






Languages
Pages
Legal


Lorenzo Fornaro, MD Unit of Medical Oncology 2
Azienda Ospedaliero-Universitaria Pisana Istituto Toscano Tumori
Pisa- Italy
Highlights STOMACH CANCER
UPDATES and NEWS from the Gastrointestinal
Cancers Symposium in San Francisco
Roma, 10-11 Febbraio 2017
Agenda
• Palliation of gastric outlet obstruction: surgery or not?
• Pretreated metastatic GC: confirmations (good or not)
• Immunotherapy: a seismic shift in metastatic GC?
• Conclusions
Agenda
• Palliation of gastric outlet obstruction: surgery or not?
• Pretreated metastatic GC: confirmations (good or not)
• Immunotherapy: a seismic shift in metastatic GC?
• Conclusions
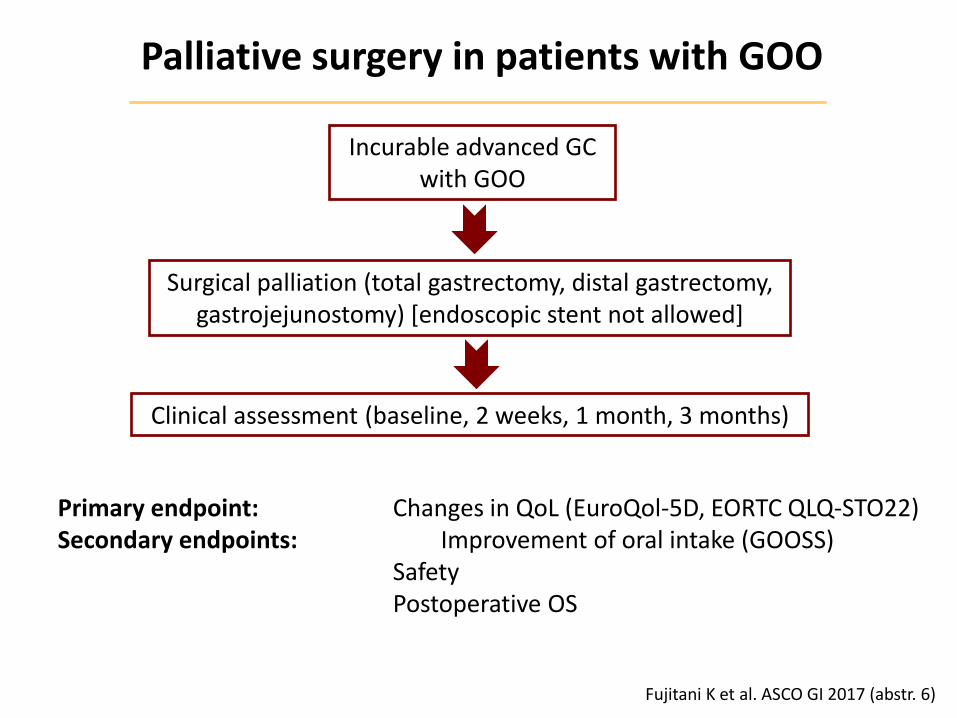
Palliative surgery in patients with GOO
Fujitani K et al. ASCO GI 2017 (abstr. 6)
Incurable advanced GC with GOO
Surgical palliation (total gastrectomy, distal gastrectomy, gastrojejunostomy) [endoscopic stent not allowed]
Clinical assessment (baseline, 2 weeks, 1 month, 3 months)
Primary endpoint: Changes in QoL (EuroQol-5D, EORTC QLQ-STO22) Secondary endpoints: Improvement of oral intake (GOOSS) Safety Postoperative OS
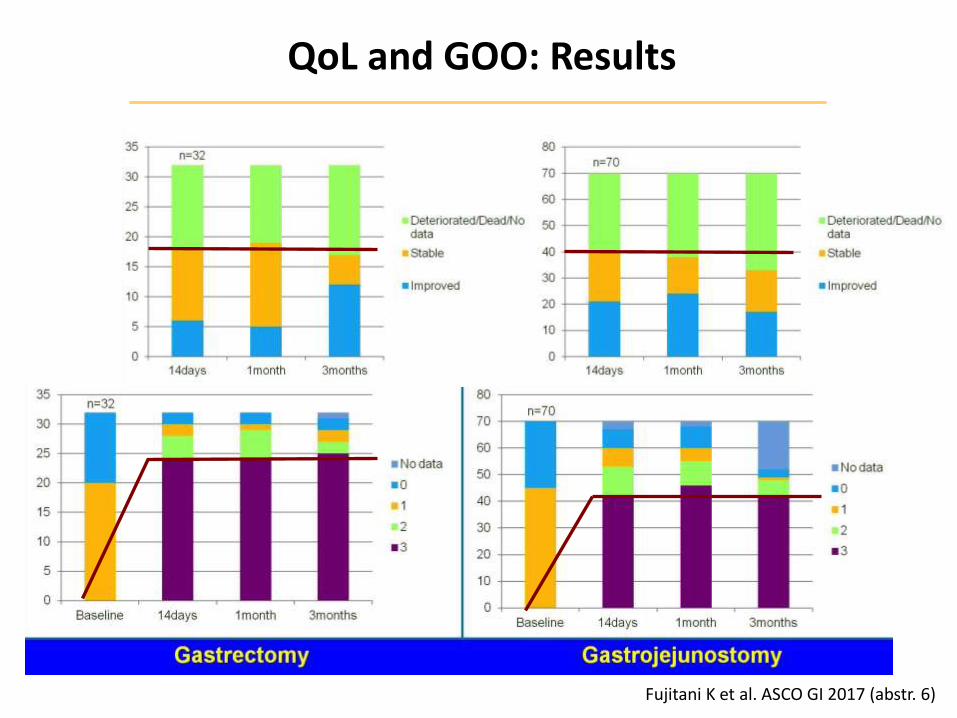
QoL and GOO: Results
Fujitani K et al. ASCO GI 2017 (abstr. 6)
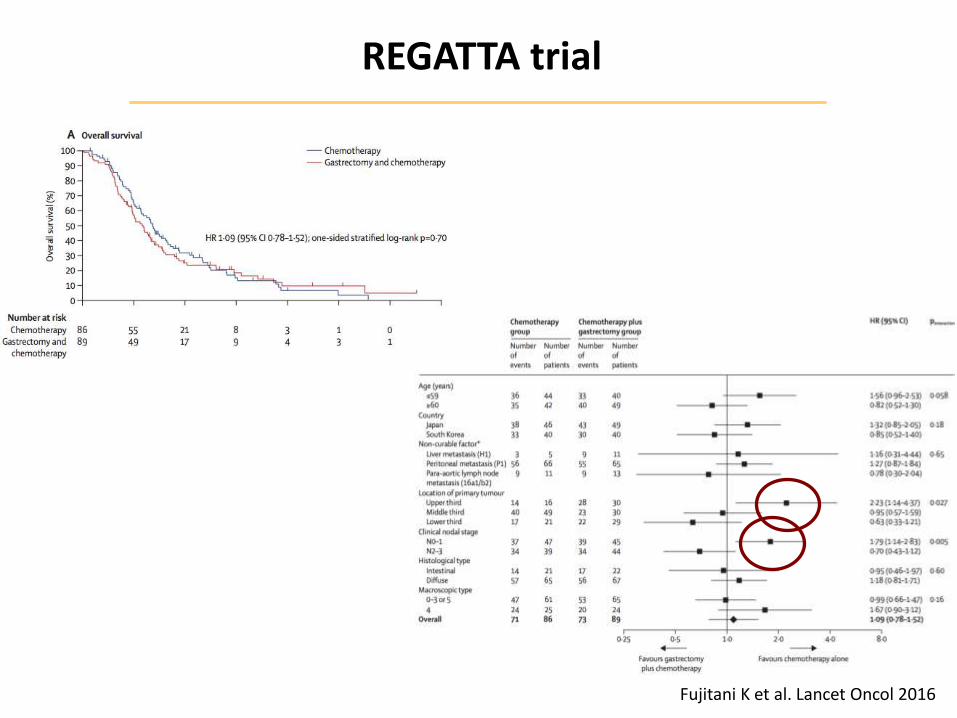
REGATTA trial
Fujitani K et al. Lancet Oncol 2016
Surgery for all patients with GOO?
• Improvements in systemic therapy
1st-line CT improves OS and QoL (RR: 35%-40%)
• Early nutritional support
Endoscopic stent: lower risks and costs, immediate recovery
• No data about long-term outcome
Selection of patients with better outcome?
• No data about CT regimens
Is CT-first reasonable after careful prognostic evaluation?
