







Languages
Pages
Legal

ICCS e-Newsletter CSI Spring 2013
David A Westerman, MBBS FRACP FRCPA
Department of Pathology
Peter MacCallum Cancer Centre
Melbourne, Australia
e-CSI - Clinical History:
• A 52 year Caucasian man presents with pancytopenia for investigation, and a previous history of “T cell lymphoma”.

e-CSI - Peripheral Blood:
• CBCNormal Range– WBC: 0.5 x 109/l (4.0 – 11.0)– RBC: 2.86 x 1012/l (4.5 – 6.5)– Hgb: 9.0 g/dl (13.0 – 18.0)– Hct: 27.0 % (40.0 –
54.0)– MCV: 95.0 fl (80.0 – 96.0)– MCH: 32.0 pg (27.0 – 32.0)– MCHC: 32.9 g/dl (31.0 –
35.0)– RDW: 17.2% (11.7 – 15.7)– Plts: 25 x 109/l (150 – 400)

e-CSI - Peripheral Blood:
• CBC Differential – Granulocytes: 75%– Lymphocytes: 9%– Monocytes: 11% – Eosinophils: 2%
e-CSI - Clinical History:
• Bone marrow aspirate and trephine biopsy were performed.
• Flow cytometric immunophenotyping was performed on the bone marrow aspirate and the results from selected 8-color tubes are provided for review.

e-CSI - Flow Cytometric Studies:
• Acquired FACS Canto II, analyzed with Kaluza
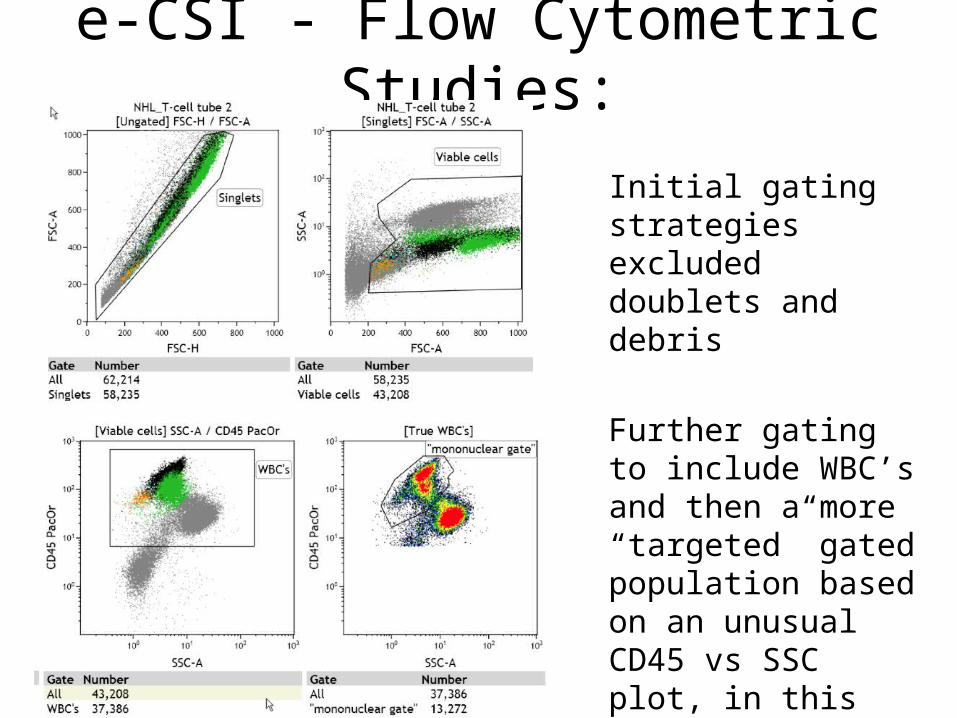
e-CSI - Flow Cytometric Studies:
Initial gating strategies excluded doublets and debris
Further gating to include WBC’s and then a more “targeted” gated population based on an unusual CD45 vs SSC plot, in this case – “mononuclear gate”

