



Languages
Pages
Legal

Central Journal of Liver and Clinical Research
Cite this article: Ergün S, Akıncı O, Tosun Y, Kandemirli SG, Velidedeoğlu M, et al. (2017) Gallbladder Duplication: A Rare Case Presentation. J Liver Clin Res 4(2): 1036.
*Corresponding authorSefa Ergün, Department of General Surgery, Istanbul Universıty Cerrahpaşa, Postal Code: 4093 Istanbul, Turkey, Tel: +9 5378935148; Fax: +9 02124143370; Email:
Submitted: 13 January 2017
Accepted: 28 August 2017
Published: 30 August 2017
ISSN: 2379-0830
Copyright© 2017 Ergün et al.
OPEN ACCESS
Case Report
Gallbladder Duplication: A Rare Case PresentationSefa Ergün1*, Ozan Akıncı1, Yasin Tosun1, Sedat Giray Kandemirli2, Mehmet Velidedeoğlu1, and Metin Kapan11Department of General Surgery, Istanbul Universıty Cerrahpaşa, Turkey2Department of Radiology, Istanbul Universıty Cerrahpaşa, Turkey
Abstract
Gallbladder duplication is a rare congenital anomaly. Identification of this anatomical variation with careful preoperative evaluation, and planning surgery accordingly is important to prevent perioperative complications.
INTRODUCTIONGallbladder duplication is a rare congenital malformation
observed in 1/4000 births [1]. Preoperative detection of the duplication and its type is important to avoid complications during cholecystectomy. Harlaftis et al., classified gallbladder duplications in two categories based on gallbladder’s relation to the common bile duct [2]. In type-1 duplication, gallbladder opens to the common bile duct through only a single cystic duct, whereas in type-2 duplication, there are two separate cystic ducts. In this paper, we present a case with type-2 duplication of gallbladder diagnosed and operated in our clinic.
CASE PRESENTATION25 year old female patient with no previous history of operation
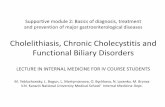
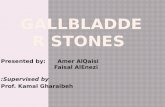
or disease presented with right upper quadrant abdominal pain that started a year ago. Abdominal ultrasonography (USG) revealed two gallbladder sacs with longitudinal lengths of 8 and 5 cm. There were multiple millimetric gallstones in both sacs, the largest was measured as 11 mm. Wall thickness of both sacs was normal. Proximal diameter of common bile duct was 7 mm. Distal segment could not be visualized (Figure 1). Magnetic resonance cholangio-pancreatography (MRCP) showed gallbladder duplication, and both cavities were draining into the common bile duct through a common cystic duct (type-1 duplication) (Figure 1,2).
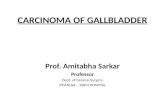
Cholecystectomy was planned due to chronic pain and multiple gallstones. Considering that the duplication was a type-1 duplication, laparoscopic cholecystectomy was planned. During laparoscopic cholecystectomy, gallbladder sacs were observed to be adhered along their longitudinal axis. After exposing Calot triangle, a single larger cystic duct and single cystic artery were detected (Figure 3). Dissection was difficult because of the different structure. Following dissection, clipping, and transection of cystic duct and artery, gallbladder sacs were separated from the liver bed. Operation time was 80 minutes and
no major bleeding occurred during the operation. During gross examination at the back table, gallbladder sacs were observed to adhere to each other. When the sacs were canalized, both sacs were observed to possess separate cystic ducts as in Type-2 duplication, and these cystic ducts were adhered to each other (Figure 3). No perioperative and postoperative complication occurred. The patient was discharged three days after the operation. Because she lived outside the city and stated that she wanted to stay in the hospital. Pathological examination showed findings consistent with chronic cholecystitis.
DISCUSSIONGallbladder anomalies can be categorized as morphology,
number and position anomalies. According to the anotomical structure, different classifications are described by Boyden, Gross and Harlaftis [1-3]. The Harlaftis classification is the most accepted classification [2]. This classification is made according to morphology and embryogenesis and there are two types. Type 1 is subdivided into septated, V-shaped or Y-shaped. Type 2 can
Figure 1 Two gallbladder sacs with multiple gallstones.
