







Languages
Pages
Legal


‘‘Happily Independent’Happily Independent’
Gwent FrailtyGwent Frailty ProgrammeProgramme
Introductory PresentationIntroductory Presentation
The Vision:The Vision:
‘Help when you need it to keep you
independent’

The Ethos:The Ethos:
People are individuals with a life, a history and a future;
They are the experts in their own life and we need to tap into that expertise;
The present system is untenable & does not treat people as well as we want it to;
We work best when we work together, with shared values and joint outcomes that keep the person at the centre.
Why Frailty?Why Frailty?
Social, environmental, physical and mental health needs closely entwined: it just makes sense!
Cuts across traditional boundaries between primary and secondary health care and between health and social care.
The evidence says it works

Frailty DefinitionFrailty DefinitionDependency
Chronic limitations on activities for daily livingWith one or more physical, or social needs, including those
who have dementia
Vulnerability ‘Running on empty’ Usual coping mechanisms aren’t working
Co-Morbidity E.g. People with a chronic condition who as a result may have
health, social care and/or housing needs.

Why Do it?Why Do it?
It’s what older people tell us they want!
Integrated model of health and social care delivery
Represents a significant shift in the way public services are provided for frail people (to a community focus)
Our current way of working is unsustainable and doesn’t deliver the goods.
Outcomes: what older people in Outcomes: what older people in Gwent told us they want.Gwent told us they want.
Be able to remain living in their own home with support
Receive services in their home
Be listened to by people who are responsible for providing services to assist them
Have their health and social care problems solved quickly and considered as a whole rather than individually.
And a bit of this……And a bit of this……
• Be safe and secureBe safe and secure• Live in good quality homesLive in good quality homes• Be able to cook, wash, clean Be able to cook, wash, clean
and go outand go out• Be able to maintain their Be able to maintain their
standardsstandards• Be financially stable to make Be financially stable to make
independent choicesindependent choices• Be receiving the benefits Be receiving the benefits
available to enable them to available to enable them to live independentlylive independently
• Not be lonelyNot be lonely
• Have a supportive familyHave a supportive family• Have good friends and Have good friends and
neighbours keeping an eye neighbours keeping an eye out for themout for them
• Have companyHave company• Be going out to social Be going out to social
activitiesactivities• Have planned for old ageHave planned for old age• Be accessing peer supportBe accessing peer support• Be able to keep a pet if they Be able to keep a pet if they
so wishso wish

Integrated Locality ApproachIntegrated Locality Approach
Acute
Intensive packages
Episodic or longer
Term interventions
Identified needs warranting integrated approach
Some identified health/social care
needs
Preventative Services
Community Context