e-CSI - Flow Cytometric Studies:
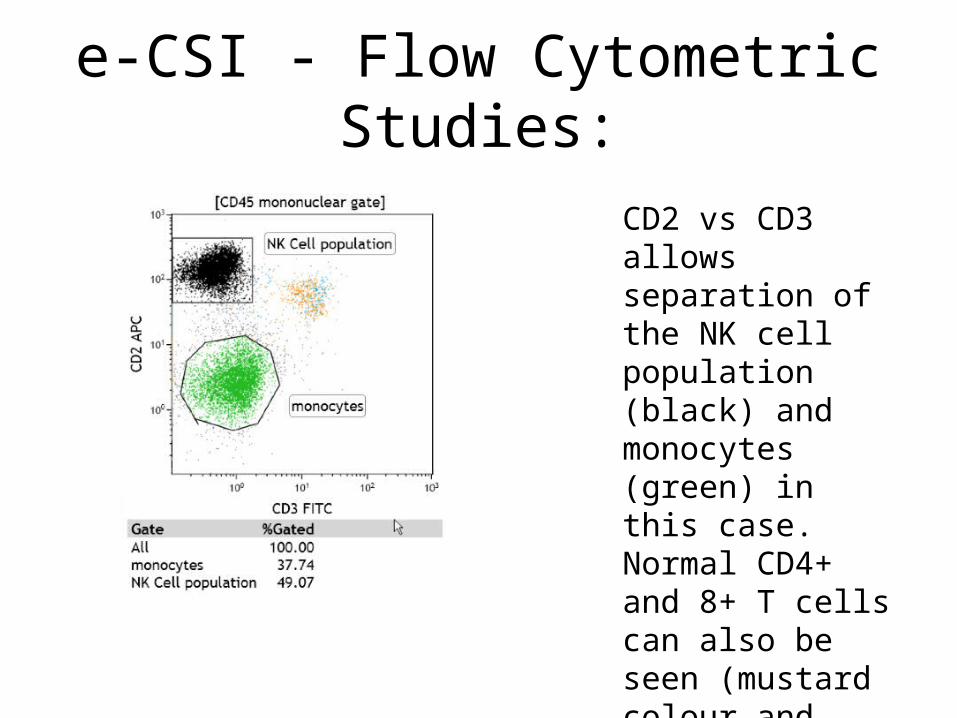
56% of mononuclear cells gated are CD2+, while T cells account for only 4%
An expanded monocytic population is also identified with weak (but normal) CD4 expression (green)
e-CSI - Flow Cytometric Studies:
CD2 vs CD3 allows separation of the NK cell population (black) and monocytes (green) in this case.Normal CD4+ and 8+ T cells can also be seen (mustard colour and blue)
e-CSI - Flow Cytometric Studies:
