








Languages
Pages
Legal


LIVER “FUNCTION” TESTS
Edith Y. Ho, M.D. M.S.
Assistant Professor of Medicine, Division of Gastroenterology
Case Western Reserve University
Louis Stokes Cleveland VA Medical Center
Director, Inflammatory Bowel Diseases Program
Co-Director, Fecal Microbiota Transplantation Program
12/18/2015

Agenda
Tests showing liver cell injury
Tests showing hepatic function / synthesis
Tests showing cholestasis
Bilirubin metabolism
Other important liver tests
Patterns in liver injury ☻


Agenda
Tests showing liver cell injury
Tests showing hepatic function / synthesis
Tests showing cholestasis
Bilirubin metabolism
Other important liver tests

2.78.6
2561
132 103 15
4.4 24 1.590
0.5
69
51 46
Ca 8.6
Mg 2.1
Phos 3
Alb 2.2
Prot 5.5
1.2

Aspartate aminotransferase
(AST)
Used to be called SGOT (Serum glutamic oxaloacetic transaminase)
Ubiquitous enzyme in many tissues
Heart
Liver
Muscle
Kidney
Red cell
Mainly in mitochondria and cytosol

Aspartate aminotransferase
(AST)
Anthony S Tavill CWRU Professor
A hepatologist with a major interest in
iron and blood

Causes of Increased AST
Physiological: newborn 1.5 x normal
Very high levels: 20-100 x normal
myocardial infarction, viral ,ischemic, toxic hepatitis
Moderate levels:
cirrhosis, muscle disease, cholestasis, trauma, surgery, liver malignancy, hemolytic anemia
Artefact: hemolyzed blood specimen

Alanine Aminotransferase
(ALT)
Used to be called SGPT (serum glutamic-pyruvic transaminase)
High amounts in liver
Lesser amounts in muscle, kidney, and heart
Associated with cytosol
Alcoholic Liver dx: liver tissue has low levels of ALT possibly due to vitamin B6 deficiency, which is needed for ALT to function
Cirrhotic livers: possibly lower ALT

Cause of Elevated ALT & AST
Degree of Elevation Common Causes
Mild to Moderate
(41-500 U/L)
Chronic viral hepatitis (B, C, Delta, E)
Drug toxicity
Alcoholic hepatitis – often not high
Non-Alcoholic Fatty liver Disease (NAFLD) / NASH
Autoimmune hepatitis
Iron or copper accumulation
Bile duct disease
Severe (>1000 U/L) Acute viral hepatitis (A, B, C, Delta, E)
Drug induced (esp. acetominophen)
Autoimmune hepatitis
Ischemia/Hypoperfusion/ after hypotension
Heat stroke (↑ muscle enzymes CPK)
* Rarely seen in bile duct stones
Hepatocellular Injury ☻

What are the major causes of
rise in ALT & AST in the US? 1.Fatty Liver also known as Non-alcoholic
Fatty Liver Disease ( NAFLD )
ALT > AST in 30% of USA
2. Chronic Hepatitis C
Biggest risk factor: IV drug use at anytime
In both NAFLD and Hep C, liver enzymes at
times can be normal

Transaminases in Alcoholic
liver disease
Usually <300 even if severe
Extremely common for AST>ALT 2:1
ALT can be normal because ALT in alcoholic liver dx
tissue is lower than normal
As a rule: if AST>ALT, consider alcoholic liver dx
EXCEPTIONS TO RULE:
In alcoholic liver dx, rule only applies if ALT & AST are < 300
Ex. AST 1000 & ALT 500: likely liver + other organs damage
In cirrhosis of any cause, AST>ALT but ratio is usually NOT >2

Kayser-Fleischer Ring (copper)
Wilson’s disease

Lactate Dehydrogenase
(LDH)
Liver
Heart
Muscle
Kidney
Brain
Red cell
Rarely used these days

