







Languages
Pages
Legal


Hperlipidemia:- Treatment Hperlipidemia:- Treatment and Managementand Management
Presented by:-Presented by:-
Dr. TewariDr. Tewari
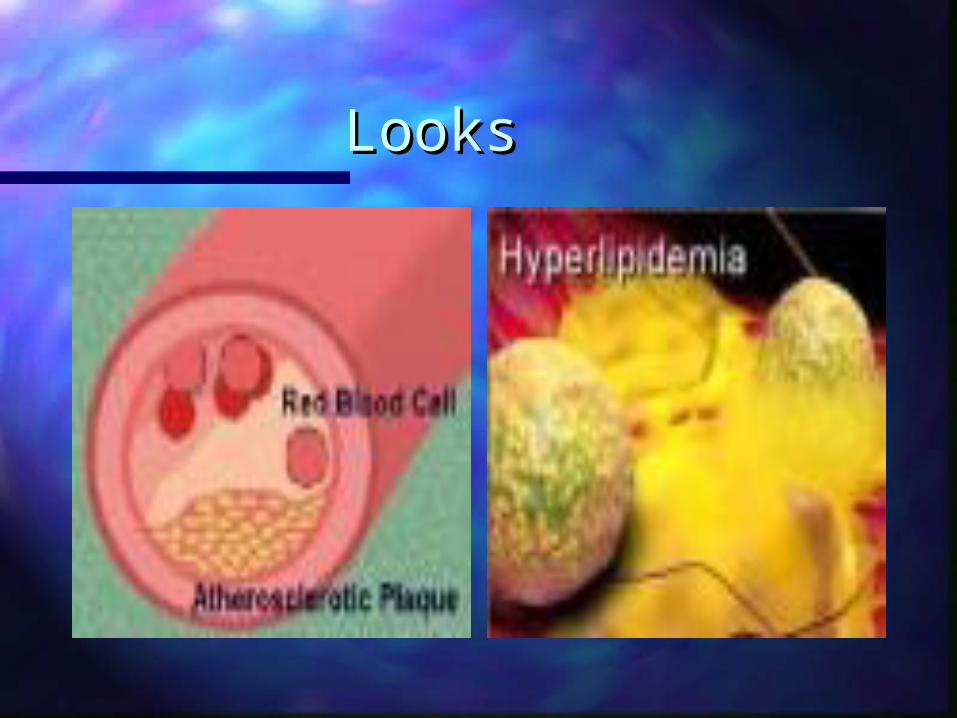
LooksLooks

Hyperlipidemia is a risk factor for accelerated vascular disease.
It is a major modifiable risk factor for coronary artery disease,
cerebrovascular disease, and peripheral vascular disease.
The most aggressive treatment of elevated lipids should be reserved
for those patients at highest risk for vascular disease:
Patients with a documented history of coronary artery disease,
cerebrovascular disease, or peripheral vascular disease.
Patients with a history of diabetes or hypertension.
Patients with an LDL-C level above 160 mg/dL.
Patients with elevated triglycerides, low levels of HDL cholesterol,
and those who smoke.

Screening recommendations for the general population are:
Every 5 years for males age 35-65
Every 5 years for females age 45-65.
Screening for adults under age 35 and over age 65 should
generally be limited to those with risk factors for
vascular disease which include:
Family history
of premature vascular disease<50 male, <60 female)
Smoking
Hypertension
Diabetes
Documented vascular disease

Elevated cholesterol levels are generally classified as:
Desirable: TC<200 mg/dL, HDL>35 mg/dL, LDL<130
Borderline: TC 200-239, HDL>35 mg/dL, LDL 131-160,
and fewer than 2 risk factors and without vascular disease
High: presence of vascular disease and LDL>160 or
TC>240 mg/dL or HDL <35 mg/dL, or 2 or more risk factors.
An additional factor to consider is the
total cholesterol/HDL ratio. The goal is to keep the ratio
below 5:1; the optimum ratio is 3.5:1.

Treatment
Step 1: Provide information on dietary modification,
physical activity, and risk factor reduction.
Diet should generally consist of =<30% fat,
<8-10% saturated fat, <300 mg/d cholesterol.
Step 2: Provide information on dietary modification,
physical activity, and risk factor reduction.
Diet should generally consist of =<30% fat,
<7% saturated fat, <200 mg/d cholesterol.

Patients who fail maximal diet therapy may be candidates for
drug therapy
Risk Category
Without CHD and with fewer than two risk factors
Goal LDL
< 160 mg/dL
Without CHD and with two or more risk factors < 130 mg/dL
With CHD <_100 mg/dL

TABLE 1Determining Patient-Specific LDL Goals Through Risk Factors
Risk-factor score*
† Age: men > 45 years; women >55 years or
postmenopausal without ERTCurrent smokerHypertensionDiabetesCHD in first-degree relative (male relative <55 years;
female relative <65 years)HDL <35 mg per dL (0.9 mmol per L);
subtract 1 risk factor if HDL >60 mg per dL

LDL goal, by risk-factor score†
0 to 1 point: <160 mg per dL (<4.15 mmol per L)2 or more points: <130 mg per dL (<3.35 mmol per L)Patients with history of CHD: <100 mg per dL (<2.60 mmol per L)

Medication Selection
The drugs of first choice for elevated LDL cholesterol are
the bile acid sequestrants (cholestyramine, colestipol)
and nicotinic acid (niacin). These medications are effective
and have no serious side effects. They can have troublesome
side effects requiring member education to improve
compliance. Niacin is preferred in the presence of elevated
triglycerides (exceeding 250 mg/dL). Bile acid sequestrants
should not be used as a single agent in the presence of
elevated triglycerides.