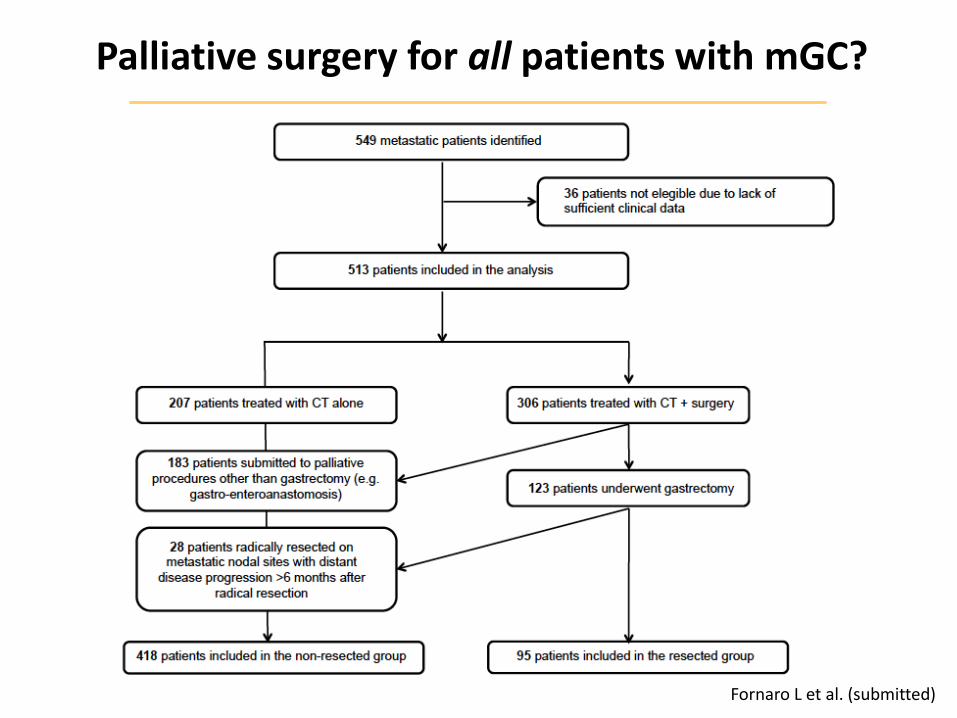
Palliative surgery for all patients with mGC?
Fornaro L et al. (submitted)
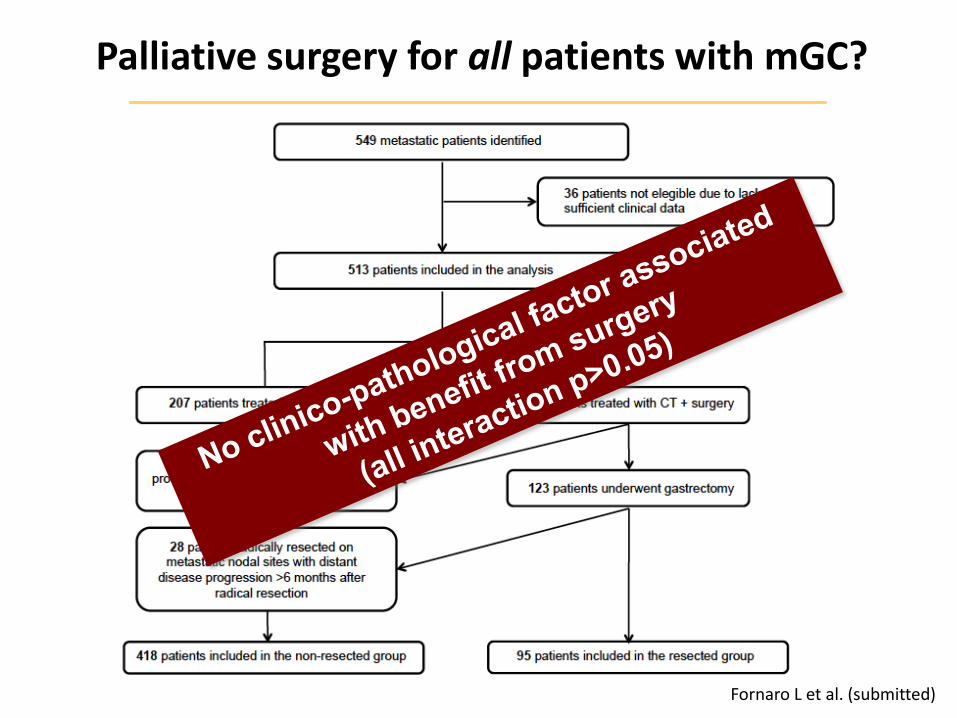
Palliative surgery for all patients with mGC?
Fornaro L et al. (submitted)
Agenda
• Palliation of gastric outlet obstruction: surgery or not?
• Pretreated metastatic GC: confirmations (good or not)
• Immunotherapy: a seismic shift in metastatic GC?
• Conclusions
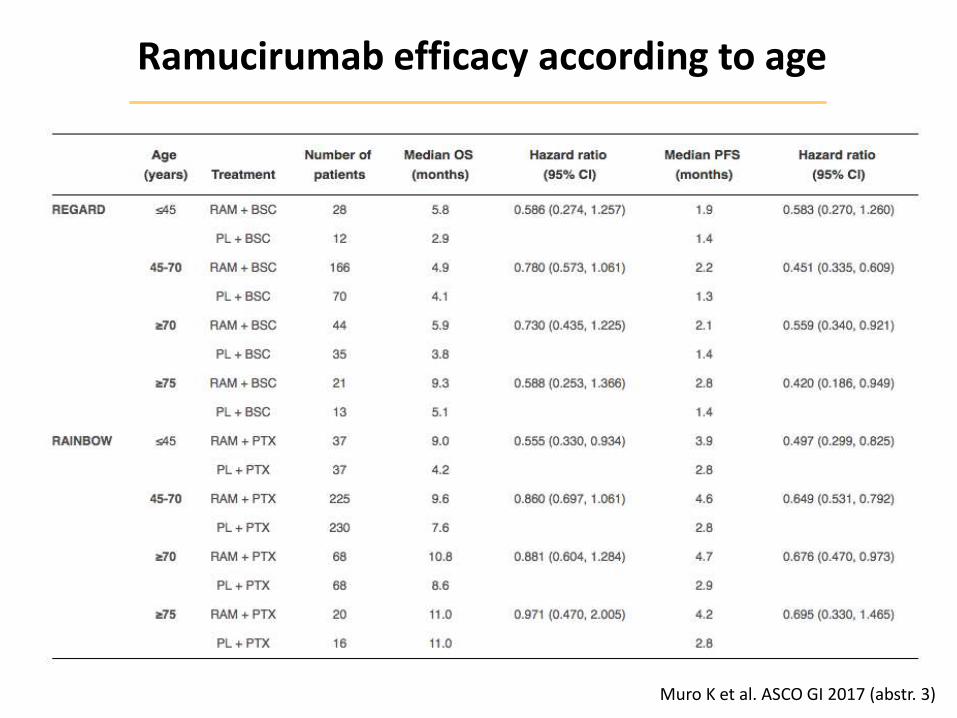
Ramucirumab efficacy according to age
Muro K et al. ASCO GI 2017 (abstr. 3)
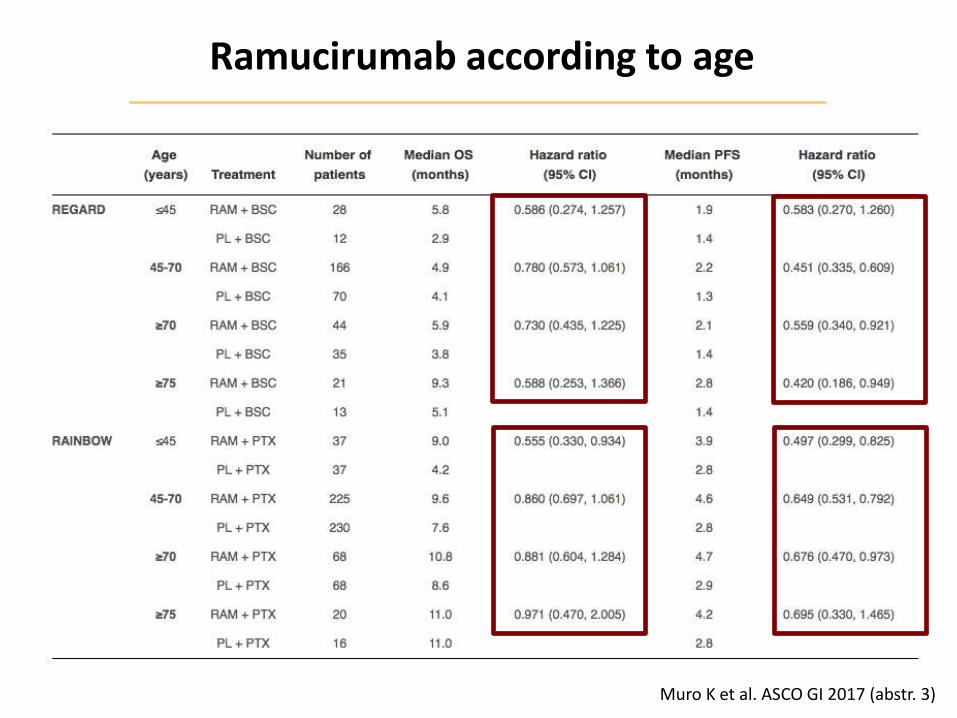
Ramucirumab according to age
Muro K et al. ASCO GI 2017 (abstr. 3)
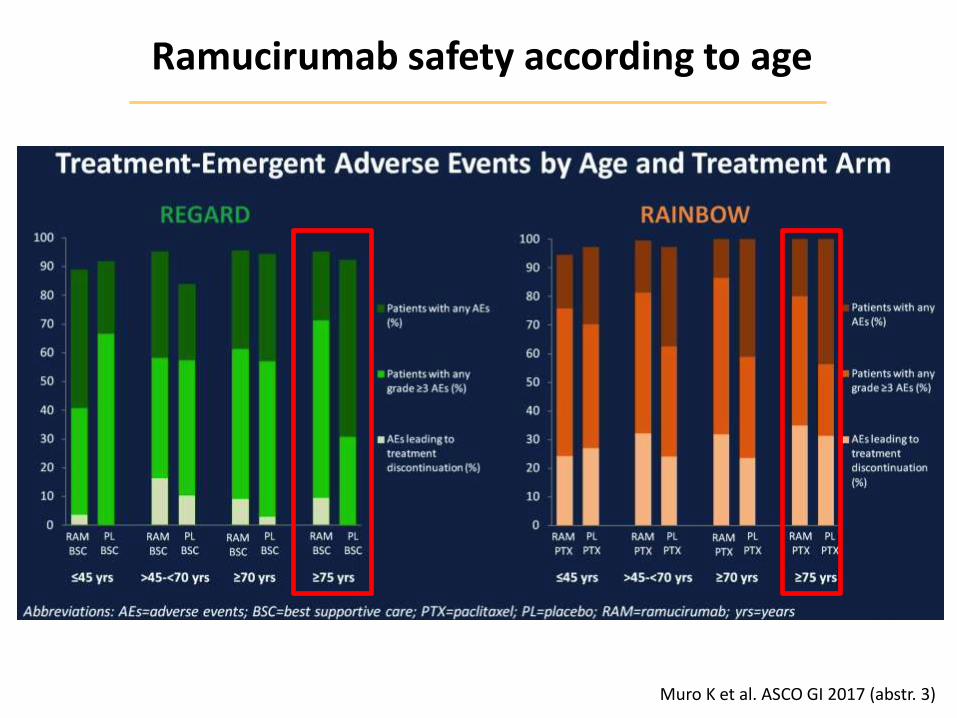
Ramucirumab safety according to age
Muro K et al. ASCO GI 2017 (abstr. 3)
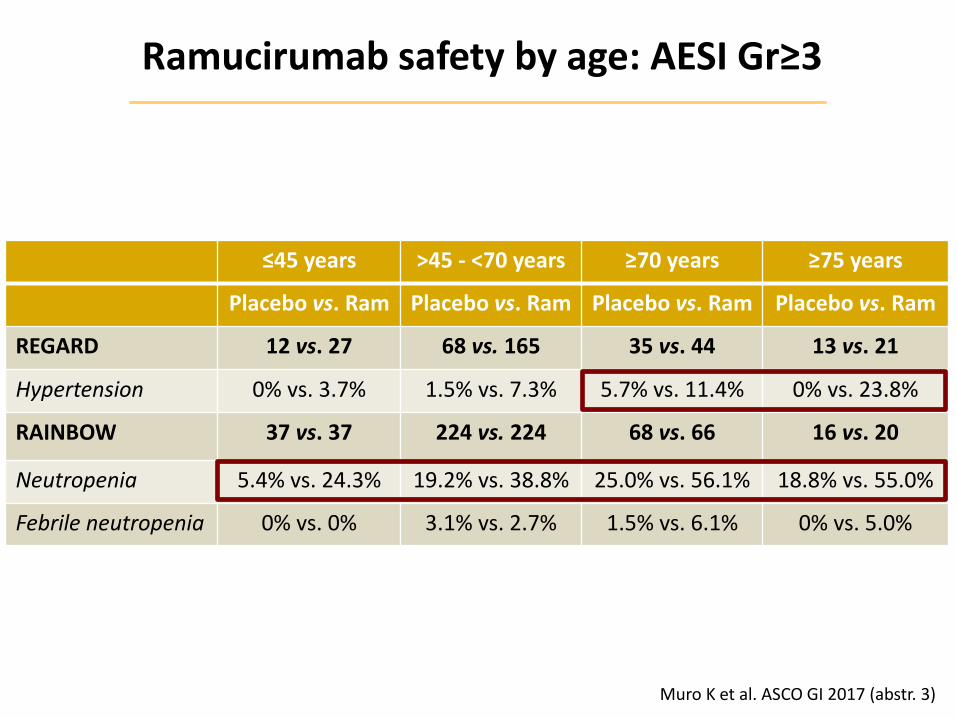
Ramucirumab safety by age: AESI Gr≥3
Muro K et al. ASCO GI 2017 (abstr. 3)
≤45 years >45 - <70 years ≥70 years ≥75 years
