscolumn to indicate folio number of the records, evidence for thatparticular item and a special comment for the next step ofevaluation of supervising officer.
4) Appropriate minute should be endorsed indicating very clearlywith the facts any ambiguity of taking the decision should also berecorded. Any recommendation also should be notified (or seekinginstructions). &
5) Any item in a check list evaluated as "No" also has to be indicatedin the minute.
6) Proper attention should be made to make references with correctfolio numbers of records minutes or any other similar orprecedence cases.
7) When making reference or minutes only one job or task should bereferred when processing for more than one job.
27
H.Safe Keeping Files
1) Files, records should be kept confidentially, securely and safely atall times in a systematic manner under responsibility of theMedical Record Officers.
2) Only action officers / Medical Record Officers have the authorityto access the files and records in the section.
3) Providing access to any outsiders or applicants is a punishableoffence.
4) Re-production of a record shall be done only with the approval ofthe supervisor.
5) Each action officer shall allocate and designate a separate drawerfor pending jobs and all those records pertaining to that categoryshall be kept under lock and key before finishing the work at theend of the day.
6) Keeping the working files on the tables temporarily is allowed atyour own risk with only a very limited number & shall be
SKSK&2?end of *•day &sha11 be put back to ^I. Medical Record Files
Medical Records &Personnel files containing medical information &reports are considered as very sensitive files.Therefore handling of theMedical files requires special care &attention in terms of security ofthe records as well as confidentiality. Handling of such files °sk^afallVet ?** "t 5*? "" ** **** £**** &key at all the time as provided with the facilities for the purposeExtraction or duplicating of any information pertaining toany of theMedica files are strictly prohibited without explicit approval of AviationMedical Assessor or DGCA. duon
J. Papers in File & Their Maintenance
1) All papers in the file should be numbered in Arabic numerals2) Each paper of attachment to a document shall contain page
number and the total number of pages (i.e. x of y where x is thepage number &y is the total number of pages in the document.
3) All papers should be filed using holes made with a two-hole-ST; ,Paperfa?teners used for filling should be arrangedneatly &tightly so that papers will not be let loose
?°theTLS refemVd t0 ln thC minUtCS Sha11 be flag8ed neatly ^dif there is anyreference in such a document to a previouscorrespondence, folio number of such papers shall also be
5) Afile shall not contain any flagged paper soon after the purposefor it which it was flagged is over.
6) If the subject matter dealt in the file requires frequent reference toany regulation or rules, a copy of such materials shall be includedto the file or in an envelope attached to the inner side of the file'sback cover.
7) Any file shall not contain more than 200 pages. New volumes maybe opened as the file swallows in size.
28
8) There should not be any loose paper attached to the file with apinor clip.
9) Files requiring special attention shall be flagged with "urgent".
K. Library and Reference Documentation
Medical Facility require a set of the own regulatory documents andaccess to a small library of appropriate, updated technical textbooks,ICAO Publications, Manuals and other reference document required forPEL functions. Therefore all ICAO publications are updated timely withrelevant amendments. Such updated publications shall be available foruse by regulatory staff and T e PEL staff requires sets of ICAOdocumentsand, as required, other States* regulatory material and othernecessary technical documentation to streamline this activity efficientlyand effectively.
Each applicant/medical holder should have a personnel file on whichis placed all medical correspondence , medical applicationsassessments, medical reports and all documentation in related to themedical assessment.
An index register system showing the file details is useful for quickreference and statistical purposes.
8. Movement of medical files and medical assessment procedure
a. The following procedure shall be strictly followed by medical unitincluding Aviation Medical Assessor, AMEs, and Nursing Officer.
1) On the receipt of the application, AMC form 67.01 for theconducting of medical assessments for the issuance of medicalassessments for the issuance of personnel licenses, NursingOfficer shall open a new file and verify check list items.
2) Attend to following preliminary test and fill the form 67.02(Ex.Height, weight)
3) Issue the prescription for investigation4) Once all applicable reports are received from the Designated
Hospital, file them with a minute.5) Submit to the examiner with the summary report and the
application at the time of the examination.6) Once Nursing Officer is satisfactory about pre-requisites for the
medical assessments, he shall handover the applicant and file tothe AME for the evaluation.
