







Languages
Pages
Legal


Growth Concerns for Children with Congenital
Hyperinsulinism
Growth Concerns for Children with Congenital
Hyperinsulinism
Adda Grimberg, MD
Scientific Director,
Diagnostic & Research Growth Center
The Children’s Hospital of Philadelphia
Adda Grimberg, MD
Scientific Director,
Diagnostic & Research Growth Center
The Children’s Hospital of Philadelphia

Disclosure Disclosure
Adda Grimberg, MD serves on the Steering Committee for the Pfizer International Growth Study database.
Adda Grimberg, MD serves on the Steering Committee for the Pfizer International Growth Study database.

The GH/IGF axis The GH/IGF axis
Henwood M, Grimberg A, Moshang T. Curr Opin Pediatr. 2002.
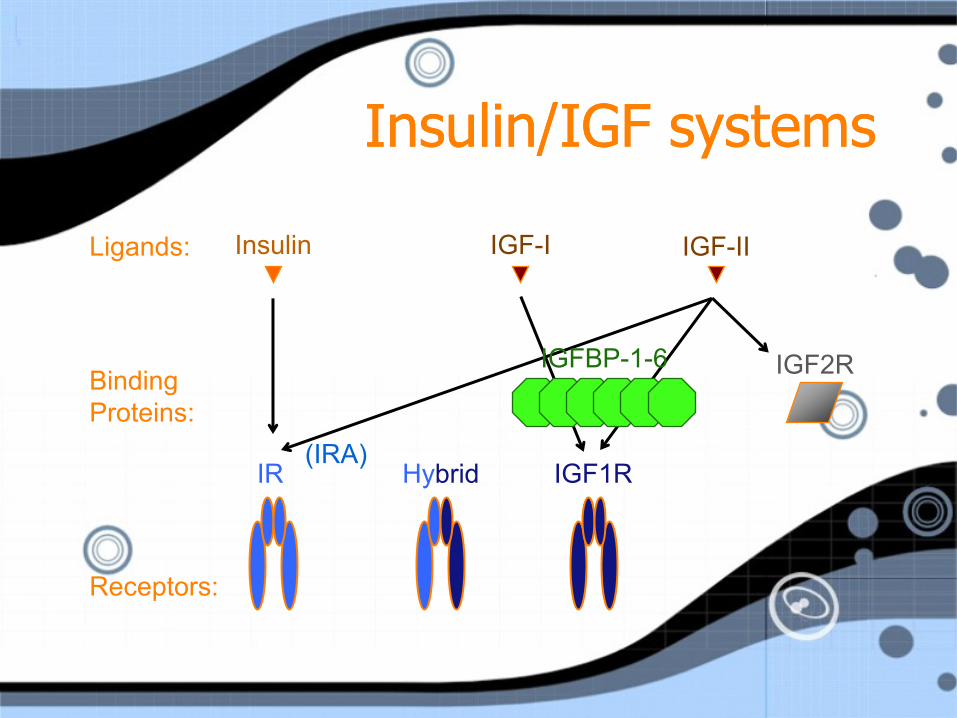
Insulin/IGF systems Insulin/IGF systems
(IRA)
Ligands: Insulin IGF-I IGF-II
Binding
Proteins:
Receptors:
IGF1R Hybrid
IGFBP-1-6
IR
IGF2R
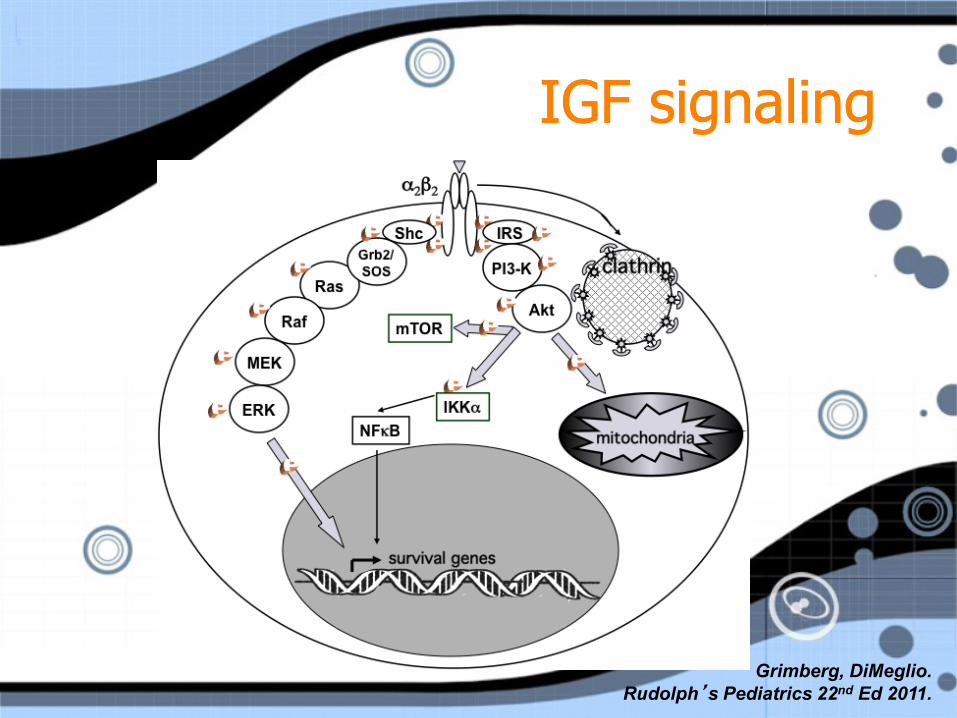
IGF signaling IGF signaling
Grimberg, DiMeglio.
Rudolph’s Pediatrics 22nd Ed 2011.