Central
Ergün et al. (2017)Email:
J Liver Clin Res 4(2): 1036 (2017) 2/3
be ductular or trabecular and arise from two separate primordia on the biliary tree and possess separate cystic ducts [2]. According to the Boyden classification vesica fellae divisa; where the fundus and body of the sac is partially or completely divided into two lumens by a longitudinal septum, and the two lobes join in the infundibulum and continue with a common cystic duct. Vesica fellae duplex, where there are two separate fundus, body, infundibulums and two separate cystic ducts [1].
Cases with gallbladder duplication have increased tendency towards development of inflammation and gallstones due to inadequate biliary drainage [4]. Differential diagnoses include gallbladder diverticulum, folded gallbladder, Phrygian cap, choleduct cyst, pericholecystic fluid, focal adenomyomatosis and vascular fibrous band [4,5].
It is important that anatomy of gallbladder and biliary tract are clearly visualized with radiological methods at the preoperative period in order to prevent possible surgical complications associated with gallbladder duplications [4,6]. Only half of the cases can be accurately diagnosed [7]. Oral cholecystography, USG, scintigraphy, MRCP, endoscopic retrograde cholangio-pancreatography (ERCP), and percutaneous transhepatic cholangiography can be used in diagnosis [8]. Due to its extensive availability, USG is the first method to aid in the diagnosis. It may be difficult to clearly visualize biliary tract in USG, and USG is
particularly inadequate for diagnosing type-1 duplication. MRCP or ERCP can provide more accurate information in such a case. This detailed anatomical information will aid the surgeon to reduce the risk of injury to the biliary tract during laparoscopic cholecystectomy. Our case was diagnosed with type-1 duplication with preoperative imaging methods (USG and MRCP); however, postoperative gross examination revealed that the sacs were draining into the common hepatic duct via two separate cystic ducts (type-2 duplication). Therefore, MRCP may not always aid in diagnosis of cystic duct duplication.
As long as gallbladder duplications are asymptomatic, they do not require treatment. Laparoscopic cholecystectomy is recommended for type-1 gallbladder duplications. For type-2 duplication, some authors advocate open cholecystectomy to avoid injury to common bile duct and right hepatic artery [7]. In their review including 21 cases with gallbladder duplications, Walbot et al., reported that laparoscopic cholecystectomy was a very successful technique [9]. Besides surgeon’s laparoscopy experience and preoperative detailed anatomical knowledge, careful dissection is also important for perioperative detection of the anatomical variations [10]. Perioperative cholangiography can be used as necessary for demonstration of the anatomy and the variations [11].
CONCLUSIONGallbladder duplication is a rare congenital anomaly, and
anatomy of the biliary tract and neighboring vascular structures should be carefully defined in these cases. In symptomatic cases with gallbladder duplication, laparoscopic cholecystectomy is a convenient and reliable surgical method.
REFERENCES1. Boyden EA. The accessory gallbladder: an embryological and com-
parative study of aberrant biliary vesicles occurring in man and the domestic mammals. Am J Anatomy. 1926; 38: 177-231.
2. Harlaftis N, Gray SW, Skandalakis JE. Multiple gall-bladders. Surg Gynecol Obstet. 1977; 145: 928-934.
3. Gross RE. Congenital anomalies of the gallbladder. A review of 148 cases, with report of a double gallbladder. Arch Surg. 1936; 32: 131-162.
4. Ozgen A, Akata D, Arat A, Demirkazik FB, Ozmen MN, Akhan O. Gall-bladder duplication: imaging findings and differential considerations. Abdom Imaging. 1999; 24: 285-288.
5. Gigot J, Van Beers B, Goncette L, Etienne J, Collard A, Jadoul P, et al. Laparoscopic treatment of gallbladder duplication: a plea for removal of both gallbladders. Surg Endosc. 1997; 11: 479-482.