Frailty Programme Layers:Frailty Programme Layers:
• Community Resource Teams
• Training, development, cultural change
• Work with LSBs etc
• Influencing & aligning
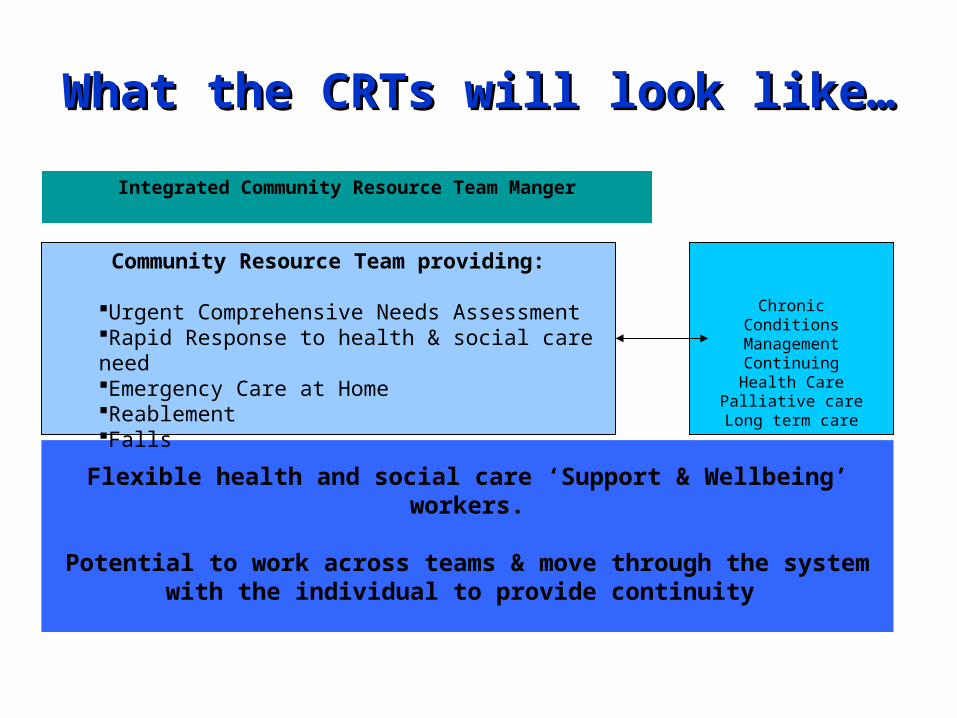
What the CRTs will look like…What the CRTs will look like…
Flexible health and social care ‘Support & Wellbeing’ workers.
Potential to work across teams & move through the system with the individual to provide continuity
Chronic Conditions
ManagementContinuing Health
CarePalliative careLong term care
Community Resource Team providing:
Urgent Comprehensive Needs AssessmentRapid Response to health & social care needEmergency Care at HomeReablement Falls
Integrated Community Resource Team Manger
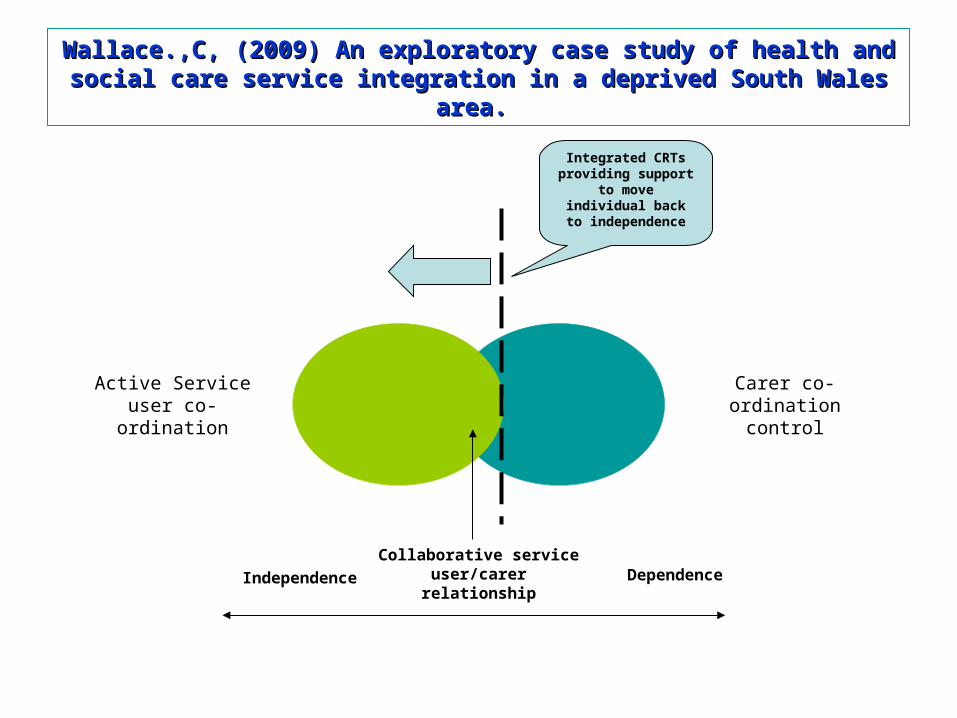
Wallace.,C, (2009) An exploratory case study of health and Wallace.,C, (2009) An exploratory case study of health and social care service integration in a deprived South Wales social care service integration in a deprived South Wales
area.area.
Carer co-ordination control
Active Service user co-ordination
Collaborative service user/carer relationshipIndependence Dependence
Integrated CRTs providing support to move individual
back to independence

