







Languages
Pages
Legal

Medical Evaluation of the Patient with Brain
Failure
Medical Evaluation of the Patient with Brain
Failure
Jane F. Potter, MDJane F. Potter, MD
Chief Section of Geriatrics & GerontologyChief Section of Geriatrics & Gerontology
University of Nebraska Medical CenterUniversity of Nebraska Medical Center

DeliriumDelirium
• Clinical Presentation: A syndrome of acquired impairment of attention, level of consciousness, and perception.

Evaluation: Confusion Assessment Method (CAM)Evaluation: Confusion Assessment Method (CAM)
Change in cognition that has Change in cognition that has bothboth:: AcuteAcute onset and fluctuating courseonset and fluctuating course AND InattentionAND Inattention
And eitherAnd either Disorganized thinkingDisorganized thinking OR altered level of consciousnessOR altered level of consciousness
Acute Onset AND FluctuationAcute Onset AND Fluctuation
Symptoms develop over Symptoms develop over hours to dayshours to days
(need a reliable informant; if not observed (need a reliable informant; if not observed may present late) may present late) ANDAND
Symptoms Symptoms varyvary through out through out the day; characteristic the day; characteristic lucid interval lucid interval
AND Inattention AND Inattention
Difficulty focusing, sustaining, and shifting Difficulty focusing, sustaining, and shifting attentionattention
Difficulty maintaining conversation or Difficulty maintaining conversation or following commandsfollowing commands
AND Either: Disorganized ThinkingAND Either: Disorganized Thinking
E.G. disorganized E.G. disorganized or incoherent or incoherent thinkingthinking
E.G. Rambling or E.G. Rambling or irrelevant irrelevant conversation conversation ((unpredictable switching unpredictable switching subjects?)subjects?)
OR: Altered Level of ConsciousnessOR: Altered Level of Consciousness
Vigilant (hyperalert, very easily startled)Vigilant (hyperalert, very easily startled)
Lethargic (drowsy, easily aroused)Lethargic (drowsy, easily aroused) Stupor (difficult to arouse)Stupor (difficult to arouse) Coma (unarousable)Coma (unarousable)

Evaluation: CAMEvaluation: CAM
Change in cognition that has Change in cognition that has bothboth:: AcuteAcute onset AND fluctuating courseonset AND fluctuating course
AND Inattention AND Inattention
And eitherAnd either Disorganized thinkingDisorganized thinking OR altered level of consciousnessOR altered level of consciousness
Risk Factorsfor Delirium Risk Factorsfor Delirium
Advanced ageAdvanced age DementiaDementia DepressionDepression Impaired physical Impaired physical
functionfunction Sensory lossSensory loss Decreased oral intake Decreased oral intake
(food and fluids)(food and fluids)
Drugs (ETOH)Drugs (ETOH) Coexisting Medical Coexisting Medical
Illness (severe, multiple, Illness (severe, multiple, CKD, LD, fractures, CKD, LD, fractures, stroke, neurological ds, stroke, neurological ds, HIV)HIV)
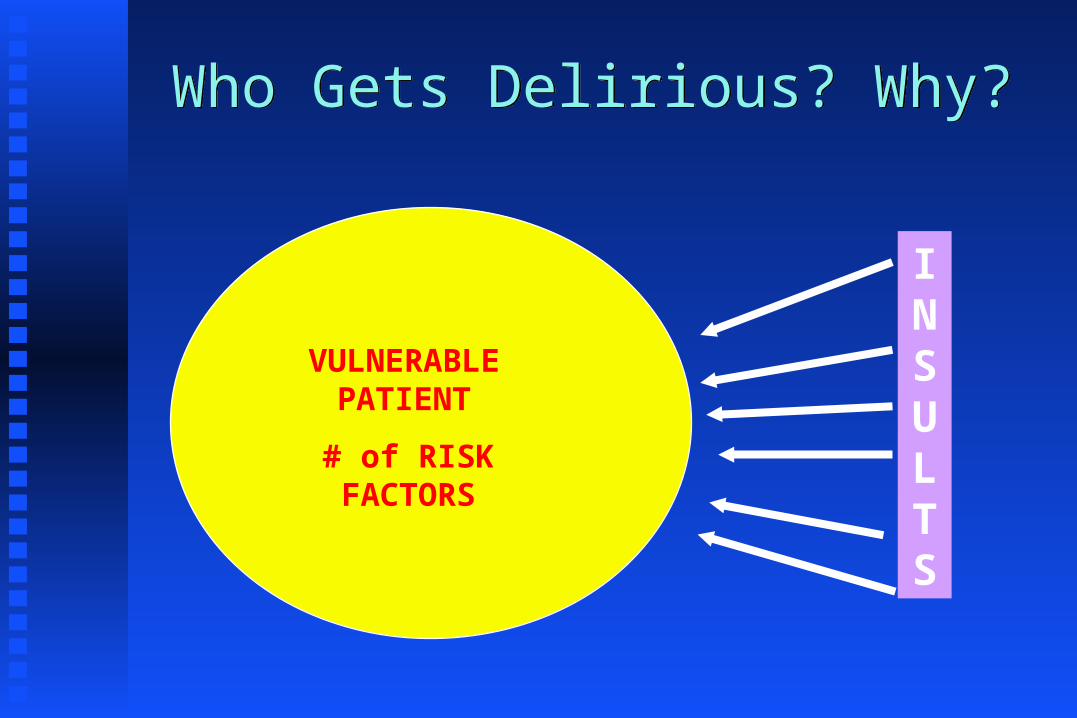
Who Gets Delirious? Why?Who Gets Delirious? Why?
VULNERABLE PATIENT
# of RISK FACTORS
INSULTS
DementiaDementia
• Clinical Presentation: A syndrome of acquired impairment of memory and other cognitive domains sufficient to affect daily life
• Etiology: Any disorder causing damage to brain systems involved in memory. Alzheimer’s disease is the most common cause in later life
Brain FailureBrain Failure The most common The most common
cause of disability in cause of disability in later lifelater life
A focus for geriatric A focus for geriatric practitionerspractitioners