HMG CoA reductase inhibitors (lovastatin, pravastatin,
fluvastatin, and simvastatin) are very effective for lowering LDL levels
in patients who do not tolerate or respond to the first line agents
of choice.
Fibrates (Gemfibrazil and clofibrate) have moderate effects on
LDL levels but are more effective in lowering elevated triglycerides.
Combination therapy may be used on high risk patients who fail
to respond to diet and single agent medication regimens. Combining a
bile acid sequestrant with either nicotinic acid or an
HMG CoA reductase inhibitor can markedly lower LDL levels

As a group, statins decrease total and LDL cholesterol levels
All statins have a minimal effect in raising HDL levels
Atorvastatin is the most effective in reducing LDL
However, unlike the more extensively studied agents
(e.g., pravastatin, simvastatin), atorvastatin has not been proved to
reduce total morbidity and mortality.
The most common adverse effects of the statins are
gastrointestinal disturbances, headache, myalgias and rash.
STATINS

Monitoring
The patient should take the statin for at least four weeks before
repeating lipid level tests. Recheck lipid levels in three months
Muscle aches are the statins' most feared adverse effect

Niacin (Nicotinic Acid)
Niacin is the oldest lipid-lowering agent that has been proved to
decrease cardiovascular morbidity and total mortality
It reduces serum triglyceride, total cholesterol and
LDL cholesterol values
It also has the beneficial effect of raising HDL levels.
An extended-release form of niacin (Niaspan) has the same
beneficial lipid-altering effects as standard niacinAlthough less effective than the statins in decreasing LDL levels,
ER niacin can increase HDL values by 20 percent, decrease triglyceride
levels by 25 percent

Adverse Effects
Flushing is the most common side effect
Abdominal pain, nausea and vomiting (all less than 8 percent
Avoid concomitant ingestion of alcohol or hot beverages
Patients who take extended-release niacin tend to have
fewer adverse effects than those who use standard
niacin preparations

Monitoring
Periodic liver function tests are mandatory
Every 12 weeks for the first year and then every six months
May promote glucose intolerance
Can also increase uric acid levels

TABLE 7National Cholesterol Education Program (NCEP) Guidelines:
Serum Triglyceride Action Limits
Triglyceride value Intervention
<200 mg per dL Normal value.
Some recommend a lower
normal value of 150 mg per dL
200 to 400 mg per L Primary treatment
is lifestyle modification:
weight control, low-fat, low-cholesterol diet, regular exercise,
smoking cessation and (in selected patients) alcohol restriction.
Medication may be considered in patients with established CHD,
family history of premature CHD, concomitant total

total cholesterol level of >=240 mg per dL and HDL
value of <35 mg per dL, genetic form of hypertriglyceridemia
(e.g., dysbetalipoproteinemia or familial combined hyperlipidemia)
or multiple risk factors.
400 to 1,000 mg per dL Treatment as in previous category
but with an emphasis on controlling
causes of secondary
hypertriglyceridemia. Medication is
recommended by some authorities and
certainly should be used if the patient has
a history of acute pancreatitis.
>1,000 mg per dL Vigorous triglyceride-lowering efforts
are required because of increased risk for
pancreatitis. Treat causes of secondary
hypertriglyceridemia (e.g., diabetes mellitus).
Institute very-low-fat diet, curtail alcohol;
if triglyceride level of <1,000 mg per dL is not
achieved, use medications.

Fibrates are used to treat hypertriglyceridemia.
This class of drugs includes clofibrate (Atromid-S), gemfibrozil (Lopid)
and fenofibrate (Tricor)
Fibric Acid Derivatives (Fibrates
Medication is generally not used to treat hypertriglyceridemia unless
fasting serum triglyceride levels are greater than 400 mg per dL
Fibrates decrease triglyceride values by 20 to 45 percent and increase
HDL levels by 7 to 15 percent.

Adverse Effects
Gastrointestinal intolerance (abdominal pain, nausea, vomiting,
diarrhea, constipation, dyspepsia) is the most common adverse effect
associated with fibrate therapy
Neuromuscular (headache, dizziness, vertigo, arthralgias) and
dermatologic reactions
Incidence of myalgias and rhabdomyolysis increases with
concomitant use of a statin
Gemfibrozil has been associated with cholelithiasis in 1 percent
of the patients
Fibrates increase gallbladder and hepatic cholesterol concentrations

Bile Acid Sequestrants
Cholestyramine (LoCholest) and colestipol (Colestid) are the two
bile acid sequestrants currently available
These agents lower LDL (20 percent) and raise HDL (5 percent).
Maximal therapeutic effect is evident after one month of therapy.

Adverse Effects
Gastrointestinal disturbances
Interfere with intestinal absorption of various vitamins and minerals
Decrease the absorption of numerous medications, including
levothyroxine, penicillin, propranolol, thiazide diuretics and digoxin

Combination regimens should be considered for use in patients
who fail to meet target values and are compliant with their current therapy
Myopathy and rhabdomyolysis are serious concerns when statins
are combined with fibrates or niacin
Compliance with bile acid sequestrants is a problem
The statins have the best compliance or maintenance rates, followed by
niacin, gemfibrozil and bile acid sequestrants

Combination therapy increases the likelihood of reaching target values,
but poor compliance is a variable that can foil even the most aggressive
therapeutic interventions.


mdchoice.com/cholesterol/ interactive_case.gif
Top Related