7) Once medical assessment is recommended by AME for theissuance of medical certificate having taken over the file, keep thefile in a designated file cabinet under lock 8b key under the safecustody of Nursing Officer for issuance certificate except examineby other DGCA medical facility shall be submit to the AviationMedical Assessor.
8) Submit the file on the next immediate date available AviationMedical Assessor for the next action.
9) If the medical certificate issue after pass medical assessment,submit to the PEL section entering the register for the issuance oflicense through the proper channel.
29
KT ^ uco"talnlng al1 medical reports to the correctdesignated cupboard and keep it under safe custody and lock andkey by the Medical Record Officer Nursing Officer
11) Generating copies, dissemination of medical information,divulging medical information, discussing medical information
Jl11!1^t"T* extraction of medical reports shall be consideredprohibited unless explicit approval is obtained from the individualconcern Aviation Medical Examiners concern, Aviation MedicalAssessor s concern or DGCA's concern
12) All aviation Medical Staff shall ensure the highest level of securityand confidentiality when handling the individual Medical Reportsana tiles
30
No
4.
8
10
11
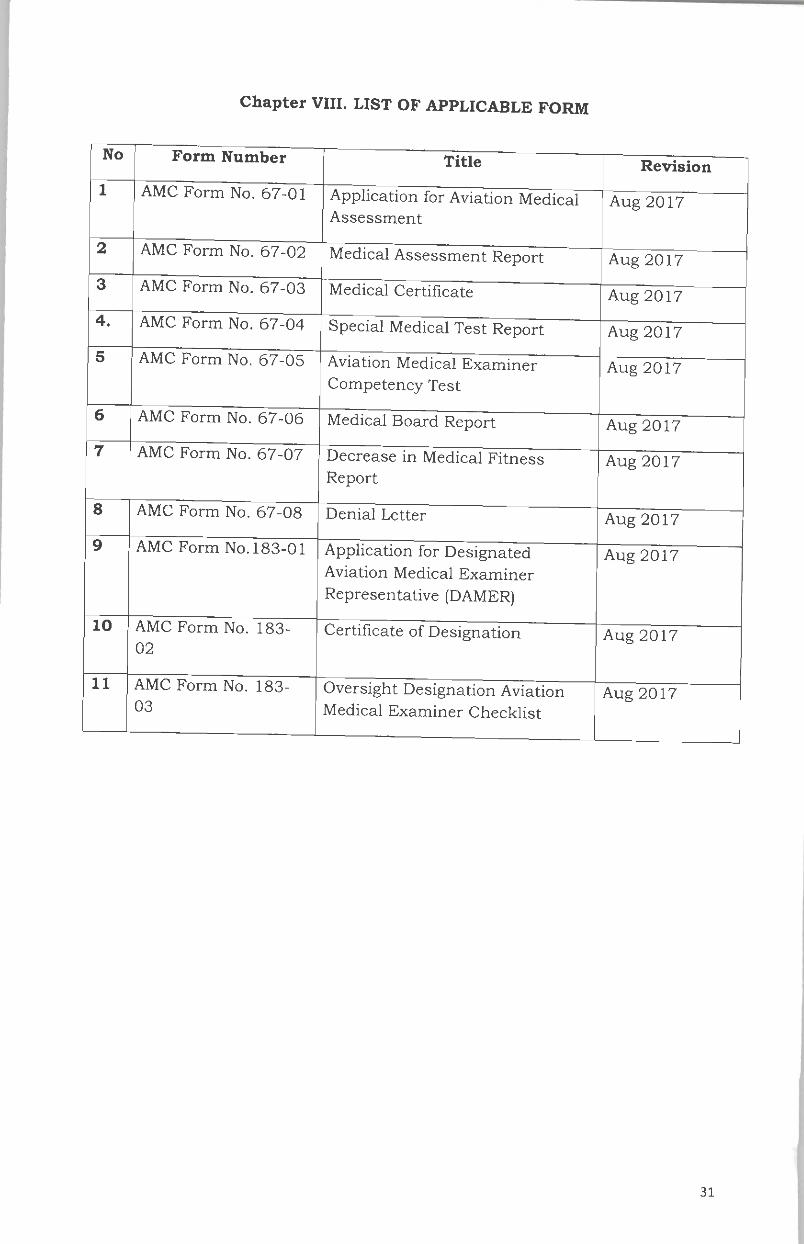
Chapter VIII. LIST OF APPLICABLE FORM
Form Number
AMC Form No. 67-01
AMC Form No. 67-02
AMC Form No. 67-03
AMC Form No. 67-04
AMC Form No. 67-05
AMC Form No. 67-06
AMC Form No. 67-07
AMC Form No. 67-08
AMC Form No. 183-01
AMC Form No. 183-
02
AMC Form No. 183-
03
Title
Application for Aviation MedicalAssessment
Medical Assessment Report
Medical Certificate
Special Medical Test Report
Aviation Medical ExaminerCompetency Test
Medical Board Report
Decrease in Medical FitnessReport
Denial Letter
Application for DesignatedAviation Medical Examiner
Representative (DAMER)
Certificate of Designation
Oversight Designation AviationMedical Examiner Checklist
Revision
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
Aug 2017
31
Appendix A. TRAINING SUBJECT FOR BASIC TRAINING IN AVIATIONMEDICINE
1. Aviation physiology• Cognition and aviation
• Decision making and communication in aviation• Sleep and fatigue as related to commercial aviation• Physics of the atmosphere; effects of altitude on trapped gas• Effects of hypoxia 5• Functional aspects ofvision relevant to aviation• Spatial disorientation• Effects of acceleration
