







Languages
Pages
Legal


Case 28
Male 35. Common variable immunodeficiency. Six
month history of slowly growing nodules right arm and
left lower leg (biopsied). Ziehl-Neelsen, PAS, Grocott
and Gram stains all negative. The best diagnosis is:
A. Necrobiosis lipoidica
B. Granulomas of immunodeficiency
C. Deep granuloma annulare
D. Atypical mycobacterial infection
E. Necrobiotic xanthogranuloma

HISTORY
Diagnosed in adulthood with common variable immunodeficiency as found to be panhypoglobulinaemic
Prior to diagnosis he had problems with recurrent ear, sinus and chest infections

HISTORY
6 month history of “insect bite” that had not healed on left lower leg and slowly become more crusty

HISTORY
• lesion on right arm had become red, raised and itchy

Case 28: Clinical differential diagnosis
Infection – bacterial such as ecthyma, leishmaniasis, TB, deep
fungus
But, multiple courses of various antibiotics for his chest had made
no difference to his skin lesions
Sarcoid
Lymphoma or other skin cancers (BCC)
So - biopsies taken from right arm and left shin for histology and
multiple cultures.

Punch biopsy skin left shin

Punch biopsy skin left shin

Punch biopsy skin right arm

Some granulomas more
well circumscribed,
“sarcoidal”
Some granulomas have central necrosis,
“necrotising granuloma”
Punch biopsy skin right arm

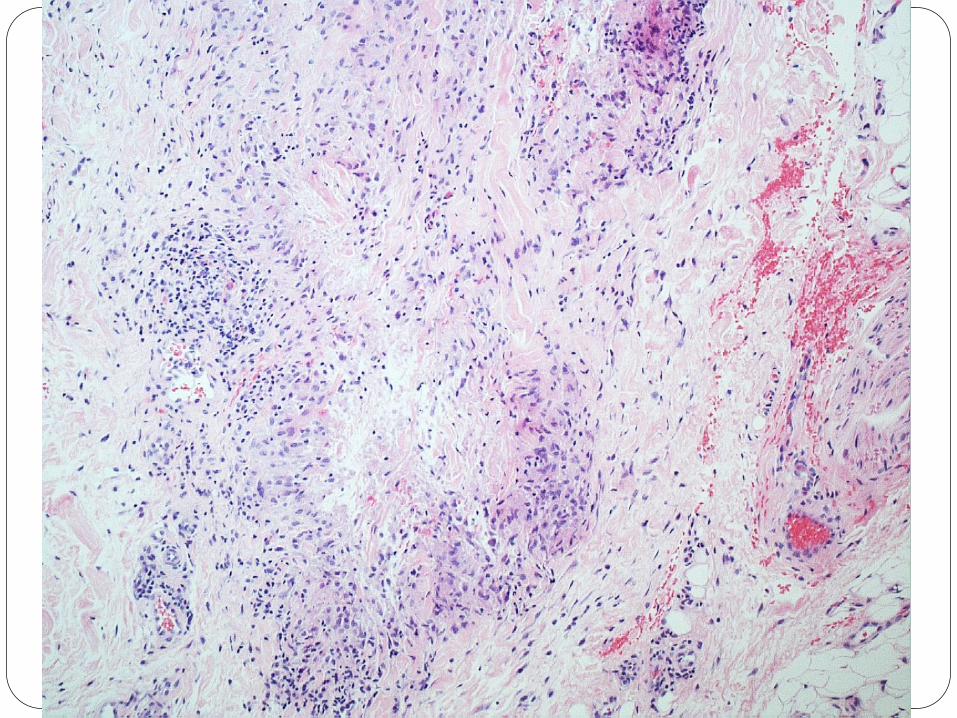
mixed granulomatous inflammation in both biopsies
necrotising, tuberculoid, sarcoidal and necrobiotic
granulomas present to varying degrees
No evidence of infection on special stains (Ziehl-Neelsen,
Gram, PAS and Grocott)
No evidence of infection on cultures including mycobacteria
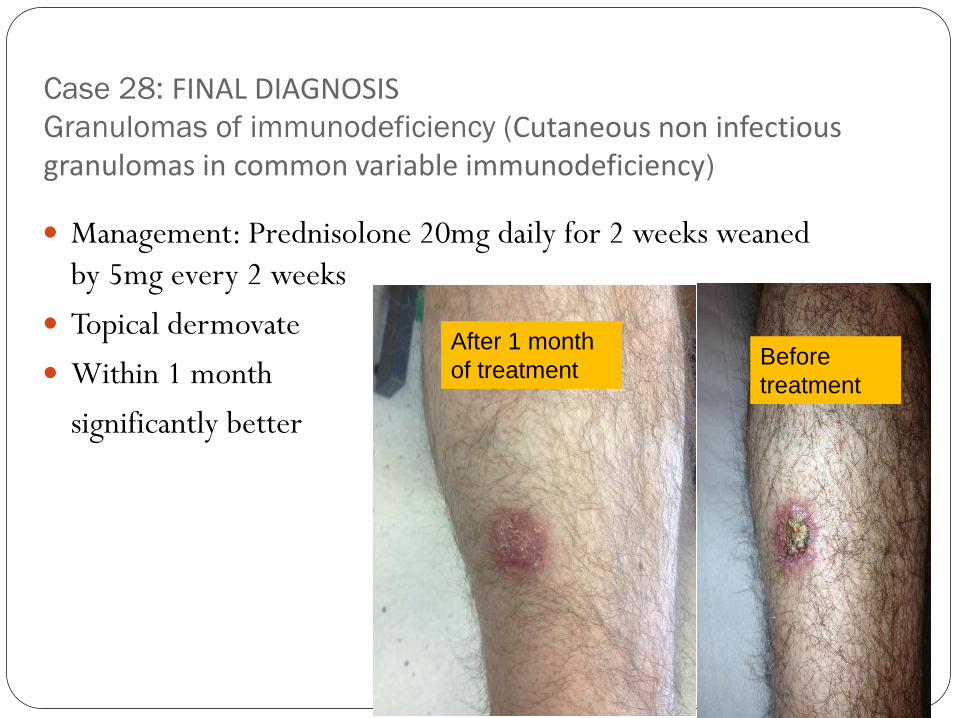
Case 28: FINAL DIAGNOSIS Granulomas of immunodeficiency (Cutaneous non infectious granulomas in common variable immunodeficiency)
Management: Prednisolone 20mg daily for 2 weeks weaned
by 5mg every 2 weeks
Topical dermovate
Within 1 month
significantly better
After 1 month
of treatment Before
treatment