Objectives:Objectives:
Identify the common (non-dementia) causes Identify the common (non-dementia) causes of cognitive dysfunction. of cognitive dysfunction.
Describe a basic approach to evaluate Describe a basic approach to evaluate physical causes of cognitive dysfunctionphysical causes of cognitive dysfunction
Understand interdisciplinary contributions Understand interdisciplinary contributions to evaluation of cognitive dysfunctionto evaluation of cognitive dysfunction
The Brain Failure Evaluation: What to ExpectThe Brain Failure Evaluation: What to Expect
Identification of reversible causesIdentification of reversible causes
Treatment of disabling conditionsTreatment of disabling conditions
Family information, counseling, and referralFamily information, counseling, and referral
CAREFULCAREFUL
CLINICAL OBSERVATION CLINICAL OBSERVATION
IS EVERYTHING!IS EVERYTHING!
Brain Failure:Evaluation
Brain Failure:EvaluationBrain Failure:Evaluation
History/physicalHistory/physical NeurologicNeurologic MedicationsMedications MoodMood AbilitiesAbilities SocialSocial

The Brain Failure EvaluationHistoryThe Brain Failure EvaluationHistory
Collateral SourceCollateral Source
Onset, Course, Progression, Risk FactorsOnset, Course, Progression, Risk Factors
Characteristic Course of Alzheimer’s DiseaseCharacteristic Course of Alzheimer’s Disease
HISTORY OF SYMPTOMSHISTORY OF SYMPTOMS
From a From a
caregiver or caregiver or
someone close someone close
to the patientto the patient
HISTORY OF SYMPTOMSHISTORY OF SYMPTOMS
What were the What were the first symptoms?first symptoms?
How have things How have things changed?changed?
Is this typical Is this typical for AD?for AD?
TYPICAL SYMPTOMS OF ALZHEIMER’S DISEASE TYPICAL SYMPTOMS OF ALZHEIMER’S DISEASE
Functional loss in reverse order to Functional loss in reverse order to which skills were gainedwhich skills were gained
Brain Failure: Case 1Brain Failure: Case 1
An 83 year old widower is evaluated because An 83 year old widower is evaluated because his family is concerned that he is mildly his family is concerned that he is mildly
cognitively slowed. He is still successfully cognitively slowed. He is still successfully maintaining homes in Arizona and Iowa. maintaining homes in Arizona and Iowa.
He describes a 9 month history of decline in He describes a 9 month history of decline in his golf game, a 6 month history of his golf game, a 6 month history of
unexplained falls, and a 1 month history of unexplained falls, and a 1 month history of urinary incontinence.urinary incontinence.

