







Languages
Pages
Legal

Tiirkish Neiirosiirgery 11: 56 - 59, 2001 Berkmaii: LYl1lphaligioma of the skiill
Lymphangioma of the Skull: A Case Report
Kafatasinda Lenfanjiom: Olgu Sunumu
M. ZAFER BERKMAN, SIRZAT BEK, DENIz OZCAN
Okmeydani Social Security Hospita!, Departments of Neurosurgery (MZB, SB)and Pathology (DÖ), Sisli, Istanbul, Turkey
Reeeived : 3.5.1998 ~ Aeeepted : 13.7.1998
Abstraet: Lymphangioma is a relatively eommon tumorof soft tissue, but a rare primary lesion of bone. Very feweases of skulllymphangioma have been reported to date.We deseribe a patient with solitary lymphangioma of theskull that was treated by total excision and autogenousbone graftingo We also review the literature on this formof neoplasia.
Key Warrls: Lymphangioma, skull, tumor
INTRODUCTION
Lymphangioma is a relatively common softtissue tumor that most often arises in the neck andaxilla (5,7,9,10,15,16). Although this neoplasm canaffect internal organs, central nervous system (CNS)involvement is uncommon, and bone involvement iseven more unusuaL. Skull lymphangioma isparticularly rare, but the literature does contain a fewcases that have involved the cranium (6,12,13), skullbase (l5), scalp (lO), and vertebrae (2,4,11). The caseof skulllymphangioma documented in this report issignificant because there have been only a few suchcases described to date.
56
Özet: Lenfanjiom, yumusak dokunun kismen sik f:i~,.:tkemigin nadir primer lezyonudur. Günümüze bd"" P"I.;
