







Languages
Pages
Legal


“FRACTURE RESISTANCE OF ENDODONTICALLY
TREATED MAXILLARY INCISORS WITH
DIFFERENT POST AND CORE MATERIALS: A
COMPARITIVE EVALUATION”
Dissertation submitted to
THE TAMILNADU Dr. M.G.R. MEDICAL UNIVERSITY
In partial fulfillment for the Degree of
MASTER OF DENTAL SURGERY
BRANCH IV
CONSERVATIVE DENTISTRY AND ENDODONTICS
MAY 2020

CERTIFICATE
This is to certify that DR. GANESHAMOORTHY.T post graduate student
(2017-2020) from the Department Of Conservative Dentistry and Endodontics,
J.K.K.Nataraja Dental College, Komarapalayam, Namakkal District–
638183,Tamilnadu has done the dissertation titled “FRACTURE RESISTANCE
OF ENDODONTICALLY TREATED MAXILLARY INCISORS WITH
DIFFERENT POST AND CORE MATERIALS: A COMPARITIVE
EVALUATION” under my direct guidance and supervision in the partial fulfillment
of the regulations laid down by THE TAMIL NADU DR. M.G.R MEDICAL
UNIVERSITY, CHENNAI, FOR M.D.S BRANCH – IV CONSERVATIVE
DENTISTRY AND ENDODONTICS DEGREE EXAMINATION. It has not been
submitted (partial or full) for the award of any other degree or diploma.
Dr. J.V. Karunakaran. M.D.S,
Professor & Head, Department of Conservative Dentistry & Endodontics, J.K.K.Nataraja Dental College Komarapalayam, Namakkal Dist – 638183, Tamilnadu.
Dr. A. Siva Kumar. M.D.S,
Principal, J.K.K.Nataraja Dental College Komarapalayam, Namakkal Dist – 638183, Tamilnadu.
CERTIFICATE – II
This is to certify that this dissertation work titled “FRACTURE
RESISTANCE OF ENDODONTICALLY TREATED MAXILLARY INCISORS
WITH DIFFERENT POST AND CORE MATERIALS: A COMPARITIVE
EVALUATION” of the candidate DR. GANESHAMOORTHY.T with registration
number 241717101 for the award of MDS in the branch of CONSERVATIVE
DENTISTRY AND ENDODONTICS. I personally verified the urkund.com website
for the purpose of plagiarism check. I found that the uploaded thesis file contains from
introduction to conclusion pages and result and result shows ONE percentage of
plagiarism in the dissertation.
Guide & Supervisor Sign with Seal


ACKNOWLEDGEMENT
I take this opportunity to sincerely thank my post graduate teacher and my
guide Dr.J.V.Karunakaran.M.D.S, Professor and Head, Department of
Conservative Dentistry & Endodontics, J.K.K.Nattrajah Dental College, for his
academic and technical assistance, perseverance in motivating and supporting
me throughout my study period.
My sincere thanks to Dr.A.Sivakumar.M.D.S, Principal, J.K.K. Nattrajah
Dental College,who had helped with his advice and immense support throughout my
postgraduate curriculum.
I would like to express my sincere gratitude to Dr.N.S.Mohan Kumar.M.D.S,
Professor, Dr.S.Senthil Kumar.M.D.S, Reader, Department of Conservative
Dentistry & Endodontics J.K.K.Nattraja Dental College, for his valuable
suggestions, support and encouragement throughout my post graduate curriculum.
I extend my sincere thanks to Mr. Rajaganeshan, Chief Administrative
Officer, J.K.K.Nattraja Dental College & Hospital, for his constant support
throughout my study period.
I thank Dr.Satyanarayanan.M.D.S, Reader Dr.JayaprakashM.D.S, Senior
Lecturer, Dr.Ragavendran.M.D.S, Senior Lecturer, Dr.Chris Susan Abraham
M.D.S, Dr.C.S.Anagha M.D.S Senior Lecturer for their support, guidance and
constant encouragement throughout the completion of this work.
I am profoundly thankful to Mr. Muthukumar, in PSG Institute of
Technology, for helping in fracture resistance testing and I thank Dentcare Dental,
for guiding in processing the samples.
I extend my gratefulness to Mr. Ramakrishnan, our College Librarian’s for
their valuable assistance rendered during the course of the study.
I am thankful to Mr. Chinnarasu, Dental Technician, and our department
support staff for their help throughout my thesis.
My sincere thanks to Mr.M.Prasad Krishnan, for his guidance in
biostatistics. I thank Mr. Murali Sundar Chakra Printers, SPY Printers, Erode for
processing the dissertation.
I thank all my batchmates, colleagues, friends and family for their eternal
support. Above all, am thankful to God Almighty, to have given me the strength to
choose the right path and to have given these wonderful people in my life.
CONTENTS
S.No. INDEX PAGE No.
1. INTRODUCTION 1
2. REVIEW OF LITERATURE 7
3. MATERIALS AND METHODS 26
4. RESULTS 38
5. DISCUSSION 43
6. SUMMARY 61
7. CONCLUSION 62
8. BIBLIOGRAPHY 63
INTRODUCTION
Introduction
1
Endodontically treated teeth have been reported to be more susceptible to
fracture when compared to vital teeth. This necessitates adequate protection of
remaining tooth structure by proper restoration protocols. Excessive tooth structure
removal during endodontic therapy and subsequent dehydration of both coronal and
radicular dentin are principal factors which have been responsible for affecting the
fracture resistance of restored tooth structure after completion of endodontic
treatment procedure.The remaining dentin in a endodontically treated tooth should
be preserved as resistance to fracture depends primarily on remaining root dentin
thickness, especially in the buccolingual direction. (Sedgley and Messer in 1992)80
A number of reasons have been put forward for the tooth being susceptible
for fracture of root structure. This includes loss of tooth structure due to caries or
trauma, excessive removal of tooth structure during root canal preparation, the
dehydration of dentin subsequent to endodontic treatment, excessive radicular
dentinal structural loss during post space preparation, creation of excessive stress
during obturation and increased use of higher concentration of irrigants with
prolonged exposure times. This in a clinical situation would mean a reduction in the
long term survival rate, which is undesirable. The achievable target of endodontic
therapy should be reinforcement of the residual tooth structure in such a way that it
prevents untoward events in the long term. (Johnson M.E., et al in 2000)38
.
The anatomy of the root canal system and its variations, curvature of the
roots especially in posterior teeth pose a challenge to the clinician during preparation
of the root canal space, irrigant delivery, replacement and debridement in the apical
one third. In the case of curved canals this becomes even more difficult where in
order to access the apical third of the canal system and to achieve sufficient
Introduction
2
cleansing and debridement, a considerable amount of dentin in the coronal and
middle third of the root is removed which weakens the root structure and decreases
fracture resistance. (Sornkul E al in 1992)91
Earlier with hand instrumentation it was common practice to enlarge the
canal to three sizes from the first initial file to bind at the apical third of the root.
This enlargement allowed efficient cleansing and allowed the irrigants and
medicaments to reach the entire length of the canal system. The introduction of NiTi
hand instruments in endodontics almost two decades ago, improved preparations as
they were flexible. The most significant advantage was the predictable control of the
preparation. The alloy was resistant to corrosion, had the property of super-elasticity
and shape memory. With the advent of nickel titanium rotary instrumentation, things
changed and negotiation of even severely curved canals became much easier to
accomplish, was more complete and reduced the clinical working time. These rotary
instruments when used to prepare the canal exert considerable stresses in certain
areas resulting in formation of microcracks or craze lines which later predisposes the
tooth to vertical root fracture. These areas of most stress are mostly located in the
mid root canal wall area. It has been observed that lateral forces result in high stress
concentrations in radicular dentin in the coronal one-third of the root, and make the
teeth susceptible to fracture at the cemento enamel junction. There is a direct
proportional correlation between thickness of the root and the ability of the tooth to
resist lateral dislodging forces. The amount of remaining radicular and coronal
dentin in a tooth is directly proportional to the fracture resistance. (Lertchirakarn
V., et al in 2002)44
Introduction
3
A potential relationship between nickel titanium rotary instrument design and
the incidence of vertical root fractures has been reported. (Kim H.C et al in 2010)42
The geometry of the rotary instruments and their mechanical cutting action decide
the kind of difficulty and complications encountered during usage, as also the
operator training and skill.
Different types of fractures occur in roots of endodontically treated teeth and
can either be horizontal and vertical root fractures. Clinical studies have shown that
11% - 13% of extracted teeth with endodontic treatment done have been associated
with vertical fractures of the root (Fuss Z., et al in 1999)28. Craze lines and cracks
occur on the walls of the root canal which become areas of increased stress
concentration. These cracks can spread or extend slowly over a period of time to the
surface eventually resulting in a vertical root fracture (Yoldas O., et al in 2012)107.
Vertical fracture of the root is one of the serious complications of root canal
treatment procedure with a very unfavourable prognosis. This can occur before,
during, or after root canal obturation and most often leads to the removal of the
affected tooth. (Meister F et al in 1980)49
This has lead to various researchers looking to reinforce the structure of both
the crown and the root after the completion of endodontic treatment. The commonly
used root canal filling material is gutta percha in combination with a sealer. The low
elastic modulus of gutta percha presents little or no capacity to reinforce roots after
completion of endodontic therapy. (Ribero F.C., et al in 2008)64 Thus there is a
compelling need to develop materials and techniques to overcome the shortcomings
of current endodontic obturation materials and post endodontic restorations to
reinforce root structure post therapy. Coronal leakage after endodontic treatment

Introduction
4
procedure can be effectively prevented by use of intra orifice barriers. (Yavari H R.,
et al in 2012)106 This procedure involves placing additional material into the canal
orifices immediately after removal of the coronal portion of gutta-percha and sealer.
This also improves the fracture resistance of the root structure. (Roghanizad N.,
et al in 1996)70 Materials like resin modified glass ionomers, flowable composites,
and bonded amalgam can ideally be used as intra-orifice barriers. Swartz D B., et al
in 198395
stated that failure rates of endodontically treated teeth was almost double
in cases where the process of adequate post endodontic restoration has not been
followed. Newer generation of materials tend to improve the bond between radicular
dentin and the sealer and the sealer core interface which helps to increase the
fracture resistance and reduces ingress pathways. To reinforce the roots, the modulus
of elasticity of the root filling material should approximate that of radicular dentin.
(Williams C., et al in 2006)105 This presents the concept of a monoblock, which
aims at creating mechanically sound homologous units with radicular dentin.
This is easier said than done as the complexity of the canal system,
difficulties in access and cleansing present difficulties in predictably achieving the
target of a monoblock unit. Priming the radicular dentinal surface and creating a
bond between the sealer and dentin, sealer and core material would effectively
achieve this. A number of sealer and core materials have been formulated with the
aim of achieving this objective. The modulus of elasticity of the post, the filling
material and the sealer has to match that of radicular dentin so that the load stresses
are evenly distributed and borne by the components of the monoblock (Tay F.R.,
et al in 2007)96.

Introduction
5
Traditionally the rotary NiTi file systems were designed to be used in a
sequence and consisted of multiple rotary tools. Recently the advances in metallurgy
have seen introduction of newer file systems with a single rotary file which are
efficient. Also rotary files for use in reciprocating motion have been designed. A new
concept of endodontic file adjusting to the size of the canal and which works with
vibration and continuous irrigation, the self adjusting file system has been developed
and this system also prepares the canal system symetrically centered in the root
following the path of the canal limiting excessive removal of the radicular dentinal
structure. (Metzger Z, et al in 20)35 These single file systems have been based on
practicality, simplicity, reduce clinical working time and have been reported to
reduce the amount of stresses on the canal walls. They have also been recommended
and designed for a single use which tackles the issue of sterilization and cross
contamination.
The cast post and core method of post endodontic reconstruction has been
traditionally used and can be considered as gold standard. This technique has its own
limitations. There is a greater removal of radicular dentinal structure, need for
multiple clinical leading to more turnover time and has a elastic modulus which is
high compared to tooth structure. (200 Gpa) which can lead to fractures. (Sarkis-
Onofre R et al in 2014)85 Glass fiber posts have been used to restore
endodontically treated teeth, mainly because they are aesthetic, faster to execute and
have an elastic modulus near that of tooth structure (30-50 GPa).
For post preparations survival rates ranging from 71 to 100% for fiber posts
and 50 to 97.1% for metal posts have been reported. No difference in the survival
among different kinds of metallic posts were reported. No differences were reported
Introduction
6
between fiber and metal posts by most studies conducted. Studies also showed that
the longevity of the restored teeth is increased by remaining dentine height, number
of walls and ferrule. Post loss of retention was the reason for failure fiber posts.
Metallic post failures were mostly related to root fracture, post fracture or crown
or post retention loss. Metal based and fiber posts present similar clinical behavior
at short to medium term follow-up. Remaining dental structure and ferrule increase
the survival of nonvital teeth and long term analysis has been recommended.
(Malferrari et al in 2003)45
This study aims to comparatively analyse resistance to fracture of metallic
and fibre reinforced post and core preparations in upper central incisor teeth.

REVIEW OF
LITERATURE
Review of Literature
7
CampanellaV., et al in 201922 attempted to analyse the clinical fitting of
a cast metal post and core obtained by means of an intraoral optical scanning and
digital workflow. They noted that Customization of post-and-cores using computer-
aided-design and computer-aided-manufacturing (CAD-CAM) requires the scanning
of a pattern and the subsequent digital design. The case report describes the
production of a CAD-CAM customized post-and-core designed from an intraoral
scan and milled from a metal block. The use of an intraoral scanner for post-
endodontic rehabilitation could lead to a faster and more efficient CAD-CAM
customized post and core realization. The use of a high resistance material such as
metal is paramount in cases with high loss of coronal structure. The patient has been
treated with bisphosphonate for years. The risk of osteonecrosis of the jaw after
extraction was high.
Stankiewicz NR and Wilson in 199893 reviewed the literature regarding the
use of a ferrule for post and core preparations. They noted that a ferrule is a metal
ring or cap used to strengthen the end of a stick or tube. It has been proposed that the
use of a ferrule as part of the core or artificial crown may be of benefit in reinforcing
root-filled teeth. They observed that literature demonstrates that a ferrule effect
occurs owing to the artificial crown bracing against the dentin extending coronal to
the crown margin. Overall, it can be concluded that a ferrule is desirable, but should
not be provided at the expense of the remaining tooth or the root structure.
Robbins JW., et al in 200268 in their article aimed to provide a rationale for
the restoration of endodontically treated teeth. Treatment recommendations have
been made in the areas of post design, placement technique, cements, core materials,
and definitive restorations, based on a review of the clinical and laboratory data.
Review of Literature
8
Fokkinga WA., et al in 200426 did a structured analysis of in vitro failure
loads and failure modes of fiber, metal, and ceramic post-and-core systems and
sought to aggregate literature data on in vitro failure loads and failure modes of
prefabricated fiber-reinforced composite post systems and to compare them to those
of prefabricated metal, custom-cast, and ceramic post systems. They found that
significantly more favorable failures occurred with prefabricated post systems than
with prefabricated and custom-cast metal post systems. The authors concluded that
the variable "post system" had a significant effect on mean failure loads and that the
fibre reinforced post systems more frequently showed favorable failure modes than
did metal post systems.
Aritopoulou II., et al in 20062 in their review of materials used in post and
core systems discuss a plethora of prefabricated post and core materials currently
available for the restoration of endodontically treated teeth. The materials presented
demonstrate a variety of mechanical properties and esthetic potential, while the
selection of the optimum post and core system depends upon clinical judgment and
the specific clinical situation.
A comparative study of fracture resistance of endodontically treated teeth
filled with Resilon and guttapercha in a in-vitro setting was done by Shetty R.R.,
et al in 200982 and they found that Resilon was superior and the results were
statistically significant. The weakest tooth in terms of fracture resistance were those
that belonged to the guttapercha without sealer. The authors also note that in this
clinically relevant comparison between Resilon and guttapercha, the monoblock
concept is important not only to resist microbial leakage through the material, but
also holds the root as a single unit thereby increasing fracture resistance.