Brain Failure:RecognitionBrain Failure:Recognition
In patients or families presenting with a In patients or families presenting with a complaint of cognitive dysfunction a complaint of cognitive dysfunction a
negative screening test does not exclude negative screening test does not exclude dementia. dementia.
The Brain Failure EvaluationPhysicalThe Brain Failure EvaluationPhysical
Special SensesSpecial Senses
Heart / Lung / Liver / KidneyHeart / Lung / Liver / Kidney
Bladder / Bone / MobilityBladder / Bone / Mobility
VisionVision
HearingHearing
Brain Failure: Special SensesBrain Failure: Special Senses
A 79 year old widower is a member of a A 79 year old widower is a member of a
multigenerational household. He has had multigenerational household. He has had
progressive cognitive problems over the last progressive cognitive problems over the last
7 years. He is independent in all self care 7 years. He is independent in all self care
activities, but at night he wanders about activities, but at night he wanders about
knocking things over and urinating in trash knocking things over and urinating in trash
canscans
•Brain Failure:Case 2•Brain Failure:Case 2
Brain Failure: Case 3Brain Failure: Case 3 A 68 year old married man suffers from A 68 year old married man suffers from
AD. Despite successful treatment of an AD. Despite successful treatment of an
associated depression, he is inattentive and associated depression, he is inattentive and
often does not respond to his wife or often does not respond to his wife or
daughter.daughter.
Brain Failure: organ system dysfunctionBrain Failure: organ system dysfunction Heart and Lung: hypoxic encephalopathyHeart and Lung: hypoxic encephalopathy Hepatic encephalopathyHepatic encephalopathy Renal encephalopathyRenal encephalopathy Thyroid disordersThyroid disorders HyperparathyroidismHyperparathyroidism
Brain Failure: Case 4Brain Failure: Case 4 A 75 year old widow is evaluated at the A 75 year old widow is evaluated at the
request of her family for progressive request of her family for progressive cognitive impairment over the last 9 cognitive impairment over the last 9 months. Her MMSE is 18. During the months. Her MMSE is 18. During the interview she admits to exertional fatigue, interview she admits to exertional fatigue, and lack of energy. On exam she has and lack of energy. On exam she has diffuse expiratory wheezing in all lung diffuse expiratory wheezing in all lung fields.fields.