az kafatasilenfanjiomu olgusu bildirilmistir. YazarlilI' t,it,1i
olarak eksize edilip otojen kemik grefti ile tedavi edijel!bir kafatasi soliter lenfanjiomu bildirmisler; lenfanjiom iIP
ilgili literatürü ineelemislerdir.
Anahtar Kelimeler: Lenfanjiom, kafatasi, tümör
CASE REPORT
A 28-year-old female was admitted with thecomplaints of constant headache and a swellingnear the midline of the frontal area of her skull,both of which had been present for 6 months. Theswelling was approximately 1 cm in diameter whenit was first noticed, but had enlarged in the past 2months. There was no history of trauma or systemicillness.
Physical examination revealed a firm, painless,fixed swelling of 5 cm diameter on the frontal aspectof the cranium. The patient's neurologicalexamination and laboratory values were normaL.
TiirkisJi Neurosiirgery 11: 56 - 59, 2001
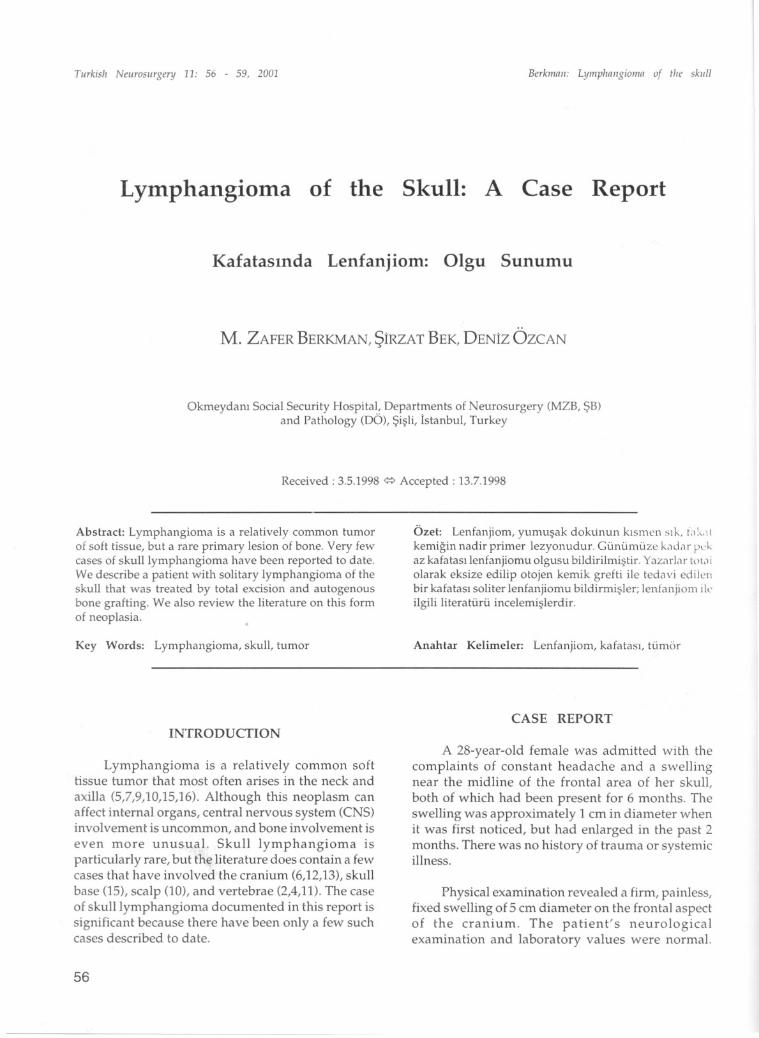
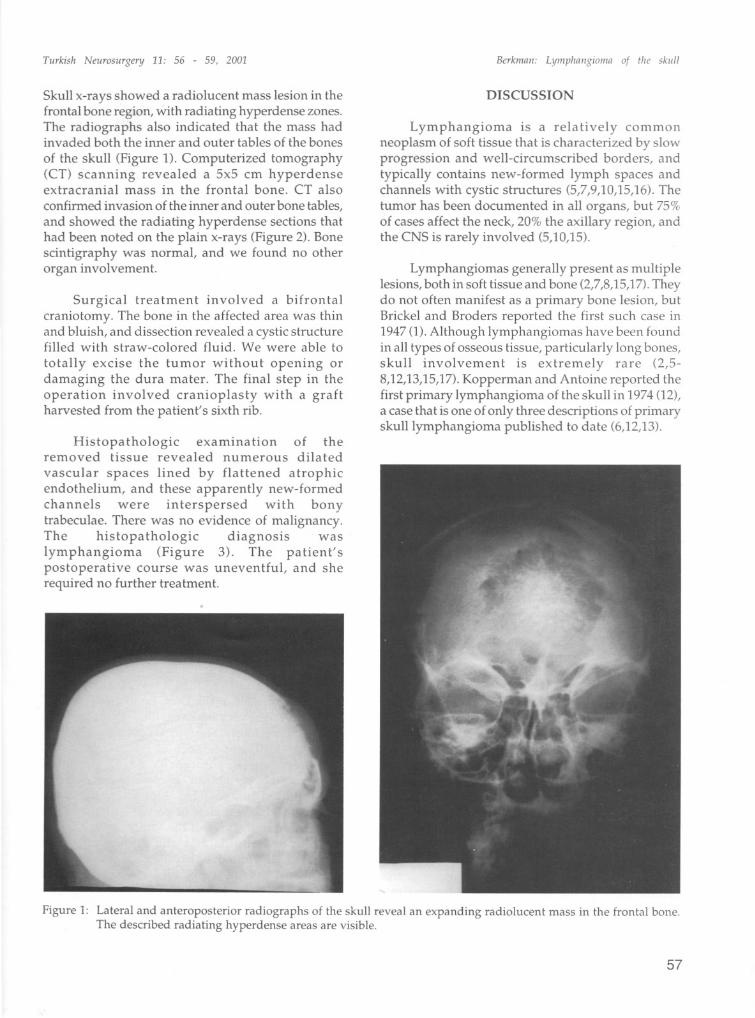
Skull x-ray s showed a radiolucent mass lesion in thefrontal bone region, with radiating hyperdense zones.The radiographs also indicated that the mass hadinvaded both the inner and outer tables of the bonesof the skull (Figure 1). Computerized tomography(CT) scanning revealed a 5x5 cm hyperdenseextracranial mass in the frontal bone. CT alsoconfirmed invasion of the inner and outer bone tables,and showed the radiating hyperdense sections thathad been noted on the plain x-rays (Figure 2). Bonescintigraphy was normal, and we found no otherorgan involvement.