Review of Literature
9
A new concept in endodontic files, the self adjusting files was discussed by
Metzger Z., et al in 201035 and they compared it with the rotary nickel titanium file
systems. This was a single file system which was designed as a hollow thin
cylindrical nickel titanium lattice that adapts to the cross section of the root canal.
This file is used after preparation of the canal to # 20 k-file. It was operated with a in
and out motion with vibration and continuous irrigant flow which is also activated
by vibration. The self adjusting file is operated with a transline vibration resulting in
circumferential pressure which allows the files abrasive surface to remove a thin
uniform hard tissue layer from the entire root canal surface resulting in a canal with
similar cross-section but with larger dimensions. The straightening of the root canals
was also reduced due to lack of a rigid metal core and high pliability. This concept
allowed the file to retain the original shape of the root canal both in cross-section as
well as longitudinally. The author claims that the file has got a high amount of
mechanical endurance and failure when it occurs happens as small tears in the metal
lattice network. They proposed this as a method of overcoming the many
shortcomings of the rotary nickel titanium file systems.
The mechanical properties of the self adjusting files system was evaluated by
Hof R., et al in 201035 and they observed that this file system was mechanically
sound and was able to endure the canal preparation procedure with very little loss of
efficiency under the recommended operating conditions. They noted that the irrigant
flow was within the confines of the canal and did not cross the apical constriction.
The reduction in efficiency was found to be about 40% after continuous operation
for 30 minutes. They also found that the self adjusting file was elastically
compressible from a dimension of 1.5mm to the size of a #20 k-file and that

Review of Literature
10
compressing the self adjusting file creates a circumferential force which coupled
with in and out vibration and rough surface removes dentin from the canal walls.
The current developments in rotary root canal instrument technology and
clinical use was reviewed by Peters O.A., et al in 201060. The review summarised
clinical and laboratory findings for several current instruments with some guidelines
and usage parameters. This discuss the development of the nickel titanium alloy
developed first for the U.S. navy which has got a shape memory and super elasticity.
They compare it with steel instruments which can withstand a maximum of 3%
elastic deformation while Nickel titanium instruments can withstand a 7% elastic
deformation without permanent damage or plastic deformation. Steel can also
withstand upto 20 bending cycles whereas nickel titanium can be bent upto 1000
times and the difference is due to the atomic structure of the two alloys. They
discuss in detail the rotary instrument design, usage and fracture prevention of
nickel titanium instruments, and usage parameters and strategies. They observe that
clinical studies on the rotary instruments are sparse and that the results of the current
studies indicate that their use leads to a reduced incidence of gross preparation errors
and possibly improved clinical outcomes.
Vallabhaneni S., et al in 2012103 in their review of single file rotary
endodontic systems observe that the recently introduced files such as self adjusting
file, twisted file, wave one, protaper next and reciproc etc., claim to be able to
completely prepare and clean the root canals with only use of a single instrument
after the preparation of a glide path. This reduces clinical time, reduces instrument
fatigue, cost effective and reduces cross contamination. The advent of nickel
titanium rotary files removes the smear and debris effectively even from curved root

Review of Literature
11
canals. They suggest further clinical studies of these single file systems and discuss
in detail the individual method and technique of use of these systems.
In a in-vitro study of comparison of fracture resistance of roots of
endodontically treated teeth using different root canal filling materials Ravi N., et al
in 201261 found that the highest fracture resistance of almost more than 75% was
found in the resilon obturated roots when compared with other filling materials
(guttapercha) independent of the filling technique used. The authors suggest long
term clinical studies which are evidence based to assess whether resilon reduces the
vertical root fractures clinically.
Rippe M.P., et al in 201347 evaluated the effect of the root canal filling
methods on resistance to root fracture. They also used finite element analysis to
assess the expansion of the root canal sealer in two different filling techniques. The
authors observed that vertical root fractures have been the cause of fracture of many
root canal treated teeth and are most likely caused by the propagation of small
critical and less pronounced defects rather than the force exerted during the filling
procedure or the canal preparation. These fractures occur in the area of increased
occlusal stresses during mastication that originate in small defects and propagate
through small and constant impulses which result in root fracture. They also
discussed the role of the sealer expansion as one of the cause of stress concentration
in the root canal which would weaken the root. They found that the filling technique
influenced the fracture strength but did not influence the fracture type. The finite
element analysis revealed that greater the sealer thickness the greater the
concentration of the stresses in the root canal.

Review of Literature
12
Capar I.D, et al in 201413 in their evaluation of the fracture strength of roots
instrumented with self adjusting file and the protaper rotary systems concluded that
instrumentation with both the systems did not change the fracture strength of the
standardized roots with respect to their cross-sectional diameter and weight within
the limitation and standardization conditions of this study. This study was a in-vitro
study on mandibular premolars with straight canals. They observe that
standardization of the samples is an important step and a lot of variables could affect
the results of the study. The filling of the canals with a adhesive sealer did not
significantly strengthen the roots compared with instrumented but not filled canals.
Ertas H et al in 201425 evaluated the effects of the physical and
morphological properties of roots on the fracture resistance. The authors observed
that for study of fracture resistance of roots standardization is very important and the
roots if not distributed among the groups equally the variables could possibly affect
the results. This leads to large standard deviations within the groups rendering the
results meaningless prompting the researchers to use more number of samples. This
study principally aimed to determine how the physical properties of weight volume
and density and morphological properties of mesio-distal dimensions affect the
fracture resistance and the important criteria for standardization in fracture
resistance studies. They concluded that the volume or weight of the root as the most
important determining factor in root fracture and that the roots should be equally
distributed according to their volumes or weights rather than the morphological
dimensions which cannot closely simulate the entire strength of the root.
The fracture resistance of roots instrumented with three different single file
systems in curved root canals of the mesial root of maxillary molars was studied by

Review of Literature
13
Nur B.G. et al in 201557. They hypothesized that the instrument design, kinematics
and mechanical behaviour of the single file rotary systems affect the extent of
dentinal defects which subsequently translates into vertical root fracture
susceptibility. They compared three file systems namely Waveone, Reciproc and
Oneshape which are single file Niti systems. They concluded that the oneshape
rotary file system enhances the fracture strength of the roots as compared with the
control group within the limitations of this study. The Waveone and Reciproc rotary
file systems were found to be similar to the control group. All the three single file
systems had different designs and kinematics.
Muttlib N.A et al in 201553 in their study compared the adaptation of fiber
reinforced composite post system and cast post-and-core and found that both
cast post-and-core and fiber reinforced composite post systems showed similar
adaptation to the canal.
Mankar S et al in 201546 in their invitro assessment of the fracture
resistance of teeth restored with cast posts and cores with or without cervical ferrule
and cemented with zinc phosphate, glass ionomer, or resin cement. The authors
concluded that the inclusion of ferrule in tooth preparations for posts increased the
fracture resistance regardless of the luting agent.
Dastjerdi R et al in 201563 in their study compared the fracture resistance
of endodontically treated maxillary central incisors restored with different posts and
cores. And found that within the limitations of this study fiber reinforced posts
showed acceptable fracture resistance with favorable fracture patterns for
reconstruction of upper central incisors.

Review of Literature
14
Sreedevi S et al in 201592 an invitro study on the effects of post-
core design and ferrule on the fracture resistance of endodontically treated maxillary
central incisors observed that endodontically treated teeth have significantly
different physical and mechanical properties compared to vital teeth and are more
prone to fracture. The study aimed to compare the fracture resistance of
endodontically treated teeth with and without post reinforcement, custom cast post-
core and prefabricated post with glass ionomer core and to evaluate the ferrule effect
on endodontically treated teeth restored with custom cast post-core. Reinforcement
of endodontically treated maxillary central incisors with post and core, improved
their fracture resistance to be at par with that of endodontically treated maxillary
central incisor, with natural crown. The fracture resistance of endodontically treated
maxillary central incisors is significantly increased when restored with
custom cast post-core and 2 mm ferrule. The authors concluded that with the use of
a 2 mm ferrule, teeth restored with custom cast post-core had a significantly higher
fracture resistance than teeth restored with custom cast post-core or
prefabricated post and glass ionomer core without ferrule
Shamseddine L et al in 201681 investigated the influence of a contra bevel
on the fracture resistance of teeth restored with cast post and core and found that in
the presence of a ferrule and a crown in the anterior teeth, adding a secondary
ferrule to the cast post and core will not increase the resistance to fracture.
Shamseddine L et al in 201681 in a randomized clinical trial assessed the
influence of impression technique on the fabrication of cast metal posts. Direct and
indirect techniques are used for intra canal impression and fabrication of cast metal
posts. However, whether those techniques affect the accuracy of cast metal posts is
Review of Literature
15
unknown. The purpose of this randomized clinical trial was to evaluate the accuracy
of cast metal posts depending on tooth position and impression technique. Both of
the intra canal impression techniques resulted in cast posts that were shorter than the
impressed post space. The authors concluded that the discrepancy was greatest for
the indirect technique. Nevertheless, all posts were considered clinically acceptable
and were cemented.
Upadhyaya V., et al in 2016100 in their in vitro study to evaluated the effect
of design and material of post with or without ferrule on stress distribution using
finite element analysis. The highest amount of stress was seen in the cervical region.
Overall, the stress in the tapered post system was more than the parallel one.
FRC post and composite resin core recorded minimal stresses within the post but the
stresses transmitted to cervical dentin were more as compared to other systems.
Minimal stresses in cervical dentine were observed where the remaining coronal
dentin was strengthening by ferrule. The authors concluded that a rigid material
with high modulus of elasticity for post and core system creates most uniform stress
distribution pattern. Ferrule provides uniform distribution of stresses and decreases
the cervical stresses.
Schwendicke F., et al in 201678 in their study assessed the cost effectiveness
of a metal and fiber post systems to provide post-retained restorations. The risk of
tooth loss and other complications differs between different post systems, as do the
initial treatment costs. They assesses the cost-effectiveness of cast metal, preformed
metal, glass fiber, and carbon fiber post-retained restorations. The authors concluded
that patients not willing to invest additional money for longer tooth retention,
preformed metal seemed most suitable to retain restorations. For payers with
Review of Literature
16
additional willingness to pay, glass fibre post seemed suitable. Cast metal was only
cost effective under very high willingness to pay. Carbon fibre is not
recommendable on the basis of their cost effectiveness.
Kar S., et al in 201739 in their study compared the effect of ferrule length
on fracture resistance of endodontically treated mandibular premolar teeth, restored
with prefabricated glass fiber post luted with resin cement, composite core and a
full coverage metal crow. A ferrule has been described as a key element of tooth
preparation when using a post and a core. It is a vertical band of tooth structure at
the gingival aspect of crown preparation. It lessens the stress transmission to the
root which is due to forces from posts or bending during seating of the post. The
incorporation of a ferrule can help to withstand the forces of occlusion, preserve the
hermetic seal of the luting cement, and minimize the concentration of stresses at the
junction of post and core. The authors observed that the results of this study showed
that fracture resistance of endodontically treated teeth increases as ferrule length
increases.
MarchionattiA M E., et al in 20178 in their systematic review was to
compare the clinical performance and failure modes of teeth restored with intra
radicular retainers. Evaluated retainers were fiber (prefabricated and customized)
and metal (prefabricated and cast) posts, and follow-up ranged from 6 months to 10
years. Most studies showed good clinical behavior for evaluated intra-radicular
retainers. Reported survival rates varied from 71 to 100% for fiber posts and 50 to
97.1% for metal posts. Studies found no difference in the survival among different
metal posts and most studies found no difference between fiber and metal posts. Two
studies also showed that remaining dentine height, number of walls and ferrule
Review of Literature
17
increased the longevity of the restored teeth. Failures of fiber posts were mainly due
to post loss of retention, while metal post failures were mostly related to either root
fracture, post fracture and crown and/or post loss of retention. In conclusion, metal
and fiber posts present similar clinical behavior at short to medium term follow-up.
Remaining dental structure and ferrule increase the survival of restored pulpless
teeth. The authors felt that studies with longer follow up would throw more light on
the issue.
Savychuk A., et al in 201777 compared the impact of the post type (glass
fiber post-and-resin core or cast post-and-core) along with the ferrule effect on the
stress fields generated in endodontically treated mandibular lateral incisors and
canines using a finite element analysis. Maximum principal stresses in dentin were
highest in incisors, with a ferrule. Stress parameters in composite resin core in both
incisors and canines were critically close to the tensile failure limit of
the core material. Cast post-and-cores cemented in incisors without a ferrule
accumulated the highest stresses, exceeding the tensile failure limit of resin-
modified glass ionomer cement. They also observed that the tooth preparations with
a ferrule led to a remarkable rise in stress in the dentin of mandibular incisors but
favored the mechanical integrity of the restoration.
Tsintsadze N et al in 201797
assessed the push out strength, the cement
layer thickness and the interfacial nanoleakage of prefabricated fiber posts,
CAD/CAM fiber posts and metal cast posts cemented into oval-shaped root canals.
Sections from six roots per group were used to measure the cement thickness and
subsequently for the thin-slice push-out test, whereas the sections from the
remaining four teeth were assigned to interfacial nanoleakage test. The cement
Review of Literature
18
thickness around the posts was measured in micrometers on the digital images
acquired with a digital microscope using the Digimizer software. Thin-slice push-
out test was conducted using a universal testing machine at the crosshead speed of
0.5 mm/minute. The interfacial nanoleakage was observed under light microscope
and quantified by scoring the depth of silver nitrate penetration along the post-
cement dentin-interfaces. CAD/CAM-fabricated fiber posts achieved retention that
was comparable to that of cast metal posts and significantly higher than that of
prefabricated fiber posts. The cement layer thickness around CAD/CAM-fabricated
fiber posts was significantly lower than around prefabricated fiber posts, but higher
than that around cast metal posts. No differences were observed in interfacial
nanoleakage between CAD/CAM fabricated and prefabricated fiber posts, while
nanoleakage recorded in cast metal posts was significantly lower. CAD/CAM
fabricated fiber posts could represent a valid alternative to traditionally used posts
in the restoration of endodontically-treated teeth with oval or wide root canals,
offering the advantages of better esthetics, retention, and cement thickness values
that are comparable to cast post and cores.
Pantaleon S., et al in 201873 in this in vitro study examined the effect of
varying residual axial wall heights, residual coronal tooth structure, and the absence
of 1 proximal axial wall on the fracture resistance and failure mode of
endodontically treated teeth restored with metal posts. The authors found that the
specimens with 2-mm ferrule of uniform height were more resistant to fracture than
specimens with a 2-mm ferrule and 1 missing interproximal wall. An increased wall
height of 3 or 4 mm was associated with a significant increase in fracture resistance
and can compensate for the missing interproximal wall.

Review of Literature
19
Khiavi H A S., et al in 201841 in their study compared the fracture strength
of endodontically treated maxillary central incisors restored with nickel chromium
(Ni-Cr) and non-precious gold alloys. As fiber posts are not recommended for teeth
under lateral loads, a new alloy containing >80% copper was introduced with a
modulus of elasticity closer to that of dentin and easier preparation. Based on the
results of this study the authors concluded that the fracture strength of teeth restored
with cast non precious gold post and cores was significantly higher than that of
teeth restored with cast nickel chromium post and cores. Due to adequate
mechanical properties, non-precious post and cores seem to be a suitable choice for
restoration of severely damaged anterior teeth, provided that other properties are
proven to be acceptable.
Nokar S., et al in 201856 investigated the stress distribution of
different post and core materials in radicular dentin by three-dimensional finite
element analysis method. The authors were able to detect two stress concentration
sites with the first group showing the lowest stress levels in the cervical region,
while the stress levels detected in the second group were higher than those in the
first group and lower than those found in the third group. Fiber-reinforced posts
induced a higher stress concentration between the middle and cervical thirds of the
root compared to other posts. Based on the observations the authors concluded that
since cast posts induce lower stresses in dentin, they are recommended for clinical
use. Fiber reinforced posts and all ceramic restorations caused the maximum
stresses in dentin.
Hendi A R., et al in 201934 in an vitro study compared the retention of posts
and cores fabricated using full-digital, half-digital, and conventional techniques.
Review of Literature
20
They assessed the accuracy of these techniques in terms of the presence of apical
gap. They observe that Conventional cast metal posts and cores are fabricated using
direct and indirect techniques, both of which need impression materials and
considerable laboratory time and work scheduling and that Digital techniques have
the capacity to substitute for conventional methods in fabricating the posts and
cores but their accuracy remains unknown. The apical gap of each post in the canals
was defined with parallel digital radiography. The data were analyzed using the
Kruskal-Wallis test (α=.05) and Mann-Whitney test at the adjusted α=.016. They
came to the conclusion that the conventional technique was more accurate and
resulted in higher retention than both the full and half digital techniques. However,
the retention and gap of all the posts fell within clinical guidelines recommended.
Alkhatri R., et al in 20191 measured the fracture resistance and failure
modes of endodontically treated teeth restored with three different computer aided
design or computer aided manufacturing (CAD/CAM) fabricated post and core
systems. Fracture of the post and core or fracture of the root above the level of the
acrylic resin was considered as a favorable fracture, while nonfavorable fractures
were those where the root fracture occurred below the level of the acrylic resin. The
authors found that there was no significant difference between metal and zirconia
samples in terms of nonfavorable fracture, and that PICN material can be used in the
fabrication of post and core assemblies using CAD/CAM.
In their retrospective clinical study Martino N., et al in 201948 evaluated the
clinical survival rate of custom fabricated cast metal and prefabricated (both metal
and fiber reinforced composite resin post) post and cores as a function of patient
and restoration related variables. They found that the mean survival time for each