Management
Prednisolone 20mg daily for 2 weeks weaned by 5mg every 2
weeks
Topical dermovate
Within 1 month
Significantly better After 1 month of
treatment rbBefore
treatment
bbbbb

Follow up
Stopped steroid after 8 weeks and has had no further skin
issues to date
Lesions completely healed with scarring.
Repeat CT chest/abdo/pelvis has excluded internal
granulomas
No further skin lesions since (1 year later)

Case 28 differential diagnosis
necrobiosis lipoidica:
also shins,
full thickness dermis mainly with only
extension into subcutis;
also plasma cells, lymphocytes

Case 28 differential diagnosis
necrobiosis lipoidica: also shins, full thickness dermis mainly
with only extension into subcutis; also plasma cells, lymphocytes

necrobiosis lipoidica

Case 28 Differential diagnosis:
deep (subcutaneous) granuloma annulare

Case 28 Differential diagnosis:
deep (subcutaneous) granuloma annulare
10 year old girl.
Firm subcutaneous nodules on scalp.

necrobiotic granuloma

necrobiotic granuloma

Necrobiotic granuloma: loss of collagen and elastic fibres (elastic van Gieson)

deep (subcutaneous) granuloma annulare:
clinical features
• Children mainly, 1-6yrs especially, mean 4.7years.
• Present with sometimes tender nodule(s) 10-35mm on lower legs (shins) > scalp (occiput) > feet, buttocks, fingers, hands, forehead.
• Mobile (less so on scalp).
• Often misdiagnosed as tumour and 6 month average to diagnosis – get frozen sections from orthopaedics.
• A few have typical GA lesions.
• No rheumatoid arthritis or other A/I disease.
• Mostly regress within months to few yrs so don’t
need to treat but up to19% recur (same site).
• ?trauma related in some:
6/14 just started shoes/new shoes (Aberdeen study1).
• CT/MRI:confined to subcutis.