Surgical treatment involved a bifrontalcraniotomy. The bone in the affected area was thinand bluish, and dissection revealed a cystic structurefilled with straw-colored fluid. We were able tototally excise the tumor without opening ordamaging the dura mater. The final step in theoperation involved cranioplasty with a graftharvested from the patient's sixth rib.
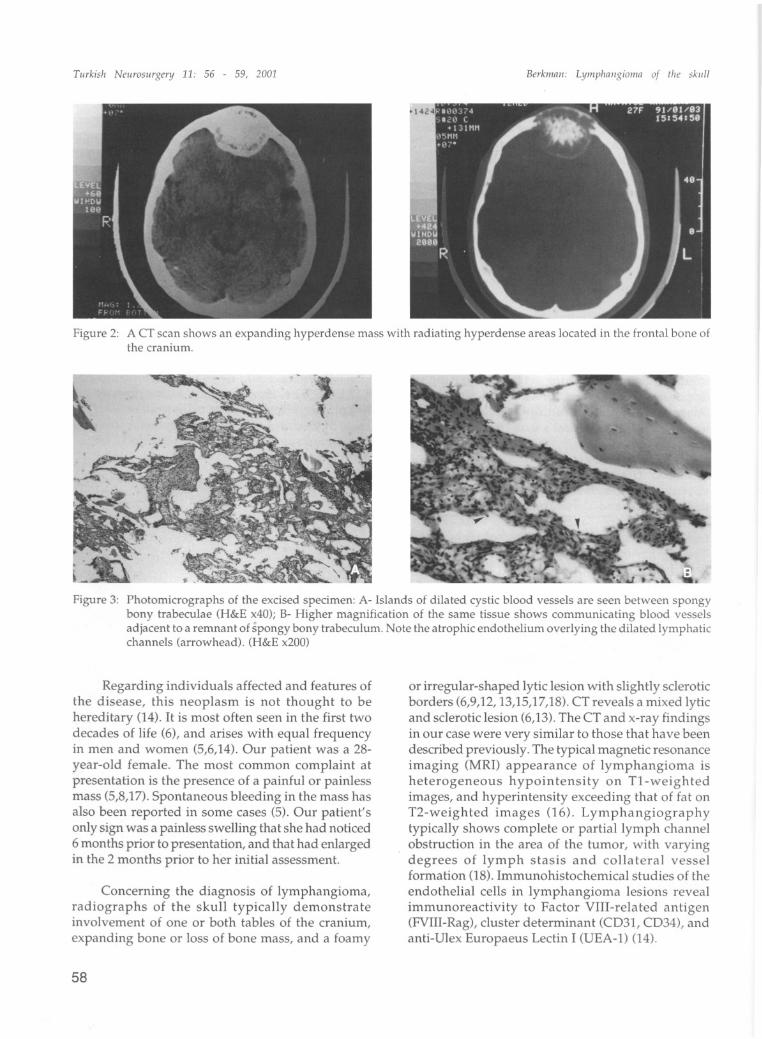
Histopathologic examination of theremove d tissue revealed numerous dilated
vascular spaces lined by flattened atrophicendothelium, and these apparently new-form edchannels were interspersed with bonytrabeculae. There was no evidence of malignancy.The histopathologic diagnosis waslymphangioma (Figure 3). The patient'spostoperative course was uneventful, and sherequired no further treatment.
Berkmoii: LympJioiigioiiio of ilie skiill
DISCUSSION
Lymphangioma is a relatively commonneoplasm of soft tissue that is characterized by slowprogression and well-circumscribed borders, andtypically contains new-formed lymph spaces andchannels with cystic structures (5,7,9,10,15,16). Thetumor has been documented in all organs, but 75%of cases affect the neck, 20% the axillary region, andthe CNS is rarely involved (5,10,15).