6. Brodsky D, Drevet D, Champion M, Joffre P. Gallbladder duplication. Apropos of a case of echographic finding. J Radiol. 1994; 75:195-198.
7. Kim RD, Zendejas I, Velopulos C, Fujita S, Magliocca JF, Kayler LK, et al. Duplicate gallbladder arising from the left hepatic duct: report of a case. Surg Today. 2009; 39: 536-539.
8. McDonald KL, Lwin T. Sonographic and scintigraphic evaluation of gallbladder duplication. Clin Nucl Med. 1986; 11: 692-693.
9. Walbolt TD, Lalezarzadeh F. Laparoscopic management of a dupli-cated gallbladder: a case study and anatomic history. Surg Laparosc Endosc Percutan Tech. 2011; 21: e156-158.
Figure 2 Two gallbladder sacs.
Figure 3 Gross examination of gallbladder at back table.
http://onlinelibrary.wiley.com/doi/10.1002/aja.1000380202/fullhttp://onlinelibrary.wiley.com/doi/10.1002/aja.1000380202/fullhttp://onlinelibrary.wiley.com/doi/10.1002/aja.1000380202/fullhttps://www.ncbi.nlm.nih.gov/pubmed/337542https://www.ncbi.nlm.nih.gov/pubmed/337542https://www.ncbi.nlm.nih.gov/pubmed/10227894https://www.ncbi.nlm.nih.gov/pubmed/10227894https://www.ncbi.nlm.nih.gov/pubmed/10227894https://www.ncbi.nlm.nih.gov/pubmed/9153181https://www.ncbi.nlm.nih.gov/pubmed/9153181https://www.ncbi.nlm.nih.gov/pubmed/9153181https://www.ncbi.nlm.nih.gov/labs/articles/8176679/https://www.ncbi.nlm.nih.gov/labs/articles/8176679/https://www.ncbi.nlm.nih.gov/pubmed/19468813https://www.ncbi.nlm.nih.gov/pubmed/19468813https://www.ncbi.nlm.nih.gov/pubmed/19468813file:///H:/xampp/htdocs/JSCIMED/SciMed/Articles/Liver/V4/4.2/I/Sonographic and scintigraphic evaluation of gallbladder duplication.file:///H:/xampp/htdocs/JSCIMED/SciMed/Articles/Liver/V4/4.2/I/Sonographic and scintigraphic evaluation of gallbladder duplication.https://www.ncbi.nlm.nih.gov/pubmed/21654293https://www.ncbi.nlm.nih.gov/pubmed/21654293https://www.ncbi.nlm.nih.gov/pubmed/21654293
Central
Ergün et al. (2017)Email:
J Liver Clin Res 4(2): 1036 (2017) 3/3
Ergün S, Akıncı O, Tosun Y, Kandemirli SG, Velidedeoğlu M, et al. (2017) Gallbladder Duplication: A Rare Case Presentation. J Liver Clin Res 4(2): 1036.
Cite this article
10. Cummiskey RD, Champagne LP. Duplicate gallbladder during laparo-scopic cholecystectomy. Surg Laparosc Endosc. 1997; 7: 268-270.
11. Causey MW, Miller S, Fernelius CA, Burgess JR, Brown TA, Newton C. Gallbladder duplication: evaluation, treatment, and classification. J Pediatr Surg. 2010; 45: 443-446.
https://www.ncbi.nlm.nih.gov/pubmed/9194295https://www.ncbi.nlm.nih.gov/pubmed/9194295https://www.ncbi.nlm.nih.gov/pubmed/20152372https://www.ncbi.nlm.nih.gov/pubmed/20152372https://www.ncbi.nlm.nih.gov/pubmed/20152372
Gallbladder Duplication: A Rare Case PresentationAbstractIntroductionCase Presentation DiscussionConclusionReferencesFgiure 1Fgiure 2Fgiure 3
Top Related