






Languages
Pages
Legal

9K-wire fixation in pelvic fractures is used as a temporary measure to match the fragments and maintain the reduction before definitive fixation. Sometimes this wire is used to guide the cannulated screw at the right place.
Sacroiliac Screw Fixation in Pelvic Fracture
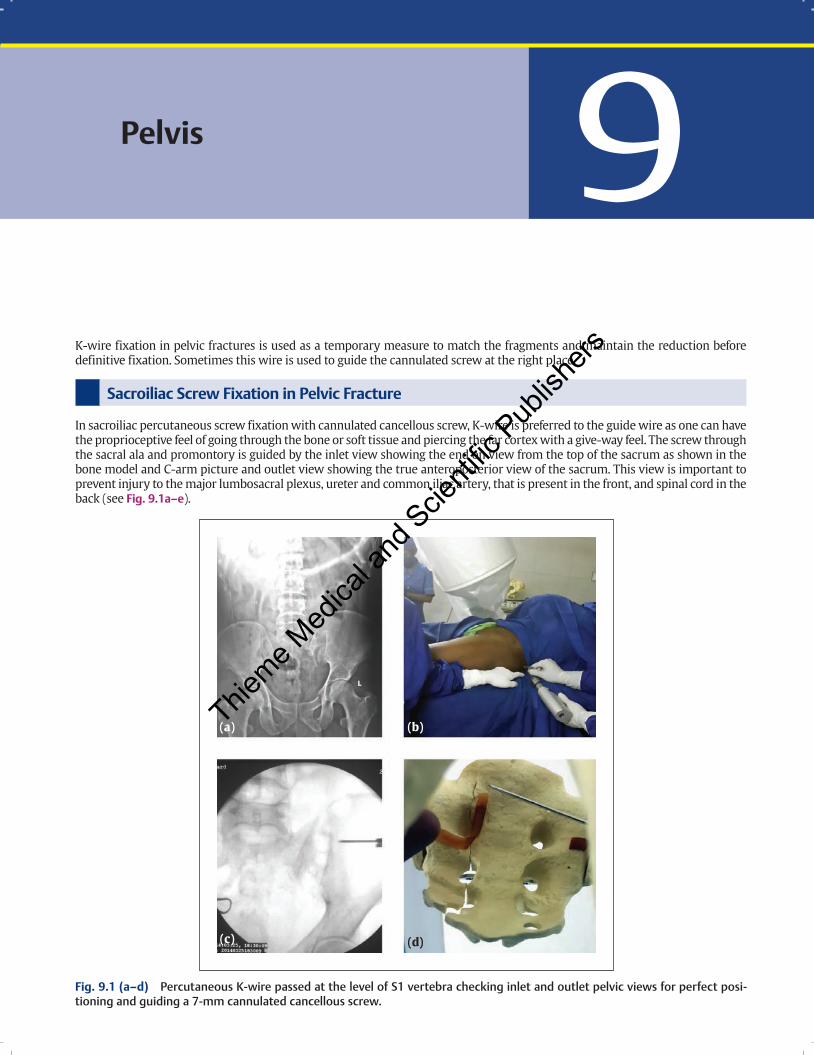
In sacroiliac percutaneous screw fixation with cannulated cancellous screw, K-wire is preferred to the guide wire as one can have the proprioceptive feel of going through the bone or soft tissue and piercing the far cortex with a give-way feel. The screw through the sacral ala and promontory is guided by the inlet view showing the end on view from the top of the sacrum as shown in the bone model and C-arm picture and outlet view showing the true anteroposterior view of the sacrum. This view is important to prevent injury to the major lumbosacral plexus, ureter and common iliac artery, that is present in the front, and spinal cord in the back (see Fig. 9.1a–e).3
Pelvis
(a) (b)
(c) (d)
Fig. 9.1 (a–d) Percutaneous K-wire passed at the level of S1 vertebra checking inlet and outlet pelvic views for perfect posi-tioning and guiding a 7-mm cannulated cancellous screw.