Brain Failure = DisabilityBrain Failure = Disability
Families/Patients are complaining of the Families/Patients are complaining of the disabilitydisability caused by brain dysfunction.caused by brain dysfunction.
The population at risk is characterized by a The population at risk is characterized by a burden of burden of co-morbiditiesco-morbidities..
Look for Look for un or under-treatedun or under-treated comorbidities comorbidities causing dysfunction.causing dysfunction.
High yield for disorders of bladder, bone, High yield for disorders of bladder, bone, mobility.mobility.
Families/Patients are complaining of the Families/Patients are complaining of the disabilitydisability caused by brain dysfunction.caused by brain dysfunction.
The population at risk is characterized by a The population at risk is characterized by a burden of burden of co-morbiditiesco-morbidities..
Look for Look for un or under-treatedun or under-treated comorbidities comorbidities causing dysfunction.causing dysfunction.
High yield for disorders of bladder, bone, High yield for disorders of bladder, bone, mobility.mobility.
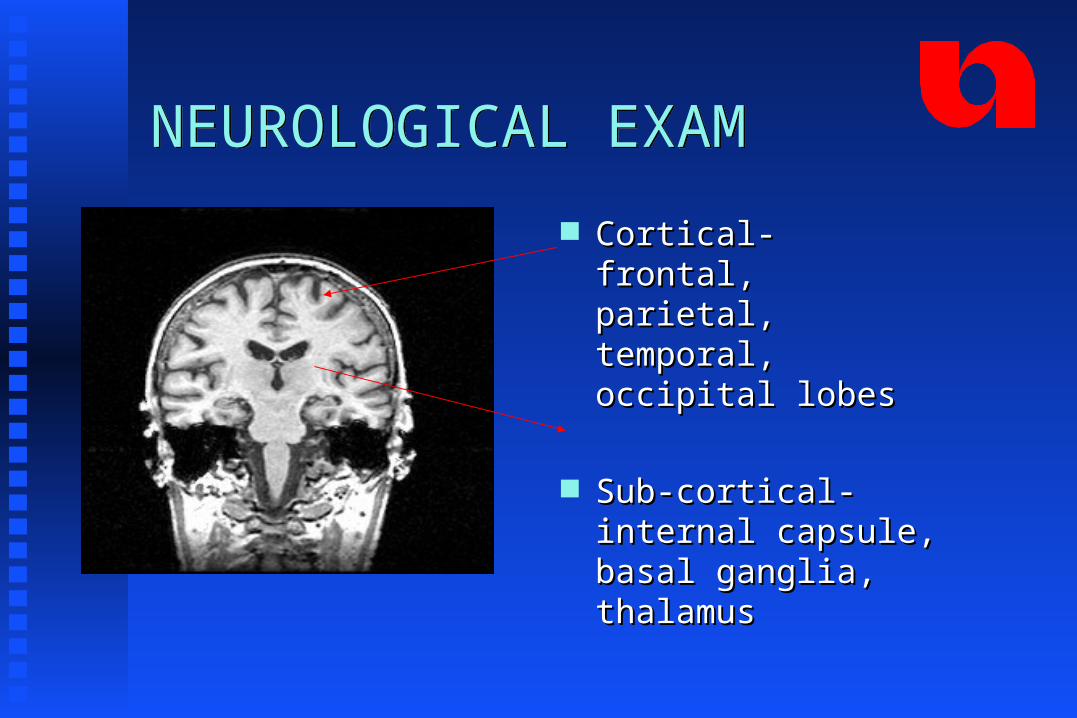
NEUROLOGICAL EXAMNEUROLOGICAL EXAM
Cortical- frontal, Cortical- frontal, parietal, temporal, parietal, temporal, occipital lobesoccipital lobes
Sub-cortical- internal Sub-cortical- internal capsule, basal ganglia, capsule, basal ganglia, thalamusthalamus
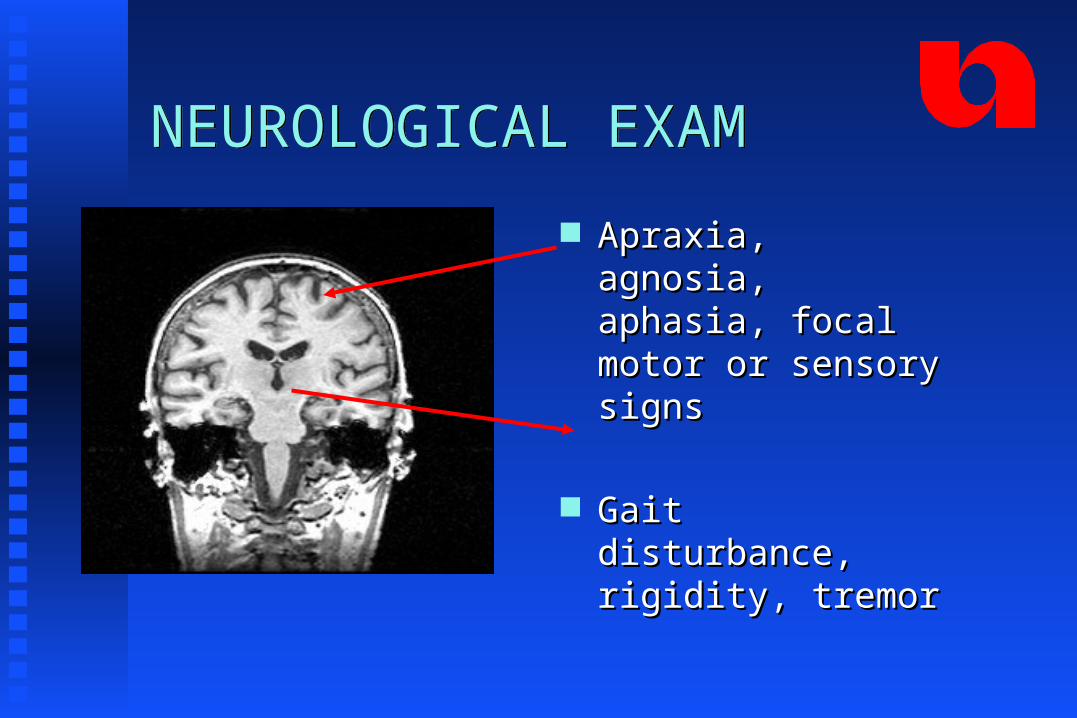
NEUROLOGICAL EXAMNEUROLOGICAL EXAM
Apraxia, agnosia, Apraxia, agnosia, aphasia, focal motor or aphasia, focal motor or sensory signs sensory signs
Gait disturbance, Gait disturbance, rigidity, tremorrigidity, tremor
Frontal Lobe Release signsFrontal Lobe Release signs
MovieClips\Glabellar.movMovieClips\Glabellar.movGlabellar tapGlabellar tap PalmomenttalPalmomenttal GraspGrasp
GaitGait
CorticalCortical
SubcorticalSubcortical
Sutton’s Law:Sutton’s Law:
““Gee, Willy, why do you rob banks?Gee, Willy, why do you rob banks?
“BECAUSE
THAT’S
WHERE THE
MONEY IS”