Placebo vs. Ram Placebo vs. Ram Placebo vs. Ram Placebo vs. Ram
REGARD 12 vs. 27 68 vs. 165 35 vs. 44 13 vs. 21
Hypertension 0% vs. 3.7% 1.5% vs. 7.3% 5.7% vs. 11.4% 0% vs. 23.8%
RAINBOW 37 vs. 37 224 vs. 224 68 vs. 66 16 vs. 20
Neutropenia 5.4% vs. 24.3% 19.2% vs. 38.8% 25.0% vs. 56.1% 18.8% vs. 55.0%
Febrile neutropenia 0% vs. 0% 3.1% vs. 2.7% 1.5% vs. 6.1% 0% vs. 5.0%
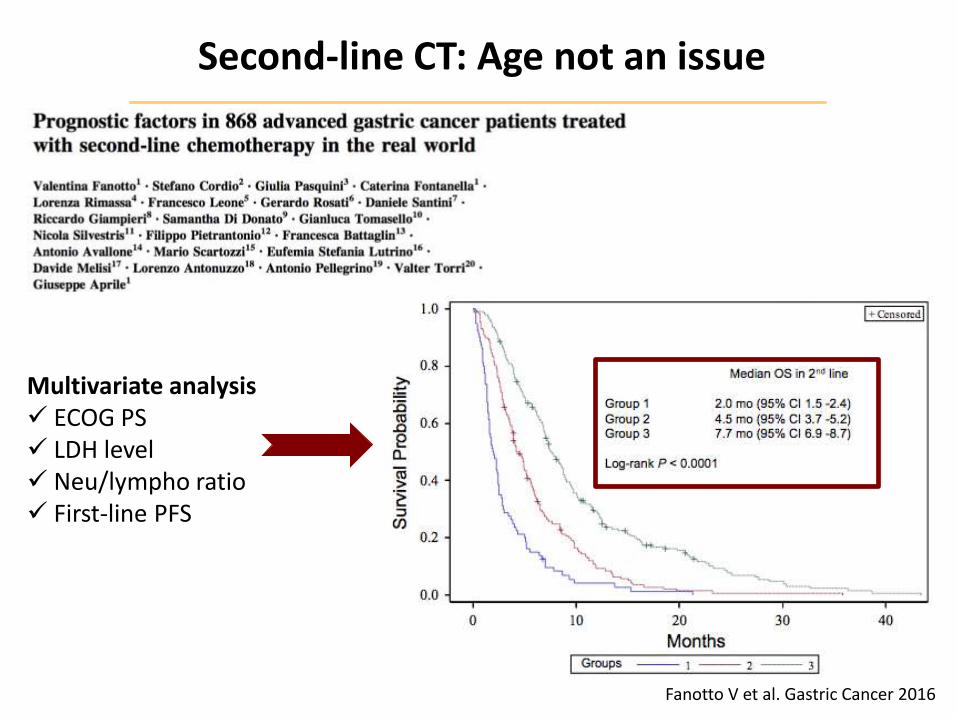
Second-line CT: Age not an issue
Fanotto V et al. Gastric Cancer 2016
Multivariate analysis ECOG PS LDH level Neu/lympho ratio First-line PFS
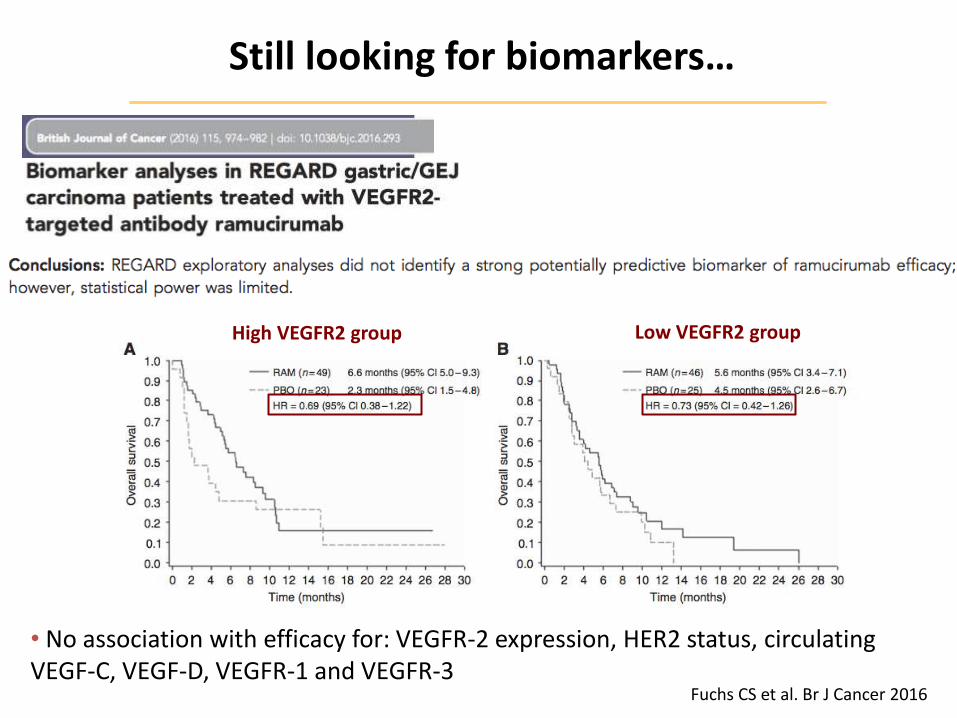
Still looking for biomarkers…
Fuchs CS et al. Br J Cancer 2016
• No association with efficacy for: VEGFR-2 expression, HER2 status, circulating VEGF-C, VEGF-D, VEGFR-1 and VEGFR-3
High VEGFR2 group Low VEGFR2 group
Agenda
• Palliation of gastric outlet obstruction: surgery or not?
