







Languages
Pages
Legal


Annual Meeting
Late Breakers, I Activity No. 0217-0000-10-098-L01-P Monday, October 18 9:15 a.m.–10:45 a.m. Convention Center: Room 16 Moderator: LeAnn B. Norris, Pharm.D., BCPS, BCOP Clinical Assistant Professor, Department of Clinical Pharmacy and Outcomes Sciences, South Carolina College of Pharmacy, Columbia, South Carolina 9:15 a.m. Cardiovascular Therapeutics
Larisa H. Cavallari, Pharm.D., FCCP, BCPS Associate Professor, Department of Pharmacy Practice, University of Illinois at Chicago, College of Pharmacy, Chicago, Illinois
9:30 a.m. HIV Frank Romanelli, Pharm.D., MPH, BCPS Associate Dean and Associate Professor of Pharmacy, Health Sciences, and Medicine, University of Kentucky, Lexington, Kentucky
9:45 a.m. Ambulatory Care Jill S. Burkiewicz, Pharm.D., BCPS Professor of Pharmacy Practice, Midwestern University–Chicago, College of Pharmacy, Downers Grove, Illinois
10:00 a.m. Critical Care Sara D. Brouse, Pharm.D., BCPS Associate Professor, Texas Tech University of Health Sciences Center, School of Pharmacy, Dallas, Texas; Advanced Practice Pharmacist, Critical Care/Cardiology, VA North Texas Healthcare System, Dallas, Texas
10:15 a.m. Medication Safety Francesca E. Cunningham, Pharm.D. Residency Program Director, Veterans Health Administration and PBM, Center for Medication Safety, Hines, Illinois
10:30 a.m. Psychiatry Tawny B. Smith, Pharm.D. Director, Psychiatric Pharmacy Program, University of Texas, College of Pharmacy, Austin, Texas
Faculty Conflict of Interest Disclosures Sara D. Brouse: no conflicts to disclose Jill S. Burkiewicz: no conflicts to disclose Larisa H. Cavallari: no conflicts to disclose Francesca E. Cunningham: no conflicts to disclose

Annual Meeting
Frank Romanelli: no conflicts to disclose Tawny B. Smith: no conflicts to disclose Learning Objectives
1. Describe a ‘late breaking’ HIV related therapeutic report. 2. Describe limitations in the HIV-Ab response. 3. Define ‘broadly neutralizing Abs (BN Abs).’ 4. Discuss implications of newly discovered BN Abs. 5. Evaluate the clinical literature comparing dopamine versus norepinephrine for shock reversal and
apply the evidence to clinical practice in the ICU. 6. Compare/contrast the adverse effects of dopamine and norepinephrine described in the SOAP-II
trial.
Self-Assessment Questions Self-assessment questions are available online at www.accp.com/am
Frank Romanelli, Pharm.D., MPH, BCPS, AAHIVEAssociate Dean and Associate Professor of Pharmacy
University of Kentucky College of Pharmacy
ACCP FALL MEETING 2010 Late Breaking Papers - HIV
Disclosures
The presenter has no disclosures to reportregarding this presentation.
Objectives
Describe a ‘late breaking’ HIV related therapeutic report.
Describe limitations in the HIV-Ab response. Define ‘broadly neutralizing Abs (BN Abs).’ Discuss implications of newly discovered BN
Abs.
Zhou T, Georgiev I, Wu X, et al. Structuralbasis for broad and potent neutralization of
HIV-1 by antibody VRC01. Science 2010;July 8 (Epub ahead of print).
Neutralizing Antibodies A Step Forward?
Recognition that ‘early’ Abs are particularly ineffective Major impediment in vaccine development Thailand vaccine trial: 30% reduction in infection rates
(p>0.05)/vaccine abandoned Previously ‘broadly neutralizing Abs’ (BN Abs) defined by
ability to negate ~ 40% of HIV strains
Neutralizing Antibodies Structural basis for broad and potent neutralization of HIV-1 by antibody VRC01.
Long recognized that most HIV targeted Abs do not sufficiently neutralize HIV
Focus on critical Ab sites associated with minimal mutations Donor 45 (AA male with long-standing HIV): probed for BN
Abs Three unique BN Abs indentified (VRC01, VRC02, VRC03)
Zhou T, Georgiev I, Wu X, et al. Science 2010;epub:1-8.