Review of Literature
21
group to be 12.0 years for fiber reinforced composite resin posts, 11.8 years
for cast metal post-and-cores, and 10.2 years for prefabricated metal posts. Although
the mean survival time differed by 1.8 years among groups, with prefabricated metal
posts having a slightly higher risk of failure, this effect was not statistically
significant (P=.067). The effect of post type also failed to reach significance when
controlling for patient demographics and post position in a Cox proportional hazards
analysis (P=.106). However, the Cox model did show that survival was associated
with tooth position (P=.003), cement (P=.021), and type of restoration (P<.001).
Fontana PE., et al in 201927 investigated the influence of ferrule thickness
on fracture resistance after mechanical cycling of teeth restored with different
intracanal posts. A thicker ferrule statistically increased the fracture resistance only
for cast post and core when it was at least 1 mm thick, despite causing more
unfavorable failures. The authors suggest that the ferrule thickness should be
considered when choosing different intracanal posts, to reduce the occurrence of
unfavorable failures. In the absence of a ferrule, the use of a cast post and core
presents more favorable failures, and in the presence of a 1 mm thick ferrule, the use
of a glass fiber post seemed a better clinical decision.
Schwindling F S., et al in 201979 proposed the concept and feasibility of a
three dimensional guided removal and preparation of dental rot posts. They
presented a novel method to remove glass fiber reinforced composite root posts in a
minimally invasive way while simultaneously shaping the canal for a new post
endodontic restoration. A conebeam computed tomography scan was imported into
conventional implant-planning software and matched to a stone cast of the intraoral
situation. Position, length, and axis of the future post were planned virtually. Based

Review of Literature
22
on this planning, a tooth-supported splint was three dimensionally printed. This
splint allowed use of a 2.2-mm spiral drill for removal of the fractured post and
shaping of the root canal for a new cast post-and-core. This metal post-and-core was
adhesively cemented and prepared for a zirconia single crown veneered in the labial
aspect. This method currently requires use, ionizing three dimensional imaging.
Additional refinements to this approach can be made regarding spiral drill design
and coating as well as regarding the post-and-core workflow. The authors concluded
that guided post endodontic management is feasible. More research is needed to
balance higher radiation doses against therapeutic success.
Byakova SF., et al in 201911 compared the accuracy of cone beam
tomography ex vivo and in vivo for the detection of artificially created large and
small vertical root fractures in extracted teeth restored with post and core. They
found that the width of the fracture affected the detectability of vertical root
fractures invitro in teeth with metal cast post cores. Root fractures in vivo was less
detectable because of low image quality, making the assessment of sound tooth
tissue impossible.
Ozturk C., et al in 201958 compared the fracture resistance and fracture
mode of endodontically treated thin walled teeth restored with different post
systems. Restoration of the teeth with extensive root canals with different post
systems is a challenge for clinicians. Evaluation of these systems is important for
clinical success. The authors observed that the type of fracture encountered with
fibre posts mode would permit repair of the tooth and was favourable.
Bacchi A., et al in 20193 evaluated the influence of ferrule and the post type
on the fracture strength and stress distribution in premolar teeth. They were prepared
Review of Literature
23
with a cast post and core or a glass fiber post with a core with or without a ferrule
and fracture strength and failure patterns assessed. Stress distribution was evaluated
using finite element analysis. The authors concluded that the Ferrule effect was
shown to be more important than type of post used in the analysis. Both posts
showed potential to withstand functional loads irrespective of presence of ferrule.
Bakirtzoglou E., et al in 20194 in their in vitro analysis of the retention and
resistance form of complete coverage restorations with two different types of cast
post and core designs. The authors concluded that the standard cast post and core
design with a 2 mm of ferrule height offers superior resistance, although not
statistically significant (p=0.061), when compared to the core design encircling the
axial wall ferrule. Both cast post and core designs offered equal retention with
different failure modes during decementation.
Sary SB., et al in 201976
studied the effect of technique of restoration of the
fracture resistance of endodontically treated teeth with flared root canals. This study
was done in anterior teeth and compared the impact of post and core systems on
resistance to fracture of endodontically treated anterior teeth with flared root canals
and to assess their fracture pattern. The authors observed that the resistance to
fracture of wide root canals can be enhanced by using one piece CAD-
CAM post and core as an alternative to the use of either glass fiber post relined with
composite resin increasing the thickness of luting cement or the use of cast post and
core system. They also noted that as this was an in vitro investigation and further in
vivo studies are needed to confirm the same.
Haralur S B., et al in 201831 evaluated the efffect of multiple fiber
reinforced composite and Ni-Cr cast posts on the resistance to fracture of

Review of Literature
24
endodontically treated teeth with wide root canals. The endodontically treated teeth
with thin remaining radicular dentin thickness are inherently predisposed to fracture.
Therefore it requires the proper selection and the execution of post and core
technique used. The posts were cemented with self-adhesive resin cement and
subsequently restored with full veneer metal crown. The restoration of
endodontically treated teeth with larger canals by multiple fibre reinforced
composite and metal posts provides substantially higher fracture resistance in
comparison to wider single post.
Carvalho M A., et al in 201814 in this critical present a survey of the current
knowledge on adhesive approaches to restore endodontically treated teeth with and
without extensive coronal tissue loss. Adhesive procedures have changed the way to
restore endodontically treated teeth. It started with the shift from cast post and core
to fiber post. The original focus on strength also shifted towards failure modes,
revealing that catastrophic failures are still a concern when restoring endodontically-
treated teeth even with fiber posts. As an alternative, postless approaches have been
proposed in order to improve the chances of repair. The preservation of tooth
structure of endodontically treated teeth is paramount. Partial versus full coverage of
the treated tooth, the role of the ferrule, the post type effect on catastrophic failures
and postless alternatives as endocrowns and postless buildups are reviewed. There is
a consensus that the remaining tooth structure plays an important role in tooth
survival, although the current literature still is contradictory on the influence
of post type on root fractures as well as the benefits of avoiding a post or partially
restoring a tooth. More clinical studies should be carried out with the modern
postless adhesive alternatives to conventional approaches.
Review of Literature
25
Munaga S., et al in 201852 in their comparative clinical evaluation of
composite overcast gold post and core buildups in endodontically treated teeth
observe that the management of non-vital teeth includes endodontic treatment and
restoration followed by post and core restoration in selected cases. And conducted
the present study to compare the indirect cast post, and core buildup with direct
composite post build up in patients. The authors concluded that both composite
post buildup and cast gold post and core build-up exhibited similar properties and
therefore have recommended both of these techniques for clinical use.
Haralur S B., et al in 201931 in their study compared the teeth restored with
custom-made cast metal posts and cores cemented with different luting agents in
terms of coronal microleakage after thermocycling. The apical seal provided by a
root canal filling may be breached via coronal leakage. The authors observed that in
this study a complete coronal seal was not achieved with any of the luting agents.
The highest and the lowest degree of microleakage was by zinc phosphate and
Panavia luting agents, respectively.

MATERIALS AND
METHODS

Materials and Methods
26
ARMAMENTARIUM
Collection of teeth
1. Disposable gloves (Dispodent, Chennai)
2. 2% Thymol solution (Alpha chemicals, Maharastra, India)
3. Normal saline solution (Nirlife Health Care, Nirma products, India)
4. Vented labelled glass bottles
5. Tissue forceps (GDC Fine Crafted Pvt Ltd, Hosiarpur)
6. Large bore needles
Selection & standardization of samples
1. Stainless steel trays (GDC Fine Crafted Pvt Ltd, Hosiarpur)
2. Glass beakers
3. Ultrasonic scaler unit (Woodpecker)
4. Illuminated Magnifying Lens
5. Electronic weighing Scale
6. Vernier Calipers Digital
7. Diamond disc (AXIS,SYBRON ENDO, Kevakarr group, Denaher USA)
8. Indelible marker pen bold and fine (Camlin)
9. DG-16 Endodontic probe (Dentsply Maillefer, Ballaigues, Switzerland)
10. Operating microscope (AM-3000 Series, China)
11. Stainless steel tweezers(GDC Fine Crafted Pvt Ltd,Hosiarpur)
12. RadioVisiography unit (Skanray Technologies Pvt Ltd, India)
13. RVG analysis software
Canal preparation
1. Size 8, 10, 15 K file of 21mm length (Dentsply, Maillefer, Ballaigues,
Switzerland) Endo block (Dentsply Maillefer, Ballaigues, Switzerland)

Materials and Methods
27
1. X-smart plus (Dentsply Maillefer, Ballaigues, Switzerland)
2. 28 gauge side-vent needle (Prime dent)
3. 5ml syringe with leur-lock needle (Dispovan, Hindustan Syringes and
Medical Devices Ltd, Faridabad, India)
4. 5ml, 10ml Unolock Syringe (Hindustan Syringes and Medical Devices Ltd,
Faridabad, India)
5. Endoprep RC (Anabond Stedman Pharma Research, India)
Irrigating solutions
1. Normal saline (Nirlife Health Care, Nirma products, India)
2. 5% Sodium Hypochlorite solution (Nice chemicals Pvt Ltd, India)
3. Sterile Distilled water (Ives drugs, Pvt Ltd, India)
4. 17% EDTA solution (pulpdent corporation, USA)
Obturation of samples
2. Lentulospiral size 25 (Mani Inc, Tochigi, Japan)
3. Hand spreaders 21mm size:15-40 (Mani Inc, Tochigi, Japan)
4. AH plus resin sealer (Dentsply Maillefer, Ballaigues, Switzerland)
5. Gutta percha points and paper points 2%,4% ,6% (Dentsply Maillefer,
Ballaigues, Switzerland)
6. Mixing pad and agate spatula (GC Corporation, Tokyo, Japan)
7. Spirit lamp (GDC Fine Crafted Pvt Ltd, Hosiarpur)
8. GP condenser (Dispodent , India )
9. GP cutter (Generic)
10. Cotton holder
11. Stainless steel tray (GDC Fine Crafted Pvt Ltd, Hosiarpur)
12. Heat carrier Touch N Heat (Sybron Endo, Kavo Kerr, Germany)

Materials and Methods
28
Post space preparation
1. Reamers (Mani Inc, Tochigi, Japan)
2. Files (Mani Inc, Tochigi, Japan)
Fabrication of post and core
1. Air rotor unit (NSK, Nakanishi INC, Tochigi, Japan)
2. Crown preparation kit (Diatech, Coltene Whaldent, Pvt Ltd, Mumbai)
3. Mouth mirror (GDC Fine Crafted Pvt Ltd, Hosiarpur)
4. Probe (GDC Fine Crafted Pvt Ltd, Hosiarpur)
5. Tweezer (GDC Fine Crafted Pvt Ltd, Hosiarpur)
6. Stainless steel tray (GDC Fine Crafted Pvt Ltd, Hosiarpur)
7. Fornax centrifugal induction casting machine (BEGO, Canada)
8. Phosphate bonded investment material (Adantatec)
9. Laser sintering machine (SISMA MYSINT 100, S.p.A. via dell'Industria,
136013 Piovene Rocchette (VI) Italy)
10. Geo crowax pattern material, Modelling wax (Renfert, Hilzingen, Germany)
11. Inlay wax Medium, Dental inlay casting wax, GC corporation, Tokyo, Japan)
12. Luxacore, (DMG Dental Milestones Guaranteed, Germany)
13. Reforpost, Angelus (Dental Avenue India Pvt Ltd, Mumbai)

Materials and Methods
29
Luting procedure
1. Cementation media type I Glass ionomer luting cement (Fuji GC corporation,
Tokyo, Japan)
2. Rely x (U200Self adhesive resin cement, 3M ESPE)
3. Mixing pad (GC Corporation, Tokyo, Japan)
4. Agate spatula (generic)
Preparation for Fracture testing
1. Sterile self sealing pouches (AK Product; West Bengal; India)
2. Base former unit – custom stainless steel (1.5” X 1.5” X 1.5”)
3. Epoxy resin polymer and monomer (ROTEX Roto Polymers And Chemicals
Orakkadu Village Chennai, India)
4. Emery paper (3M 100,180,400)
5. Storage containers (genric)
6. Mounted 3mm diameter Stainless Steel Tip or fracture testing
7. Stainless steel millimetre scale
8. Wax knife and carver set (GDC INDIA)
9. White soft paraffin (Medisan, Trichy, India)
10. Sticky wax (DPI Model Cement,Dental products of India, Mumbai)
11. Stainless steel wire - 19 Gauge (Sendent, Salem, TN)
12. Bunsen burner
Materials and Methods
30
Fracture testing
1. Universal testing machine (Zwick Roell Z010,Germany)
2. Storage media (SonyDVD-RW. Sandisk Ultra, Sandisk)
3. Digital SLR camera (Canon EOS 1300D)
Fracture strength analysis and tabulation
1. HP and DELL computing systems
2. Zip lock covers(5cmx5cm)
3. Storage boxes for individual groups
4. Magnifying loupe with illumination
5. Observation sheets
6. Software for fracture recording and analysis (Zwick Roell, 2125 Barrett Park
Drive, Suite 107 44 Kennesaw, GA, USA)
Fracture type analysis and tabulation
1. Magnifying loupe – Illuminated (Generic)
2. Observation sheets.
Statistical Analysis
1. SPSS Version 16.0 software for statistical analysis.

Materials and Methods
31
MATERIALS AND METHODS
1. Collection of teeth:
Seventy two extracted human permanent maxillary central incisor teeth were
collected and stored in isotonic saline solution for a maximum of 72 hours.
Sufficient protocols for infection control as per OSHA and CDC guideline
regulations in collection, storing, sterilization and handling were followed.
2. Selection of samples:
Teeth with mature and intact root apices were selected for the purpose of the
study. Teeth with gross destruction, restorations and those that were treated
endontically were discarded. They were then observed for presence of cracks under
magnification and those with such damage were excluded. The teeth thus selected
were cleansed ultrasonically and stored in normal saline solution at 4°C until use. A
total of forty eight teeth were selected for the purpose of the study.
3. Standardization of samples
The teeth which confirmed to the inclusion criteria were kept moist with
normal saline throughout the experimental procedure to avoid dehydration. The
mesiodistal and buccolingual diameters of the selected teeth at the level of the
cemento enamel junction was then tabulated with the help of digital Vernier
callipers. The samples were then weighed using a precision weighing machine and
the results tabulated. The samples were evenly distributed based on their weights
across the six experimental and control groups (n=8). The selected teeth were then
rinsed with distilled water and stored in normal saline at 4°C in separate glass
bottles.


Materials and Methods
32
4. Preparation of the Sample:
Access preparation was done and the working length was determined by
passively placing a size 15K file (Dentsply Maillefer, Ballaigues, Switzerland) into
the canal until the tip was visualized at the apical foramen using a magnifying loupe
and was adjusted to the apical foramen. Then the actual canal length was measured
and working length was calculated by subtracting 0.5mm from this measurement
and recorded for each sample.
5. Root Canal Preparation Technique
Canal preparation was done using hand files to a master apical file size of 40
using step back technique. 3% Sodium hypochlorite irrigation (8 ml) was used as
initial rinse during the cleansing and shaping of the canal system. The canal systems
of the experimental groups were prepared with hand files with care not to remove
excessive dentin.
6. Final Rinse of Samples
Subsequent to the canal preparation the samples were irrigated with a final
rinse of 5ml of the irrigant solution. 5ml of 17% EDTA was delivered using a 28-
gauge side vent needle (Neo endo). The exposure time of the final rinse solution was
three minutes. After the completion of three minutes a post-final rinse irrigation of
5ml of distilled water was done to flush out the remaining final rinse irrigant from
within the canal system.
7. Obturation of the samples
The canals were then dried and then coated with a sealer using a
lentulospiral. The roots were obturated using the cold lateral condensation technique


Materials and Methods
33
using gutta-percha points (2%) with a zinc oxide eugenol sealer. Excess gutta-percha
was removed using a gutta-percha cutter and entrance filling done with zinc oxide
eugenol cement. The filled samples were then stored at 24 degree Celsius. The
quality of root canal fillings were confirmed with radiovisiography. The samples
were then stored at 37°C at 100% relative humidity for 72 hours. Each group was
processed and stored separately for further analysis.
8. Post space preparation
With the use of a diamond disc (Mani Inc, Japan), the teeth were decoronated
3mm from the deepest point of cemento enamel junction by comparing mesial and
distal surfaces using, at a level corresponding to the clinical gingival margin Digital
Vernier Caliper. After decoronation, one fourth of length of entire samples were
marked using marker and the gutta percha has been removed using Touch N Heat
device.(Sybron Endo). The walls were cleared of the sealer using hedstrom files and
a size-1 peeso reamer with care not to remove radicular dentin. The samples were
assessed using radiovisiography for consistent finish and gutta-percha removal
from within the canal system.
9. Crown preparation
Crown preparation was done using TF–12 flat end tapered fissure bur (SS
White burs) with the tip diameter of 1mm around the finish line, core ferrule was
given using thin tapered fissure burs. A anti rotation notch was given for a depth of
about 2mm using Flat end tapered fissure bur on the thickest portion of the root to
prevent the rotational displacement of the cast post preparation.