Thieme M
edica
l and
Scie
ntific
Pub
lishe
rs
K-Wiring: Principles and Techniques162
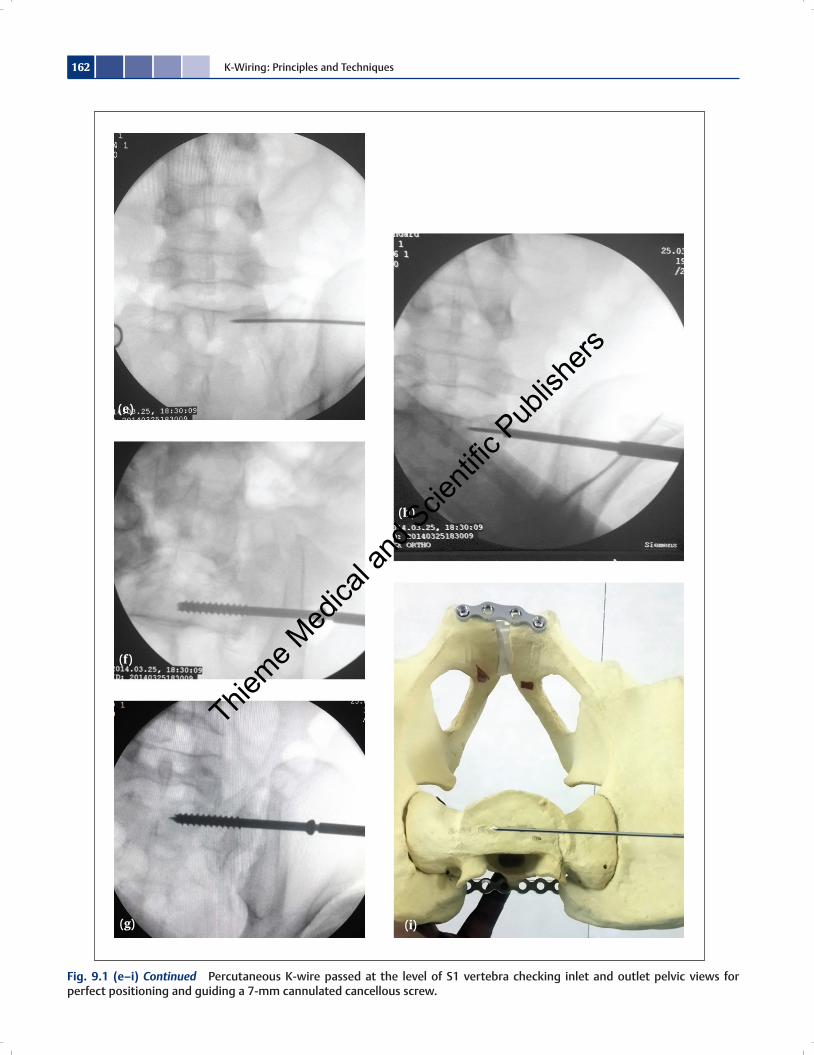
Fig. 9.1 (e–i) Continued Percutaneous K-wire passed at the level of S1 vertebra checking inlet and outlet pelvic views for perfect positioning and guiding a 7-mm cannulated cancellous screw.