Causes of raised LDH
Degree of
Elevation
Common Causes
Mild to
Moderate
Viral hepatitis
Malignancy elsewhere
Pulmonary embolism
Severe Myocardial infarction (5 x)
– CPK, troponin used now
Blood disorders (5-20 x)

Case 1 69 y.o. ♀ homemaker of Hungarian/German ancestry
No FH of liver dx or diabetes
Lifelong abstinence from alcohol
Meds: Thyroid replacement x 40 years
Asymptomatic - normal physical exam
Lab data:
Fasting glucose 80, AST 100, ALT 120
Iron studies:
Serum iron 157 µg/dl TIBC 250 µg/dl
Iron Saturation 63% Serum ferritin 1235 mg/L

Hemochromatosis (iron)

Agenda
Tests showing liver cell injury
Tests showing hepatic function / synthesis
Tests showing cholestasis
Bilirubin metabolism
Other important liver tests
Patterns in liver injury

Tests reflecting Liver Synthesis
Tests If liver synthesis
compromised
Serum albumin Low
Prothrombin time (PT) / INR High
Bilirubin High
Plasma cholinesterase activity –
still used in Europe but not in US
Low

Problems with Serum Albumin
Half life 20 days
Decreases in advanced liver disease,
malnourished state, sepsis, proteinuria (eg.
nephrotic syndrome)
Can be lost in GI tract (eg. inflammatory
condition, enteropathy etc). Note this also
lowers globulin levels

Total protein vs serum albumin
Bulk of Total protein – albumin = globulins
Gamma globulin levels high
- common in autoimmune liver dx
Albumin and globulin levels are both low
- protein losing enteropathy
- skin exfoliation

Caput medusa

CT abdomen
Ascites

Prothrombin time (PT) / INR
Very important point for students. You do not need
to remember which factor is responsible for this and
that. Just know:
PT measures how long it takes for blood to clot
Factor VIII (8) not made in liver
Factor VII (7) half life of 6 hours
patient usually has major loss of liver function
before PT gets longer

Increased Prothrombin time (PT)
Is prolongd PT due to vitamin K deficiency or poor liver function?
Give patient 1 or 2 vitamin K shots:
If PT corrects there is vitamin K deficiency
If PT does not correct consider liver disease
Note: both can occur at same time
Vitamin K is
needed for
synthesis of
factors
2,7,9,10

Spider angiomasPalmar
erythema
GynecomastiaLeukonychia
Icterus

Agenda
Tests showing liver cell injury
Tests showing hepatic function / synthesis
Tests showing cholestasis
Bilirubin metabolism
Other important liver tests
Patterns in liver injury

Cholestasis
Term used to describe conditions where bile
flow is impeded
Lab tests showing cholestasis are typically
enzymes found around biliary cananicular
apparatus and bile ductules:
Bilirubin
Alkaline phosphatase
Gamma glutamyl transpeptidase GGTP
5-nucleotidase
Bile acids
When bile flow obstructed, these markers rise
in blood

Alkaline phosphatase
isoenzymes (Alk Phos)
Bone
Liver can be verified by doing GGT or GGTP
Kidney
Intestine
Placenta
Mammary gland
(Few labs measure heat labiality and test may not
be reliable)

Causes of raised Alk Phos
Physiological:
- until puberty x 2, last trimester pregnancy
Bone disease (normal GGTP & 5-nucleot):
- Osteomalacia (softening of the bones), paget’s disease of bone, hyperparathyroidism, bone cancer
Liver and Biliary disease (↑ GGTP):
- cholestasis, hepatitis, biliary obstruction, space occupying lesions in liver