2. Clinical aviation medicine• Aspects ofincapacitation in flight• Effects of ageing as related to flight safety• Cardiological conditions relevant to flight• Neurological conditions relevant to flight• Ophthalmological conditions relevant to flight• Ear/nose/throat conditions relevant to flight• Respiratory conditions relevant to flight• Psychiatric conditions relevant to flight• Metabolic/endocrine conditions relevant to flight• Other conditions relevant to flight (especially gastroenterological,
haematological, urological, renal, gynaecological/obstetricorthopaedic and oncological disease)
• Medication relevant to flight
3. Public Health
• Introduction to the World Health Organization International HealthRegulations (2005)
• Knowledge of SARPs related to public healthAnnex 6- Operation ofAircraft: On board medical suppliesAnnex 9- Facilitation: Public Health Emergencypreparedness planning, Aircraft General DeclarationAnnex 11 - Air Traffic Services: Aspects relevant to publichealth emergencies in contingency planningAnnex 14 - Aerodromes: Aspects relevant to public healthemergencies in aerodrome emergency planning ProceduresforMr Navigation Services - Air Traffic Management: See Part IIIChapter 18, Appendix
Annex 18 - The Safe Transport ofDangerous Goods by AirCarriage of medical items by air e.g. radioactive materials andbiological specimens
l.
ii.
iii.
iv.
32
4. Regulatory medicine
! ?rZT°n, 0n/ntemational Civi' Aviation and its AnnexesICAO Standards and Recommended Practices, with focus onmedically related SARPs
• DGCA Indonesia Licence types and differences in medicalrequirements
• ICAO Annex 1: difference between "Licence" and "MedicalAssessment". Validity periods of Medical Assessments
• Application of "Flexibility Standard" 1.2.4.9 in Annex 1andaccredited medical conclusion
' St?3"011 ^CVidenCe ~CritiCal aPPraiSSl «*«**« -Ports and' diTsIoT " mCdiCal f'tneSS " administrati- Process for an "unfit"• Other medical regulations in the ICAO Annexes (psychoactive
substances, fatigue, oxygen) 'oacuve• Principles ofrisk management• Principles of safety management, as applied to aviation medicine
5. Medical Assessment Procedure for Class 2and Class 3
DIREKTUR JENDERAL PERHUBUNGAN UDARA
ttd
Dr. Ir. AGUS SANTOSO, M.Sc
Salinan sesuai aslinyaKEPALA BAGIAN HUKUM
ENDAH PURNAMA SARIPembina /(IV/a)
NIP. 19680704 199503 2 001
33
Top Related