• Pretreated metastatic GC: confirmations (good or not)
• Immunotherapy: a seismic shift in metastatic GC?
• Conclusions
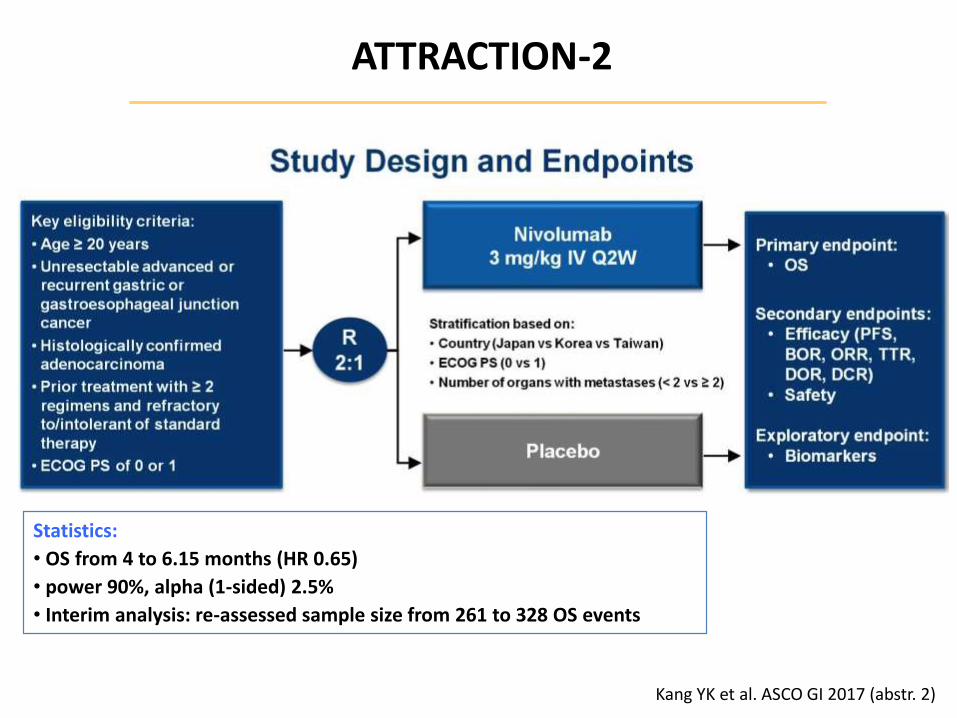
ATTRACTION-2
Kang YK et al. ASCO GI 2017 (abstr. 2)
Statistics:
• OS from 4 to 6.15 months (HR 0.65)
• power 90%, alpha (1-sided) 2.5%
• Interim analysis: re-assessed sample size from 261 to 328 OS events
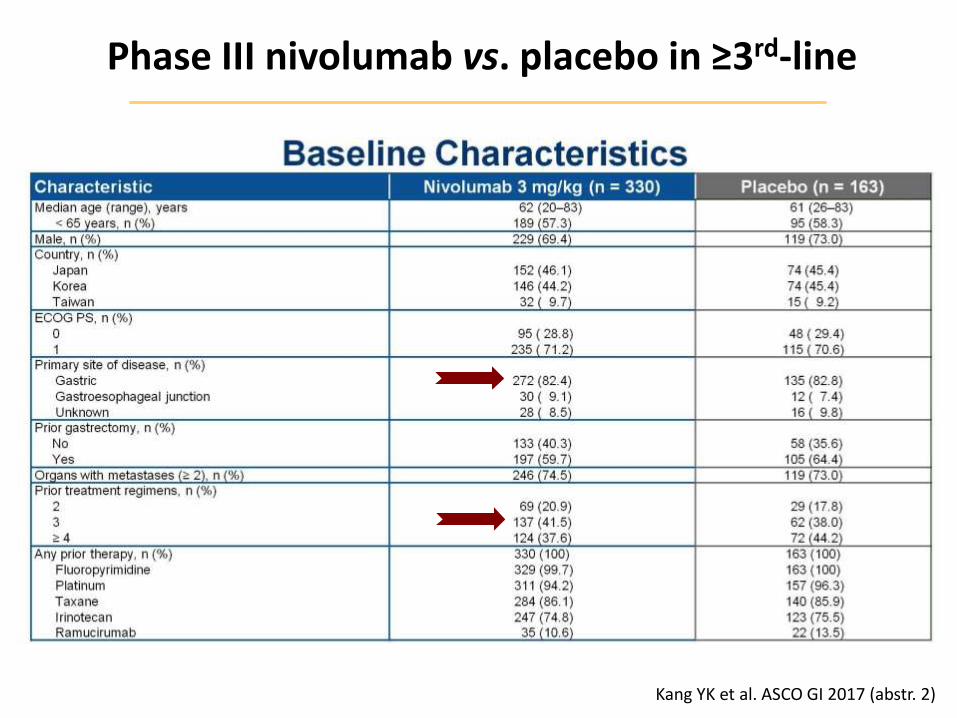
Phase III nivolumab vs. placebo in ≥3rd-line
Kang YK et al. ASCO GI 2017 (abstr. 2)
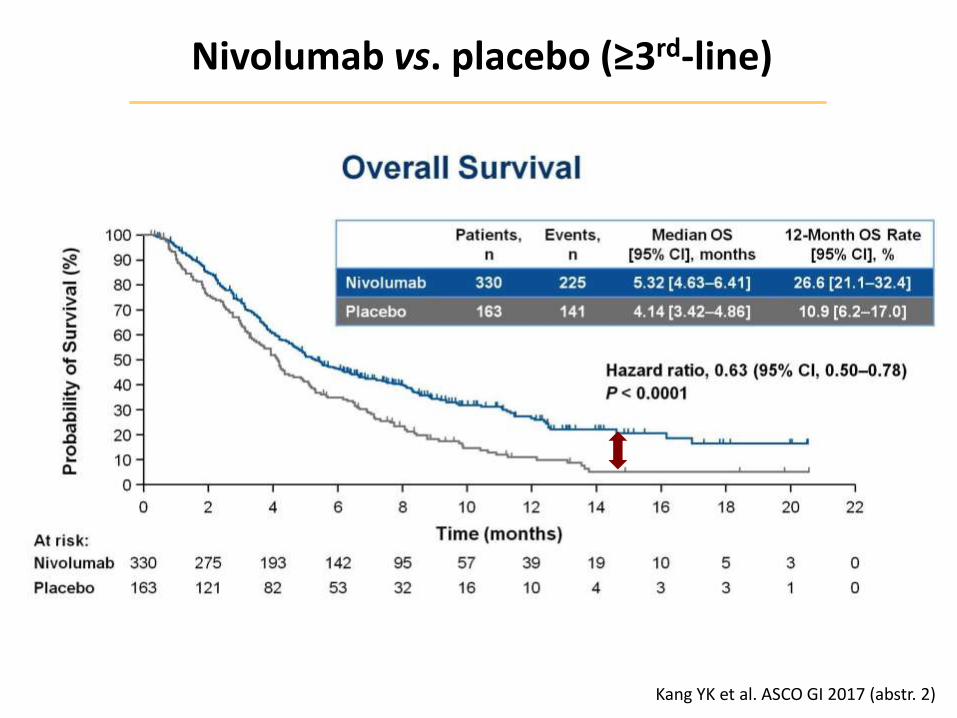
Nivolumab vs. placebo (≥3rd-line)
Kang YK et al. ASCO GI 2017 (abstr. 2)