Materials and Methods
34
10. Indirect Pattern Procedure For Cast Post And Core
In all groups, the excess gutta percha was removed using TOUCH N HEAT
(Sybron Endo, Kavo Kerr, Germany) after removal of the entrance filling. The post
space preparation was refined using Hedstrom files, Reamers and size 1 Peeso
reamers. A minimum apical seal of 5 mm of gutta-percha filling was retained. The
apical end of the post space preparation was assessed, gauged and standardised to a
specific width. The walls were cleansed so no sealer remained and sealed with
cotton plugs and stored.
14. Fabrication Of Cast Post And Core
GROUP I (ORDEN ALLOY POST AND CORE)
Direct technique was used to fabricate a post and core pattern using a
prepared stainless steel sprue former (18 g) with a medium Inlay wax (Dental inlay
casting wax, GC). The core height of all samples in the group was standardized to
3mm. A separating media was used to aid the easy removal and insertion of the
pattern. Subsequently after debubblizing and investing the pattern was cast (BEGO
Induction casting machine) with Non precious gold alloy (Orden alloy) using a lost
wax technique.
GROUP- II (GOLD ALLOY POST AND CORE)
Direct technique was used to fabricate a post and core pattern using a
prepared stainless steel sprue former (18 g) with a medium Inlay wax (Dental inlay
casting wax, GC). The core height of all samples in the group was standardized to
3mm. A separating media was used to aid the easy removal and insertion of the

Materials and Methods
35
pattern. Subsequently after debubblizing and investing the pattern was cast (BEGO
Induction casting machine) with gold alloy (20 carats) using a lost wax technique.
GROUP -III (COBALT CHROMIUM POST AND CORE)
Direct technique was used to fabricate a post and core pattern using a
prepared sprue former (18 g) with a modeling wax (Geo Crowax, Renfert, Hilfingen,
Germany). The core height of all samples in the group was standardized to 3mm. A
separating media was used to aid the easy removal and insertion of the pattern.
Subsequently after debubblizing and investing the pattern was cast (BEGO
Induction casting machine) with cobalt chromium alloy (Co Cr alloy (Colado CC,
Ivoclar,Vivadent) using a lost wax technique.
GROUP- IV (TITANIUM ALLOY)
Root canal impressions that were obtained using direct wax patterns were
scanned with a digital scanner to generate and transfer the data to digital design
software for three dimensional image generation. A special software was used to
design post and core which was then fabricated using a laser sintering process.
(SISMA MYSINT 100, laser metal fusion)
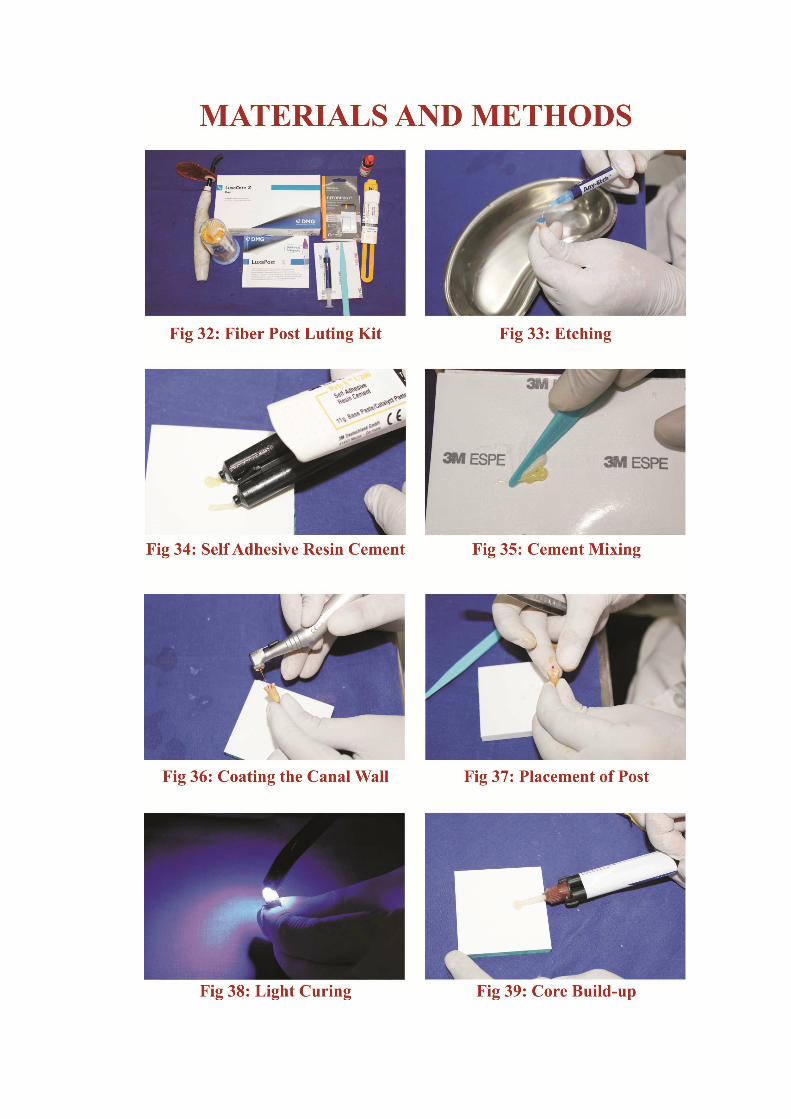
12. Post luting Core Preparation Technique For Glass And Carbon Fiber Post:
GROUP- V (GLASS FIBER POST)
The length of the post in the canal was marked and the trimmed glass fiber
post was replaced in the canal to confirm its length. A 37% phosphoric acid etchant
was applied into the canal for 15 seconds and the canal flushed with distilled water
(5ml). The canal was dried subsequently with paper points. The Rely X U200 Self
adhesive resin cement (3M ESPE) base and catalyst were mixed in 1:1 ratio on a

Materials and Methods
36
mixing pad for 10 seconds and applied into the post space with a lentulo spiral (size
25). The presilanated fiber Post (Luxapost, DMG Dental Milestones Guaranteed,
Germany) was then seated in the canal and the adhesive resin cement was light
cured for 30 seconds on each surface. The core was established with the successive
layered addition of a core buildup resin (Luxacore, (DMG Dental Milestones
Guaranteed , Germany) and finishing done.
GROUP- VI (CARBON FIBER POST)
The same procedure as in the glass fiber post was followed and a Carbon
Fiber Post (Reforpost, Angelus, Dental Avenue India Pvt Ltd, Mumbai) was then
seated in the canal and the adhesive resin cement was light cured for 30sec on each
surfaces. The core was established with the successive addition of composite resin
(Luxacore, (DMG Dental Milestones Guaranteed, Germany).
13. Luting the cast post and core
The metallic cast posts and cores were cut from the sprues tested for seating
and assessed with radiovisiography for apical fit after which they were luted to the
respective prepared teeth using type I glass ionomer cement (Fuji GC corporation,
Japan).
14. Finishing the crown preparation
The excess cement was removed and after 24 hours the refining of the crown
preparation was done with a tapering fissure bur flat end.
15. Preparation for fracture testing
The samples belonging to each group were removed from the temporary
bases and mounted on formers (1.5” X 1.5” X 1.5”) with the help of a custom made
Materials and Methods
37
stainless steel base block. The apical root ends embedded vertically along the long
axis of the block at an angle of 30 degrees in such a way that the crown of the tooth
was visible. The clear epoxy resin was prepared. poured and allowed to set for 72
hours and the sample blocks coded. The samples were kept covered by moist cotton
and wet towel to prevent dehydration till they were ready for fracture testing.
17. Fracture testing procedure:
The samples were tested with the help of a universal testing machine. A
custom made metal indenter of size 3 millimetres was mounted on the upper arm jig
and the tooth specimen block was mounted on the lower arm jig. A cross head speed
of 1mm/min was set and the load applied on the surface of the tooth vertically
parallel to the long axis of the tooth from above. The force required to fracture the
tooth sample was recorded in Newton.
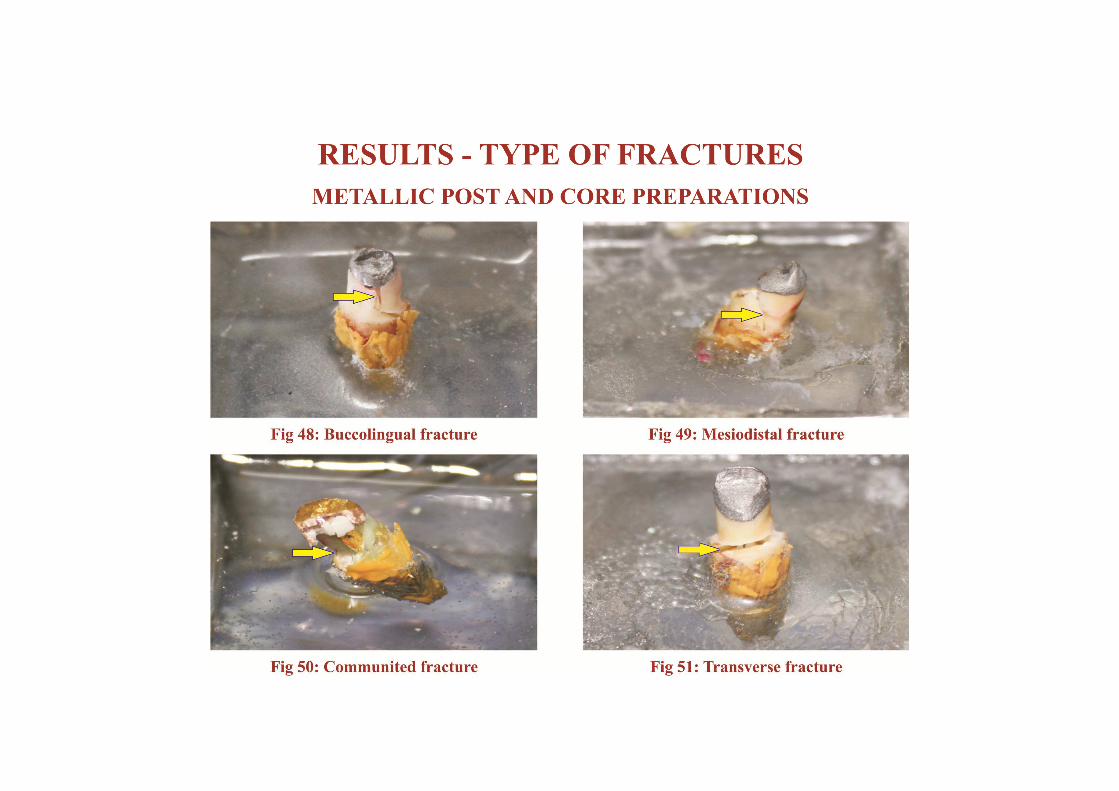
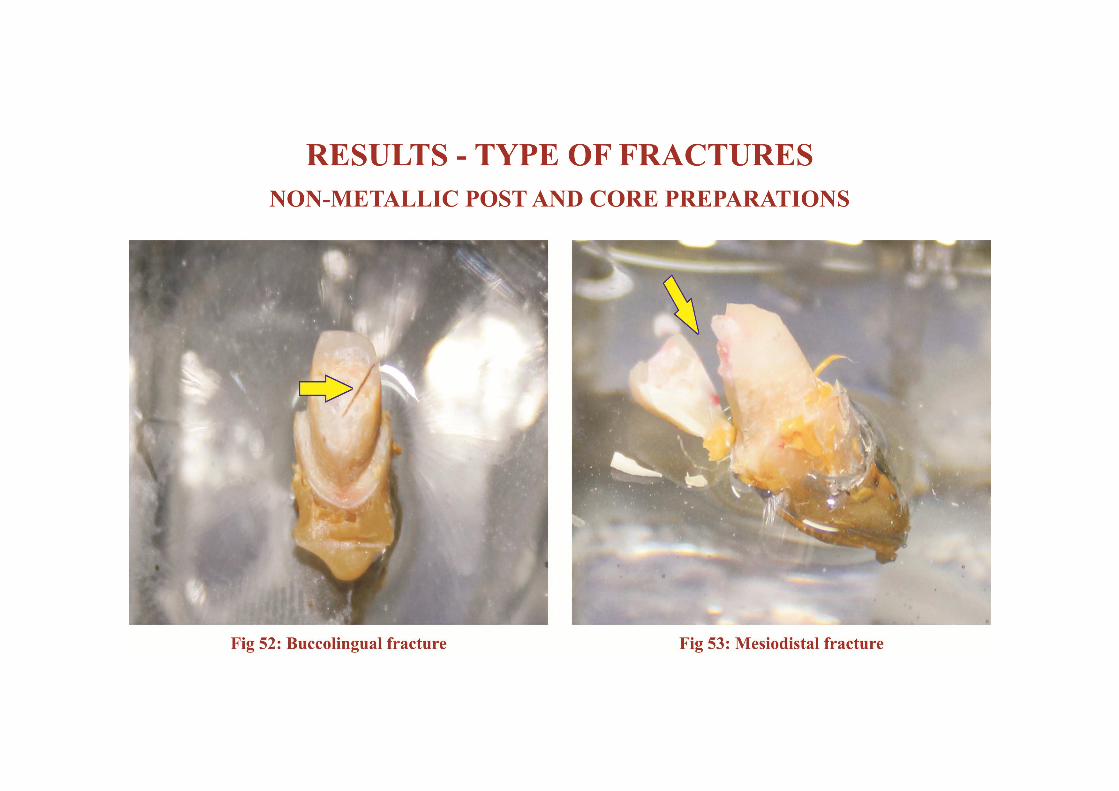
18. Tabulation of result:
The result of the fracture testing was tabulated after recording the maximum
load at which fracture occurred. The fracture strength results and the type of fracture
were analysed. The type of fractures which have taken place in each sample were
observed under magnification, grouped and recorded. The results were assessed by
two different operators and the results compared and tabulated.
19. Statistical analysis:
The samples were distributed across the groups based on their weights and
homogeneity. They were subjected to a statistical test to assess the normality of
these continuous variables. The results of the fracture test were statistically analysed
using one way ANOVA test of variance with Tukey post hoc test for multiple
comparisons.

Table 1: GROUPING – POST AND CORE
GROUPS (n= 8) POST AND CORE TYPE
I ORDEN ALLOY
II GOLD ALLOY
III NICKEL CHROMIUM ALLOY
IV TITANIUM
V GLASS FIBER POST
VI CARBON FIBER POST

RESULTS

TABLE 2: TYPES OF FRACTURE -INCIDENCE
TOTAL
SAMPLES
PERCENTAGE OF INCIDENCE
Buccolingual Mesiodistal Communited Transverse Others
(n=48) 12.5% 60.5% 18.7% 4.15% 4.15%
CHART I: FRACTURE TYPES - INCIDENCE
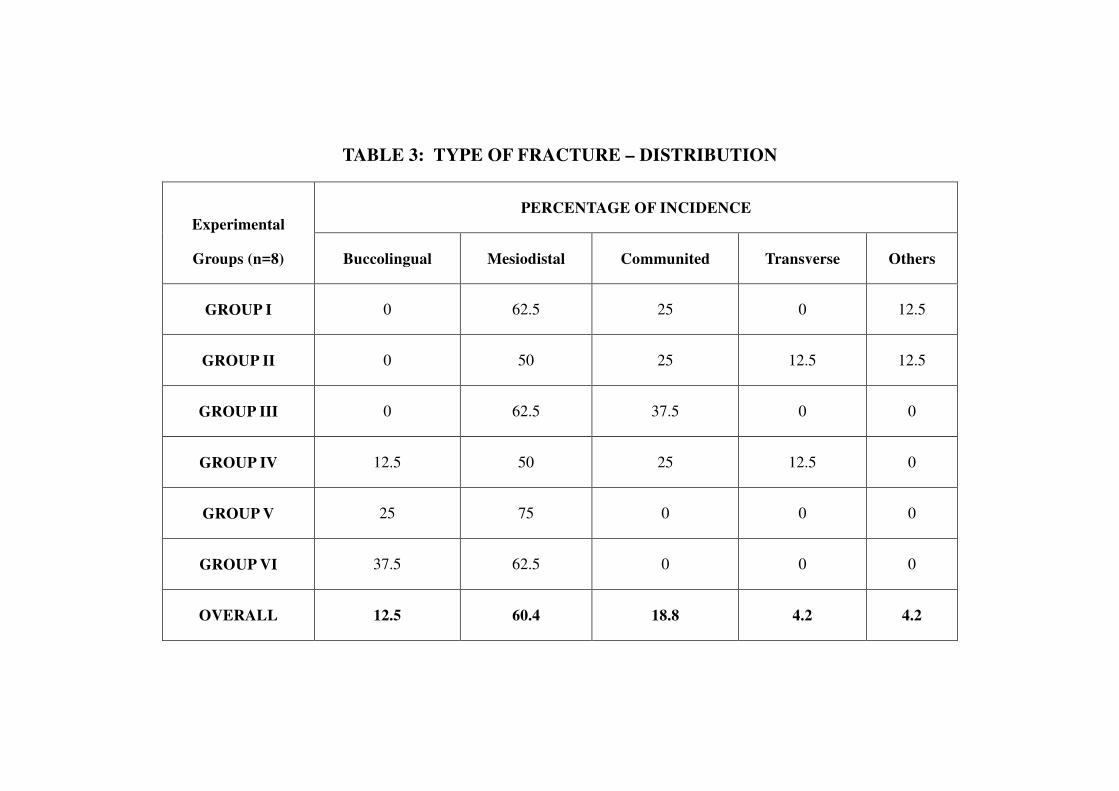
TABLE 3: TYPE OF FRACTURE – DISTRIBUTION
Experimental
Groups (n=8)
PERCENTAGE OF INCIDENCE
Buccolingual Mesiodistal Communited Transverse Others
GROUP I 0 62.5 25 0 12.5
GROUP II 0 50 25 12.5 12.5
GROUP III 0 62.5 37.5 0 0
GROUP IV 12.5 50 25 12.5 0
GROUP V 25 75 0 0 0
GROUP VI 37.5 62.5 0 0 0
OVERALL 12.5 60.4 18.8 4.2 4.2