Causes of raised Alk Phos and
normal bilirubin
Incomplete biliary obstruction
Bone disease
Infiltrating liver lesions
Placenta
Clinical Point: if liver alk phos is elevated,
do a liver imaging study (ex. ultrasound , CT
or MRI)!
• Primary or secondary
malignancy
• Granulomas
• Liver abscess
• Amyloid /other oddities
• Primary biliary cirrhosis
• Fat
Infiltrative Pattern ☻
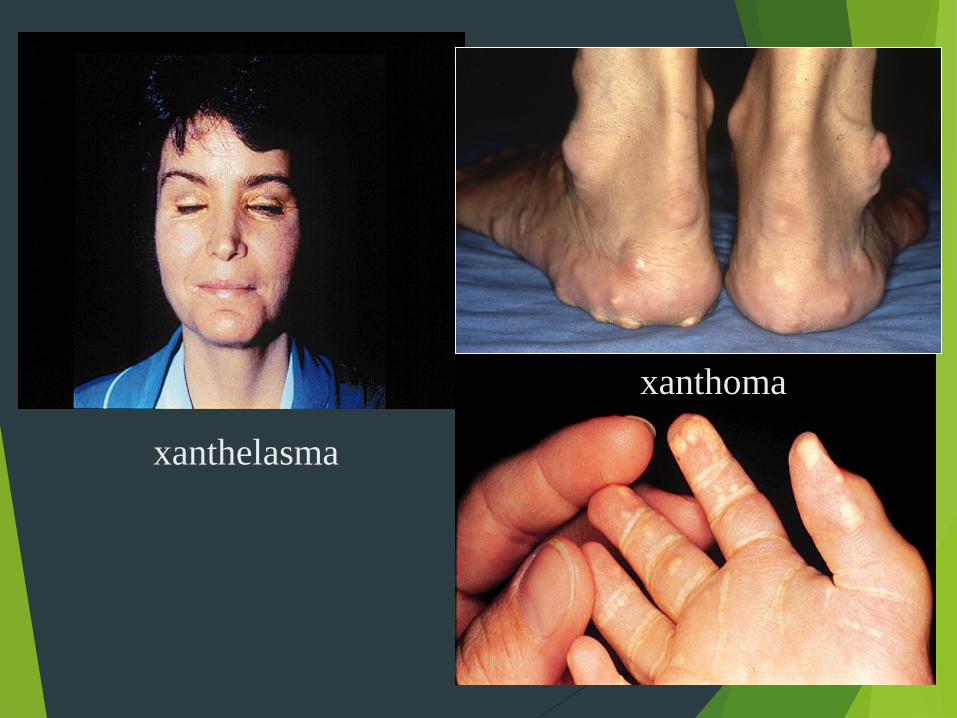
xanthelasma
xanthoma

Agenda
Tests showing liver cell injury
Tests showing hepatic function / synthesis
Tests showing cholestasis
Bilirubin metabolism
Other important liver tests
Patterns in liver injury

Bowel ← Ampulla of Vater ← Bile Ducts ← Canaliculus
bacteria
Senescent
RBCs
Heme Bilirubin
Bilirubin
Mono + Diglucuronide
RES Hepatocyte
Bilirubin +
Albumin
Circulation
UDP-
Glucuronyltransferase
UrobilinogenMRP2 transport
protein
UDP-
glucaronyl
sterocobilinogen
Urobilin
(yellow)
Stercobilin
(brown)
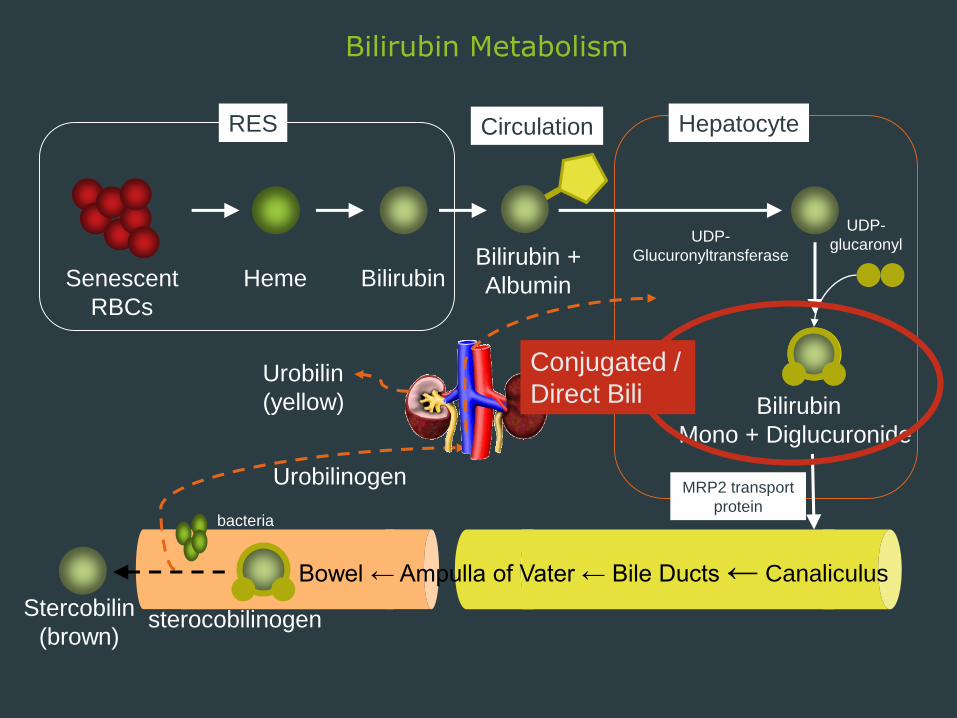
Bilirubin Metabolism