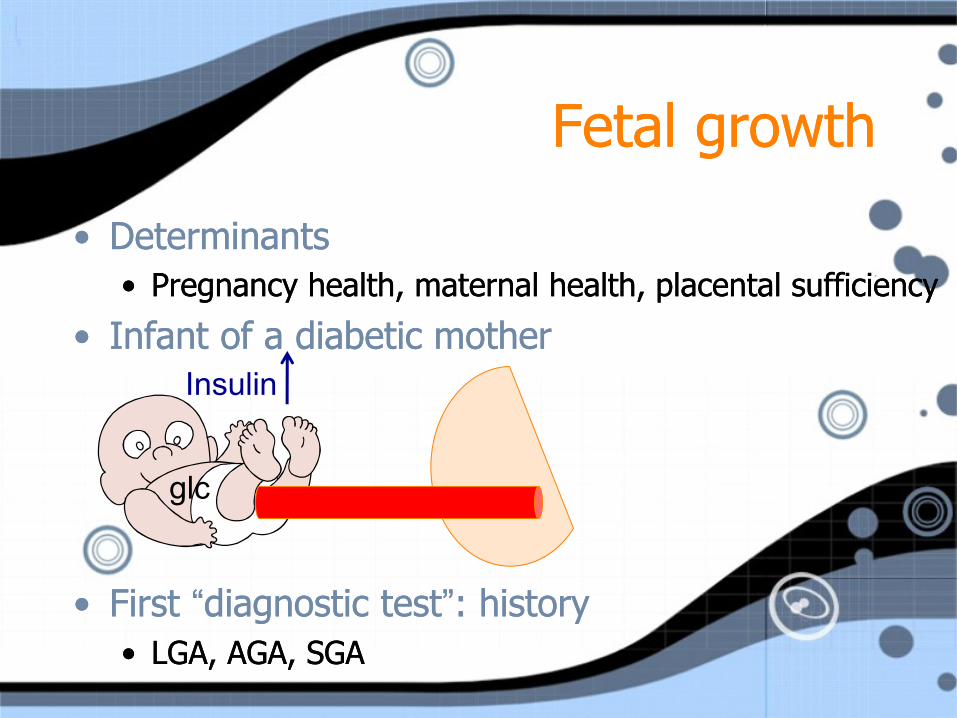
Fetal growth Fetal growth
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
glc

Fetal growth Fetal growth
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
glc

Fetal growth Fetal growth
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
glc
Insulin
Fetal growth Fetal growth
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
• Determinants
• Pregnancy health, maternal health, placental sufficiency
• Infant of a diabetic mother
• First “diagnostic test”: history
• LGA, AGA, SGA
glc
Insulin

Transition Transition
• Fetal growth determinants to
post-natal growth determinants
• Physiologic rechanneling
• Catch-up growth
• Catch-down growth
• Fetal growth determinants to
post-natal growth determinants
• Physiologic rechanneling
• Catch-up growth
• Catch-down growth

Normal growth Normal growth
• Follows pattern • Fastest first 2 years of life
• Steady age 3 years until puberty
• Pubertal growth spurt
• Stop
• Based on
• Reference population
• Family
• Gender
• Follows pattern • Fastest first 2 years of life
• Steady age 3 years until puberty
• Pubertal growth spurt
• Stop
• Based on
• Reference population
• Family
• Gender
(post-natal)

Growth charts Growth charts

WHO vs CDC growth charts (boys)
WHO vs CDC growth charts (boys)
Weight Length Weight Length
“Use of WHO and CDC growth charts for children aged 0-59 mos in the US.” DHHS, CDC. MMWR 59(9). Sept 10, 2010.
https://www.cdc.gov/growthcharts