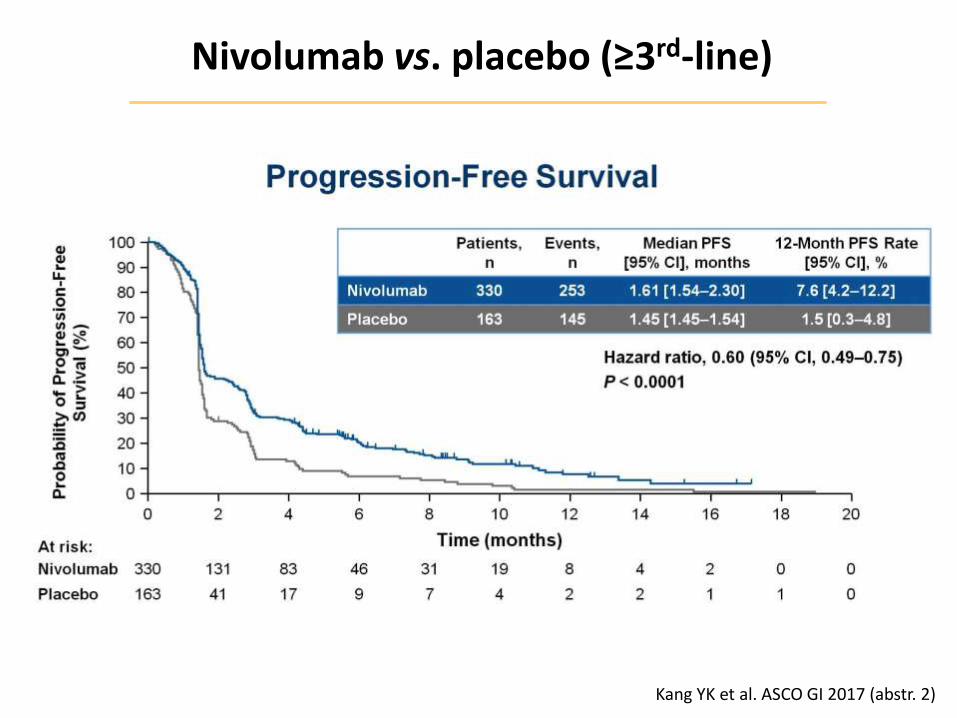
Nivolumab vs. placebo (≥3rd-line)
Kang YK et al. ASCO GI 2017 (abstr. 2)
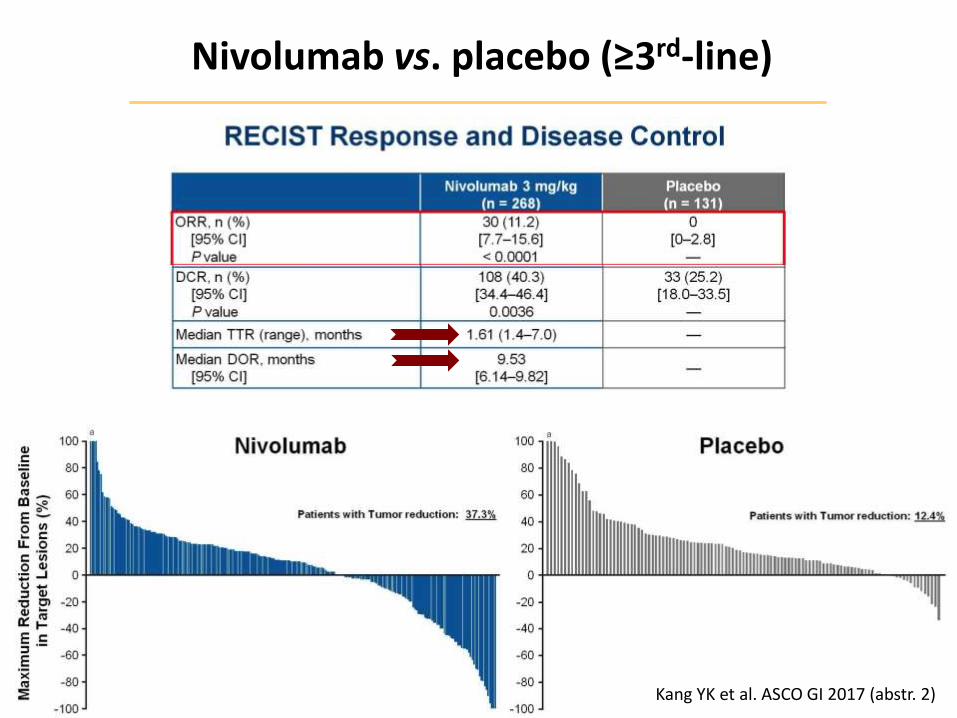
Nivolumab vs. placebo (≥3rd-line)
Kang YK et al. ASCO GI 2017 (abstr. 2)
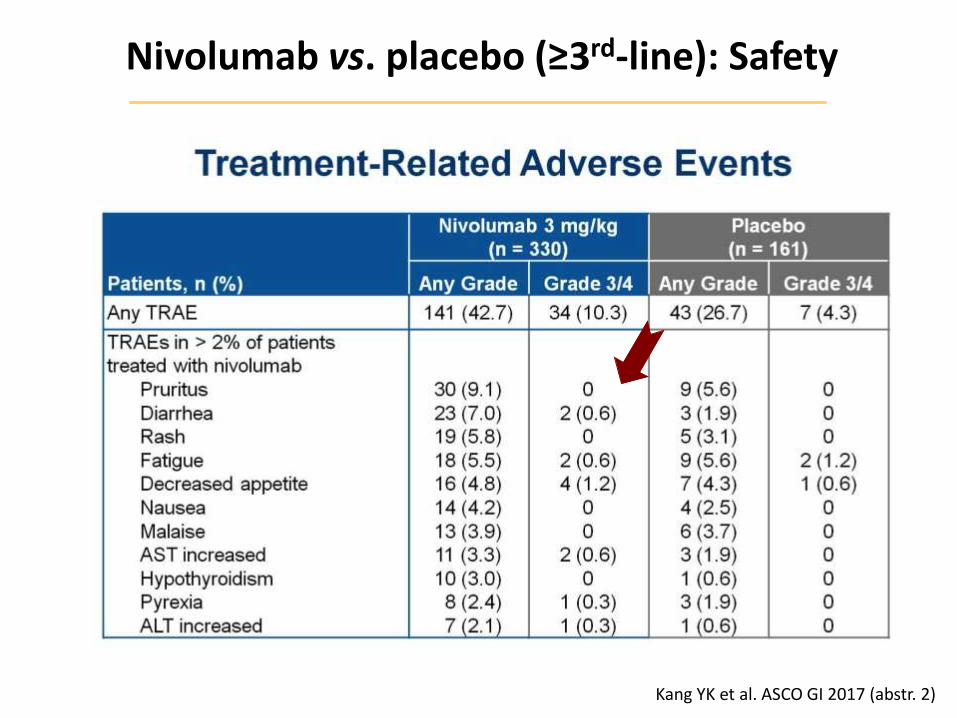
Nivolumab vs. placebo (≥3rd-line): Safety
Kang YK et al. ASCO GI 2017 (abstr. 2)
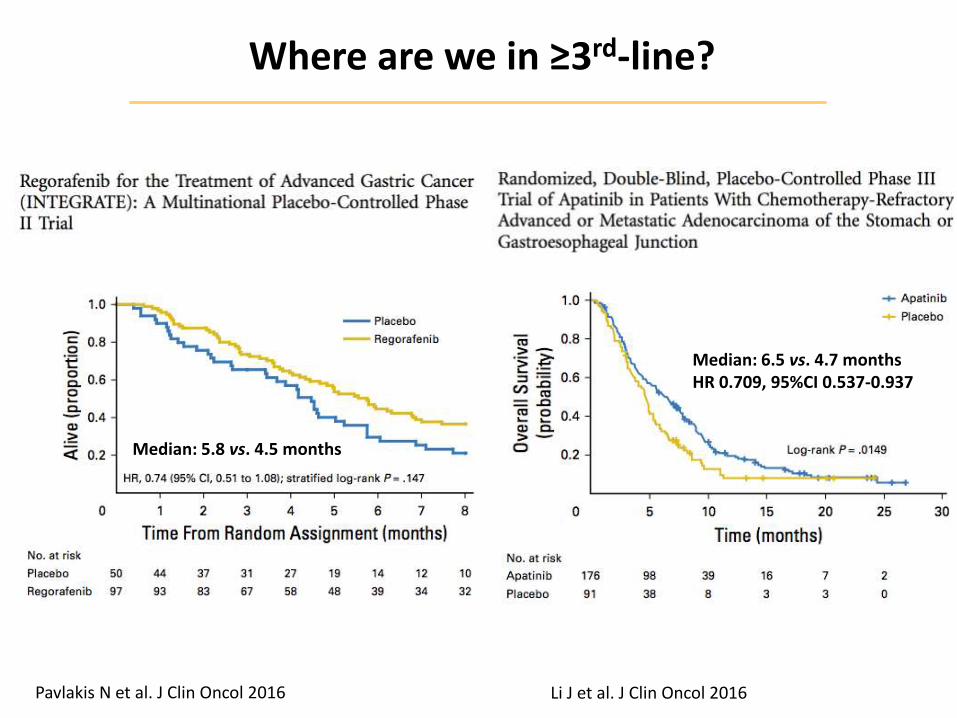
Where are we in ≥3rd-line?
Li J et al. J Clin Oncol 2016
Median: 6.5 vs. 4.7 months HR 0.709, 95%CI 0.537-0.937
Median: 5.8 vs. 4.5 months
Pavlakis N et al. J Clin Oncol 2016
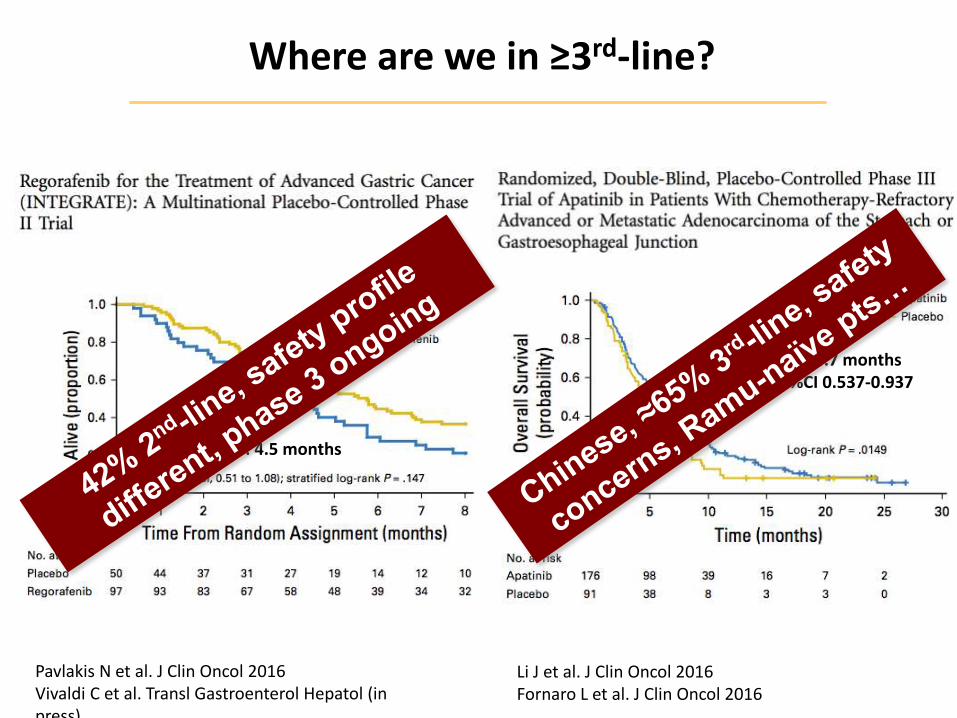
Where are we in ≥3rd-line?