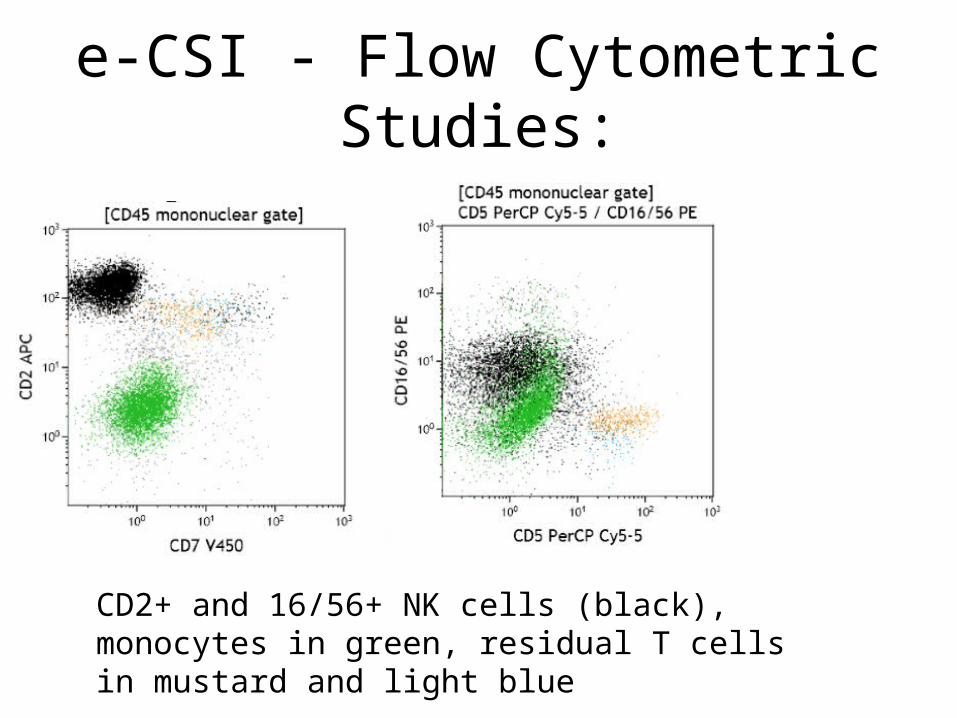
CD2+ and 16/56+ NK cells (black), monocytes in green, residual T cells in mustard and light blue
e-CSI - Flow Cytometric Studies:
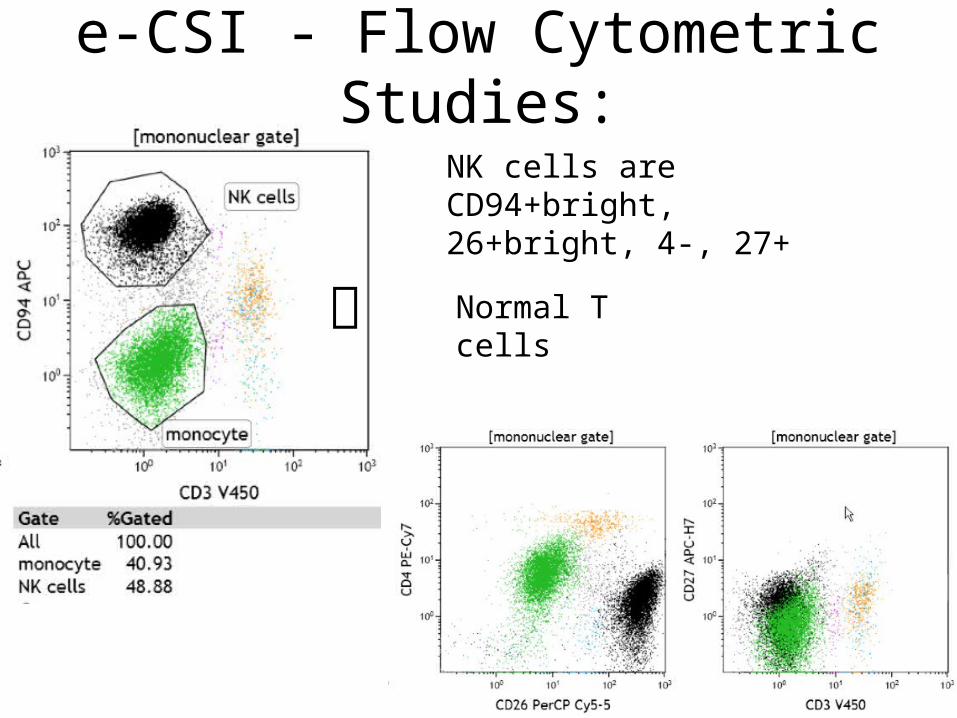
NK cells are CD94+bright, 26+bright, 4-, 27+
Normal T cells
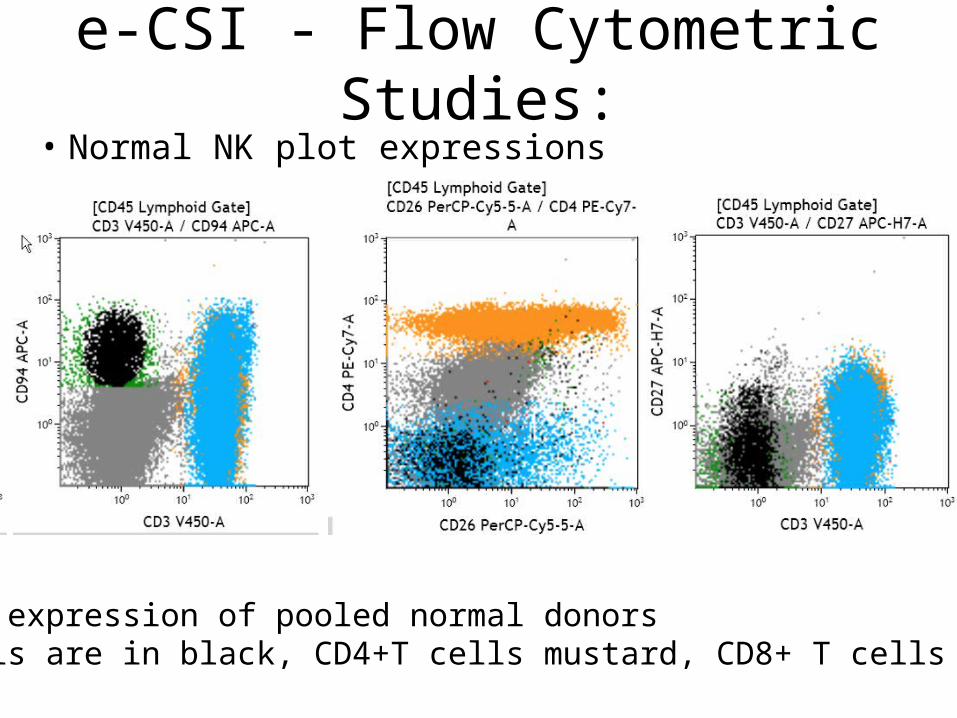
e-CSI - Flow Cytometric Studies:• Normal NK plot expressions
Normal expression of pooled normal donorsNK cells are in black, CD4+T cells mustard, CD8+ T cells in blue