deep (subcutaneous) granuloma annulare:
histological features
• Multiple well circumscribed nodules of necrobiosis in subcutaneous tissue with
palisading macrophages around the nodules, mucin in centre, normal between.
• Loss of elastin. Little other inflammation.
• Often vascular spaces at edge of nodule
• Central mucin – grey/blue not eosinophilic like rheumatoid nodule
• Usually not recognized before biopsy unless paediatric
dermatologist, diagnosis often doubted especially if recurs.
• Unusual sites for necobiotic disorders a clue
Evans MJ, Blessing K, Gray ES.
Pseudorheumatoid nodule (deep granuloma annulare) of
childhood: clinicopathologic features of twenty patients.
Pediatr Dermatol. 1994 Mar;11(1):6-9

Differential diagnosis – infective granulomas e.g.
Atypical mycobacterial infection (such as M. chelonae infection)
also shows necrotising granulomas (and suppurative granulomas)

Differential diagnosis –
Necrobiotic xanthogranuloma

Br J Dermatol. 1994 Jan;130(1):118-20.
Cutaneous sarcoid-like granulomas in primary immunodeficiency disorders.
Levine TS(1), Price AB, Boyle S, Webster AD.
Author information:
(1)Department of Cellular Pathology, Northwick Park Hospital and Clinical Research
Centre, Harrow, Middlesex, U.K.
We report the occurrence of cutaneous sarcoid-like granulomas in one patient with
common variable immunodeficiency and another with 'thymoma and
hypogammaglobulinaemia'. To our knowledge, this is the first time that such skin
lesions have been described in patients with primary immunodeficiency. These
granulomas may be attributed to a combination of interleukin-2 deficiency and a
profound CD4 lymphopenia. The lesions are similar to the non-infectious 'papular
eruption' associated with human immunodeficiency virus infection, and might
reflect a common pathogenic mechanism.

COMMON VARIABLE IMMUNODEFICIENCY
X-LINKED AGAMMAGLONULINEMIA
ISOLATED IgA DEFICIENCY
HYPER IgM SYNDROME
Di GEORGE SYNDROME
SEVERE COMBINED IMMUNODEFICIENCY
IMMUNODEFICIENCY WITH THROMBOCYTOPENIA
AND ECZEMA
GENETIC DEFICIENCIES OF COMPLEMENT,
IMMUNODEFICIENCY SYNDROMES

Common variable Immunodeficiency
(CVID)
Low levels of most or all Ig classes
Lack of B lymphocytes or plasma cells that are capable of
antibody production
Frequent bacterial infections

Signs and symptoms of CVID
Recurrent bacterial infections The most common are sinusitis, pneumonia, bronchitis, otitis, conjunctivitis and
gastrointestinal infection.
Streptococcus and haemophilus most common
Autoimmune phenomena in 20-50% Rheumatoid arthritis/haemolytic anaemia/neutropaenia/thrombocytopaenia
Malignancy – B cell lymphomas
Granulomatous disease – skin and internal organs

Dermatologic manifestations of CVID
Alopecia areata.
Vitiligo
Skin granulomas - both sarcoid-like
(non-necrotising) and tuberculoid (necrotising)
Increased risk of actinic keratosis,
squamous cell carcinomas and melanoma.
Increased risk of polymorphic light eruption and atopic
dermatitis.
MANAGEMENT
All skin lesions suggestive of infection need biopsy
Imaging. This is likely to be required and may have to be
extensive, including different modalities (CT scanning, MRI)
according to the clinical manifestations of disease.

Management of granulomas
Exclude infection
Oral steroids
Other immunosuppressant's
TNF alpha antagonists

Take home message:
Non-infectious granulomas are not uncommonly seen in the
skin of patients with immunodeficiency disorders
Infection must be ruled out first
Treatment is with immunosuppressive agents eg steroids
Investigation for possible immunodeficiency should be
considered especially in children and young adults with
unusual granulomatous skin pathology.

Case 28
Male 35. Common variable immunodeficiency. Six
month history of slowly growing nodules right arm and
left lower leg (biopsied). Ziehl-Neelsen, PAS, Grocott
and Gram stains all negative. The best diagnosis is:
A. Necrobiosis lipoidica
B. Granulomas of immunodeficiency
C. Deep granuloma annulare
D. Atypical mycobacterial infection
E. Necrobiotic xanthogranuloma
Top Related