CHART II: FRACTURE TYPES - DISTRIBUTION

TABLE 4: FRACTURE LOAD ANALYSIS
EXPERIMENTAL
GROUPS (n=8)
MAXIMUM
VALUE
MINIMUM
VALUE MEAN
CONFIDENCE INTERVAL
AT 95% STANDARD
DEVIATION MEDIAN
LOWER
BOUND
UPPER
BOUND
I 579.53 285.71 427.92 340.8238 510.4283 101.70 410.91
II 650.71 216.54 361.11 247.8979 474.3266 135.42 357.50
III 928.84 444.74 742.88 591.8977 893.8758 180.60 790.42
IV 672.36 284.32 482.32 349.5759 615.0758 158.78 484.46
V 472.62 203.12 336.96 255.6189 418.3055 97.29 322.05
VI 690.27 182.54 323.67 181.9662 465.3924 169.50 287.12

CHART III – EXPERIMENTAL GROUPS - FRACTURE MEAN
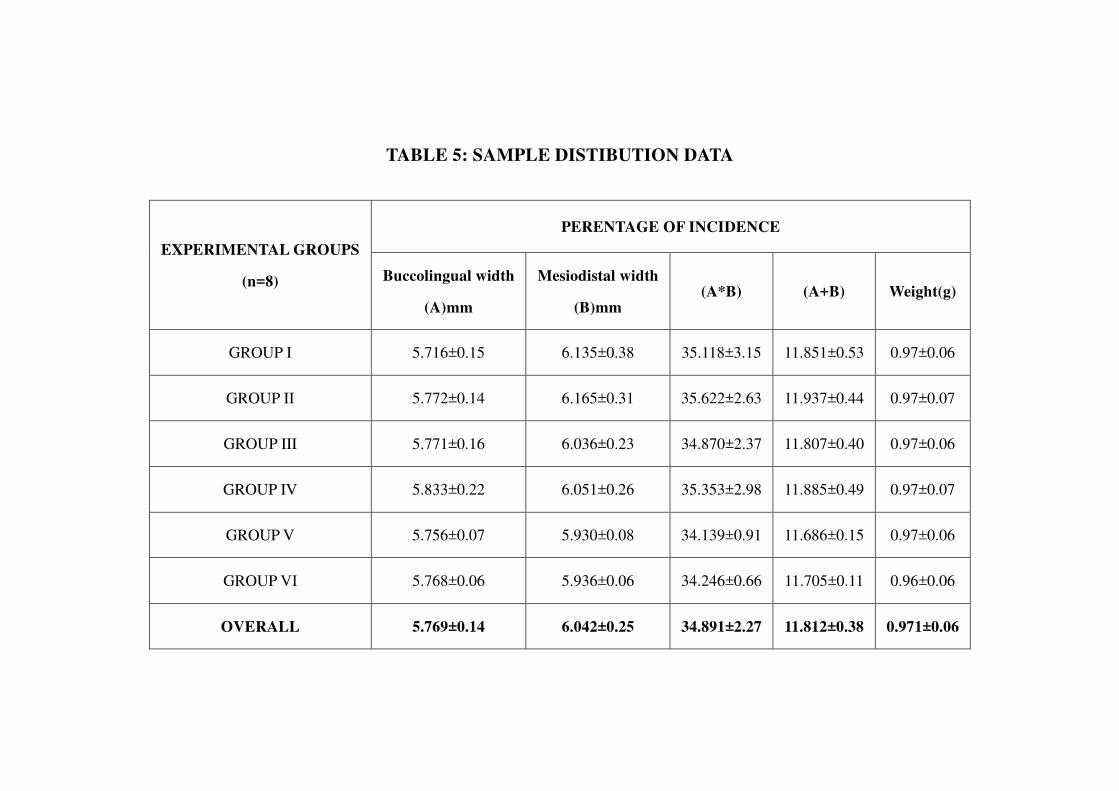
TABLE 5: SAMPLE DISTIBUTION DATA
EXPERIMENTAL GROUPS
(n=8)
PERENTAGE OF INCIDENCE
Buccolingual width
(A)mm
Mesiodistal width
(B)mm (A*B) (A+B) Weight(g)
GROUP I 5.716±0.15 6.135±0.38 35.118±3.15 11.851±0.53 0.97±0.06
GROUP II 5.772±0.14 6.165±0.31 35.622±2.63 11.937±0.44 0.97±0.07
GROUP III 5.771±0.16 6.036±0.23 34.870±2.37 11.807±0.40 0.97±0.06
GROUP IV 5.833±0.22 6.051±0.26 35.353±2.98 11.885±0.49 0.97±0.07
GROUP V 5.756±0.07 5.930±0.08 34.139±0.91 11.686±0.15 0.97±0.06
GROUP VI 5.768±0.06 5.936±0.06 34.246±0.66 11.705±0.11 0.96±0.06
OVERALL 5.769±0.14 6.042±0.25 34.891±2.27 11.812±0.38 0.971±0.06

38
TABLE 6: NORMALITY ANALYSIS FOR SAMPLES
SL. NO. GROUPS COMPARED SIGNIFICANCE
1 Buccolingual Width (B) NORMAL
2 Mesiodistal Width (B) NORMAL
3 A*B NORMAL
4 A+B NORMAL
5 Weight(G) NORMAL
Since the p-values of all the groups are more than 0.05, it can be concluded that the distribution is normal at 5% level of significance.
ANALYSIS AND INTERPRETATION:
Normality Testing is used to test whether the distribution is normal at 5% level of significance.
Note 1: If “p” value is more than 0.05, then we can conclude that the distribution is normal.
Note 2: If “p” value is less than 0.05, then we can conclude that the distribution is non-normal.

39
TABLE 7: STATISTICAL ANALYSIS – VALUE CORRELATION
SL.NO. GROUPS COMPARED CORRELATION
1 Buccolingual Width (A) and Weight positive correlation
2 Mesiodistal Width (B) and Weight positive correlation
3 A*B and Weight positive correlation
4 A+B and Weight positive correlation
5 Groups Combined positive correlation
ANALYSIS AND INTERPRETATION:
Correlation is a statistical tool that is used to determine the degree of relationship between two or more variables.
• When r = +ve, there is positive correlation between the variables.
• When r = –ve, there is negative correlation between the variables.
• When r = 0, there is no relationship between the variables.
The co-efficient of correlation “r” will lie between –1 and +1, (i.e.) –1 ≤ r ≤ +1.
Note 1: If “p” value is more than 0.05, then we can conclude that the correlation is not statistically significant.
Note 2: If “p” value is less than 0.05, then we can conclude that the correlation is statistically significant.

40
TABLE 8: METALLIC AND NON-METALLIC POST AND CORE GROUP COMPARISON
Student’s t- test
Group N Mean Std.
Deviation
I-IV 32 503.56 202.84407
V-VI 16 330.32 133.69303
SL.NO. GROUPS COMPARED t-value p-value SIGNIFICANCE
1
[Groups I-IV]
&
[Groups V-VI]
t = 3.089 p= 0.003 Significant
Combination of groups I-IV is comparatively better/higher than the combination of groups V-VI.
ANALYSIS AND INTERPRETATION:
Student’s “t” test for two independent groups is used to compare the significance of difference between means of two groups at 5% level of
significance.
Note 1: If “p” value is more than 0.05, then we can conclude that there is no significant difference between the two groups considered with
regard to mean.
Note 2: If “p” value is less than 0.05, then we can conclude that there is a significant difference between the two groups considered with
regard to mean.

41
TABLE 9: STATISTICAL COMPARISON BETWEEN GROUPS -
FRACTURE RESISTANCE
TWO GROUP COMPARISON Student’s t- test
SL.NO. GROUPS COMPARED t-value p-value SIGNIFICANCE
1 GROUP I ,II 1.116 0.283 non significant
2 GROUP I,III 4.298 0.001 significant
3 GROUP I,IV 0.816 0.428 non significant
4 GROUP I,V 1.828 0.089 non significant
5 GROUP I,VI 1.492 0.158 non significant
6 GROUP II,III 4.784 0.000 significant
7 GROUP II,IV 1.643 0.123 non significant
8 GROUP II,V 0.410 0.688 non significant
9 GROUP II,VI 0.488 0.633 non significant
10 GROUP III,IV 3.065 0.008 significant
11 GROUP III,V 5.597 0.000 significant
12 GROUP III,VI 4.787 0.000 significant
13 GROUP IV,V 2.208 0.044 significant
14 GROUP IV,VI 1.932 0.074 significant
15 GROUP V,VI 0.192 0.850 non significant
ANALYSIS AND INTERPRETATION:
Student’s “t” test for two independent groups is used to compare the significance of
difference between means of two groups at 5% level of significance.
Note 1: If “p” value is more than 0.05, then we can conclude that there is no
significant difference between the two groups considered with regard to mean.
Note 2: If “p” value is less than 0.05, then we can conclude that there is a significant
difference between the two groups considered with regard to mean.
42
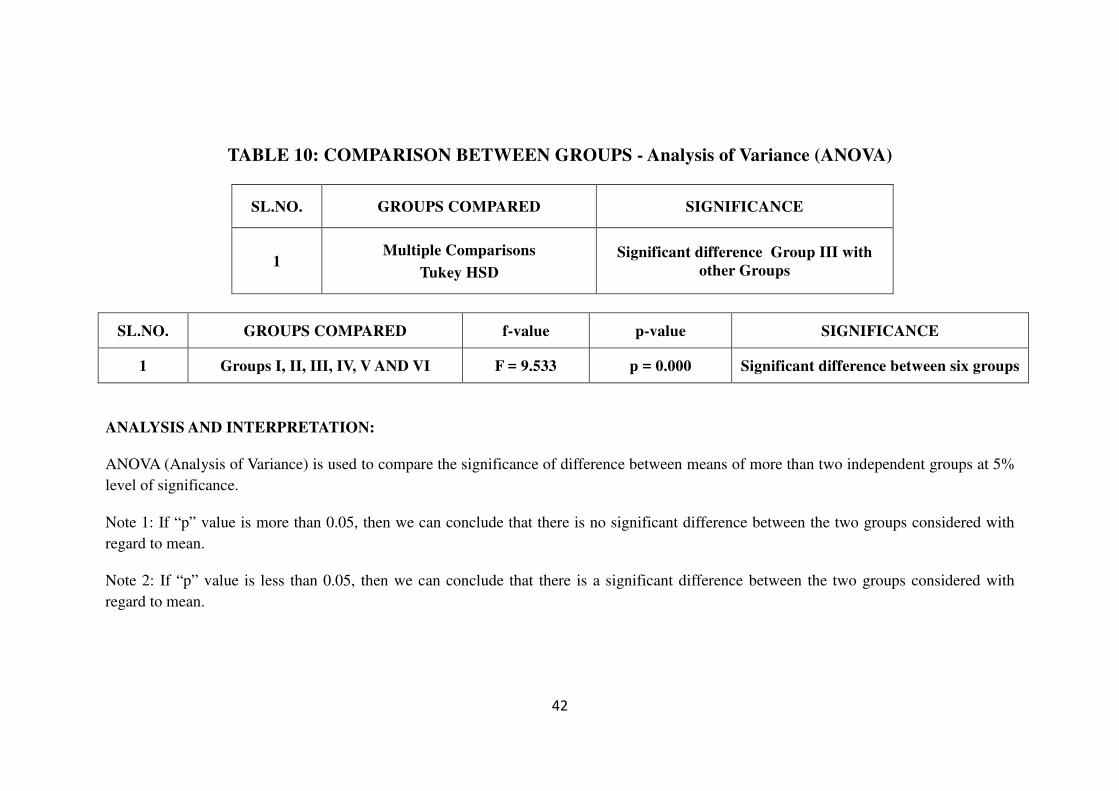
TABLE 10: COMPARISON BETWEEN GROUPS - Analysis of Variance (ANOVA)
SL.NO. GROUPS COMPARED SIGNIFICANCE
1 Multiple Comparisons
Tukey HSD
Significant difference Group III with
other Groups
SL.NO. GROUPS COMPARED f-value p-value SIGNIFICANCE
1 Groups I, II, III, IV, V AND VI F = 9.533 p = 0.000 Significant difference between six groups
ANALYSIS AND INTERPRETATION:
ANOVA (Analysis of Variance) is used to compare the significance of difference between means of more than two independent groups at 5%
level of significance.
Note 1: If “p” value is more than 0.05, then we can conclude that there is no significant difference between the two groups considered with
regard to mean.
Note 2: If “p” value is less than 0.05, then we can conclude that there is a significant difference between the two groups considered with
regard to mean.