e-CSI - Flow Cytometric Conclusion:
1. NK cells 56% of mononuclear gate expressing: CD2+, 3-, 4-, 5 partial, 7-, 8-, 16/56+, 26+ bright, 27-, 94+ bright, TCR αβ- & γδ-
2. Monocytes –normal expression compared to controls with this panel of markers but expanded in number
e-CSI – cont.
• Correlation with morphology and subsequently immunohistochemistry was performed
e-CSI – morphology
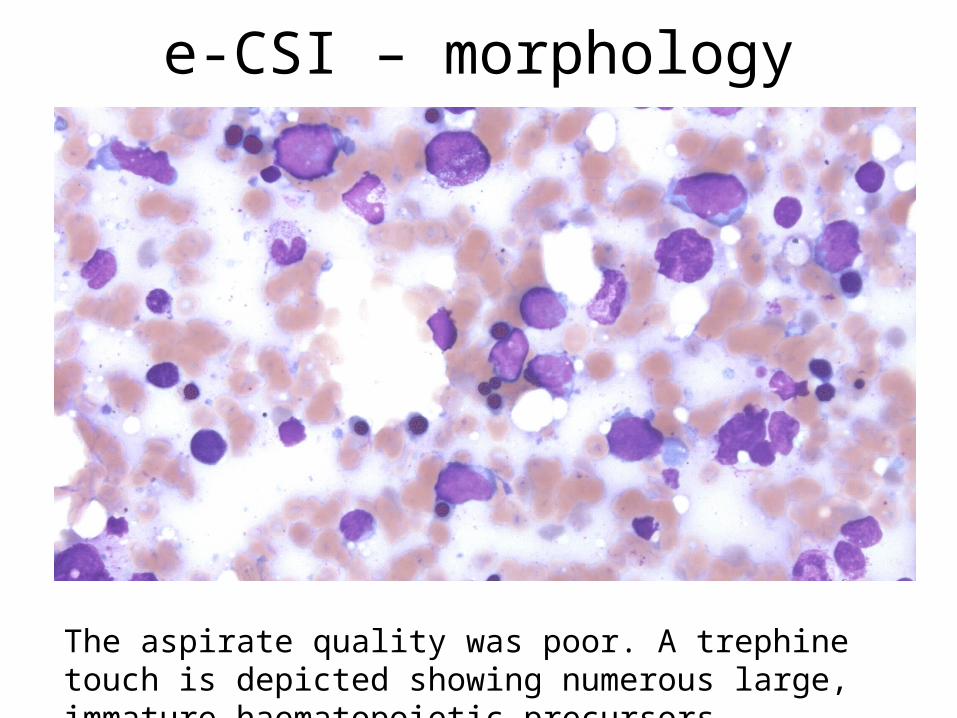
The aspirate quality was poor. A trephine touch is depicted showing numerous large, immature haematopoietic precursors
e-CSI – morphology
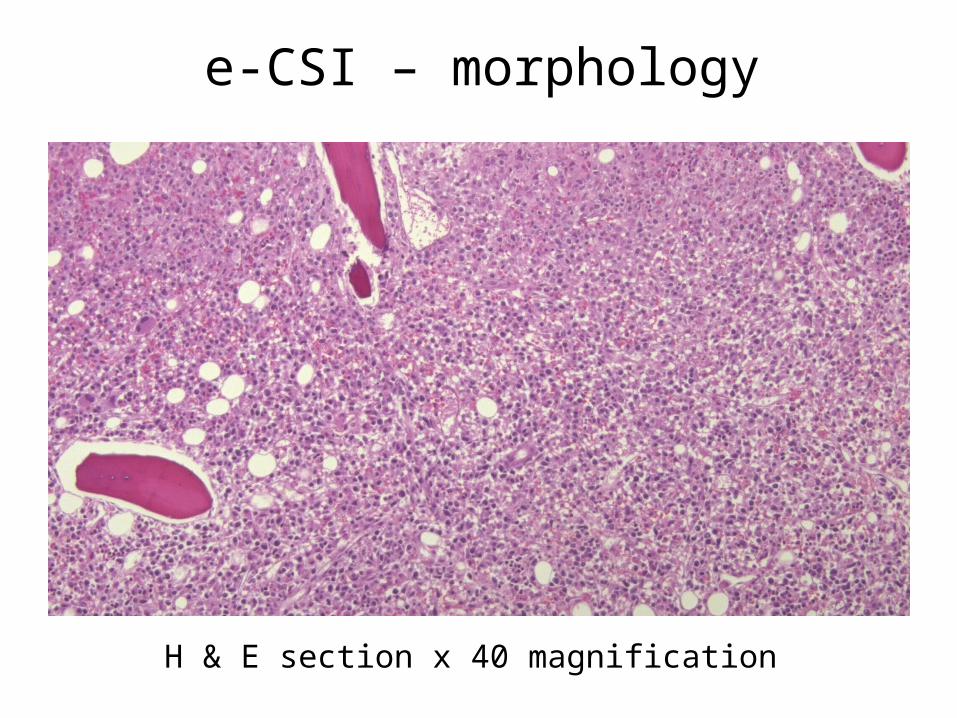
H & E section x 40 magnification

