







Languages
Pages
Legal

FIRST EMERGENCY APPEAL
Ministry of HealthEthiopia
August 2002
EMERGENCY APPEAL FOR HEALTH AND NUTRITION, WATERAND SANITATION IN ETHIOPIA
I. INTRODUCTION AND BACKGROUND INFORMATION.
1.1 Geography and Climate
Ethiopia is located in the horn of Africa with a total surface area of 1.25 million
square kilometers. The characteristic topography of the country consists of
northern and central plateaus separated from the southern plateau by the
Ethiopian rift valley. More than half of the country lies at least 1,500 meters
above sea level. Its climate is strongly associated with the altitude and the land
relief of the country.
Ethiopia is a natural museum for varied flora and fauna, ethnic mosaics with
cultural diversity and short distant geographical relief difference, which
contributes to its climatic comfort. With in a 100 km radius one can sense the
weather contrariety. But, this situation doesn’t secure the country from burden of
diseases.
1.2 Demography
Ethiopia has a population of approximately 65 million, of which more than 51
million (85 percent) live in rural areas. 44.7% of the population is below 15 years
of age while 17.8 % are under five years of age. The high population densities, in
most of the regions, together with the poverty and illiteracy have contributed to
the burden of diseases as well.
1.3 Economy
More than 50 million people live in rural area and depend predominately on
traditional agriculture for their livelihood. Ethiopian economy is dominated by
agriculture, which during 1996/7 accounted for 51% of the GDP, 85% of total
employment, and 85% of exports and for more than 70% of total export earnings.
During the same year, the service sector accounted for 24% of GDP while the
industrial sector contributed about 11% of GDP, 15% of export earnings and less
than 2% of the labor force. Trade and transport contribute 14% of GDP. In spite
of recent achievements in economic growth, poverty remains a problem. With per
capita 1GNP estimated at $110 in 1996, Ethiopia ranks one of the world’s poorest
countries.
This low economical status of the people has influenced the pattern of disease
occurrence in the country.
1.4 Political and Administrative Set up
Ethiopia is a Federal Democratic Republic country composed of nine (9) National
Regional States and two (2) Administrative Councils. The national regional states
as well as the administrative councils are further divided into 62 zones and 523
woredas. There are also 2 zones and 7 woredas classified as special. Beyond
the woreda there are about 10,000 kebeles, which are further, divided into
villages. The health system management is benefiting from the on going process
of democratization and decentralization.
1.5 Health Profile
The Health Policy of the Federal Democratic Republic of Ethiopia (FDRE) was
developed based on the critical examination of the nature, magnitude and root
cause of the prevailing health problems of the country, and the awareness of
newly emerging ones. Focusing on the commitment to democracy, rights and
powers of the people, the health policy aims at promoting the decentralization
process as the most appropriate system of the full exercise of these rights and
powers in pluralistic society.
1 HSDP = Health Sector Development Program GDP= Gross Domestic Product

Ethiopia is undergoing a “Health Sector Reform” through the Health Sector
Development Program (HSDP). The overall goal of the HSDP is to improve the
health status of the population. The structure of the health delivery system has a
pyramid shape, which is broad at the bottom and narrow at the top (Primary
health Care Units at the base, and the specialized referral hospitals at the apex
of the pyramid).
1.6 Health Problem
Ethiopia has extremely poor health status relative to other low-income countries
(largely attributable to potentially preventable infectious diseases and nutritional
deficiencies). The Health Service coverage is 50.4%. Nearly one out of 10 babies
born in Ethiopia does not survive to celebrate his or her first birthday. Under 5
mortality is also high: one out of every six child dies before reaching his or her
fifth birthday. Survey show that mortality has declined during the past 15 years,
the decline having become more pronounced during the last 10 years. Under –5
mortality is 21 percent lower now than it was 5 to 9years ago. Although, there is a
trend of decreasing under-5 mortality, still infant and under-five mortality rate are
high at 97/1000 and 166/1000 live births respectively ( DHS 2000)
The total burden of diseases, as measured by premature death from all causes is
approximately 350 Discounted Life Year (DLY’s) lost per 1000 population.
Communicable diseases, nutrition deficiency, and HIV/AIDS dominate Ethiopia’s
burden of disease. Epidemic-prone diseases such as meningococcal meningitis,
cholera, measles, and bacillary dysentery are also prominent health problem in
the country.
2. THE EXTENT OF THE CURRENT DRAUGHT PROBLEM IN
ETHIOPIA.
A. Climatic condition
The current climatic trends have caused quite a stress on food availability
countrywide. The poor belg rain experienced in many areas has caused serious
food shortage in several part of the country. The impact of the rain on three
important sources of food has particularly been severe. These are:
• The belg crops in a number of areas
• Early maturing non-belg crops, which are important sources of food during
the lean months before the Meher Harvest
• Livestock condition in some of the pastoral areas
A multi-agency team has recently completed its assessment of the above
conditions and has comeback with a worrying picture of the food situation in the
country in the coming two months.
B. Rainfall condition
The onset of this year’s belg rain in most parts of South Tigray the eastern parts
of Oromia, the low lands of east shoa (Fentale area) East and West Hararge and
Bale, several areas in SNNPR, most notably Sidama , Hadiya and Kembat
Timbaro zones as well as Alaba special woredas, the northern parts of Somali
the rain was late, its cessation early and the distribution was poor. In Afar, on the
other hand, the February-May rains completely failed.
In Amhara region, while several woreda did not get rain as of April, few others
experienced serious frost damage.
C. Crop conditions.
The poor rain has caused failure of both the Belg and non-Belg crops planted in
many areas.