(e)
(h)
(i)
(f)
(g)
Thieme M
edica
l and
Scie
ntific
Pub
lishe
rs
163Pelvis
Acetabulum Fracture
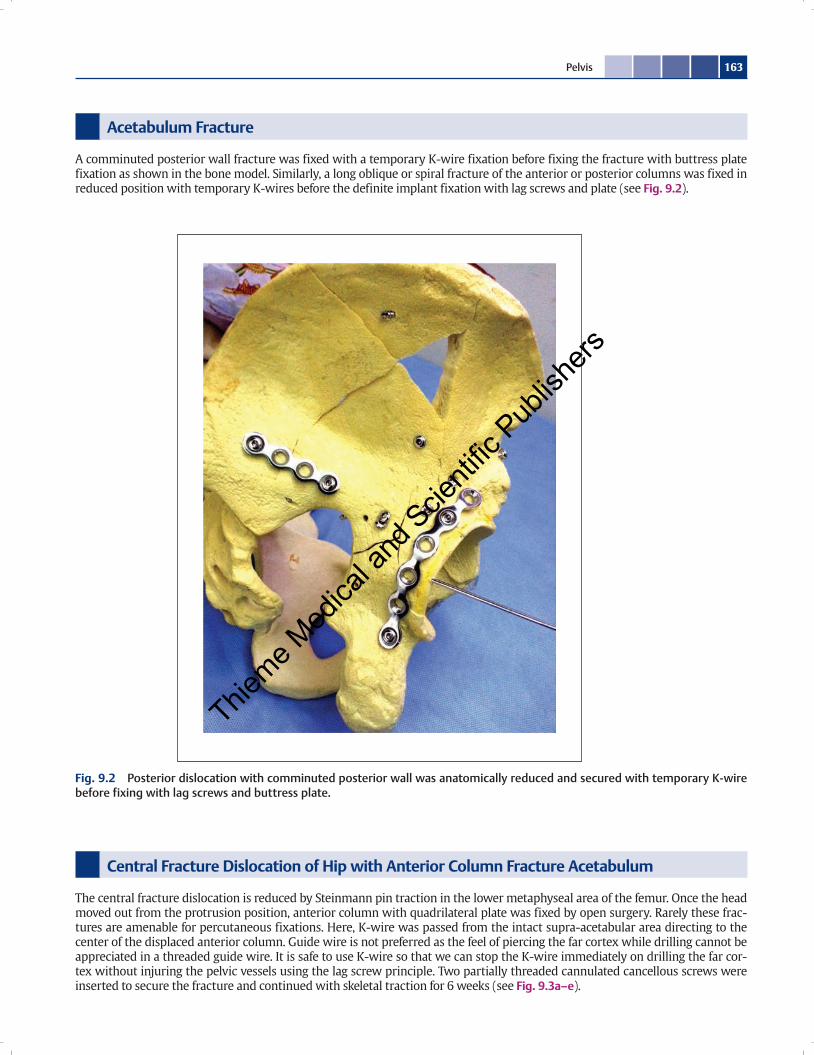
A comminuted posterior wall fracture was fixed with a temporary K-wire fixation before fixing the fracture with buttress plate fixation as shown in the bone model. Similarly, a long oblique or spiral fracture of the anterior or posterior columns was fixed in reduced position with temporary K-wires before the definite implant fixation with lag screws and plate (see Fig. 9.2).
Fig. 9.2 Posterior dislocation with comminuted posterior wall was anatomically reduced and secured with temporary K-wire before fixing with lag screws and buttress plate.