Neutralizing Antibodies Structural basis for broad and potent neutralization of HIV-1 by antibody VRC01.
BN Abs active against an unprecedented 90% of HIV strains (notably inclusive of almost all sexually transmitted strains)
VRC01: gp120 specific, avoids confirmationally fluid areas of binding site, not affected by glycan shielding, lacks any auto-reactivity
Source of ‘elite control’?
Zhou T, Georgiev I, Wu X, et al. Science 2010;epub:1-8.
Viral Spiking
Viral Spiking
Credit: NIAID VRC
Challenges
Illicit Ab production in sufficient quantity Illicit Ab response in a timely fashion (within the
window of opportunity)
Clinical Implications
Exogenous administration of Abs (passive immunization) – perinatal transmission?
Ab infused microbicides Vaccine development (active immunization) Gene therapy
HIV Vaccine Research‘Renaissance’
Closing in on HIVs Achilles Heal?
“We are going to be at this a whole before any clinical benefits are
realized.”- Gary Nabel, MD, PhD

LATE BREAKERS, IAMBULATORY CARE
Jill S. Burkiewicz, PharmD, BCPS
Background
National Osteoporosis Foundation:1
Recommends adequate calcium intake of at least 1,200 mg daily, including supplements if necessary, for those age 50 and older
Vitamin D intake of 800-1000 international units
Consider not only impact on bone health, but overall patient health
1. NOF Clinician’s Guide: http://www.nof.org/sites/default/files/pdfs/NOF_ClinicianGuide2009_v7.pdf
Calcium &Vascular Disease:Pros Cardiovascular (CV) risk factors Calcium supplementation ↑ HDL levels1
Small, transient decreases in blood pressure2
Observational studies Inverse relationship between calcium intake and:
Ischemic stroke3
Ischemic heart disease mortality4
1. Reid IR , et al. Am J Med 2002;112:343-7.2. Reid IR, et al. J Clin Endocrinol Metab 2005;90:3824-9.
3. Iso H, et al. Stroke 1999;30:1772-9.4. Bostick RM, et al. Am J Epidemiol 1999:149:151-61.
Calcium & Vascular Disease:Cons Randomized, controlled trial with CV events
pre-specified as secondary endpoints1
Postmenopausal women randomized to calcium supplementation(citrate 1g) or placebo for 5 years Increased risk of MI (RR 2.12, 95% CI 1.01-4.47)
Supplementation acutely ↑serum calcium2
↑ serum calcium levels are a CV risk factor3
Evidence of vascular calcification in patients with renal disease on calcium supplementation4
1. Bolland MJ, et al. BMJ 2008;336:262-6.2. Reid IR Aust N Z J Med 1986:16:193-7.
3. Lind L, et al. J Clin Epidemiol 1997:50:967-73.4. Russo D, et al. Kidney Int 2007;72:1255-61.
Effect of calcium supplements on risk of myocardial infarction and cardiovascular
events: meta-analysis
Bolland MJ, Avenell A, Baron JA, et al. BMJ 2010;341:c3691.
July 29, 2010Bolland MJ, et al. BMJ 2010;341:c3691.
Study Objective & Design
Objective: To investigate whether calcium supplements
increase the risk of cardiovascular disease.
Design: Meta-analysis
Patient-level and trial-level data
Bolland MJ, et al. BMJ 2010;341:c3691.