The prospect of the long cycle meher crops, Maize and sorghum, which are
planted in April, is also very poor in several areas. The poor rain since April has
severely affected their performances.

D. Livestock condition.
The poor Belg rain has caused acute shortages of water and pasture in several
areas- both cropping and pastoral. The situation is much severe in Somali,
pastoral areas of Oromia and Afar where the February – May rain completely
failed. The rainfall situation in the preceding seasons was also poor. Water and
pasture are seriously short in several areas, most notably in Abala, Beraile,
Erebiti, Koneba, and Dalol woredas of zone two, Amibara, Buremedaitu and
Awash Fentale woredas of zone three and Fursi Artuma and Semurobi woredas
of zone five. In this areas the watering points have dried up while pasture is
seriously short.
Many livestock in these zones have died while the rest are in bad shape. The
shortage of pasture and water has caused abnormal migration of livestock from
one woreda to the others. In addition to water and pasture shortages serious live
stock diseases has been reported in many area of the region. (Details can be
obtained from the DPPC report).
E. Food situation.
The crop failure and poor live stock conditions discussed above have caused
considerable food shortages in all the affected areas. The poor live stock
condition in Afar and the neighboring pastoral areas of Oromia and Somali have
severely curtailed the supply of milk and its impact on the population, particularly
on children is serious. While the poor livestock condition has depressed their
prices grain prices have been increasing considerably making it unaffordable to
many.
Based on the above information the climatic, rainfall, crop, livestock conditions
and food situation in the country a total of 6,000,000 people expected to be
affected according to data released from DPPC. The death of livelihood animals
mainly for the pastoralists worsens the situation of malnutrition to children and
pregnant women since the staple diets of pastoralists are based on milk and milk
products.
II. SITUATIONAL ASSESSMENT
Different teams from the Ministry of Health, Ethiopia, WHO and UNICEF,
assessed the overall health situation in Afar, Somali, Amhara, Oromiya and
SNNPR. The objectives of the rapid assessment were to look at the type
and magnitude of drought related health problems, identify immediate
needs and assess the adequacy of existing capacity of the regions in
handling the situation. The aim was also to identify most vulnerable groups,
assess any indication of malnutrition and come up with plan of action for
immediate measures.
The following were some of the important findings of the need assessment on
health, nutrition, water, sanitation and hygiene, which need interventions. The
worst scenario was observed in Afar and Somali regions.
Ø Deficiency diseases like anemia, in children of under-five years and pregnant
mothers, are observed. The health of mothers, especially pregnant mothers,
is extremely worrying as anemia is being aggravated by severe malnutrition.
Ø Malaria outbreak is expected to occur in the woredas as majority of the
population has migrated to water points where the outbreak is likely. More
cases than usual are being reported to health institutions in the visited sites.
Even though there were no cases of meningococcal meningitis seen in the
woredas up to the time of visit, there is also fear by health institutions that an
epidemic could occur.
Ø The water supply that the communities are using for all purposes is potentially
contaminated. Most are from rivers and stagnant small water bodies. Bloody
diarrhoeal diseases have affected both adults and children since four months
back.
Ø Although no cases were seen and no reports were made to health institutions
recently, there is a potential threat for measles epidemic in the areas visited
particularly zone three of Afar region, as the routine EPI is non-existent and
previous attempts of mass immunization were not successful. This may
reflect the picture of the whole region.
Ø There are numerous cases of whooping cough (Pertusis) in children of under-
five years in Andido town. There are reports that children in neighboring
kebeles are also experiencing the same type of disease for the last two to
three months.
Ø There is critical shortage of drugs and medical supplies in all health
institutions visited in both woredas of Afar Region.
Ø The health service provision in Afar and Somali is tragically poor in all terms,
i.e. all public health programs like vaccinations, health education, and
environmental sanitation activities are either nonexistent or very low and
limited to static sites. EPI out reach activities are totally nonexistent in both
Regions.
Ø All reports from informants and our observations indicate that so many
mothers and elderly remain behind at home only due to "lack of strength" as
they express, which could be due to ill health and starvation.
Ø As a result high rate of malnutrition is eminent, as the population is
completely dependent up on the livestock, camels and their products for
subsistence. Signs of malnutrition in children of under-five years are apparent
in these areas, including specific deficiency diseases like anemia.
Ø Carcasses were scattered all over the whole areas visited, some being in and
around the rivers. We think the cause of such massive death of livestock and
camels are not only shortage of pasture and water, but also some other
diseases. Offending smell from carcasses has polluted the areas and made
the environment unhealthy.
Ø Gross absence of logistics supplies such as motorcycles, cars (pick-ups), etc,
poor preparedness for disaster prevention and emergency handling, poor
management of all existing resources (financial, material, and human
resources) was observed in both Regions.
Based on the findings the teams concluded that:
1. The drought situation in Afar, neighboring regions of Amhara and Oromiya,
and SNNPR is an emergency. Although there is no overt malnutrition
observed on the vulnerable groups, unless supplementary feeding is provided
within short period of time, large number of these vulnerable groups will be
affected.
2. The Afar Regional Health Bureau does not have the capacity to deal with this
emergency. Unless urgent and timely interventions are made, the impact on
health of the people could be disastrous.
3. The pastoralists have already lost their livestock. The loss is expected to
increase as a result of disease and long tracking. Therefore, shortage of food
will remain in the area for longer period of time.
4. Massive accumulation of carcasses created unhealthy environment, which
endangers lives of humans and remaining livestock.
5. Information gathered from the health facilities and residents on disease
condition and malnutrition is only a tip of an iceberg. The fact that there is no
habit of utilizing the health facilities and high mobility from place to place
makes it a reality to consider existence of more problems in the region.