e-CSI – morphology
H & E section x 200 magnification; Effacement by an undifferentiated population of large blast-like cells

e-CSI – morphology
CD2 demonstrates a dominant positive population, including mitotic figures

CD3 shows cytoplasmic staining, in keeping with staining of CD3 epsilon chains of NK cells
e-CSI – morphology

e-CSI – morphology
TIA shows a significant positive population, while some granzyme positivity was also seen (not shown), in keeping with the cytotoxic function of NK cells
e-CSI – morphology
• EBV ISH is not a validated in our mercuric chloride fixed trephines, so was not tested
• TP53 IHC (not shown) showed positivity in about 20% of cells
• Insufficient material was available for cytogenetics
• TCR gene rearrangement studies were polyclonal

e-CSI – Diagnosis
• Aggressive NK-cell leukaemia• Reactive monocytosis
e-CSI – Aggressive NK-cell leukaemia
• This is a rare disorder with a preponderance in Asian and South American populations, and young to middle aged
• There is a strong association with EBV• Patients present with fever, cytopenias,
constitutional symptoms, leukaemic cells, DIC, or haemophagocytic syndrome. Skin involvement is uncommon
e-CSI – Aggressive NK-cell leukaemia
• Morphologically: NK cells in this disorder vary from typical large granular lymphocyte morphology to atypical forms with folded nuclei, and nucleoli to frank blasts
• The typical phenotype is CD2+ CD3- CD3ε+ CD56+ CD57- CD16+ CD11b+
• FAS ligand (CD95) is found on neoplastic cells, and also in the serum
• T cell receptor genes are germline

e-CSI – Aggressive NK-cell leukaemia
• >90% cases are EBV positive• Karyotypic anomalies vary and include 11q,
6q, 17p deletions• The prognosis is poor and median survival
measureable in just a few months• Typically the disease is refractory to aggressive
chemotherapy

e-CSI – References• Chan JKC, Jaffe ES, Ralfkiaer E et al. WHO Classification of Tumours
of Haematopoietic and Lymphoid Tissues. 4TH edition, pp276-277.• Dearden CE, Johnson R, Pettengell R et al. Guidelines for the
management of mature T-cell and NK-cell neoplasms (excluding cutaneous T-cell lymphoma). Br J Haematol 2011; 153, 451–485.
• Kawa-Ha K, Ishihara S, Ninomiya T et al. CD3-negative lymphoproliferative disease of granular lymphocytes containing Epstein-Barr viral DNA. J Clin Inves 1989; 84: 51-55.
• Kwong YL, The Diagnosis & management of extranodal NK/T cell lymphoma, nasal-type and aggreesive NK-cell leukemia. J Clin Exp Hematopath. 2011; 51: 21-27.
• Suzuki R, Suzumiya J, Nakamura S et al. Aggressive natural killer-cell leukemia revisited: large granular lymphocyte leukemia of cytotoxic NK cells. Leukemia 2004; 18: 763–770.
Top Related