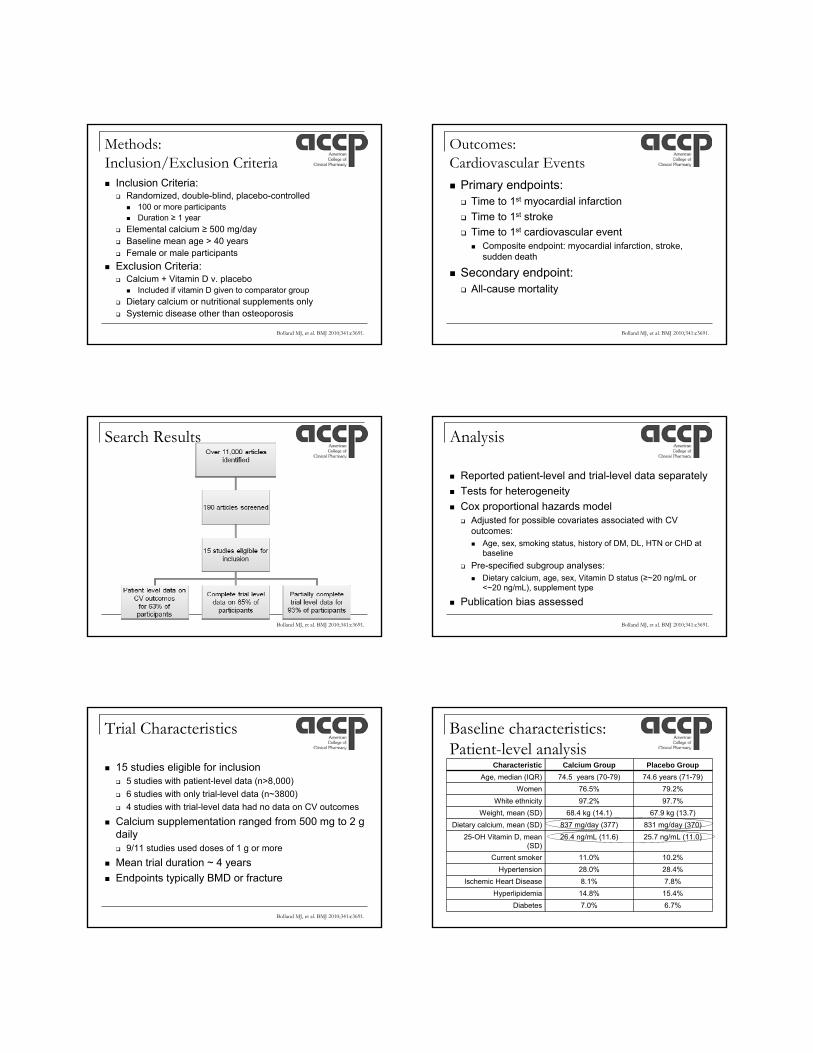
Methods: Inclusion/Exclusion Criteria Inclusion Criteria:
Randomized, double-blind, placebo-controlled 100 or more participants Duration ≥ 1 year
Elemental calcium ≥ 500 mg/day Baseline mean age > 40 years Female or male participants
Exclusion Criteria: Calcium + Vitamin D v. placebo
Included if vitamin D given to comparator group
Dietary calcium or nutritional supplements only Systemic disease other than osteoporosis
Bolland MJ, et al. BMJ 2010;341:c3691.
Outcomes: Cardiovascular Events Primary endpoints: Time to 1st myocardial infarction
Time to 1st stroke
Time to 1st cardiovascular event Composite endpoint: myocardial infarction, stroke,
sudden death
Secondary endpoint: All-cause mortality
Bolland MJ, et al. BMJ 2010;341:c3691.
Search Results
Bolland MJ, et al. BMJ 2010;341:c3691.
Analysis
Reported patient-level and trial-level data separately
Tests for heterogeneity
Cox proportional hazards model Adjusted for possible covariates associated with CV
outcomes: Age, sex, smoking status, history of DM, DL, HTN or CHD at
baseline
Pre-specified subgroup analyses: Dietary calcium, age, sex, Vitamin D status (≥~20 ng/mL or
<~20 ng/mL), supplement type
Publication bias assessed
Bolland MJ, et al. BMJ 2010;341:c3691.
Trial Characteristics
15 studies eligible for inclusion 5 studies with patient-level data (n>8,000)
6 studies with only trial-level data (n~3800)
4 studies with trial-level data had no data on CV outcomes
Calcium supplementation ranged from 500 mg to 2 g daily 9/11 studies used doses of 1 g or more
Mean trial duration ~ 4 years
Endpoints typically BMD or fracture
Baseline characteristics: Patient-level analysis
Characteristic Calcium Group Placebo Group
Age, median (IQR) 74.5 years (70-79) 74.6 years (71-79)
Women 76.5% 79.2%
White ethnicity 97.2% 97.7%
Weight, mean (SD) 68.4 kg (14.1) 67.9 kg (13.7)
Dietary calcium, mean (SD) 837 mg/day (377) 831 mg/day (370)
25-OH Vitamin D, mean (SD)
26.4 ng/mL (11.6) 25.7 ng/mL (11.0)
Current smoker 11.0% 10.2%
Hypertension 28.0% 28.4%
Ischemic Heart Disease 8.1% 7.8%
Hyperlipidemia 14.8% 15.4%
Diabetes 7.0% 6.7%

Results
Patient-level data5 studies, n=8151
HR (95% CI)
Trial-level data8 studies, n=6116
HR (95% CI)
MI 1.31 (1.02-1.67)* 1.27 (1.01-1.59)
Stroke 1.20 (0.96-1.50) 1.12 (0.92-1.36)
Composite (MI, stroke,
sudden death)
1.18 (1.00-1.39) 1.12 (0.97-1.30)
Death 1.09 (0.96-1.23) 1.07 (0.95-1.19)
*NNH=69 Bolland MJ, et al. BMJ 2010;341:c3691.