6. EPI activities are more or less discontinued; there is shortage of essential
drugs and supplies in these regions. Population in the affected areas (all
regions) could not afford to pay for medical expenses due to massive death of
their livestock and failure of crops.
III. OBJECTIVES OF THE APPEAL
A. Health
• To provide of emergency equipment, drugs and medical supplies
(Emergency health kits) where intervention is mandatory.
• To develop capacity building in proper case management of malnutrition
related infections, acute nutritional conditions and diarrhoeal diseases.
• To build temporary treatment shelters to facilitate services when the need
arises.
• To conduct surveillance to monitor the health situation before the worst
comes.
• To implement Measles immunization campaign for those under five years
of age and conduct assessment on under 10 and 15 years.
B. Water, sanitation and hygiene.
• To participate and control of the proper disposal of carcasses and related
environmental sanitation.
• To control the proper waste disposal in concentration camps.
• To control the water quality of water distributed to the community.
• To provide health education to the community on water use and waste
disposal.
C. Nutrition
• To improve case management of malnutrition in under five children at the
health facility level.
• To strengthen the referral system of acutely ill malnourished children.
• To ensure the provision of Vitamin A supplement.
IV. GOVERNMENT POLICY AND ACTIONS
The Ethiopian government had established Disaster Prevention and
Preparedness Commission (DPPC) to monitor trends of disasters related to
food shortage and other unusual events that needs massive intervention. The
health sector part was fully delegated to the Ministry of Health, Ethiopia. Thus
health related consequences would be fully addressed by the ministry.
Diseases related to Malnutrition (Marasmus, Marasmus Kwashiorkor,
Kwashiorkor), Malaria, Diarrhea both bloody and watery, Measles and
epidemics like meningitis and cholera are expected while people are coming
together to a concentration camps and food distribution centers.
The primary principles and intention of the health sector according to the
health policy is to prevent likely happenings before it comes to reality. Beside
the prevention aspect there is also a need to prepare the fertile ground for
treatment approaches. The over all aim is to decrease morbidity and mortality
related to the disaster situation of the country. Specific activity of the health
sector was already mentioned above. The government efforts done so far to
address the health related problems were:
a. Established a committee “Health problems due to natural
calamities” composed of different departments and services.
b. Revitalized the “Health response task force” composed of
International, bilateral agencies and NGOs.
c. Deployed essential drugs from the available stock (21 Kits) to the
priority areas identified by the government.
d. Deployed Health manpower (8 health workers from the center and
Addis Ababa health bureau) to those priority areas to participate in
the surveillance and treatment procedures.
e. Reassessed the vaccination and cold chain status of Afar and
Somali regions before the materialization of mass campaigns.
f. Working with WHO closely to secure funds from emergency fund
for the above mentioned activities.
g. Working with the Netherlands embassy to secure funds for drugs
that can be locally purchased.
h. Daily communicates the regions and collect update information
about the situation.
V. ACTIVITIES TO BE PERFORMED BY THE HEALTH SECTOR.
In order to implement the above-mentioned tasks, there is a need of:
A. Supply of essential drugs (Emergency health kits) and medical supplies.
B. Supply of for measles, Meningitis vaccines and Vitamin A.
C. Environmental clearing. (Burning of carcasses)
D. Maintenance and quality control of water supply system.
E. Awareness raising workshops to the community leaders
F. Updating health workers on epidemic diseases management.
G. Transport, fuel cost and daily subsistence allowance to health workers
deployed from the center and other regions.
VI. IMPLEMENTATION OF THE APPEAL
6.1 Institutional operational modalities.
According to the Health delivery system of Ethiopia as described above, the
implementation of this appeal document will utilize the existing health care
facilities as well as temporary treatment shelters, food distribution centers and
mass campaigns.
• The Ministry of health will provide the technical support in the area of
coordination and capacity building in collaboration with the WHO,
UNICEF and other partner agencies.
• The focus will be health institutions to implement preventive as well as
curative procedures. Chiefs and other leaders will be other active
partners in the implementation of the appeal document.
6.2 Collaboration
• The appeal document will be implemented by the Ministry of Health,
Ethiopia in collaboration with different partners, NGOs, International
and bilateral agencies. The Ministry of Health, Ethiopia is the overseer
of the appeal document implementation.
6.3 Monitoring and evaluation.
• Monitoring and supervision will be conducted through the use of the
existing government guideline and regulations.
• Supervisory checklist for health facility assessment will be used during
the monitoring process.