Geriatrician’s Law:Geriatrician’s Law:
Go for the MEDS
Because that’s where the money is
Inspect the Drug BagInspect the Drug Bag
Three or more Three or more drugs increase the drugs increase the likelihood of an likelihood of an adverse effect or adverse effect or drug interactiondrug interaction
Drugs and Brain FailureDrugs and Brain Failure Many drugs can do this, e.g.
Sedatives, anxiolytics, anticholinergics, H2-blockers, centrally acting antihypertensives (clonidine, alpha-methyl dopa) antiarhythmics, beta blockers, digoxin, sinemet, selegeline.
Check all for CNS S.E.s Try a “Drug Holiday”

Alcohol and Brain Failure Alcohol and Brain Failure
Volume of Volume of
distribution for distribution for ETOH ETOH
with agewith age
No more than one/day No more than one/day
after age 65; stop all if after age 65; stop all if
cognition impairedcognition impaired
Brain Failure: Case 4Brain Failure: Case 4 An 83 year old widow presents with a An 83 year old widow presents with a
history of progressive cognitive failure. history of progressive cognitive failure. During interview she admits to a long term During interview she admits to a long term pattern of one drink before dinner. On pattern of one drink before dinner. On questioning, her daughter feels that she questioning, her daughter feels that she likely exceeds one drink per day.likely exceeds one drink per day.
Depression as Brain FailureDepression as Brain Failure
Emotional illness Emotional illness
slows cognitive slows cognitive
function function

Depression as a Cause of Brain FailureDepression as a Cause of Brain Failure
Dementia Insidious onset Long duration No psychiatric history
Conceals disability (often unaware of memory loss)
“Near-miss” answers
Day-to-day fluctuation in mood
Depression Abrupt onset Short duration Previous psychiatric history
Highlights disabilities (may complain of the memory loss)
“Don’t know” answers
Diurnal variation in mood, but generally more consistent
The Brain Failure EvaluationThe Brain Failure Evaluation
UNDERSTAND THE NORMAL UNDERSTAND THE NORMAL
AGE-RELATED CHANGES IN AGE-RELATED CHANGES IN
BRAIN AND MEMORYBRAIN AND MEMORY

Brain Failure vs Normal AgingBrain Failure vs Normal Aging
Normal aging Normal aging does not cause does not cause dysfunction dysfunction
The Brain Failure EvaluationLaboratory
The Brain Failure EvaluationLaboratory B-12, Folate, TSHB-12, Folate, TSH Chem profile, UA, ?OChem profile, UA, ?O2 sat sat
CBCCBC Other as indicated Other as indicated

The Brain Failure EvaluationRadiology & OtherThe Brain Failure EvaluationRadiology & Other
Head CT, ? Head MRIHead CT, ? Head MRI Chest X-rayChest X-ray EKG, EEGEKG, EEG
Things that Cause the Brain to Fail (whether or not an underlying dementia is present)
Things that Cause the Brain to Fail (whether or not an underlying dementia is present)
DrugsDrugs Emotional Illness (including depression)Emotional Illness (including depression) Metabolic/endocrine disordersMetabolic/endocrine disorders Eye/ear/environmentEye/ear/environment Nutritional/neurologicalNutritional/neurological Tumors/traumaTumors/trauma InfectionInfection Alcoholism/anemia/ atherosclerosisAlcoholism/anemia/ atherosclerosis
DEMENTIA

Therapy for ADTherapy for AD Cholinesterase inhibitorsCholinesterase inhibitors Vitamin EVitamin E NMDA inhibitor- MemantineNMDA inhibitor- Memantine ? Vaccination? Vaccination Not EstrogenNot Estrogen Not Anti-inflammatoriesNot Anti-inflammatories
Top Related