Subgroup Analysis:Dietary Calcium Intake
Dietary calcium intake Myocardial InfarctionHR (95% CI)
Above median (>805 mg/day)
1.85 (1.28-2.67)
Below median (<805 mg/day)
0.98 (0.69-1.38)
Pre-specified subgroup analysis
Bolland MJ, et al. BMJ 2010;341:c3691.
Author’s conclusions
Treatment of 1000 people with calcium for 5 years: Causes 14 additional myocardial infarctions
Prevents 26 fractures
Supplementation of calcium without coadministered vitamin D is associated with an increased risk of MI
Reconsideration of the role of calcium supplementation in prevention and treatment of osteoporosis is needed
Bolland MJ, et al. BMJ 2010;341:c3691.
Discussion: Limitations
NOF recommends adequate calcium ANDvitamin D Meta-analysis excluded studies that included
vitamin D
High dietary calcium intake
Trials did not have CV events specified as the primary endpoint
Incomplete data in 15% of participants
Vitamin D & CV Health
In observational studies, Vitamin D deficiency is associated with CV disease and multiple CV risk factors1
Women’s Health Initiative2
Coadministration of calcium 500 mg + vitamin D 200 IU BID had no effect on CHD or stroke risk
Patient population differed from current meta-analysis
1. Reddy Vanga S, et al. Am J Cardiol 2010;106:798-805.2. Hsia J, et al. Circulation 2007;115;846-854.
Clinical Applicability
Assess dietary intake of calcium and vitamin D prior to recommending supplementation
Take an active role in reducing CV risk factors for all patients

Comparison of Dopamine and Norepinephrine in the Treatment of
Shock
De Backer D., et al. N Engl J Med 2010; 362(9): 779-89
Sara Brouse, Pharm.D., FCCP, BCPS, AQ Cardiology
Associate Professor of Pharmacy Practice
Advanced Practice Pharmacist in Critical Care/Cardiology
TTUHSC School of Pharmacy/VA North Texas Medical Center
Surviving Sepsis Campaign 2008Maintain MAP ≥ 65mmHg. (1C)
Norepinephrine or Dopamine centrally administered are the initial vasopressors of choice. (1C)
Epinephrine, phenylephrine, or vasopressin should not be administered as the initial vasopressor in septic shock. (2C)
Vasopressin 0.03 units/min may be subsequently added to norepinephrineDellinger RP, Levy MM, Carlet, JM, et al: Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med 2008; 36:296 –327.
+++
++++
++++
Lefkowitz RJ, Hoffman BB, Taylor P. Neurotransmission. In: Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 9th Ed. Eds. Molinoff PB & Ruddon RW. The McGraw Hill Co. Neurotransmission. P120‐121.
++++
++++
++++
++++
0
0
+++
+++
+
++
++++
0
0
0
++ 0
Drug α1 β1 β2 DA
Dopamine (DA) +++ ++++ + ++++
Epinephrine ++++ ++++ +++ 0
Norepinephrine (NE)
++++ ++ 0 0
Isoproterenol 0 ++++ +++ 0
Dobutamine + ++++ ++ 0
Catecholamine Receptor Effects
Lefkowitz RJ, Hoffman BB, Taylor P. Neurotransmission. In: Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 9th Ed. Eds. Molinoff PB & Ruddon RW. The McGraw Hill Co. Neurotransmission. P120‐121.