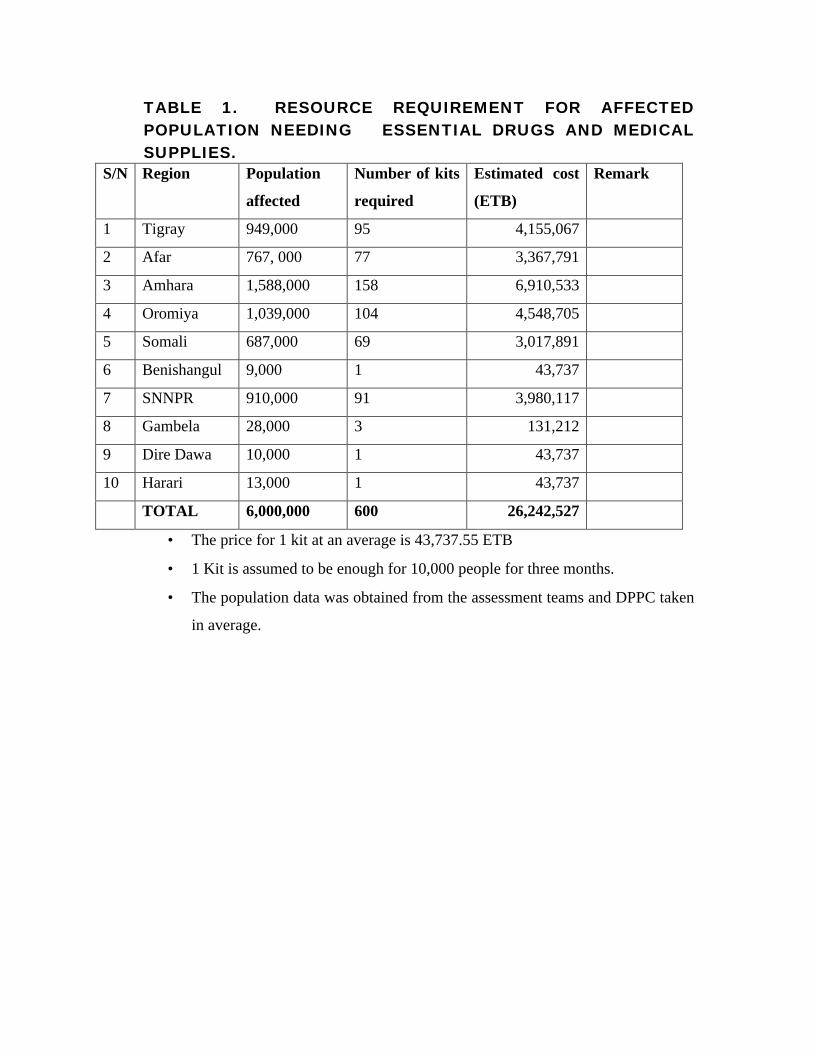
TABLE 1. RESOURCE REQUIREMENT FOR AFFECTEDPOPULATION NEEDING ESSENTIAL DRUGS AND MEDICALSUPPLIES.
S/N Region Population
affected
Number of kits
required
Estimated cost
(ETB)
Remark
1 Tigray 949,000 95 4,155,067
2 Afar 767, 000 77 3,367,791
3 Amhara 1,588,000 158 6,910,533
4 Oromiya 1,039,000 104 4,548,705
5 Somali 687,000 69 3,017,891
6 Benishangul 9,000 1 43,737
7 SNNPR 910,000 91 3,980,117
8 Gambela 28,000 3 131,212
9 Dire Dawa 10,000 1 43,737
10 Harari 13,000 1 43,737
TOTAL 6,000,000 600 26,242,527
• The price for 1 kit at an average is 43,737.55 ETB
• 1 Kit is assumed to be enough for 10,000 people for three months.
• The population data was obtained from the assessment teams and DPPC taken
in average.
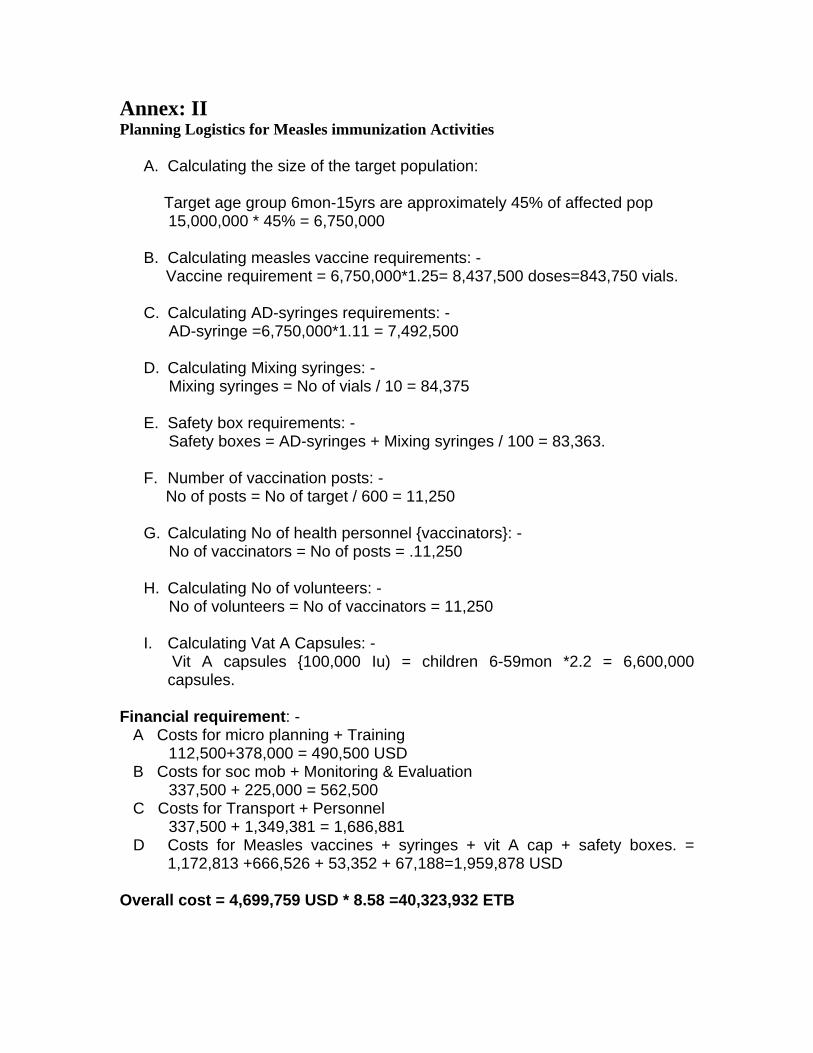
Annex: IIPlanning Logistics for Measles immunization Activities
A. Calculating the size of the target population:
Target age group 6mon-15yrs are approximately 45% of affected pop 15,000,000 * 45% = 6,750,000