Median: 6.5 vs. 4.7 months HR 0.709, 95%CI 0.537-0.937
Median: 5.8 vs. 4.5 months
Pavlakis N et al. J Clin Oncol 2016 Vivaldi C et al. Transl Gastroenterol Hepatol (in press)
Li J et al. J Clin Oncol 2016 Fornaro L et al. J Clin Oncol 2016
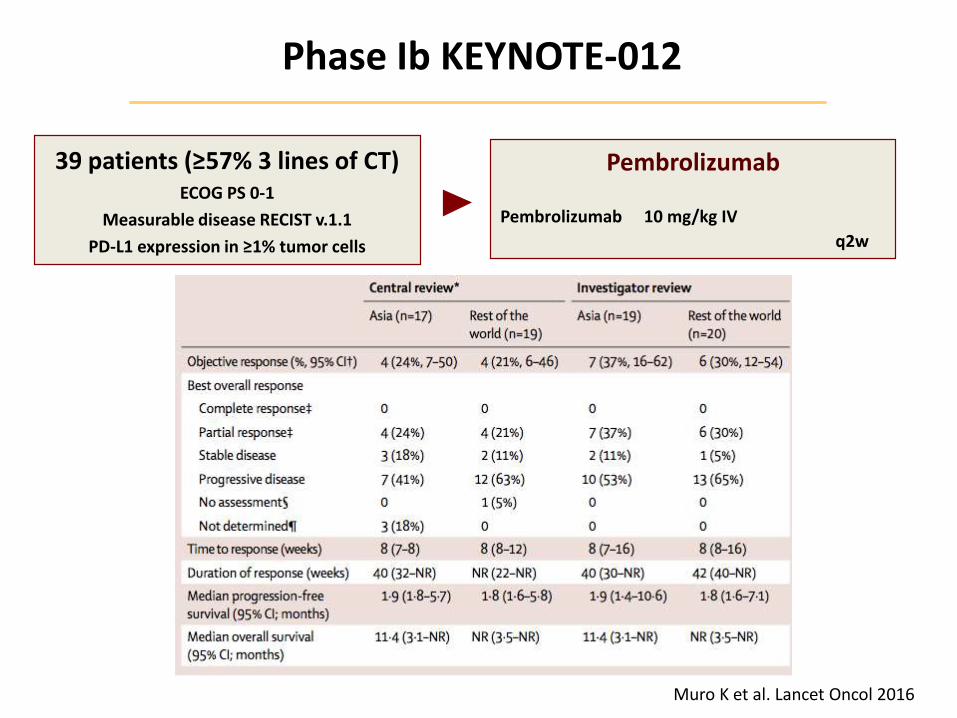
Phase Ib KEYNOTE-012
Muro K et al. Lancet Oncol 2016
Pembrolizumab
Pembrolizumab 10 mg/kg IV
q2w
39 patients (≥57% 3 lines of CT) ECOG PS 0-1
Measurable disease RECIST v.1.1
PD-L1 expression in ≥1% tumor cells
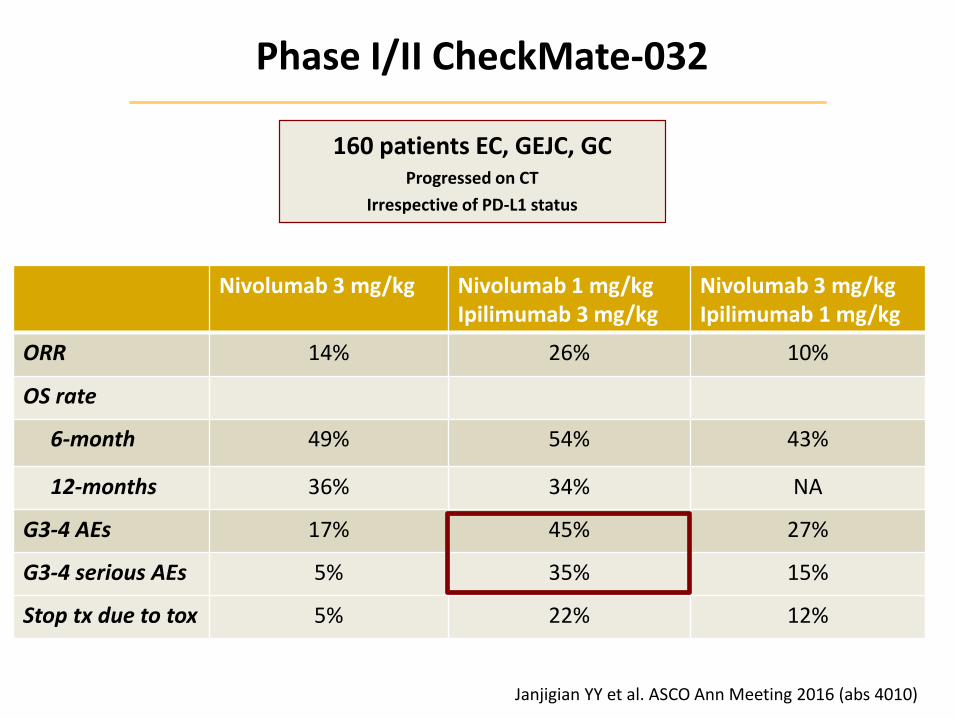
Phase I/II CheckMate-032
Janjigian YY et al. ASCO Ann Meeting 2016 (abs 4010)
160 patients EC, GEJC, GC Progressed on CT
Irrespective of PD-L1 status
Nivolumab 3 mg/kg Nivolumab 1 mg/kg Ipilimumab 3 mg/kg
Nivolumab 3 mg/kg Ipilimumab 1 mg/kg
ORR 14% 26% 10%
OS rate
6-month 49% 54% 43%
12-months 36% 34% NA
G3-4 AEs 17% 45% 27%
G3-4 serious AEs 5% 35% 15%
Stop tx due to tox 5% 22% 12%
Selection criteria for immunotherapy?
• Tumor location in the stomach
GEJ vs. gastric body
• TCGA molecular subgroups
MSI and EBV
• Target expression
PD-L1+
Selection criteria for immunotherapy?