Sympathetic Nerve Terminal
Lefkowitz RJ, Hoffman BB, Taylor P. Neurotransmission. In: Goodman & Gilman’s The Pharmacological Basis of Therapeutics. 9th Ed. Eds. Molinoff PB & Ruddon RW. The McGraw Hill Co. Neurotransmission. P120‐121.
Dopamine Metabolism
Riker RR et al. JAMA 2009;301(5):489‐99.
Study Group Design/Pop Dose Results
Martin et al. (n=32)
P, R studyHyperdynamic sepsis
DA 2.5‐25 g/kg/min vs NE 0.5‐5 g/kg/min
Effectiveness: DA 10 –25 g/kg/min effective in 31% (5 of 16); NE effective in 93% (15 of 16) ; Survival 17% DA vs 59% NE
Martin et al. (n=97)
P, Obs studyHyperdynamic sepsis
DA 5–15 g/kg/min If no response, DA 16 –25 g/kg/min orNE 0.5–5.0 g/kg/min
Favorable outcome: use of NE‐‐mortality 62% vs. 82% with DA or E or both (p <0.001; RR, 0.68; 95% CI 0.54–0.87)
Sakr et al.(n=3147)
Cohort, MC observational study
N=375 (35%) received DA (dosing variable)
Higher ICU mortality (DA 42.9% vs. NE 35.7%, p=.02) and hospital mortality (49.9% vs. 41.7%, p=.01)
Cochrane Rev 2004
Meta‐analysis NE vs DASeptic
Mortality RR 0.88 (0.57‐1.36)
Povoa et al. (n=897)
Cohort, MC observational studyN=458 septic shock
50.5% received DA and 73% received NE (dosing variable)
NE group had a higher hospital mortality (52% vs. 38.5%, p = 0.002)NE independent risk factor for death
Martin C, et al. Chest 1993;103:1826–1831. Martin C. Crit Care Med. 2000 Aug;28(8):2758‐65. Sakr Y. Crit Care Med. 2006 Mar;34(3):589‐97. Povoa et al. Crit Care Med. 2009 Feb;37(2):410‐6; Mullner M et al. Cochrane Database SystR 2004(3) CD003709

Study ObjectiveTo evaluate whether norepinephrine could reduce death rates in patients with shock more than dopamine
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Methods: Study DesignProspective, Double‐blind, Randomized, Multicenter trial
Study period 28 days
December 2003 to October 2007 in Belgium, Austria, & Spain
1679 Medical/Surgical ICU patients in whom a vasopressor was required for shock syndrome
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Inclusion Criteria > 18 years old
Vasopressor agent needed for treatment of shock
“Shock” defined as mean arterial pressure (MAP) less than 70mmHg or systolic blood pressure (SBP) < 100mmHg despite “adequate” fluid resuscitation and signs of tissue hypoperfusion
“Adequate” fluids defined as > 1000mL of crystalloids or 500mL of colloids
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Exclusion Criteria
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89. bpm=beats/minute
Less than 18 yrs old
Already received a vasopressor agent for > 4 hours during current shock episode
Serious arrhythmia
Atrial fibrillation with heart rate > 160 bpm
Ventricular tachycardia
Declared braindead
Methods
Riker RR et al. JAMA 2009;301(5):489‐99.
Dopamine dosed at 2mcg/kg/min & titrated by increments of 2 until max 20mcg/kg/min
Norepinephrine dosed at 0.02mcg/kg/min & titrated to max 0.19mcg/kg/min
Prior vasopressors were discontinued (if received) and transitioned to study drug
Lack of efficacy: open label norepinephrine added
Weaning: open‐label weaned 1st, then study drug
28‐day study period
De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
EndpointsPrimary endpoint
Mortality at 28 days
Secondary endpoints
ICU mortality / Hospital mortality
ICU length of stay
Number of days without need for organ support
Time to hemodynamic stability
Use of dobutamine or other inotropics
Adverse effects
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.