B. Calculating measles vaccine requirements: - Vaccine requirement = 6,750,000*1.25= 8,437,500 doses=843,750 vials.
C. Calculating AD-syringes requirements: - AD-syringe =6,750,000*1.11 = 7,492,500
D. Calculating Mixing syringes: - Mixing syringes = No of vials / 10 = 84,375
E. Safety box requirements: - Safety boxes = AD-syringes + Mixing syringes / 100 = 83,363.
F. Number of vaccination posts: - No of posts = No of target / 600 = 11,250
G. Calculating No of health personnel {vaccinators}: - No of vaccinators = No of posts = .11,250
H. Calculating No of volunteers: - No of volunteers = No of vaccinators = 11,250
I. Calculating Vat A Capsules: - Vit A capsules {100,000 Iu) = children 6-59mon *2.2 = 6,600,000capsules.
Financial requirement: - A Costs for micro planning + Training 112,500+378,000 = 490,500 USD B Costs for soc mob + Monitoring & Evaluation 337,500 + 225,000 = 562,500 C Costs for Transport + Personnel 337,500 + 1,349,381 = 1,686,881 D Costs for Measles vaccines + syringes + vit A cap + safety boxes. =
1,172,813 +666,526 + 53,352 + 67,188=1,959,878 USD
Overall cost = 4,699,759 USD * 8.58 =40,323,932 ETB
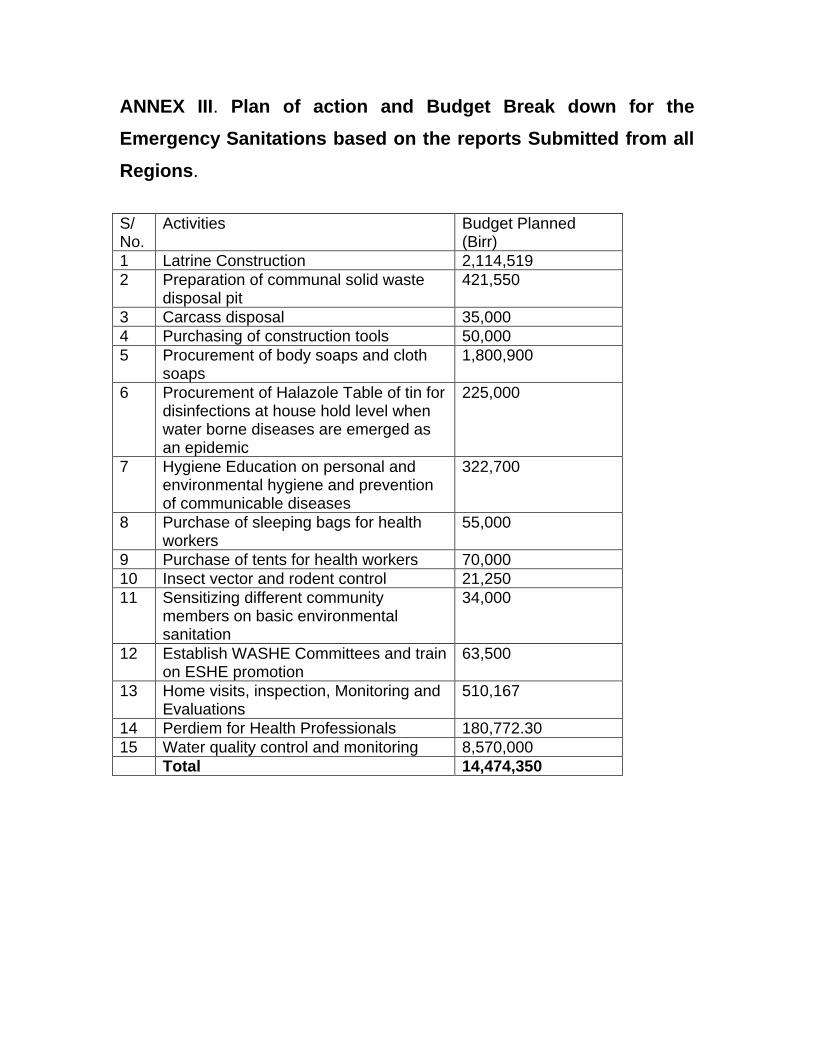
ANNEX III. Plan of action and Budget Break down for the
Emergency Sanitations based on the reports Submitted from all
Regions.
S/No.