Team Composition:Team Composition:
It is proposed that each locality team will include the following members:
Administrative supportA team of Support & Wellbeing Workers Registered General NursesRegistered Mental NursesSocial WorkersPharmacistSpecialty Doctors
Occupational Therapists
PhysiotherapistsDietetics/SALT/podiatryConsultant Physician
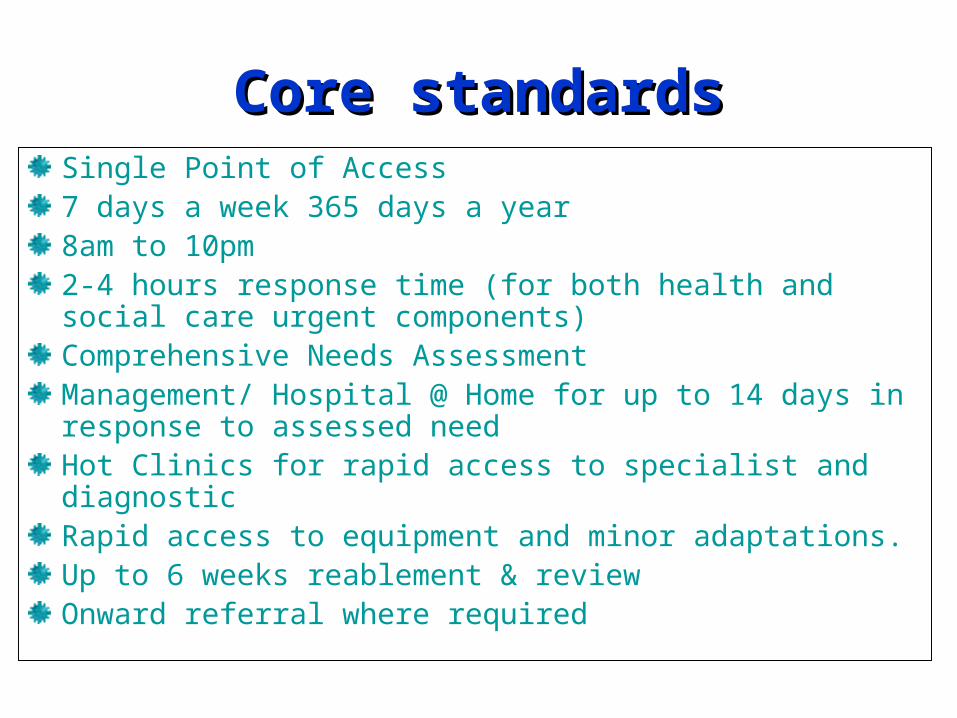
Core standardsCore standardsSingle Point of Access7 days a week 365 days a year8am to 10pm2-4 hours response time (for both health and social care urgent components)Comprehensive Needs AssessmentManagement/ Hospital @ Home for up to 14 days in response to assessed needHot Clinics for rapid access to specialist and diagnostic Rapid access to equipment and minor adaptations.Up to 6 weeks reablement & reviewOnward referral where required

Case Scenario 1Case Scenario 1• Mrs Jones, a 45 year old lady with Multiple Sclerosis, develops
urinary symptoms. Her GP visits and treats Mrs Jones for a urinary tract infection. 24 hours later however she is still not coping and is ‘off her feet’. The GP refers her, via the Single Point of Access, to the Community Resource Team.
• They visit within the hour and assess her thoroughly. They exclude other potential diagnoses and assess that Mrs Jones needs support to help her recover. The registered nurse arranges for social care and occupational therapy to help Mrs Jones get back to independence as quickly as possible. A Support & Wellbeing Worker visits 3 times a day to help Mrs Jones with her daily living needs.
• After a week, the infection is resolved, but Mrs Jones is still unsteady and lacking in confidence. Further reablement support is developed by the therapists in the team and delivered by the Support & Wellbeing Worker. A discharge letter summarising Mrs Jones’ outcomes and onward referral is sent to her GP.

Case Scenario 2Case Scenario 2
• Mrs Jones is 70 years old and is bed ridden. She is cared for by her husband who is normally a physically fit 75 year old.
• Mr Jones develops chest pain and is rushed to hospital by ambulance leaving Mrs Jones alone. Mrs Jones is referred to the Community Resource Team for support during her social care crisis.

Story so far………Story so far………
Established what older people want ‘Towards Independence for Older people in Gwent’
Articulated the vision‘Happily Independent’
Achieved executive and political sign up to the Strategic Outline CaseSeven implementation workstreams up and runningLocality Implementation Groups set up (Franchise Model)
The Workstreams:The Workstreams:
Communication & Stakeholder EngagementWorkforce PlanningGovernance & StructuresPerformance Management & EvaluationInformation Sharing & Single Point of AccessFinancial Modelling Locality Planning
Locality Frailty Locality Frailty Implementation Groups Implementation Groups
Each Borough to assess local need and design their specific CRT in response, e.g.
• Size/number• Location• Date to ‘go live’

Coming soon…….Coming soon…….
• Response to bid heard for ‘pump prime’ funding expected late Spring 2010
• Final, detailed plans to be presented to Boards, Cabinets etc September 2010
• Community Resource Teams up and running in all localities by end of March 2011
Pieces of work we need to Pieces of work we need to do…………..do…………..
Carers Strategy
Mental Health
Knowledge Management
Referral management (criteria, screening, Frailty Index etc);
Out of hours/ On Call arrangements, including cross-boundary cover at times of peak demand.
Falls Strategy
Telecare

Contacts:Contacts:
Programme Manager:Lynda Chandler – [email protected]: 01495 742411
Website:http//:www.gwentfrailty.torfaen.gov.uk
Top Related