• Tumor location in the stomach
GEJ vs. gastric body
• TCGA molecular subgroups
MSI and EBV
• Target expression
PD-L1+
Not mutually exclusive
Regional differences
Tumor vs. host factors
Single biomarker unlikely
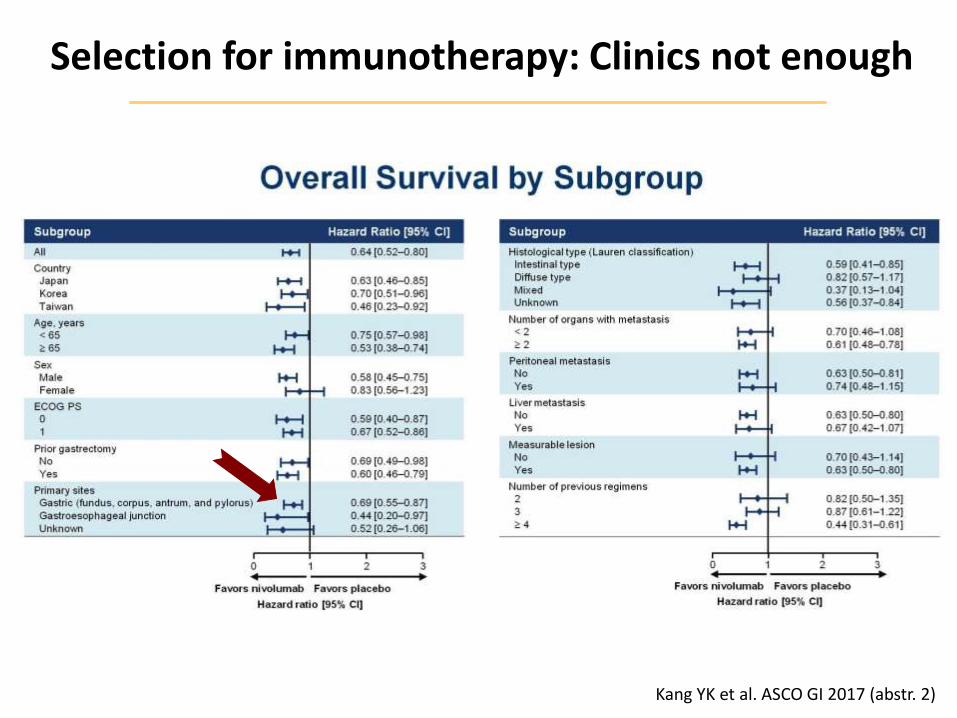
Selection for immunotherapy: Clinics not enough
Kang YK et al. ASCO GI 2017 (abstr. 2)
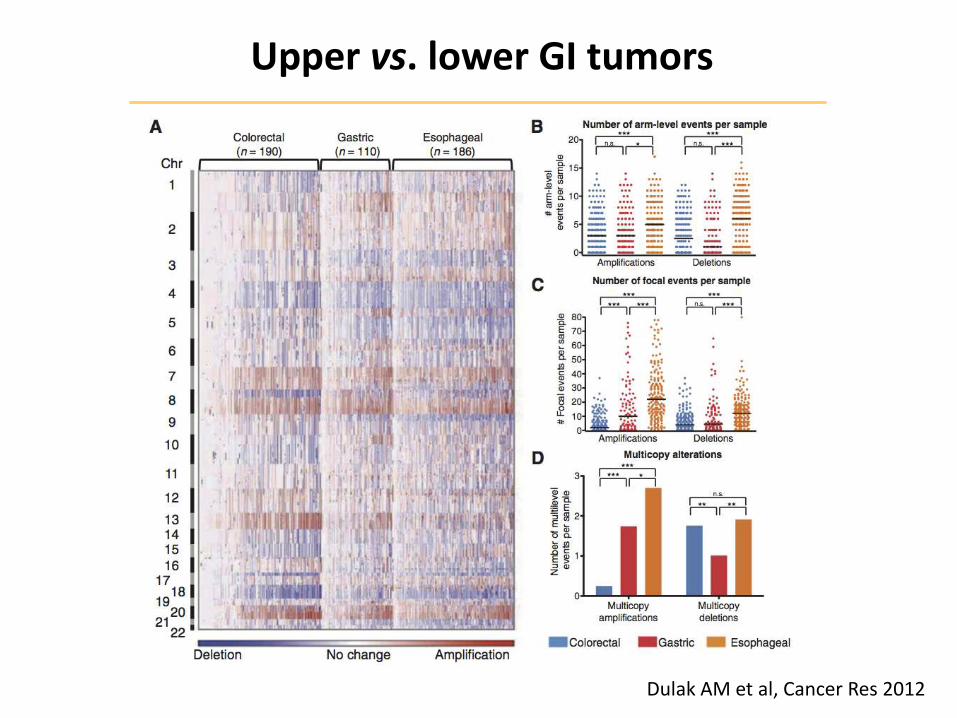
Dulak AM et al, Cancer Res 2012
Upper vs. lower GI tumors
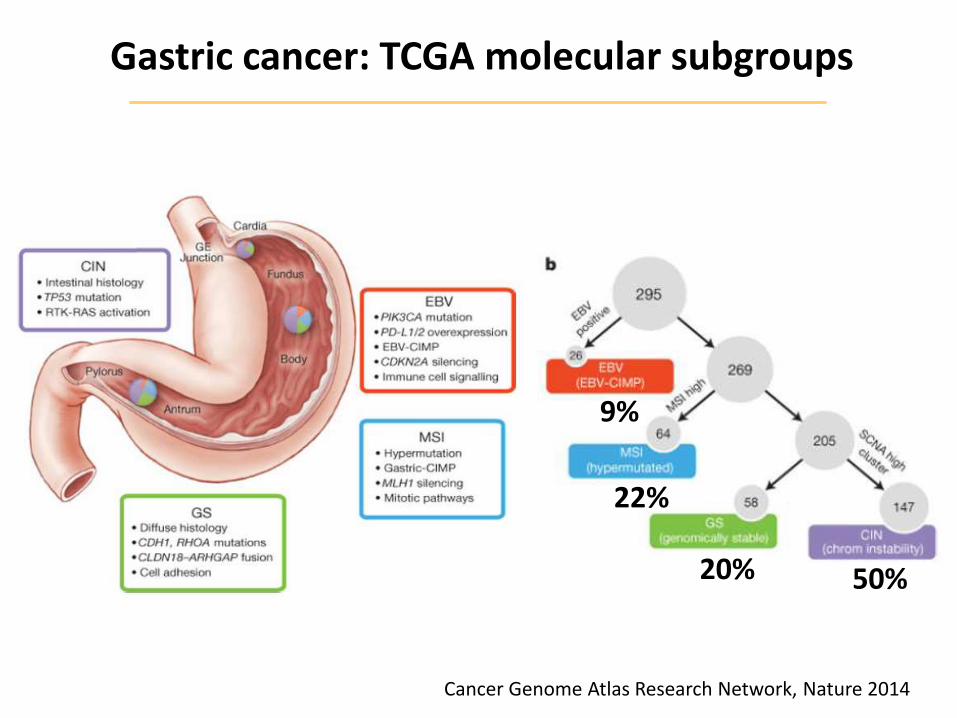
Cancer Genome Atlas Research Network, Nature 2014
9%
22%
20% 50%
Gastric cancer: TCGA molecular subgroups
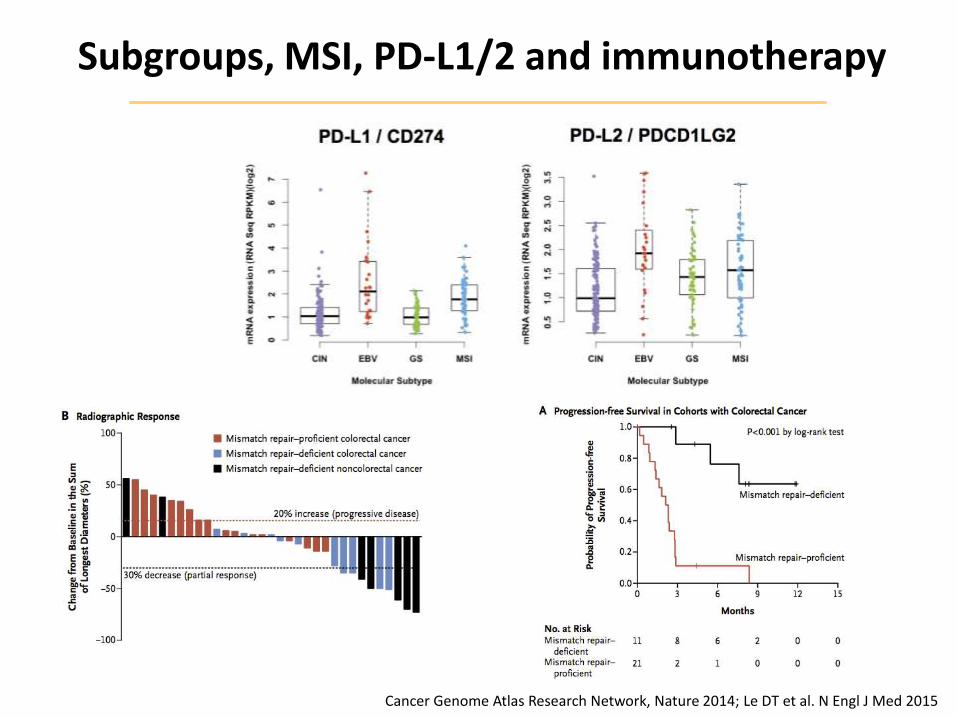
Subgroups, MSI, PD-L1/2 and immunotherapy
Cancer Genome Atlas Research Network, Nature 2014; Le DT et al. N Engl J Med 2015
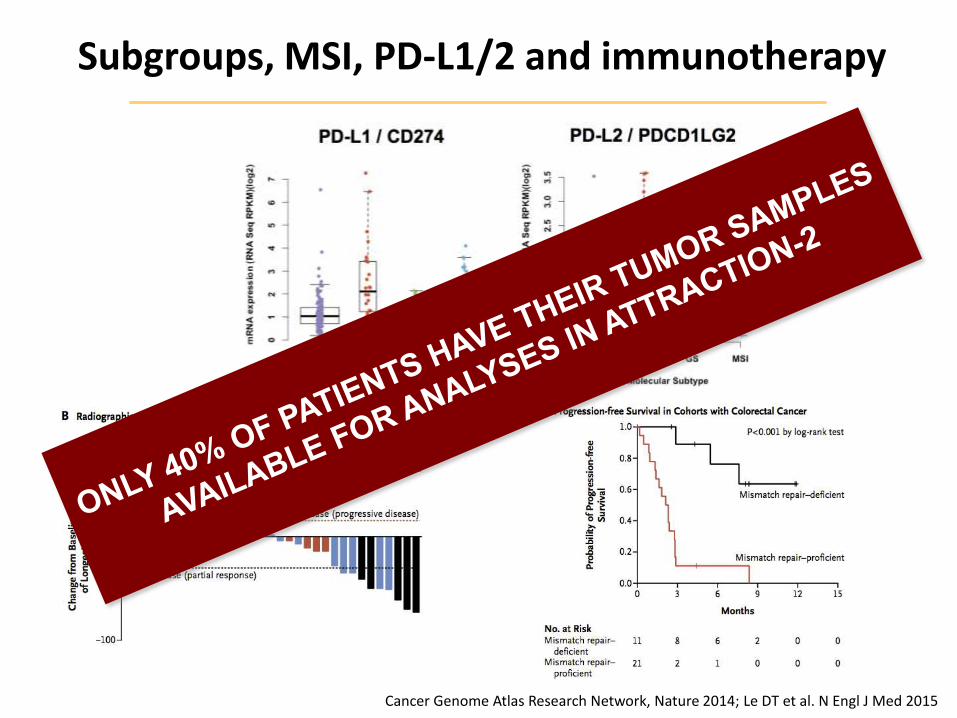
Subgroups, MSI, PD-L1/2 and immunotherapy
Cancer Genome Atlas Research Network, Nature 2014; Le DT et al. N Engl J Med 2015
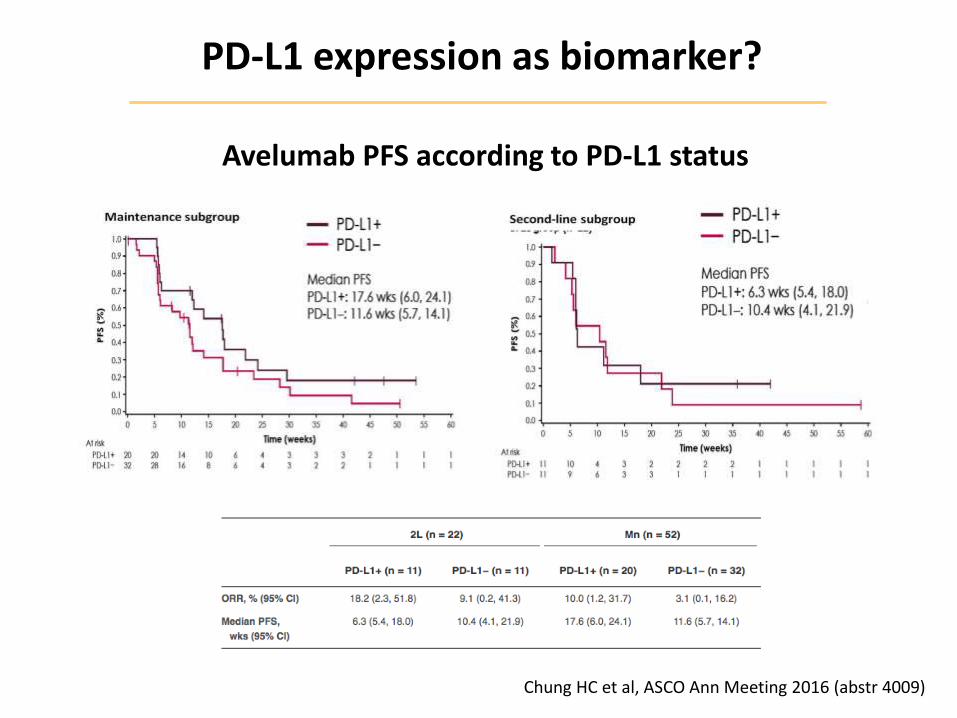
Chung HC et al, ASCO Ann Meeting 2016 (abstr 4009)
PD-L1 expression as biomarker?