Lymphangiomas generally present as multiplelesions, both in soft tissue and bone (2,7,8,15,17).Theydo not often manifest as a primary bone lesion, butBrickel and Broders reported the first such case in1947 (1).Although lymphangiomas have been foundin all types of osseous tissue, particularly long bones,skull involvement is extremely ra re (2,58,12,13,15,17).Kopperman and Antoine reported thefirst primary Iymphangioma of the skull in 1974 (12),a case that is one of only three descriptions of primaryskull Iymphangioma published to date (6,12,13).
Figure 1: Lateral and anteroposterior radiographs of the skull reveal an expanding radiolucent mass in the frantal bone.The described radiating hyperdense areas are visible.
57
Tiirkislr Neurosiirgery 11: 56 - 59, 2001 Berkiiinii: Lymplrniigioiiin of tire skI/II
Figure 2: A CT sean shows an expanding hyperdense mass with radiating hyperdense areas loeated in the frontal bone ofthe eranium.
Figure 3: Photomierographs of the exeised specimen: A- Islands of dilated eystic blood vessels are seen between spongybony trabeeulae (H&E x40); B- Higher magnifieation of the same tissue shows eommunieating blood vesselsadjaeent to a remnant of spongy bony trabeeulum. Note the atrophie endothelium overlying the dilated lymphatieehannels (arrowhead). (H&E x200)
Regarding individuals affeeted and features ofthe disease, this neoplasm is not thought to behereditary (14). it is most often seen in the first twodecades of life (6), and arises with equal frequencyin men and women (5,6,14). Our patient was a 28year-old female. The most comman complaint atpresentation is the presence of a painful or painlessmass (5,8,17). Spontaneous bleeding in the mass hasalsa been reported in same cases (5). Our patient'sonly sign was a painless sweIIing that she had noticed6 months prior to presentation, and that had enlargedin the 2 months prior to her initial assessment.
Conceming the diagnosis of lymphangioma,radiographs of the skuIl typicaIly demonstrateinvolvement of one or both tables of the cranium,expanding bone or lass of bone mass, and a foamy
58
or irregular-shaped lytic lesian with sIightly scIeroticborders (6,9,12, 13,15,17,18). CT reveals a mixed lyticand scIerotic lesion (6,13).The CT and x-ray findingsin our case were very similar to those that have beendescribed previously. The typical magnetic resonanceimaging (MRI) appearance of lymphangioma isheterogeneous hypointensity on T1-weightedimages, and hyperintensity exceeding that of fat onT2-weighted images (16). LymphangiographytypicaIly shows complete or partial lymph channelobstruetion in the area of the tumor, with varyingdegrees of lymph stasis and coIlateral vesselformatian (18). Immunohistochemical studies of theendotheIial ceIls in lymphangioma lesions revealimmunoreactivity to Factor VIII-related antigen(FVIII-Rag), cIuster determinant (CD31, CD34), andanti-Ulex Europaeus Lectin i (UEA-1) (14).

Tiirkisli Neiirosiirgenj 11: 56 - 59, 2001
The three different histological types ofIymphangioma are eystic lymphangioma, capillary orsimple lymphangioma, and cavernous lymphangioma(4,5,8). The cystic form is a multilocular cystic massknown as "eystic hygroma" that occurs most often inthe neck or axillae of children. No bone involvement
has been documented with this type. The lesi on incapillary or simple lymphangioma is charaeterized bycapillary-sized lymphatic channels. This type usuallyarises in the skin, but bone involvement has be en
observed. The mass in cavernous lymphangiomacontains larger lymphatic channels, and is known toarise in bone, soft tissue, and viscera. The growthconsists of endothelial cells and connective tissue, and
thus is considered to originate from mesodermalremnants. it is considered a benign congenitalmalformation rather than a tumor, and is charaeterized
by osteolytic and cystic components. When blood cellsare present, the cystic component can be confused withaneurysmal bone cysts and hemangiomas (3-6,13).When this form occurs in bone, there are of ten
abnormalities of the haversian canals and of the lymphcanals in the periosteum (1). The differential diagnosisfor lymphangioma of the skull ineludes aneurysmalbone cyst, eosinophilic granuloma, osteitis fibrosacystica, hystiocytosis X, hemangioma, solitaryplasmocytoma, osteoma, meningioma, and metastasis(3,4,6,11,13,15,17).