Central Fracture Dislocation of Hip with Anterior Column Fracture Acetabulum
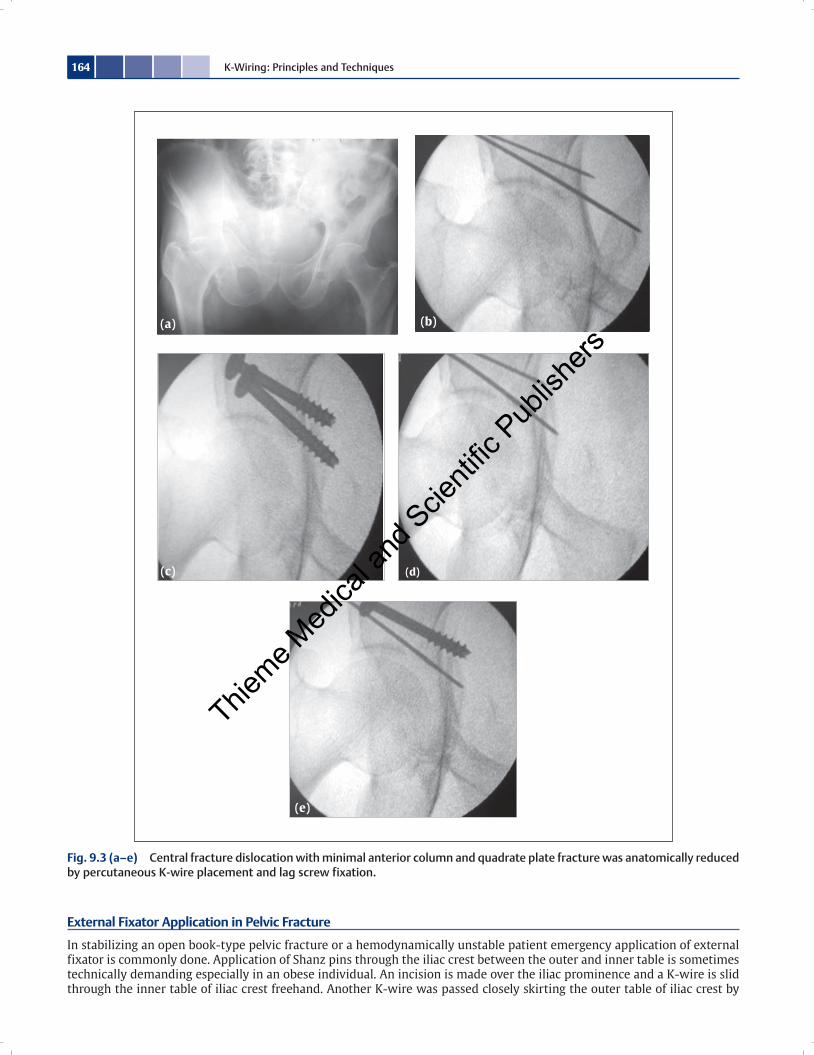
The central fracture dislocation is reduced by Steinmann pin traction in the lower metaphyseal area of the femur. Once the head moved out from the protrusion position, anterior column with quadrilateral plate was fixed by open surgery. Rarely these frac-tures are amenable for percutaneous fixations. Here, K-wire was passed from the intact supra-acetabular area directing to the center of the displaced anterior column. Guide wire is not preferred as the feel of piercing the far cortex while drilling cannot be appreciated in a threaded guide wire. It is safe to use K-wire so that we can stop the K-wire immediately on drilling the far cor-tex without injuring the pelvic vessels using the lag screw principle. Two partially threaded cannulated cancellous screws were inserted to secure the fracture and continued with skeletal traction for 6 weeks (see Fig. 9.3a–e).
Thieme M
edica
l and
Scie
ntific
Pub
lishe
rs
K-Wiring: Principles and Techniques164
External Fixator Application in Pelvic Fracture
In stabilizing an open book-type pelvic fracture or a hemodynamically unstable patient emergency application of external fixator is commonly done. Application of Shanz pins through the iliac crest between the outer and inner table is sometimes technically demanding especially in an obese individual. An incision is made over the iliac prominence and a K-wire is slid through the inner table of iliac crest freehand. Another K-wire was passed closely skirting the outer table of iliac crest by
Fig. 9.3 (a–e) Central fracture dislocation with minimal anterior column and quadrate plate fracture was anatomically reduced by percutaneous K-wire placement and lag screw fixation.