CHART IV: FRACTURE RESISTANCE ANALYSIS – EXPERIMENTAL GROUPS
METALLIC POST AND CORE
GROUP I GROUP II
GROUP III GROUP IV

CHART V: FRACTURE RESISTANCE ANALYSIS – EXPERIMENTAL GROUPS
NON METALLIC POST AND CORE
GROUP V GROUP VI

DISCUSSION

Discussion
43
The objective and aim of the root canal treatment procedure is to achieve a
three dimensional hermetic seal during canal obturation and adequately reinforce the
root canal space so as to increase resistance to fracture of the remaining tooth
structure. Endodontically treated teeth have been reported to be more susceptible to
fracture when compared to vital teeth. This necessitates adequate protection of
remaining tooth structure by proper restoration protocols.
During endodontic therapy the entire root canal system has to be adequately
accessed, cleansed of all the necrotic tissues, remnants, debris, microbes and
subsequently appropriately restored. This process of cleansing of the root canal
space is called the biomechanical preparation. The root canal system presents a
complex structure and is colonized by the microorganisms during an infection which
have been demonstrated in the dentinal tubules half way through radicular dentin.
Therefore while treating the infected root canal space the process of shaping and
cleansing i.e., the biomechanical preparation of the canal is viewed as a vital step
during endodontic therapy. The inherent variations of anatomy of the canal system,
the curvature of the roots especially in the mandibular and maxillary posterior teeth
pose a challenge during biomechanical preparation. The occlusal one third of the
canal system is highly accessible, middle one is third fairly accessible and the apical
one third is the least accessible. In the case of curved roots in order to access the
apical third of the canals and to achieve sufficient cleansing and debridement,
considerable amount of radicular dentin in the coronal and middle third is removed
intentionally which would possibly can affect the structural integrity of the of the
tooth. This makes the endodontically treated tooth more prone to fracture. (Sornkul
et al in 199291)
Discussion
44
Excessive tooth structure removal during endodontic therapy and subsequent
dehydration of both coronal and radicular dentin are principal factors which have
been responsible for affecting the fracture resistance of restored tooth structure after
completion of endodontic treatment procedure. Dentin in a endodontically treated
tooth should be preserved as much as possible. The resistance to fracture depends
primarily on remaining root dentin thickness, especially in the buccolingual
direction. (Sedgley and Messer in 1992)80
A number of reasons have been put forward for the tooth being susceptible
for fracture which includes loss of tooth structure due to caries or trauma, excessive
removal of tooth structure during root canal preparation, the dehydration of dentin
subsequent to endodontic treatment, excessive radicular dentinal structural loss
during post space preparation, creation of excessive stress during obturation and
increased use of higher concentration of irrigants with prolonged exposure times.
This in a clinical situation would mean a reduction in the long term survival rate,
which is highly undesirable. The major achievable goal of endodontic therapy
should be reinforcement of the residual tooth structure in such a way that it prevents
untoward events in the long term. (Johnson M.E., et al in 2000)38
.
Earlier with hand instrumentation it was common practice to enlarge the
canal to three sizes from the first initial file to bind at the apical third of the root.
This enlargement allowed efficient cleansing and allowed the irrigants and
medicaments to reach the entire length of the canal system. The introduction of
nickel titanium hand instruments in endodontics almost two decades ago, improved
preparations as they were flexible. The most significant advantage was the more
predictable control of the preparation. The alloy was resistant to corrosion, had the
Discussion
45
property of super elasticity and shape memory. With the advent of nickel titanium
rotary instrumentation, things changed and negotiation of even severely curved
canals became much easier to accomplish, was more complete and reduced the
clinical working time. These rotary instruments when used to prepare the canal exert
considerable stresses in certain areas resulting in formation of microcracks or craze
lines which later predisposes the tooth to vertical root fracture. These areas of most
stress are mostly located in the mid root canal wall area. It has been observed that
lateral forces result in high stress concentrations in radicular dentin in the coronal
one third of the root, and make the teeth susceptible to fracture at the cemento
enamel junction. There is a direct proportional correlation between thickness of the
root and the ability of the tooth to resist lateral dislodging forces. The amount of
remaining radicular and coronal dentin in a tooth is directly proportional to the
fracture resistance. (Lertchirakarn V., et al in 2002)44
Studies have pointed out a potential relationship between the design of the
nickel titanium rotary instruments and the incidence of vertical root fractures. (Kim
H.C et al in 201042). Traditionally the rotary nickel titanium file systems were
designed to be used in a sequence and consisted of multiple rotary tools. Advances
in metallurgy have seen introduction of newer file systems for canal preparation
with a single rotary file which are effective. Also rotary files for use in reciprocating
motion have been designed. A new rotary file adjusting to the size of the canal and
which works with vibration and continuous irrigation, the self adjusting file system
has been developed successfully. These single file systems have been formulated
due to the advances in metallurgy and have practicality, simplicity, reduce clinical
working time and have been reported to reduce the amount of induced stresses on
Discussion
46
the canal walls. The self adjusting file is hollow, flexbile and compressible and the
system works with a up and down grinding motion with the help of which it
removed dentin from the canal walls. The file literally adapts to the anatomical
pathway of the canal wall which reduces over preparation and subsequent
weakening. The self adjusting file is made of medical grade nickel titanium alloy to
form a metal lattice hollow cylinder design and sand blasted to enable it to remove
radicular dentin. The straightening of the curved canals is reduced because of the
absence of a rigid core and the pliability of the file. (Metzger Z, et al in 201035)
The file as it is inserted into the canal removes a surface layer of dentin which
results in a canal of larger dimensions but a similar cross-section. (Hof R, et al in
201035)
Next concept was the innovative migration from a continuous rotary motion
to a reciprocating motion involving different clockwise and counterclockwise
angles. The reciprocating motion has been used to rotate stainless steel files since
1958. These systems used a 90 degress clockwise and counterclockwise motion
which later evolved to 30 degrees. The reciprocation file systems that have been
introduced of late which use the superior reciprocating motion based on the Roane
technique of canal preparation which is a balanced force concept put forward by
Roane J B, et al in 198567
. The use of the reciprocating movement reduces the
various risks of continuously rotating the file through the curvature of the canal
system. The equal angle reciprocating motors reduce the cutting efficiency, increase
the required pressure, require multiple files and are poor at debridement. The use of
unequal angles of reciprocation has distinct advantages of efficient debridement and
easy advancement of the file to the established working length. The incorporation of
Discussion
47
these newer techniques have made the single file reciprocating systems more safer
and achieve the target preparation faster. The reciprocating motion shifted from the
use of equal to unequal counterclockwise angles. The use of a reciprocating motion
results in a minimal torsional and flexural stresses. This translates into a less binding
effect of the instruments on the radicular dentin. This also creates a less invasive
preparation of the canal space due to the increased canal centering.
The waveone gold reciprocating single file system (Dentsply Mallieifer
Ballaigues, Switzerland) is made with a M-wire NiTi alloy and is used with a
dedicated reciprocating motor system with a 170 degree counter clockwise motion
followed by a 50 degree clockwise motion with a rotational speed of 350rpm. This
can be used in any canal irrespective of its length, diameter or curvature. These
edges minimise the screwing effect, thereby reducing torque which along with the
enhanced cutting efficiency, allows for smoother operation.
This reciprocating single file system Reciproc (VDW Munich Germany) is
made with M-wire NiTi alloy and uses a 150 degree counter clockwise rotation
followed by a 30 degree clockwise motion with a speed of 300 rpm. It has a
continuous taper over the first 3mm of the file and followed by a decreased taper
until the shaft with an S-shaped cross section. These angles are designed in such a
way that prevents the rotation of the instrument past the angle of fracture and has
good canal centering ability. The S- shaped cross section reduces friction while
cutting and deeper flutes offers a huge capacity for debris removal from the canal
system. Both the Reciproc and Waveone reciprocation systems have been found to
be similar in their cleaning efficiency (Carvalho M S, et al in 201515) The Reciproc

Discussion
48
system single file has been found to be more efficient at cutting when compared to
the waveone system.
The single file reciprocating systems Reciproc and Waveone have been
found to be superior and suitable for canal preparation when compared to other
single file rotary systems. The reciprocating motion was found to be superior to the
rotary motion of canal preparation in terms of canal transportation, cervical dentinal
thickness and cross sectional area (Dhingra A, et al in 201523) The reciprocating
single file systems have been found to be superior in shaping severely curved canals
when compared with rotary multi file systems. They also have been found to have a
lesser preparation time and procedural errors. (Bane K, et al in 20155)
Different presentations of fractures in roots of endodontically treated teeth
have been reported. They can be classified broadly as transverse and vertical root
fractures. Vertical root fracture is one of the most serious complications of root canal
procedures with an unfavorable prognosis that can occur before, during, or after root
canal obturation and most often leads to the removal of the affected tooth. (Meister
F et al in 198049) Numerous clinical studies have shown that 11%- 13% of extracted
teeth with endodontic treatment are associated with vertical root fractures. (Fuss Z.,
et al in 199928) Various predisposing factors like age, tooth type, degree of
calcification, excessive forces applied during obturation, the wedging effect of
spreaders used during the filling procedure, excessive pressure during post
cementation, excessive post space preparation and excessive dentin removal by
instrumentation have been proposed as contributing to vertical root fractures.
Endodontic procedures during the biomechanical preparation induce craze
lines and cracks on the canal walls which become areas of high stress concentration.

Discussion
49
These cracks may spread slowly over a period of time to the surface eventually
resulting in a vertical root fracture. (Yoldas O., et al in 2012107) The cracks usually
begin at the apex of the root and propagate cervically. Judicious use of
instrumentation procedures either hand or rotary and selection of a optimal irrigation
system for customized for the tooth will minimize the incidence of such craze lines
and cracks and avoid incidence of fractures later. The change in the mechanical
properties of dentin with age and the loss of hydration after endodontic therapy has
also been a reason for the reduced tolerance of teeth to fractures. This has lead to
various researchers looking to reinforce the structure of the crown and the root after
the completion of the biomechanical preparation.
Optical coherence tomography has been suggested as a potential tool for
identification and localizing the vertical root fractures. This was introduced in 1991
and allows micrometer scale imaging of the tissues using infrared light waves which
reflect off the internal microstructure of the tissues. It has a resolution of ten
micrometers and has been suggested as a valuable tool to identify perforations, intra
canal anatomy and canal cleanliness. The sensitivity of this tool is better than that of
computerized tomography in identification of vertical root fractures (Shemesh H.,
et al in 200886)
The prognosis for teeth with transverse or horizontal root fractures is usually
good. It is very important to differentiate between the kind of fracture which has
happened, either vertical or horizontal fractures. There is a poor prognosis in
conditions with vertical type of fractures which split roots along their long axis .
Horizontal root fractures are the most common type and occur mainly in the anterior
region of the maxilla, owing to a frontal impact. They are common in the middle-

Discussion
50
third and rarely occur in the apical and coronal third of the root. Successful
management of a tooth that has sustained a transverse root fracture depends on the
fracture line position, the mobility of the coronal segment, and the status of the
radicular and coronal pulp.
The position and relationship of the fracture line to the gingival crevice are
the most important factors affecting the long term prognosis. Coronal third and
middle third type of root fractures has shown to have a unfavorable prognosis than
apical third type of root fractures. As long as the fracture is infrabony with no
communication to the gingival sulcus and the patient practices meticulous oral
hygiene, appropriate treatment options can result in successful outcome of therapy.
Fractures in the apical third of the root can be viewed in occlusal radiographs,
whereas periapical radiographic views are better for visualizing coronally located
root fractures. Verified pulp necrosis has been reported with a percentage of
incidence of 43.7% in horizontal root fractures. Treatment of transverse or
horizontal root fractures depends on the position of the tooth after it has been
fractured, the mobility of the coronal segment, the status of the pulp, and the
position of the fracture line. Repair and healing of the injury to the coronal and
apical segments occurs either by hard tissue union, which is the most desirable, bony
ingrowth across the fracture, fibrous healing, or ingrowth of granulation tissue.
Fractures as a result of fatigue have been reported in teeth which are vitan and have
been subjected to repetitive occlusal forces.
The biologic dentin post system demonstrated the highest fracture resistance
when a unidirectional force was applied and was repairable in an in vitro setting.
The masticatory forces are multi-directional in a clinical situation. Development of

Discussion
51
tooth banks have been suggested for ready availability of these dentin biologic posts.
(Kurthukoti A J., et al in 201543
)
The process of retreatment has been shown to increase further amounts of
dentin from within the canal space rendering these retreated teeth more susceptible
to fracture. The rotary files used for gutta percha removal during the retreatment
procedure have been shown to remove the surface dentin, as well as further
enlargement of the apical thirds to achieve better cleansing which contributes to a
reduced fracture resistance of the root. There has been a positive corelation between
the removal of dentin during retreatment procedures and reduction of fracture
resistance. (Ganesh A, et al in 201429)
This has lead to various researchers looking to reinforce the structure of both
the crown and the root after the completion of endodontic treatment. The commonly
used root canal filling material is gutta percha in combination with a sealer. The low
elastic modulus of gutta percha presents little or no capacity to reinforce roots after
completion of endodontic therapy. (Ribero F.C., et al in 2008)64 Thus, there is a
compelling need to develop materials and techniques to overcome the shortcomings
of current endodontic obturation materials and post endodontic restorations to
reinforce root structure post therapy.
Swartz D B., et al in 198395 stated that failure rate of endodontically treated
teeth was almost double in cases without the process of adequate post endodontic
restoration. Newer generation of materials tend to improve the bond between
radicular dentin and the sealer and the sealer-core interface which helps to increase
the fracture resistance and reduces ingress pathways. To reinforce the roots the
modulus of elasticity of the root filling material should approximate that of the
Discussion
52
dentin. (Williams C., et al in 2006105). This presents the concept of a monoblock,
which aims at creating mechanically sound homologous units with radicular dentin.
They can be classified into primary, secondary and tertiary monoblocks based on the
number of interfaces present between the bonding material and the core material. A
primary monoblock has only one interface between the material and the canal wall.
A secondary monoblock has two circumferential interfaces between the core
material and the canal walls. When a third substrate is introduced between the
bonding substrate and the abutment material it forms a tertiary monoblock. This is
easier said than done as the complexity of the canal system, difficulties in access and
cleansing present difficulties in predictably achieving the target monoblock unit.
Priming the radicular dentinal surface and creating a bond between the sealer and
dentin, sealer and core material would effectively achieve this. A number of sealer
and core materials have been formulated with the aim of achieving this. The
modulus of elasticity of the post, the filling material and the sealer has to match that
of radicular dentin so that the load stresses are evenly distributed and borne by the
components of the monoblock. (Tay F.R., et al in 200796).
Intra orifice barrier is an efficient alternative method to decrease coronal
leakage after endodontic treatment. (Yavari H R., et al in 2012)106. This procedure
involves placing additional material into the canal orifices immediately after
removal of the coronal portion of gutta-percha and sealer. This also improves the
fracture resistance of the root structure. (Roghanizad N., et al in 1996)109.
Materials like resin modified glass ionomers, flowable composites, and bonded
amalgam can ideally be used as intra-orifice barriers.

Discussion
53
A new breed of restorative materials for use as endodontic filling materials
have been introduced in conjunction with adhesive sealers and modified core
materials with a aim of increasing the fracture resistance of the endodontically
treated teeth by formation of effective bonds at the interfaces, hydrophilic and
which effectively bond to dentin. Glass fiber posts and carbon fiber posts with
different properties have been formulated. Glass fiber posts have been used to
restore endodontically treated teeth, mainly because they are aesthetic, faster to
execute and have an elastic modulus near that of tooth structure (30-50 GPa). (Scotti
R et al in 2003)45 In the present study we have use a glass fiber post and a carbon
fiber post system for evaluation.
The cast post and core method of post endodontic reconstruction has been
traditionally used and can be considered as gold standard. This technique has its own
limitations. There is a greater removal of radicular dentinal structure, need for
multiple clinical leading to more turnover time and has a elastic modulus which is
high compared to tooth structure (200 Gpa) which can lead to fractures. (Sarkis-
Onofre R et al in 2014)85
For post preparations survival rates ranging from 71 to 100% for fiber posts
and 50 to 97.1% for metal posts have been reported. No difference in the survival
among different kinds of metallic posts were reported. No differences were reported
between fiber and metal posts by most studies conducted. Two studies also showed
that remaining dentine height, number of walls and ferrule increased the longevity of
the restored teeth. Post loss of retention was the reason for failure fiber posts.
Metallic post failures were mostly related to root fracture, post fracture or crown

Discussion
54
or post retention loss. Studies with longer follow up are needed. (Scotti R et al in
2003)45
Irrigant solutions have been traditionally used for removal of smear which
consists of organic and inorganic components consisting of blood, microbes,
necrotic pulp, saliva, and debris which is generated during the process of
biomechanical preparation. They have also been used for lubrication during
instrumentation, flushing out of debris from the canal, anti-bacterial property, and
removal of smear. This process of cleansing affects the intra radicular dentinal
structure which is composed of organic and inorganic components. Therefore the use
of these solutions has to be done in a way that it achieves its targeted role without
affecting the structure or the mechanical properties of the tooth. A ideal irrigant
solution should not affect the structural integrity of the tooth structure but should
contribute to it yet at the same time achieving the objective of a clean canal system.
Hence the parameters of volume, the concentration of the irrigant, time of exposure
and mode of delivery should be ideally be matched to the particular nature of the
irrigant and its properties. No single irrigant is effective against all the constituents
of the canal space. They have thus been used in combinations as multiple rinses to
achieve the target of a clean canal system which is a prerequisite for three
dimensional obturation of the root canal system. Irrigant solutions have been shown
to have an effect on the resistance to fracture of endodontically treated teeth. The
concentration and time of exposure of the irrigant play a role in the reduction of
fracture resistance of the tooth. A number of irrigant solutions been successfully
formulated for clinical use. Sodium hypochlorite in a concentration of 5% has been
used to remove the organic debris, and chelating agents like ethylene diamine
tetraacetic acid, citric acid, have been used to remove the inorganic components in
Discussion
55
varying concentrations. Endodontic irrigation thus leads to an alteration of the
chemical composition of intra radicular dentin due to the changes effected to the
organic and inorganic phases. This change alters the properties of microhardness,
permeability and solubility of the dentinal structure which leads to changes in the
ability of the teeth to resist fracture under varying loads.
Ethylene diamine tetraacetic acid widely used irrigant has been shown
previously to affect the fracture resistance of the tooth structure depending on the
exposure time and concentration. (Uzunoglu E, et al in 2012101) Citric acid a
chelating agent with good properties of stability, anti-microbial and smear removal
capacity is also being used widely as a root canal irrigant in different concentrations.
It has been suitably modified and is available for use as a final rinse solution
(MTAD and Tetraclean). The effects of citric acid on the fracture resistance of teeth
have been evaluated for different time exposures and concentrations and has been
found not to significantly change the fracture resistance of the tooth. (Arslan H.,
et al in 201412)
Sealers have evolved as a important interface in the root canal obturation
procedures. Their role in contributing to improving the fracture strength of the roots
has been evaluated by different researchers. (Bhat S S, et al in 201215) New
research methodologies have resulted in materials that facilitate more of adhesion to
the root canal walls which increases the mechanical interlocking and reduces the risk
of fracture. (Jhamb S, et al in 200937). The adhesion of the sealer to both interfaces
of the canal wall and that of the core material results in a more effective tertiary
monoblock which resists fracture when forces are applied.