Activities Budget Planned(Birr)
1 Latrine Construction 2,114,5192 Preparation of communal solid waste
disposal pit421,550
3 Carcass disposal 35,0004 Purchasing of construction tools 50,0005 Procurement of body soaps and cloth
soaps1,800,900
6 Procurement of Halazole Table of tin fordisinfections at house hold level whenwater borne diseases are emerged asan epidemic
225,000
7 Hygiene Education on personal andenvironmental hygiene and preventionof communicable diseases
322,700
8 Purchase of sleeping bags for healthworkers
55,000
9 Purchase of tents for health workers 70,00010 Insect vector and rodent control 21,25011 Sensitizing different community
members on basic environmentalsanitation
34,000
12 Establish WASHE Committees and trainon ESHE promotion
63,500
13 Home visits, inspection, Monitoring andEvaluations
510,167
14 Perdiem for Health Professionals 180,772.3015 Water quality control and monitoring 8,570,000
Total 14,474,350
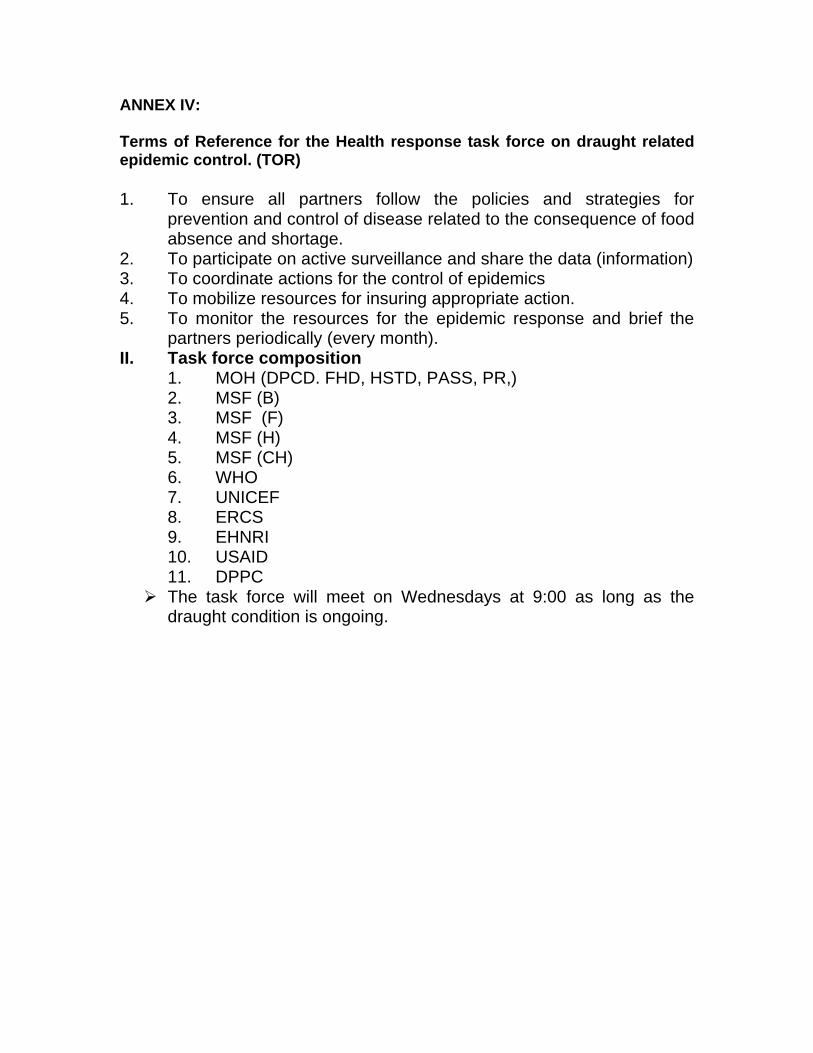
ANNEX IV:
Terms of Reference for the Health response task force on draught relatedepidemic control. (TOR)
1. To ensure all partners follow the policies and strategies forprevention and control of disease related to the consequence of foodabsence and shortage.
2. To participate on active surveillance and share the data (information)3. To coordinate actions for the control of epidemics4. To mobilize resources for insuring appropriate action.5. To monitor the resources for the epidemic response and brief the
partners periodically (every month).II. Task force composition
1. MOH (DPCD. FHD, HSTD, PASS, PR,)2. MSF (B)3. MSF (F)4. MSF (H)5. MSF (CH)6. WHO7. UNICEF8. ERCS9. EHNRI10. USAID11. DPPC
Ø The task force will meet on Wednesdays at 9:00 as long as thedraught condition is ongoing.
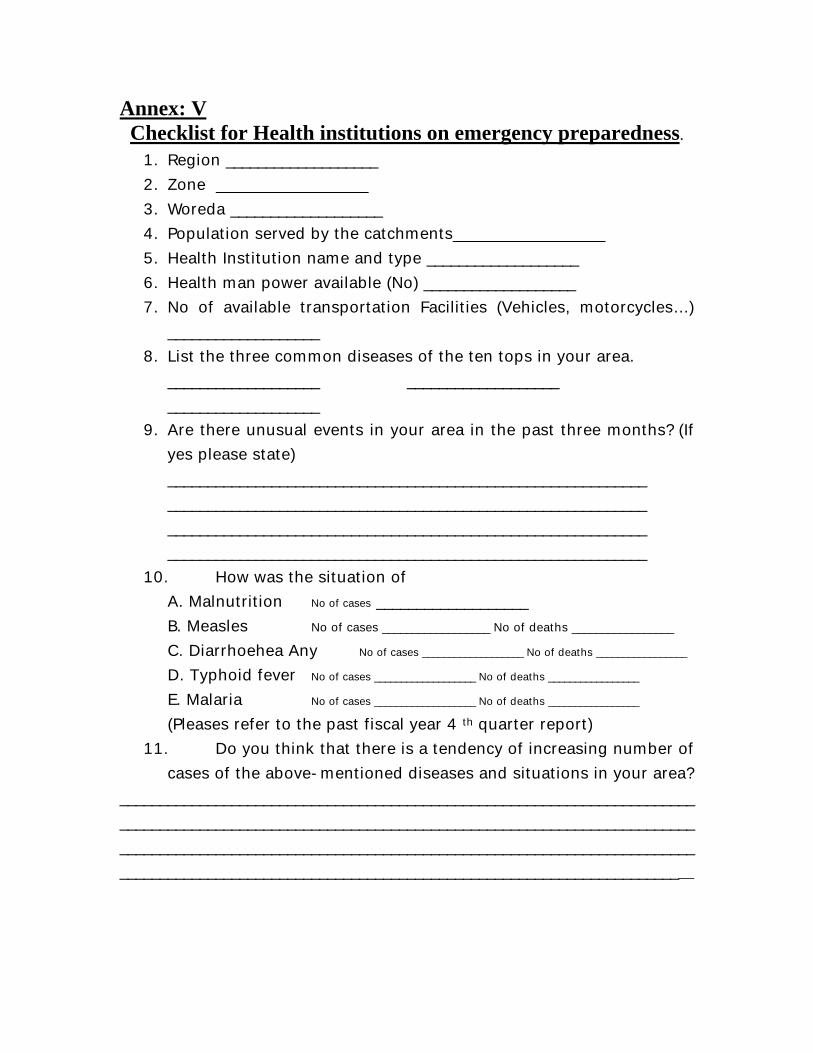
Annex: VChecklist for Health institutions on emergency preparedness.