(a)
(c) (d)
(b)
(e)
Thieme M
edica
l and
Scie
ntific
Pub
lishe
rs
165Pelvis
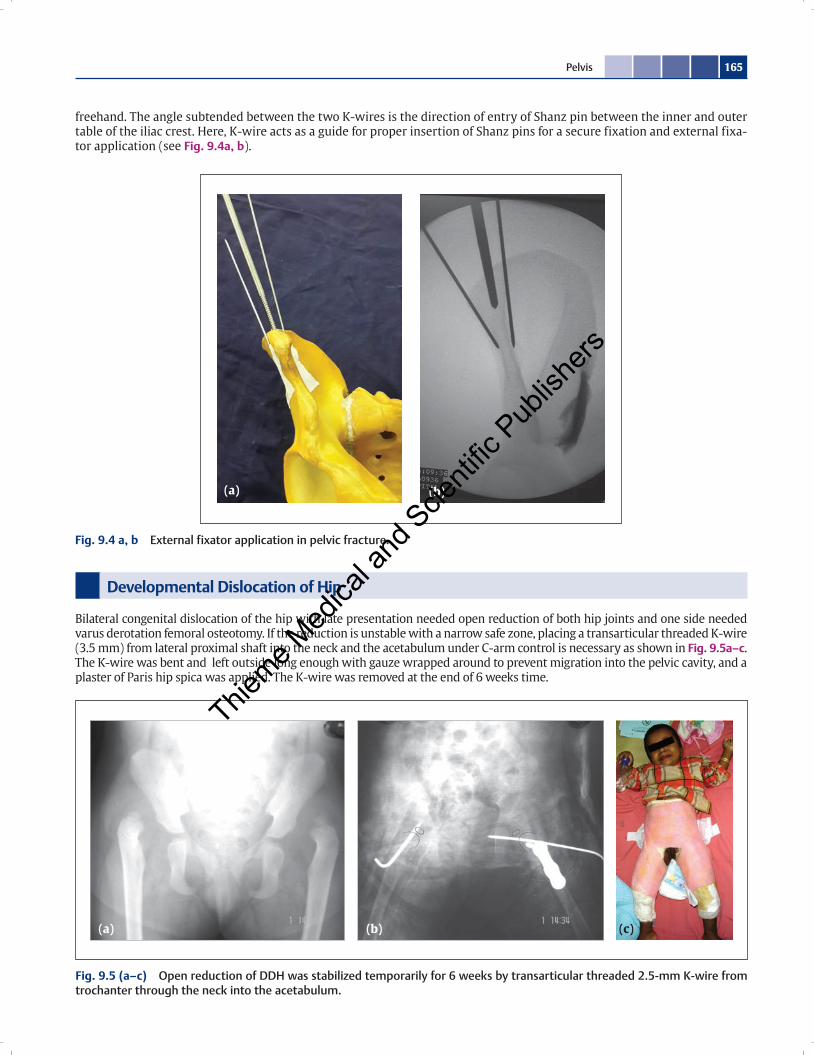
freehand. The angle subtended between the two K-wires is the direction of entry of Shanz pin between the inner and outer table of the iliac crest. Here, K-wire acts as a guide for proper insertion of Shanz pins for a secure fixation and external fixa-tor application (see Fig. 9.4a, b).
(a) (b) (c)
Fig. 9.5 (a–c) Open reduction of DDH was stabilized temporarily for 6 weeks by transarticular threaded 2.5-mm K-wire from trochanter through the neck into the acetabulum.
Developmental Dislocation of Hip
Bilateral congenital dislocation of the hip with late presentation needed open reduction of both hip joints and one side needed varus derotation femoral osteotomy. If the reduction is unstable with a narrow safe zone, placing a transarticular threaded K-wire (3.5 mm) from lateral proximal shaft into the neck and the acetabulum under C-arm control is necessary as shown in Fig. 9.5a–c. The K-wire was bent and left outside long enough with gauze wrapped around to prevent migration into the pelvic cavity, and a plaster of Paris hip spica was applied. The K-wire was removed at the end of 6 weeks time.
(a) (b)
Fig. 9.4 a, b External fixator application in pelvic fracture.
Thieme M
edica
l and
Scie
ntific
Pub
lishe
rs
Thieme M
edica
l and
Scie
ntific
Pub
lishe
rs
Top Related