Discussion
56
Selection of the obturation material and technique is very important as it
plays a role in reinforcing the root structure. As discussed previously the bio-
mechanical preparation of the root weakens the structure and using the right
obturation technique in strengthening the root. Various authors have evaluated
different obturation techniques and their effect on fracture resistance and observed
that a correctly done procedure of canal obturation improves the resistance of the
root to fracture. The use of gutta percha along with adhesive resin sealers have also
been reported to improve the fracture resistance of roots. (Sandickci T, et al in
201472) Technologies which incorporate a adhesive ionomer coating on the gutta-
percha for a thickness of two microns to which a adhesive ceramic sealer could be
bonded to form a tertiary monoblock have also been developed and evaluated. The
authors observe that all the materials used enhanced the fracture resistance of the
root. (Celikten B, et al in 201517)
Gutta percha with a resin based sealer has been used a gold standard for a
obturation procedure. There are several advantages of this system but the
hydrophobic nature and inability to sufficiently reinforce the root canal remain its
drawback. This has led to the development of hydrophilic materials which utilize the
moisture in the dentinal walls which allows the material to bond to the root canal
wall and core which reinforces the structure of the root by formation of a
monoblock. The increase in fracture resistance is also attributed to the penetration of
the dentinal tubules to varying depths and subsequent bonding due to incorporation
of nanoparticles in sealer also contributes to increased resistance to fracture. The
polymerization shrinkage of the resin based sealers that may be due to high C-factor
associated with the root canal also leads to contraction of the sealer post filling

Discussion
57
leading to a weakening of the bond between the sealer and the canal wall leading to
reduced resistance to fracture. A novel sealer C-point system has been introduced
which has got the property of sealer expansion due to its self expanding and
hydrophilic composition which significantly increased the resistance to fracture.
(Hegde V., et al in 201532)
The fracture which occurs in the root can be looked upon as a
communication which extends from root canal all the way to the external surface of
the root. There are also existence of external cracks or craze lines which extend from
the external surface into dentin which do not reach the root canal. The structural
defects in the structure of the root has been investigated and found to cause more
fractures, the reason being the amplification of induced stresses at these formed
microcracks. (Gudoutos E E, et al in 200530)
Microcracks are formed as a result of the rotational forces that are being
applied to the canal walls during the process of bio-mechanical preparation. The
procedures of endodontic therapy have contributed to the intiation and formation of
these microcracks. The formation of these microcracks may also be influenced by
the anatomy and the morphology of the root. The increased incidence of these
microcracks have been reported with the use of rotary instruments for canal
preparation. The amount of microcracks which are formed may be related to the
design features of rotary instruments like the tip size, geometry of cross-section, the
pitch which can be constant or variable, the taper which can be constant or
progressive and flute form (Yoldas O, et al in 2012107) The hand instruments
produce a lesser number of dentinal defects compared to rotary instruments. (Shori
D D.,et al in 201588)

Discussion
58
The introduction of reciprocating instruments and the self adjusting file
system for the canal preparation has drastically changes the way in which the canal
is prepared. The reciprocating file systems have been shown to produce significant
amount of incomplete dentinal cracks in the apical third of the canal system when
compared to a full sequence rotary files (Burklien S, et al in 201310) The creation of
a glide path has no significant effecting the formation of dentinal defects in
reciprocation instruments. (Saber S E, et al in 201571) The reciprocating
instruments for the canal preparation namely Reciproc and Waveone produced
defects in the roots which were not statistically significant. They caused more
defects in the apical parts of the canal compared to hand instruments which caused
more defects in the coronal and middle thirds. Both hand and reciprocating
instruments induced formation of dentinal defects during the canal preparation
(Helvacioglu-Yigit, et al in 201433)
There has been a positive correlation between the microcrack formation and
the incidence of root fractures. Investigations have revealed that the event of a root
fracture is not an instant event but a gradual propagation of craze lines and
microcracks in radicular root structure.
External craze lines and cracks are often found more commonly and were
found not to connect with the canal space. They were also in places which where in
places away from the direct contact of the rotary instruments. One possible reason is
that the stress generated during the instrumentation of the canals is transmitted to the
external surface of the teeth where it overcomes the bonds in dentin to form these
craze lines, micro cracks and eventually resulting in fractures. (Shemesh H, et al in
200986) The role of the obturation technique in formation of these defects has also

Discussion
59
been considered. The excessive forces generated during the process result in stresses
causing these defects in root dentin. Dentinal defects have been observed in root
filled with gutta percha and AH26 using lateral compaction and continuous wave
techniques. (Shemesh H, et al in 201087)
This study was to evaluate the fracture strength was done on extracted
maxillary central incisor teeth in an in vitro setting. Due to the large amount of
variations in the volume and weight of the roots among the samples selected,
sufficient protocols were followed for standardization of the controllable factors.
The anatomical variations inherent in the root structure with regard to size and
volume, the time of extraction, age of the patient, storage conditions, level of
hydration and degree of calcification would have an effect on the results of this
study. The normality testing of these variables was assessed statistically and the
distributions were found to be normal at 5% level of significance.(Table: 6,7)
For mechanical testing of the teeth structure standardization of the samples is
very important as fracture strength of the samples was being evaluated in each
experimental group prepared for a different post and core system. The mesiodistal
and buccolingual diameters at the cemento enamel junction level were recorded. To
eliminate the variations and standardize the samples the roots were distributed to the
various experimental groups equally based on their buccolingual and mesiodistal
diameters as well as their weights. (Table: 5) The teeth were mounted on the bases at
an angle of thirty three degrees to create the similar conditions as in the oral cavity.
For testing the fracture strength the forces were to the prepared samples using a
specially designed stainless steel tip with a diameter of three millimeters using in
universal testing machine with a cross head speed of 1millimeter /min. The point of

Discussion
60
seating of the stainless steel tip was also in the zone where the lower incisor would
normally occlude. The maximum load at fracture was recorded.
After the fracture testing procedure with a universal testing machine the
fractured samples and fragments were collected in separate pouches for each sample
and were further analysed for the types of root fracture encountered during the
testing procedure. They were assessed by two different operators and the results
compared, tabulated and analysed. (Table: 2 Chart: I) The result of the fracture
testing which was recorded on the universal testing machine was tabulated and
analysed statistically. (Table: 3,4 Chart: II) There was statistically significant
difference between the experimental groups in load values of root fracture.
(Table: 10)
Fracture strength testing is a method of evaluating the likelihood of the
treated root to fracture when a component of force is applied to the tooth in a
specific direction till fracture occurs. Though these values are generally indicative of
the ability of the root to resist fracture, in a clinical situation the type of forces
involved and that to which the root is subjected to is different. Also the fracture of
the tooth could be because of the creation of microcracks in radicular dentin which
serve as areas where increased concentration of stresses in the root occur. When
forces are applied to the root it leads to propagation of these cracks and eventually
results in a fracture. A statistical comparison of the metallic and non-metallic post
and core groups used in this study found a significant difference with the
combination of Groups I-IV comparatively better fracture resistance values than the
combination of Groups V-VI.

SUMMARY

Summary
61
Seventy two freshly extracted maxillary central incisors were collected
cleaned and stored in bottles containing 1% thymol in normal saline at 30 degree
Celsius. They were investigated for the presence of intact root morphology with a
patent canal free of any anomalies, gross destruction and restorations.
The weight of the tooth, the buccolingual and mesiodistal diameters were
calculated and samples evenly distributed based on their weights across the
experimental and control groups (n=8), rinsed with distilled water and stored in
normal saline at 4°C in separate glass bottles. The working lengths were calculated
the canals were prepared with hand files. The prepared samples were then obturated
and allowed to set for 48 hours, the access cavities restored. Subsequently post space
preparation was done. Based on the experimental group either wax patterns for
metallic post and core or protocols for luting a fibre post system followed by a core
preparation was followed. They were then mounted on to resin bases with the aid of
a base former. The cast post and core preparations were luted on to the teeth. They
were subjected to a fracture test under vertical loading applied with a 3mm stainless
steel tip in a universal testing machine and the load at fracture data recorded. After
the fracture testing process, type of fracture was analysed. The results tabulated and
statistically analysed.

CONCLUSION

Conclusion
62
On conclusion of the study, on the analysis of the fracture strength of roots
instrumented different post and core systems, the following conclusions are made:
Overall the Mesiodistal type of fracture was the most common among the
experimental groups with a percentage of incidence of 60.50%[Table 2 Chart I]
The communited type of fracture was the next commonest with a percentage of
incidence of 18.7% [Table 2 chart I].The incidence of buccolingual, transverse and
other type of fracture was not common and had a percentage of incidence of
12.50%, 4.15% and 4.15% respectively [Table 2 chart I].
Amongst the experimental groups in the metallic cast post and core groups
(Groups I-IV) all types of fractures were seen with the highest incidence being
mesiodistal with a incidence of 75%. The other type of fractures encountered were
communited, bucco-lingual, transverse and other group fractures with a incidence of
18.13 %, 3.13 %, 6.25% and 6.25% respectively. [Table 3]
On a statistical analysis of groups I –VI, Group III was found to have a
statistically siginificant difference with other groups. (p < 0.05)[Chart III Table10].
Within the limitations and standardization protocols used in this study, it can
be concluded that the resistance to fracture of the roots prepared with metallic cast
post and core [Groups I-V] was better than the non-metallic post and core
groups [V-VI]. There was a statistically significant difference between the metallic
and non-metallic groups in load values of root fracture (p < 0.05) [Chart III
Table 7]. Further evaluation of these different post and core systems and assessment
in a clinical setting is recommended.
BIBLIOGRAPHY

Bibliography
1. Alkhatri R, Saleh ARM, Kheder W. Evaluating Fracture Resistance And
Failure Modes Of Root Filled Teeth Restored With CAD/CAM-Fabricated Post
And Core. Clin Cosmet Investig Dent. 2019 Nov 14;11:349-355.
2. Artopoulou II, O'Keefe KL. Materials used in prefabricated post and core
systems. A review of the literature. Tex Dent J. 2006 Apr;123(4):358-63. Review.
3. Bacchi A, Caldas RA, Schmidt D, Detoni M, Matheus Albino Souza, Cecchin D,
Farina AP. Fracture Strength and Stress Distribution in Premolars Restored with
Cast Post-and-Cores or Glass-Fiber Posts Considering the Influence of Ferule.
Biomed Res Int. 2019 Jan 3;2019:2196519.
4. Bakirtzoglou E, Kamalakidis SN, Pissiotis AL, Michalakis K. In vitro
assessment of retention and resistance failure loads of complete coverage
restorations made for anterior maxillary teeth restored with two different cast
post and core designs. J Clin Exp Dent. 2019 Mar 1;11(3):e225-e230.
5. Bane K, Faye B, Sarr M, Niang S O, Ndiaye D, Machtou P Root canal shaping
by single file systems and rotary instruments: A laboratory study Iranian
Endodontic Journal 2015; 10(2): 135-139.
6. Bolla M, Muller-Bolla M, Borg C, Lupi-Pegurier L, Laplanche O, Leforestier E.
WITHDRAWN: Root canal posts for the restoration of root filled teeth.
Cochrane Database Syst Rev. 2016 Nov 28;11:CD004623. Review.
7. Brignardello-Petersen R. Preformed-metal posts seem to have a lower cost than
and similar effectiveness as cast-metal, glass-fiber, and carbon-fiber posts. J Am
Dent Assoc. 2017 Aug;148(8):e108.

Bibliography
8. Broch J, Marchionatti AM, Bergoli CD, Valandro LF, Kaizer OB. Fracture
resistance of weakened roots restored with different intracanal retainers. Gen
Dent. 2015 May-Jun;63(3):58-63.
9. Bromberg CR, Alves CB, Stona D, Spohr AM, Rodrigues-Junior SA, Melara R,
Burnett LH Jr. Fracture resistance of endodontically treated molars restored with
horizontal fiberglass posts or indirect techniques. J Am Dent Assoc. 2016
Dec;147(12):952-958.
10. Bürklein S, Tsotsis P, Schafer E. Incidence of dentinal defects after root canal
preparation: reciprocating versus rotary instrumentation. J Endod. 2013 Apr;
39(4):501-4.
11. Byakova SF, Novozhilova NE, Makeeva IM, Grachev VI, Kasatkina IV. The
detection of vertical root fractures in post-core restored teeth with cone-beam
CT: in vivo and ex vivo. Dentomaxillofac Radiol. 2019 Sep;48(6):20180327
12. Capar ID, Saygili G, Ergun H, Gok T, Arslan H, Ertas H. Effects of root canal
preparation, various filling techniques and retreatment after filling on vertical
root fracture and crack formation. Dent Traumatol. 2015 Aug; 31(4):302-7.
13. Capar ID, Arslan H, Akcay M, Uysal B. Effects of Protaper Universal, Protaper
Next, and HyFlex instruments on crack formation in dentin. J Endod. 2014. Sep;
40(9):1482-4.
14. Carvalho MA, Lazari PC, Gresnigt M, Del Bel Cury AA, Magne P. Current
options concerning the endodontically-treated teeth restoration with the adhesive
approach. Braz Oral Res. 2018 Oct 18;32(suppl 1):e74.

Bibliography
15. Carvalho MA, Lazari PC, Gresnigt M, Del Bel Cury AA, Magne P. Current
options concerning the endodontically-treated teeth restoration with the adhesive
approach. Braz Oral Res. 2018 Oct 18;32(suppl 1):e74. doi:10.1590/1807-
3107bor-2018.vol32.0074. Review.
16. Carvalho MA, Lazari PC, Gresnigt M, Del Bel Cury AA, Magne P. Current
options concerning the endodontically-treated teeth restoration with the adhesive
approach. Braz Oral Res. 2018 Oct 18;32(suppl 1):e74.5.
17. Celikten B, Uzuntas CF, Gulsahi K. Resistance to fracture of dental roots
obturated with different materials. Biomed Res Int. 2015 Feb:1-5
18. Chisnoiu A, Picos A, Lascu L, Negucioiu M, Chisnoiu R, Kui A. Dentists'
perspectives on the reconstruction possibilities of a non-vital tooth. Med Pharm
Rep. 2019 Oct;92(4):387-392.
19. Cloet E, Debels E, Naert I. Controlled Clinical Trial on the Outcome of Glass
Fiber Composite Cores Versus Wrought Posts and Cast Cores for the Restoration
of Endodontically Treated Teeth: A 5-Year Follow-up Study. Int J Prosthodont.
2017 Jan/Feb;30(1):71-79.
20. Comut A, Foran D, Cunningham RP. A technique to salvage endodontically
compromised maxillary anterior tooth. N Y State Dent J. 2014 Jan;80(1):33-7.
21. De Moraes AP, Poletto Neto V, Boscato N, Pereira-Cenci T. Randomized clinical
trial of the influence of impression technique on the fabrication of cast metal
posts. J Prosthet Dent. 2016 Jul;116(1):47-51.

Bibliography
22. Campanella V, Carosi P, Casella S, Pinto A, Di Girolamo M. Clinical fitting of a
cast metal post and core obtained by means of an intraoral optical scanning
(IOS) and digital workflow. J Biol Regul Homeost Agents. 2019 May-Jun;33(3
Suppl. 1):43-50.
23. Dhingra A, Ruhal N, Miglani A. Evaluation of Single File Systems Reciproc,
Oneshape, and WaveOne using Cone Beam Computed Tomography -An In Vitro
Study. J Clin Diagn Res. 2015 Apr; 9(4):ZC30-4.
24. Elavarasu P, Karumaran CS, Indira R, Anilkumar R, Mani R, Natarajan R. An In
Vitro Evaluation of Fracture Resistance of Endodontically Treated Maxillary
Central Incisor Restored with Custom-Made Cast Post and Core with Uniform
and Nonuniform Core Ferrule Heights. J Pharm Bioallied Sci. 2019
May;11(Suppl 2):S407-S412.
25. . Ertas H, Sagsen B, Arslan H, Ertas E.T. Effects of physical and morphological
properties of roots on fracture resistance. Eur J Dent 2014; 8(26):1-4.
26. Fokkinga WA, Kreulen CM, Vallittu PK, Creugers NH. A structured analysis of
In vitro failure loads and failure modes of fiber, metal, and ceramic post-and-
core systems. Int J Prosthodont. 2004 Jul-Aug;17(4):476-82.
27. Fontana PE, Bohrer TC, Wandscher VF, Valandro LF, Limberger IF, Kaizer OB.
Effect of Ferrule Thickness on Fracture Resistance of Teeth Restored With a
Glass Fiber Post or Cast Post. Oper Dent. 2019 Nov/Dec;44(6):E299-E308.
28. Fuss Z, Lustig J, Tamse A. Prevalence of vertical root fractures in extracted
endodontically treated teeth. Int Endod J. 1999; 32(4):283-86.
Bibliography
29. Ganesh A, Venkatesh Babu N, John A, Deenadhayalan G, Kandaswamy D A.
comparative assessment of fracture resistance of endodontically treated and
retreated teeth: An in-vitro study. Jour of Cons Dent 2014;17(1):61-65.
30. Gudoutos EE, Fracture Mechanics: An introduction 2nd edition, Dordrecht,
Netherland: Springer Publishers, 2005: 79-94.
31. Haralur SB, Al Ahmari MA, AlQarni SA, Althobati MK. The Effect of
Intraradicular Multiple Fiber and Cast Posts on the Fracture Resistance of
Endodontically Treated Teeth with Wide Root Canals. Biomed Res Int. 2018
Aug 15;2018:1671498.
32. Hegde V, Arora S. Fracture resistance of roots obturated with novel hydrophilic
obturation systems. J Conserv Dent. 2015 May-Jun;18(3):261-4.
33. Helvacioglu-Yigit D, Aydemir S, Yilmaz A. Evaluation of dentinal defect
formation after root canal preparation with two reciprocating systems and hand
instruments: An in-vitro study. Biotechnol Equip. 2015 Mar 4; 29(2):368-373.
34. Hendi AR, Moharrami M, Siadat H, Hajmiragha H, Alikhasi M. The effect of
conventional, half-digital, and full-digital fabrication techniques on the retention
and apical gap of post and core restorations. J Prosthet Dent. 2019
Feb;121(2):364.e1-364.e6.
35. Hof R, Perevalov V, Eltanani M, Zary R, Metzger Z. The self-adjusting file
(SAF) Part 2: Mechanical analysis. J Endod 2010;36(4):691-702.
36. Isidor F, Odman P, Brøndum K. Intermittent loading of teeth restored using
prefabricated carbon fiber posts. Int J Prosthodont. 1996 Mar-Apr;9(2):131-6.