1. Region ___________________2. Zone ___________________3. Woreda ___________________4. Population served by the catchments___________________5. Health Institution name and type ___________________6. Health man power available (No) ___________________7. No of available transportation Facilities (Vehicles, motorcycles…)
___________________8. List the three common diseases of the ten tops in your area. ___________________ ___________________
___________________9. Are there unusual events in your area in the past three months? (If
yes please state)________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
10. How was the situation ofA. Malnutrition No of cases ___________________B. Measles No of cases __________________ No of deaths _________________
C. Diarrhoehea Any No of cases ___________________ No of deaths _________________
D. Typhoid fever No of cases ___________________ No of deaths _________________
E. Malaria No of cases ___________________ No of deaths _________________
(Pleases refer to the past fiscal year 4 th quarter report)11. Do you think that there is a tendency of increasing number of
cases of the above-mentioned diseases and situations in your area?______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
12. Is there a drug shortage in your health institution? If yes whattypes? Please list them in groups (Anti pyretic, IV fluids… )
13. Do you think that you have enough manpower to mobilize incase if the need arises to move to temporary treatment shelters?
14. Please state health professionals available by category ofprofession.
A. Health assistants. ___________________B. Nurses. ___________________C. Pharmacists ___________________D. Doctors ___________________E. Specialists ___________________
15. Is there any epidemic preparedness committee (EPR) orhealth committee in your area? If yes please state the jobsperformed by the committee.
16. Do you have materials at hand or in your area for temporarytreatment shelters like tents, mattress…
17. Are there any institutions in your area that can serve as atemporary treatment shelter if the need arises? Please state them(Schools, military barracks, Stores…) Likely places mentioned needto be registered.
18. Have you ever had epidemic situation in your area? If yesplease state the type of the disease and control measures undertaken? State your experience.
19. How do you see the disease pattern, food scarcity and rainfallcondition of your area in comparison to the past years?
20. State the health consequences you expect from the situationand preparedness you suggest if any.
21. What are the likely assistances you expect from othersources? Please state them.
22. Name of NGO’s that are active in your area. Please list them.1. __________________________2. __________________________3. __________________________

SUMMARY
Ethiopia has an extremely poor basic health status relative to other low-income
countries (largely attributable to potentially preventable infectious diseases and
nutritional deficiencies). The health service coverage is 50.4%. Nearly one out of
10 babies born in Ethiopia do not survive their first year. Under 5 years mortality
is also high: one out of every six child dies before the age of 5. Communicable
diseases, malnutrition, micronutrient deficiencies, and HIV/AIDS dominate
Ethiopia’s burden of disease. Epidemic-prone diseases such as meningitis,
malaria, cholera, measles, and shigellosis are also prominent health problems.
The worst drought-affected areas with high morbidity are Afar, eastern part of
Oromiya and Somali regions. High levels of malnutrition, vitamin A deficiency and
other micronutrient deficiencies in children under-five years, pregnant and
lactating mothers are widespread and common. High levels of acute malnutrition
have been identified in several nutrition surveys carried out in the affected areas
during the last few months. More nutrition surveys are planned and required to
monitor the condition of malnourished populations and to target health and
nutritional services effectively.
Severely malnourished children (based on nutrition survey data, 2% of the under-
five drought-affected child population or 54,000 children) will require therapeutic
feeding and immediate assistance. Moderately wasted children under five years
(based on nutrition survey data to date, 15% of the under-five drought-affected
population or 400,000 children), and pregnant and lactating women, who are at
high nutritional risk and who constitute 5% of the total population, or 750,000
women, will require supplementary food to prevent severe malnutrition. The
need for supplementary and therapeutic food for the above target population
(approximately 1.2 million women and children) is estimated at 37,500 MT and
4,050 MTs respectively for a period of six months.
Malaria outbreaks are very likely in some of the worst affected areas. Even though currentlythere are no reported outbreaks of meningococcal meningitis there is great potential forepidemics in drought-affected areas. Existing water sources, mostly rivers and stagnantponds, are potentially contaminated. Bloody diarrhoeal disease outbreaks have affected bothadults and children since mid 2002. Basic health service infrastructure in regions like Afarand Somali is poor in all aspects - this applies both to preventive and curative services. Manymothers and elderly remain behind at home due to "lack of strength" as they express, whichcould be due to ill health and starvation. Livestock carcasses are scattered all over drought-affected pastoral areas polluting the environment and causing serious health risks.
Routine EPI coverage is as low as 5% in Somali and Afar Regions. The under-
five population in the affected areas is particularly vulnerable not only to acute
malnutrition and micronutrient deficiencies, but also to communicable diseases
such as measles, diarrhoeal diseases, malaria, Upper Respiratory Tract, skin
and eye infections. These problems need to be addressed in a comprehensive
manner.
The drought situation in Afar, Somali, neighboring regions of Amhara and
Oromiya, Tigray and SNNPR requires urgent health and nutritional interventions
such as supplementary feeding, therapeutic feeding, capacity building of health
workers in management of health and nutritional emergencies, provision of
essential drugs and insecticide treated nets, disease prevention and epidemic
control to prevent further deterioration in the existing condition of drought
affected and displaced population.