Avelumab PFS according to PD-L1 status
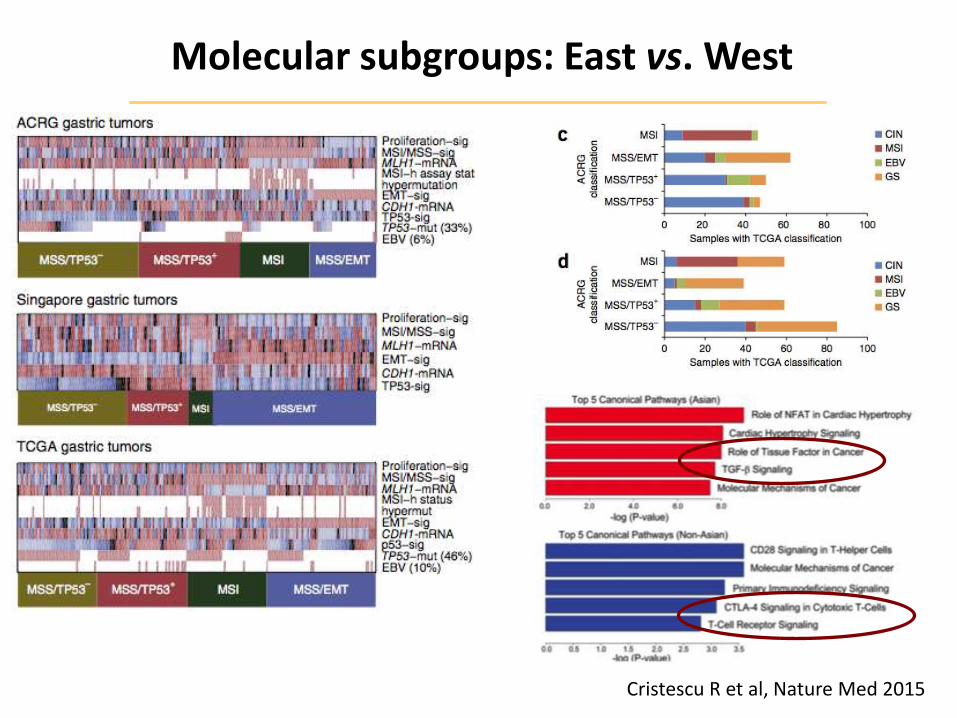
Cristescu R et al, Nature Med 2015
Molecular subgroups: East vs. West
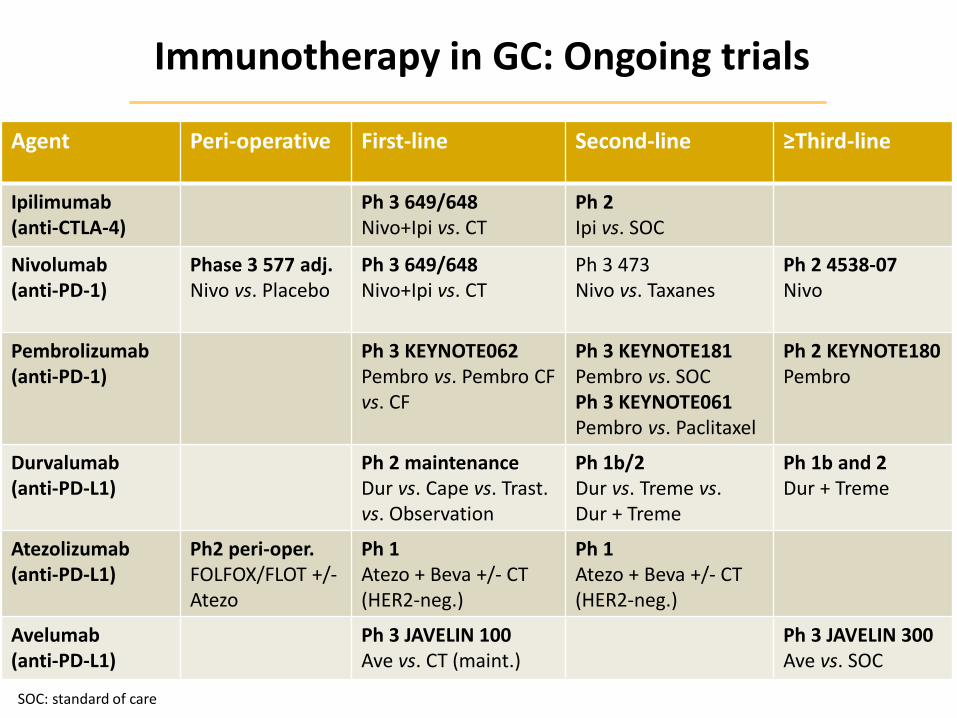
Immunotherapy in GC: Ongoing trials
Agent Peri-operative First-line Second-line ≥Third-line
Ipilimumab (anti-CTLA-4)
Ph 3 649/648 Nivo+Ipi vs. CT
Ph 2 Ipi vs. SOC
Nivolumab (anti-PD-1)
Phase 3 577 adj. Nivo vs. Placebo
Ph 3 649/648 Nivo+Ipi vs. CT
Ph 3 473 Nivo vs. Taxanes
Ph 2 4538-07 Nivo
Pembrolizumab (anti-PD-1)
Ph 3 KEYNOTE062 Pembro vs. Pembro CF vs. CF
Ph 3 KEYNOTE181 Pembro vs. SOC Ph 3 KEYNOTE061 Pembro vs. Paclitaxel
Ph 2 KEYNOTE180 Pembro
Durvalumab (anti-PD-L1)
Ph 2 maintenance Dur vs. Cape vs. Trast. vs. Observation
Ph 1b/2 Dur vs. Treme vs. Dur + Treme
Ph 1b and 2 Dur + Treme
Atezolizumab (anti-PD-L1)
Ph2 peri-oper. FOLFOX/FLOT +/- Atezo
Ph 1 Atezo + Beva +/- CT (HER2-neg.)
Ph 1 Atezo + Beva +/- CT (HER2-neg.)
Avelumab (anti-PD-L1)
Ph 3 JAVELIN 100 Ave vs. CT (maint.)
Ph 3 JAVELIN 300 Ave vs. SOC
SOC: standard of care
Agenda
• Palliation of gastric outlet obstruction: surgery or not?
• Pretreated metastatic GC: confirmations (good or not)
• Immunotherapy: a seismic shift in metastatic GC?
• Conclusions
Conclusions
• Role of palliative surgery in mGC still debated
Patient first (not symptom)
Better systemic therapy available: relevance of timing
• Ramucirumab is effective regardless of age
Established option in 2nd-line
1st-line trial ongoing
• Immunotherapy may open new ways in metastatic disease
PD-L1 and MSI: predictive role?
Monotherapy vs. combinations?
Setting: upfront ± CT vs. maintenance vs. pretreated?
Top Related