Bowel ← Ampulla of Vater ← Bile Ducts ← Canaliculus
bacteria
Senescent
RBCs
Heme Bilirubin
Bilirubin
Mono + Diglucuronide
RES Hepatocyte
Bilirubin +
Albumin
Circulation
UDP-
Glucuronyltransferase
UrobilinogenMRP2 transport
protein
UDP-
glucaronyl
Bilirubin Metabolism
sterocobilinogen
Urobilin
(yellow)
Stercobilin
(brown)
Conjugated /
Direct Bili

Bilirubin metabolism In a healthy person, ~ 250 mg of bilirubin is produced daily
Formed mostly from red cells, the rest from bone marrow ,P450
Initial breakdown in reticuloendothelial (RE) system
Unconjugated toxic bilirubin transported to liver bound to albumin
Taken up avidly by liver through bilirubin transporter
Bili is conjugated in liver with glucuronide
After conjugation, bili moves to canaliculi for transport into bile ductules (This
process is easily disturbed both across membrane and flow in ductules)
Conjugated bili flows out bile duct into intestine
About 90% bili excreted in stool as stercobilin. About 10% is converted to
urobilinogen then resorbed and excreted again (5% enterohepatic urobilinogen
cycle / 5% escapes to urine)
If no enterohepatic cycle, then no urobilinogen
When excretion compromised, conjugated bili regurgitates back to blood
Many liver disease associated with jaundice

Terms Used with Bilirubin
Total bilirubin = direct bilirubin + indirect bilirubin
Lab result given as Total and Direct bilirubin
Subtract direct from total to give indirect
Conjugated
(bound to
glucuronide)UnConjugated
Bowel ← Ampulla of Vater ← Bile Ducts ← Canaliculus
bacteria
Senescent
RBCs
Heme Bilirubin
Bilirubin
Mono + Diglucuronide
RES Hepatocyte
Bilirubin +
Albumin
Circulation
UDP-
Glucuronyltransferase
UrobilinogenMRP2 transport
protein
UDP-
glucaronyl
Bilirubin Metabolism
sterocobilinogen
Urobilin
(yellow)
Stercobilin
(brown)
Conjugated /
Direct Bili