Measuring growth Measuring growth

Plotting growth Plotting growth
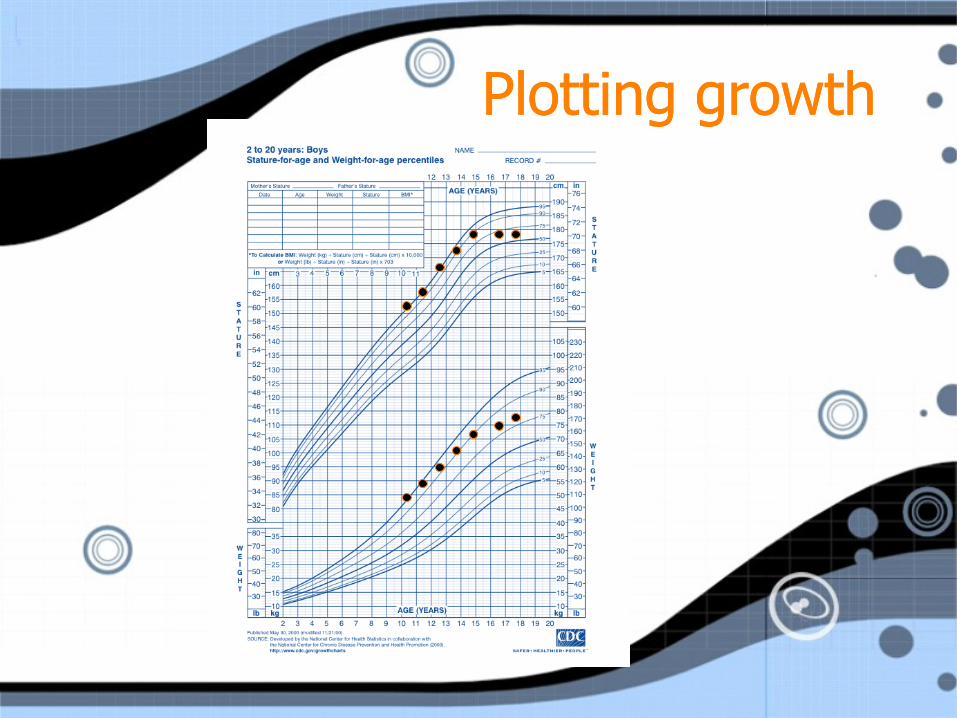
Plotting growth Plotting growth

Short Short

Slow Slow

Abnormal growth Abnormal growth
• Height < -2 SD for population
• Height < 2 SD
below parental target height
• Height falling across major %iles
• Slow growth velocity
(< 2 inches or 5 cm per year)
• Height < -2 SD for population
• Height < 2 SD
below parental target height
• Height falling across major %iles
• Slow growth velocity
(< 2 inches or 5 cm per year)

Growth is the most sensitive physical sign
of a child’s overall health.
Growth is the most sensitive physical sign
of a child’s overall health.
It is very nonspecific. It is very nonspecific.

Processes that affect growth Processes that affect growth
Systemic
disorders SGA/IUGR
GI
diseases,
Nutrition
Psycho-
social
deprivation
Normal
growth
Genetic
disorders
Endocrine
disorders

Sequence of pubertal events Sequence of pubertal events
Tanner JM. Growth at Adolescence.
Oxford, Blackwell Scientific Pub,1962:30-36.

Normal growth: sex differences Normal growth: sex differences
Girls’ peak growth rate: 11.5 years Boys’ peak growth rate: 13.5 years
National Center for Health Statistics.
Tanner JM, et al. J Pediatr. 1985.
Gro
wth
ra
te (
cm
/y)
Age (y)
2 19 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
0
12
11
10
9
8
7
6
5
4
3
2
1
Girls: solid lines
Boys: dashed lines

Evaluation of growth Evaluation of growth
• Objective: normal variant or disease?
• Pattern of growth (growth curves)
• Genetic expectation (midparental target height)
• Medical history
• Physical examination
• Laboratory/radiological analysis
• Treatment options
• Objective: normal variant or disease?
• Pattern of growth (growth curves)
• Genetic expectation (midparental target height)
• Medical history
• Physical examination
• Laboratory/radiological analysis
• Treatment options

Bone age Bone age
Male, 14 years Male, 8 years

Parental advocacy Parental advocacy
• Prepare for the measurements.
• Review the plotting.
• If questions, ask.
• Keep the data going!
• Don’t over-emphasize height.
• Foster self-esteem.
• Prepare for the measurements.
• Review the plotting.
• If questions, ask.
• Keep the data going!
• Don’t over-emphasize height.
• Foster self-esteem.
Top Related