Bibliography
37. Jhamb S, Nikhil V , Singh V. Effect of sealers on fracture resistance of
endodontically treated teeth with and without smear layer removal- An in vitro
study. J Conserv Dent 2009 july-sep;12( 3):114-17
38. Johnson M. E., Stewart G. P., Nielsen C. J., and Hatton J. F. Evaluation of root
reinforcement of endodontically treated teeth, Oral Surgery, Oral Medicine, Oral
Pathology, Oral Radiology, and Endodontics. 2000:90(3): 360-64.
39. Kar S, Tripathi A, Trivedi C. Effect of Different Ferrule Length on Fracture
Resistance of Endodontically Treated Teeth: An In vitro Study. J Clin Diagn Res.
2017 Apr;11(4):ZC49-ZC52.
40. Karteva EG, Manchorova NA, Vladimirov SB, Keskinova DA. Clinical
Assessment of Endodontically Treated Teeth, Restored with or without Radicular
Posts. Folia Med (Plovdiv). 2018 Jun 1;60(2):291-299.
41. Khiavi HA, Habibzadeh S, Safaeian S, Eftekhar M. Fracture Strength of
Endodontically treated Maxillary Central Incisors restored with Nickel
Chromium and Nonprecious Gold Alloy Casting Post and Cores. J Contemp
Dent Pract. 2018 May 1;19(5):560-567.
42. Kim HC, Lee MH, Yum J, Versluis A, Lee CJ, Kim BM. Potential relationship
between design of nickel-titanium rotary instruments and vertical root fracture. J
Endod. 2010 Jul; 36(7):1195-9.
Bibliography
43. Kurthukoti AJ, Paul J, Gandhi K, Rao DB. Fracture resistance of endodontically
treated permanent anterior teeth restored with three different esthetic post
systems: An in vitro study. J Indian Soc Pedod Prev Dent 2015 0ct-Dec; 33(4);
296-301.
44. Lertchirakarn V, Timyam A, Messer HH. Effects of root canal sealers on vertical
root fracture resistance of endodontically treated teeth. J Endod 2002;28:217-19.
45. Malferrari S, Monaco C, Scotti R. Clinical evaluation of teeth restored with
quartz fiber-reinforced epoxy resin posts. Int J Prosthodont. 2003 Jan-
Feb;16(1):39-44.
46. Mankar S, Kumar NS, Karunakaran JV, Kumar SS. Fracture resistance of teeth
restored with cast post and core: An in vitro study. J Pharm Bioallied Sci. 2012
Aug;4(Suppl 2):S197-202.
47. Marchionatti AME, Wandscher VF, Rippe MP, Kaizer OB, Valandro LF. Clinical
performance and failure modes of pulpless teeth restored with posts: a
systematic review. Braz Oral Res. 2017 Jul 3;31:e64.
48. Martino N, Truong C, Clark AE, O'Neill E, Hsu SM, Neal D, Esquivel-Upshaw
JF. Retrospective analysis of survival rates of post-and-cores in a dental school
setting. J Prosthet Dent. 2019 Jul 26. pii: S0022-3913(18)30702-9.
49. Meister F Jr., Lommel T. J., and Gerstein H. Diagnosis and possible causes of
vertical root fractures. Oral Surgery Oral Medicine and Oral Pathology 1980:
49(3): 243-253.
Bibliography
50. Metzger Z, Teperovich E, Zary R, Cohen R The self adjusting file(SAF) Part 1:
Respecting the root canal anatomy- A new concept of endodontic files and its
implementation J Endod 2010; 36(4): 679-690.
51. Mohajerfar M, Nadizadeh K, Hooshmand T, Beyabanaki E, Neshandar Asli H,
Sabour S. Coronal Microleakage of Teeth Restored with Cast Posts and Cores
Cemented with Four Different Luting Agents after Thermocycling. J
Prosthodont. 2019 Jan;28(1):e332-e336.
52. Munaga S, Das A, Kaur T, Yaqoob A, Mokashi R, Ismail PM. Comparative
Clinical Evaluation of Composite Overcast Gold Post and Core Buildups in
Endodontically Treated Teeth. J Contemp Dent Pract. 2018 Oct 1;19(10):1273-
1277.
53. Muttlib NA, Azman AN, Seng YT, Alawi R, Ariffin Z. Intracanal Adaptation of a
Fiber Reinforced Post System as Compared to a Cast Post-and-Core. Acta
Stomatol Croat. 2016 Dec;50(4):329-336.
54. Naumann M, Schmitter M, Frankenberger R, Krastl G. "Ferrule Comes First.
Post Is Second!" Fake News and Alternative Facts? A Systematic Review. J
Endod. 2018 Feb;44(2):212-219.
55. Naumann M, Schmitter M, Krastl G. Postendodontic Restoration: Endodontic
Post-and-Core or No Post At All? J Adhes Dent. 2018;20(1):19-24.
Bibliography
56. Nokar S, Bahrami M, Mostafavi AS. Comparative Evaluation of the Effect of
Different Post and Core Materials on Stress Distribution in Radicular Dentin by
Three-Dimensional Finite Element Analysis. J Dent (Tehran). 2018
Mar;15(2):69-78.
57. Nur BG, Ok E, Altunsoy M, Tanriver M, Capar ID. Fracture strength of roots
instrumented with three different single file systems in curved root canals. Eur J
Dent. 2015 Apr-Jun;9(2):189-93.
58. Öztürk C, Polat S, Tunçdemir M, Gönüldaş F, Şeker E. Evaluation of the fracture
resistance of root filled thin walled teeth restored with different post systems.
Biomed J. 2019 Feb;42(1):53-58.
59. Pereira JR, do Valle AL, Shiratori FK, Ghizoni JS, Bonfante EA. The effect of
post material on the characteristic strength of fatigued endodontically treated
teeth. J Prosthet Dent. 2014 Nov;112(5):1225-30.
60. Peters OA, Paque F. Current developments in root canal instrument technology
and clinical use: A review. Quintessence Int 2010 June; 41(6):479-88.
61. Ravi N, Mahima G, Shalini S .Comparison Of Fracture Resistance in roots of
endodontically treated teeth using different root filling materials: An in Vitro
Study. Indian Journal of Dental Sciences. September 2012; 3 (4): 7-8.
62. Rayyan MR, Aldossari RA, Alsadun SF, Hijazy FR. Accuracy of cast posts
fabricated by the direct and the indirect techniques. J Prosthet Dent. 2016
Sep;116(3):411-5.

Bibliography
63. Rezaei Dastjerdi M, Amirian Chaijan K, Tavanafar S. Fracture resistance of
upper central incisors restored with different posts and cores. Restor Dent
Endod. 2015 Aug;40(3):229-35.
64. Ribeiro F. C., Souza-Gabriel A. E., Marchesan M. A., Alfredo E., Silva-Sousa Y.
T. C, and Sousa-Neto M. D., “Influence of different endodontic filling materials
on root fracture susceptibility,” Journal of Dentistry 2008: 36(1): 69-73.
65. Rippe MP, Santini MF, Bier CA, Baldissara P, Valandro LF. Effect of root canal
preparation, type of endodontic post and mechanical cycling on root fracture
strength. J Appl Oral Sci. 2014 Jun;22(3):165-73.
66. Rippe MP, Santini MF, Bier CA, Borges AL, Valandro LF. Root canal filling:
fracture strength of fiber-reinforced composite-restored roots and finite element
analysis. Braz Dent J. 2013 Nov-Dec;24(6):619-25.
67. Roane JB, Sabala CL, Duncanson MG. The “balanced force” concept for
instrumentation of curved canals. J Endod. 1985; 11: 203-211.
68. Robbins JW. Restoration of the endodontically treated tooth. Dent Clin North
Am. 2002 Apr;46(2):367-84. Review.
69. Rodrigues JL, Seraidarian PI, Oliveira DD, Jansen WC, Alves KP, Faria-e-Silva
AL. Effect of increased post length due to the presence of the remaining coronal
structure on the fracture strength of post-retained restorations. Eur J Prosthodont
Restor Dent. 2014 Sep;22(3):132-5.
70. Roghanizad N, Jones JJ. Evaluation of coronal microleakage after endodontic
treatment. J Endod. 1996; 22(9):471-73.
Bibliography
71. Saber SE, Schäfer E. Incidence of dentinal defects after preparation of severely
curved root canals using the Reciproc single-file system with and without prior
creation of a glide path. Int Endod J. 2015 Oct 1.
72. Sandikci T, Kaptan R F. Comparative evaluation of the fracture resistances of
endodontically treated teeth filled using five different root canal filling systems.
Nigerian Journal of Clinical practice 2014;17(6):667-672.
73. Santos Pantaleón D, Morrow BR, Cagna DR, Pameijer CH, Garcia-Godoy F.
Influence of remaining coronal tooth structure on fracture resistance and failure
mode of restored endodontically treated maxillary incisors. J Prosthet Dent. 2018
Mar;119(3):390-396.
74. Santos-Filho PC, Veríssimo C, Soares PV, Saltarelo RC, Soares CJ, Marcondes
Martins LR. Influence of ferrule, post system, and length on biomechanical
behavior of endodontically treated anterior teeth. J Endod. 2014 Jan;40(1):119-
23.
75. Saritha MK, Paul U, Keswani K, Jhamb A, Mhatre SH, Sahoo PK. Comparative
Evaluation of Fracture Resistance of Different Post Systems. J Int Soc Prev
Community Dent. 2017 Nov-Dec;7(6):356-359.
76. Sary S B, Samah M S, Walid A AZ. Effect of restoration technique on resistance
to fracture of endodontically treated anterior teeth with flared root canals. J
Biomed Res. 2019 Apr 22;33(2):131-138.
Bibliography
77. Savychuk A, Manda M, Galanis C, Provatidis C, Koidis P. Stress generation in
mandibular anterior teeth restored with different types of post-and-core at
various levels of ferrule. J Prosthet Dent. 2018 Jun;119(6):965-974.
78. Schwendicke F, Stolpe M. Cost-effectiveness of Different Post-retained
Restorations. J Endod. 2017 May;43(5):709-714.
79. Schwindling FS, Tasaka A, Hilgenfeld T, Rammelsberg P, Zenthöfer A. Three-
dimensional-guided removal and preparation of dental root posts-concept and
feasibility. J Prosthodont Res. 2019 May 16. pii: S1883-1958(18)30403-1.
80. Sedgley CM, Messer HH. Are endodontically treated teeth more brittle? J
Endod. 1992 Jul;18(7):332-5.
81. Shamseddine L, Chaaban F. Impact of a Core Ferrule Design on Fracture
Resistance of Teeth Restored with Cast Post and Core. Adv Med.
2016;2016:5073459.
82. Shetty RR, Nayak M, Thomas J. Fracture Resistance of endodontically treated
roots filled with Resilon and Guttapercha - A comparative in Vitro Study. J of
ICDRO 2009; 1(3): 37-48.
83. Singh S, Thareja P. Fracture resistance of endodontically treated maxillary
central incisors with varying ferrule heights and configurations: In vitro study. J
Conserv Dent. 2014 Mar;17(2):115-8
84. Skupien JA, Cenci MS, Pereira-Cenci T. Although Cast Post and Cores Present
Acceptable Survival, Patient-related Factors May Influence Survival. J Evid
Based Dent Pract. 2016 Mar;16(1):62-3.
Bibliography
85. Skupien JA, Sarkis-Onofre R, Cenci MS, Moraes RR, Pereira-Cenci T. A
systematic review of factors associated with the retention of glass fiber posts.
Braz Oral Res. 2015;29.
86. Shemesh H, van Soest G, Wu MK, Wesselink PR. Diagnosis of vertical root
fractures with optical coherence tomography. J Endod. 2008 Jun; 34(6):739-42.
87. Shemesh H, Wesselink PR, Wu MK. Incidence of dentinal defects after root
canal filling procedures. Int Endod J. 2010 Nov; 43(11):995-1000.
88. Shori DD, Shenoi PR, Baig AR, Kubde R, Makade C, Pandey S.
Stereomicroscopic evaluation of dentinal defects induced by new rotary system:
"ProTaper NEXT". J Conserv Dent. 2015 May-Jun;18(3):210-3.
89. Solomon CS, Osman YI. In vitro comparison of endodontic posts in structurally
compromised roots of maxillary incisors. SADJ. 2011 Jun;66(5):220-3.
90. Sonkesriya S, Olekar ST, Saravanan V, Somasunderam P, Chauhan RS,
Chaurasia VR. An in vitro comparative evaluation of fracture resistance of
custom made, metal, glass fiber reinforced and carbon reinforced posts in
endodontically treated teeth. J Int Oral Health. 2015 May;7(5):53-5.
91. Sornkul E, Stannard JG. Strength of roots before and after endodontic treatment
and restoration. J Endod 1992; 18:440-3.
92. Sreedevi S, Sanjeev R, Raghavan R, Abraham A, Rajamani T, Govind GK. An In
Vitro Study on the Effects of Post-Core Design and Ferrule on the Fracture
Resistance of Endodontically Treated Maxillary Central Incisors. J Int Oral
Health. 2015 Aug;7(8):37-41.
Bibliography
93. Stankiewicz NR, Wilson PR. The ferrule effect: a literature review. Int Endod J.
2002 Jul;35(7):575-81. Review.
94. Stavridakis M, Brokos Y, Krejci I. Is the glass half empty or half full? A novel
"philosophical" approach to the "mystery" of the so-called ferrule effect. Med
Hypotheses. 2018 Jun;115:35-41.
95. Swartz DB, Skidmore AE, Griffin JA. Twenty years of Endodontic success and
Failures. Journal of Endodntics. 1983; 9(5):198-202.
96. Tay FR, Pashley DH. Monoblocks in root canals: A hypothetical or a tangible
goal. J Endod 2007; 33:391-8.
97. Tsintsadze N, Juloski J, Carrabba M, Tricarico M, Goracci C, Vichi A, Ferrari M,
Grandini S. Performance of CAD/CAM fabricated fiber posts in oval-shaped
root canals: An in vitro study. Am J Dent. 2017 Oct;30(5):248-254.
98. Tsintsadze N, Juloski J, Carrabba M, Tricarico M, Goracci C, Vichi A, Ferrari M,
Grandini S. Performance of CAD/CAM fabricated fiber posts in oval-shaped
root canals: An in vitro study. Am J Dent. 2017 Oct;30(5):248-254.
99. Türker SA, Özçelik B, Yilmaz Z. Evaluation of the Bond Strength and Fracture
Resistance of Different Post Systems. J Contemp Dent Pract. 2015 Oct
1;16(10):788-93.
100. Upadhyaya V, Bhargava A, Parkash H, Chittaranjan B, Kumar V. A finite
element study of teeth restored with post and core: Effect of design, material,
and ferrule. Dent Res J (Isfahan). 2016 May-Jun;13(3):233-8.
Bibliography
101. Uzunoglu.E, Aktemur S, Uyanik M O, Durmas V, Nagas E Effect of
ethylenediaminotetracetic acid on root fracture with respect to concentration at
different time exposures J Endod 2012; 38: 1110-1113.
102. Vadavadagi SV, Dhananjaya KM, Yadahalli RP, Lahari M, Shetty SR,
Bhavana BL. Comparison of Different Post Systems for Fracture Resistance:
An in vitro Study. J Contemp Dent Pract. 2017 Mar 1;18(3):205-208.
103. Vallabhaneni S, More GR, Gogineni R. Single file endodontics. Indian J Dent
2012; 4(2): 822-826.
104. Wang CH, Du JK, Li HY, Chang HC, Chen KK. Factorial analysis of variables
influencing mechanical characteristics of a post used to restore a root filled
premolar using the finite element stress analysis combined with the Taguchi
method. Int Endod J. 2016 Jul;49(7):690-9.
105. Williams C, Loushine RJ, Weller RN, Pashley DH, Tay FR. A comparison of
cohesive strength and stiffness of Resilon and gutta-percha. J Endod
2006;32:553-555.
106. Yavari HR, Samiei M, Shahi S, Aghazadeh M, Jafari M, Abdolrahimi M, et al.
Microleakage comparison of four dental materials as intra-orifice barriers in
endodontically treated teeth. Iran Endod J. 2012; 7(1):25-30.
107. Yoldas O, Yilmas S, Atakan G, Knudsen C, Kasan Z Dentinal microcrack
formation during root canal preparations by different rotary niti instruments
and the self-adjusting file J. Endod 2012;38:232-5.
Top Related