Bowel ← Ampulla of Vater ← Bile Ducts ← Canaliculus
bacteria
Senescent
RBCs
Heme Bilirubin
Bilirubin
Mono + Diglucuronide
RES Hepatocyte
Bilirubin +
Albumin
Circulation
UDP-
Glucuronyltransferase
UrobilinogenMRP2 transport
protein
UDP-
glucaronyl
Bilirubin Metabolism and Associated Disease Targets
sterocobilinogen
Urobilin
(yellow)
Stercobilin
(brown)
Conjugated /
Direct BiliIsolated unconjugated hyperbilirubinemia:
Overproduction of bilirubin:
hemolysis
hematoma absorption
malfunctioning erythropoiesis
Defective conjugation (UDP):
Gilbert’s syndrome (<5 mg/dl)
Crigler-Najjar syndrome

Bowel ← Ampulla of Vater ← Bile Ducts ← Canaliculus
bacteria
Senescent
RBCs
Heme Bilirubin
Bilirubin
Mono + Diglucuronide
RES Hepatocyte
Bilirubin +
Albumin
Circulation
UDP-
Glucuronyltransferase
UrobilinogenMRP2 transport
protein
UDP-
glucaronyl
Bilirubin Metabolism and Associated Disease Targets
sterocobilinogen
Urobilin
(yellow)
Stercobilin
(brown)
Conjugated /
Direct Bili
Isolated conjugated hyperbilirubinemia
Problem with excretion of conjugated bili:
Defective biliary transport protein
Dubin-Johnson syndrome
Rotor syndrome

Elevated Bili and normal Alk Phos
Isolated hyperbilirubinemia☻
Type of ↑ Bili Causes
Unconjugated Overproduction of bilirubin:
- hemolysis
- hematoma absorption
- malfunctioning erythropoiesis
Defective conjugation:
- Gilbert’s syndrome (<5 mg/dl)
- Crigler-Najjar syndrome
Conjugated Problem with excretion of bili:
- Defective biliary transport protein
- Dubin-Johnson syndrome
- Rotor syndrome

Elevated Alk phos and Bili
Cholestatic Pattern ☻
Degree of Elevation Common Causes
Low ( < normal) Wilson’s Disease
Mild to Moderate Biliary obstruction (if bile duct dilated)
Hepatitis
Cirrhosis
Primary Biliary Cirrhosis
Sepsis
Medication/ Drug Toxicity
Severe (>1000 IU/L) Malignant infiltration by tumor

What patterns of liver injury
would you expect to see here?
1) Hepatocellular injury – predominately ↑ AST & ALT
2) Cholestasis – predominately ↑ alk phos & ↑ bili
3) Isolated hyperbilirubinemia – predominately ↑ bili
4) Infiltrative disease – predominately ↑ alk phos

Agenda
Tests showing liver cell injury
Tests showing hepatic function / synthesis
Tests showing cholestasis
Bilirubin metabolism
Other important liver tests
Patterns in liver injury

Other important liver tests
Alpha fetoprotein (AFP)
Ferritin, serum iron, total iron binding capacity
Ceruloplasmin for Wilson’s disease
Alpha-1-antitrypsin
Ammonia
Antimitochondrial antibody (AMA) for Primary biliary
cirrhosis (PBC)
Antinuclear antibody (ANA) for autoimmune hepatitis
Many viral antibody tests
Virus detection

Summary
Tests showing liver cell injury: AST, ALT, LDH
Tests showing hepatic function / synthesis: Albumin,
PT /INR, bilirubin
Tests showing cholestasis: Alk Phos, bilirubin
Bilirubin metabolism & associated diseases
Variety of tests to check for liver diseases
Patterns in liver injury:
1) Hepatocellular injury – predominately ↑ AST & ALT
2) Cholestasis – predominately ↑ alk phos & bili
3) Isolated hyperbilirubinemia – predominately ↑ bili
4) Infiltrative disease – predominately ↑ alk phos
In real life, patients can present with mixed patterns!

LIVER “FUNCTION” TESTS
Edith Y. Ho, M.D. M.S.
Assistant Professor of Medicine, Division of
Gastroenterology
Case Western Reserve University
Louis Stokes Cleveland VA Medical Center
Director, Inflammatory Bowel Disease Program
Co-Director, Fecal Microbiota Transplantation Program
12/17/2015
Top Related