Statistics Estimated 765 patients/ group for 80% power to show 15% mortality difference
Predefined boundaries for early discontinuation Superiority of norepinephrine over dopamine
Superiority of dopamine over norepinephrine
No difference between dopamine or norepinephrine
1o endpoint: unadjusted chi square
2o endpoints: unpaired student’s t‐test or wilcoxon rank‐sum test
Cox proportional‐hazards regression model
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Methods: Study Design
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Baseline Characteristics DA (n=858) NE (n=821)Age 68 (55‐76) 67 (56‐76)
APACHE II Score / SOFA Score 20 (15‐28)/ 9 (7‐12) 20 (14‐27)/ 9 (6‐12)
Reason for admission, No. (%)Medical 565 (65.9%) 532 (64.8%)
Cause of Shock, No. (%)SepsisCardiogenicHypovolemicOther (intoxication, anaphylactic)
542 (63.2%)135 (15.7%)138 (16.1%)48 (5.9%)
502 (61.1%)145 (17.6%)125 (15.2%)44 (5%)
Open‐Label Norepinephrine, No. (%) 157 (18.3%) 107 (13%)
Mechanical Ventilation, No. (%)Fi02
615 (71.7%)0.59 +/‐0.24
580 (70.6%)0.58 +/‐0.23
Renal Replacement Therapy, No. (%) 63 (7.3%) 61 (7.4%)
Corticosteroids, No. (%) 101 (11.8%) 76 (9.3%)
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Results: Primary EndpointTime period
DA NE Odds Ratio (95%CI)
P-value
ICU Mortality
50.2% 45.9% 1.19 (0.98-1.44) 0.07
Hospital Mortality
59.4% 56.6% 1.12 (0.92-1.37) 0.24
28-Day Mortality
52.5% 48.5% 1.17 (0.97-1.42) 0.10
6-Month Mortality
63.8% 62.9% 1.06 (0.86-1.31) 0.71
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Results: Secondary EndpointsAchievement of MAP goal of 65 (mean +/‐ SD)
DA 6.3 ± 5.6 hrs vs NE 6 +/‐ 4.9 hrs
Support‐free days through day 28
Vasopressors: DA 11 days vs NE 12.5 days
Mech vent: DA 8.5 days vs NE 9.5 days
ICU not needed: DA 8.1 days vs NE 8.5 days
Riker RR et al. JAMA 2009;301(5):489‐99.
Results: Standard of Care Fluids
Day 1 DA received more than NE
Hydrocortisone use:
DA 344 (40.1%) vs NE 326 (39.7%)
Drotrecogin alfa use (septic shock):
DA 102 pts (18.8%) vs NE 96 pts (19.1%)
*Open‐label NE: DA 26% vs NE 20%
Riker RR et al. JAMA 2009;301(5):489‐99.

Results: Safety
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
ADRs DA, no. (%) NE, no. (%)
Atrial fibrillation 207 (20.5%) 90 (11%)
VT/VF 31 (3.6%) 12 (1.5%)
Skin ischemia 56 (6.5%) 34 (4.1%)
Arterial occlusion 23 (2.7%) 20 (2.4%)
Refractory shock 196 (46%) 155 (41%)
Forest Plot By Type of ShockHazard Ratio (95% CI)
NE Better DA Better
0.5 1.51.0
Type of Shock
HypovolemicCardiogenic
SepticAll Patients
Author’s Conclusions“Although there was no significant difference in the rate of death between patients with shock who were treated with dopamine as the first‐line vasopressor agent and those who were treated with norepinephrine, the use of dopamine was associated with a greater number of adverse events”
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
DiscussionOne of the largest studies to compare DA and NE head‐to‐head in shock syndromes
50% mortality rate consistent with norm
High external validity including multiple forms of shock syndromes
Early difference in cardiogenic shock mortality due to arrhythmias from dopamine
Riker RR et al. JAMA 2009;301(5):489‐99.
LimitationsNo mention of standard of care measures used or treatment of underlying cause ? Implemented similarly between groups
Type of shock included
Definition of “adequate administration of fluids” (1 L crystalloid, 500mL colloid)
Definition of resolution of shock ill‐defined
Definition of “Equipotent” vasopressor dose
Open‐label NE allowed (26% DA & 20% NE)
Riker RR et al. JAMA 2009;301(5):489‐99.De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
Interpretation: Does NE no longer ‘leave ‘em dead’?Data challenges consensus guideline recommendation for dopamine as 1st‐line
Minimizes perception that norepinephrine causes excessive harmful organ vasoconstriction
Implications for treatment of cardiogenic shock
Guideline change may be warranted
Consistent with SOAP 1 study
Implications for procurement & administration
De Backer D, et al. N Engl J Med 2010;362(9):779‐89.
QUESTIONS?
Top Related