Surgery is the definitive treatment forIymphangioma of the skull, and total excision is alwaysnecessary. Studies have shown that cureHage alone isnot successful (5,6). Bone grafting has generally yieldedpoor results because the grafted bone tends to becomeinvolved with the angiomatous process, and new boneformation is compromised (6); however, grafting isrequired when tumor removal results a large bonedefect (2). Recurrence is almost always associated withsubtotal tumor remova], and usually occurs within ayear of the initial surgery (l0,16). Radiotherapy is noteffectiye when applied alone, but may be used asadjunctive treatment in cases of subtotal excision ortumor recurrence (2,4,6). Currently, chemotherapy isnot used to treat this disease (6). Although selerosingagents have been applied to these tumors in the past,this method is no longer considered a good alternatiyeto surgery (5).
In conelusion, the case of skulllymphangiomadescribed in this report is one of a smail handful inthe literature. Although this lesion is extremely rare,lymphangioma should be considered in thedifferential diagnosis of any solitary expanding orlytic lesion of the cranium.
Berkmaii: Lymphallgiol1la of the skiill
Correspondence: M. Zafer BerkmanHalaskargazi Caddesi, Mimler AptNo: 337 Kat: 4 Sisli, Istanbul, TurkeyTel: +90 (212) 2881114Fax: +90 (212) 2749101
REFERENCES
1. Bickel WH, Broders AC: Primary lymphangioma of theilium. Report of a case. J Bone Joint Surg 29:517-522,1947
2. Cohen J, Craig JM: Multiple lymphangiectases of bone.J Bone Joint Surg 37:585-596, 1955
3. Devaney K, Vinh TA, Sweet DE: Skeletal-extraskeletalangiomatosis. J Bone Joint Surg 76:878-891,1994
4. Edwards WH, Thompson RC, Varsa EW:Lymphangiomatosis and massive osteolysis of thecervical spine. Clin Orthop 177:222-229, 1983
5. Enzinger FM, Weiss SW: Soft tissue tumorso 2nd ed. StLouis, CV Mosby Co. 1988, pp 614-637
6. Evans DA, Baugh RF, Gildsdorf JR, Heidelberger KP,Niparko JK: Lymphangiomatosis of skuii manifestingwith recurrent meningitis and cerebrospinal fluidotorrhea. Otolaryngology-Head and Neck Surgery103:642-666,1990
7. Harris R, Prandoni AG: Generalized primarylymphangiomas of bone: Report oL case associatedwith congenital lymphedema of forearm. Ann Int Med33:1302-1313, 1950
8. Hilliard RI, McKendry JBJ, Phillips JM: Congenitalabnormalities of the lymphatic system: A new clinicalclassification. Pediatrics 86:988-994, 1990
9. Huvos AG: Bone tumors Diagnosis, Treatment andProgress. 2nd ed. Philadelphia, WB Saunders Co, 1991,pp 563-566
10. Inci S, Bavbek M, Özcan OE, Önol B, Gedikoglu G:Lymphangioma of the scalp. Turkish Neurosurgery2:203-206, 1992
11. Keenen TL, Buehler KC, Campbell JR: Solitarylymphangioma of the spine. Spine 20:102-105,1994
12. Kopperman M, Antoine JE: Primary lymphangiomaof the calvarium. Am J Roentgenol 121:118-120, 1974
13. Nazarian GK, Gebarski SS, Niparko JK: Craniallymphangiomatosis causing CSF otorrhea andrecurrent meningitis: CT features. J Comput AssistTomogr 14:121-123,1990
14. Ramani P, Shah A: Lymphangiomatosis. Am J SurgPathol 17:329-335, 1993
15. Rogers HM, Chou SN: Lymphangioma of thecraniovertebral junction. Case report. J Neurosurg38:510-513, 1973
16. Siegel MJ, Glazer HS, St Amour TE, Rosenthal DD:Lymphangiomas in children: MR imaging. PediatricRadiology 170:467-470, 1989
17. Snopfner CE, Aiien RP: Lymphangioma of bone.Radiology 76:449-453, 1961
18. Winterberger AR: Radiographic diagnosis oflymphangiomatosis of bone. Radiology 102: 321-324,1972
59
Top Related