The climatic and weather forecast prediction of the country shows that the
situation goes worse and the sole victims of the famine situation increase
exponentially. This is the second appeal document prepared based on the
population figure 15,000,000.
The activities are more or less a continuation of the first appeal document. The
total budget required for current draught situation is 180,447,247 Birr or
21,055,688 USD. Major activities included in this appeal document were:
Procurement of Emergency health kits and distribution to epidemic sites,
Procurement of Measles and Meningitis vaccine and Vitamin A supplementation,
Environmental sanitation and hygiene, Awareness raising workshops, Updating
health workers on epidemic management, Health education team with audio
visual mobile car, and DSA for stationed health workers.
In addition long-term activities were included in this appeal document assuming
that the draught situation might continues sometime longer than the expected
next Belg rain crop yields. Thus activities like Malaria control, Maintenance of
cold chain, Therapeutic foods (F-100, F-75), HIV/ AIDS awareness, Quality
control water resources, Capacity building of health man power in disaster
management, strengthening, IDSR activities and Monitoring and evaluation
The promises made by different international, bilateral organizations and NGO’s in responsefor the first appeal document was good. We thank all the organizations who are full heartedlyworking with us in our “ Health response task force”.
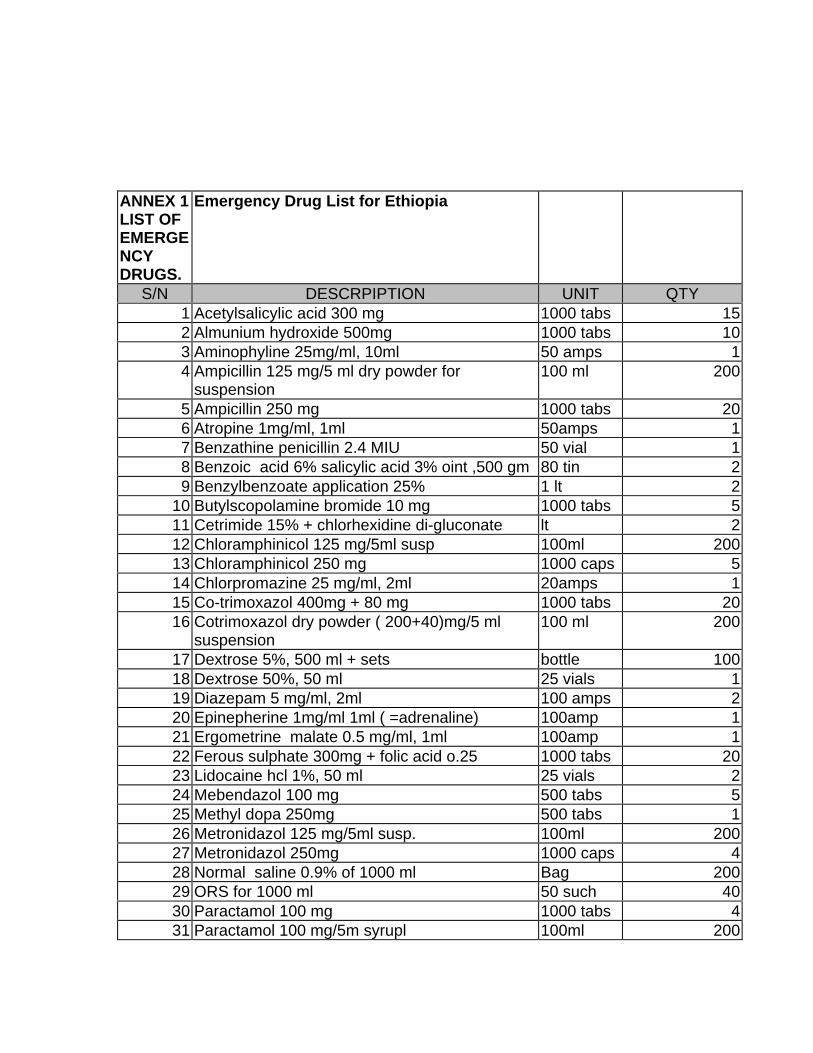
ANNEX 1LIST OFEMERGENCYDRUGS.
Emergency Drug List for Ethiopia
S/N DESCRPIPTION UNIT QTY1 Acetylsalicylic acid 300 mg 1000 tabs 152 Almunium hydroxide 500mg 1000 tabs 103 Aminophyline 25mg/ml, 10ml 50 amps 14 Ampicillin 125 mg/5 ml dry powder for
suspension100 ml 200
5 Ampicillin 250 mg 1000 tabs 206 Atropine 1mg/ml, 1ml 50amps 17 Benzathine penicillin 2.4 MIU 50 vial 18 Benzoic acid 6% salicylic acid 3% oint ,500 gm 80 tin 29 Benzylbenzoate application 25% 1 lt 2
10 Butylscopolamine bromide 10 mg 1000 tabs 511 Cetrimide 15% + chlorhexidine di-gluconate lt 212 Chloramphinicol 125 mg/5ml susp 100ml 20013 Chloramphinicol 250 mg 1000 caps 514 Chlorpromazine 25 mg/ml, 2ml 20amps 115 Co-trimoxazol 400mg + 80 mg 1000 tabs 2016 Cotrimoxazol dry powder ( 200+40)mg/5 ml
suspension100 ml 200
17 Dextrose 5%, 500 ml + sets bottle 10018 Dextrose 50%, 50 ml 25 vials 119 Diazepam 5 mg/ml, 2ml 100 amps 220 Epinepherine 1mg/ml 1ml ( =adrenaline) 100amp 121 Ergometrine malate 0.5 mg/ml, 1ml 100amp 122 Ferous sulphate 300mg + folic acid o.25 1000 tabs 2023 Lidocaine hcl 1%, 50 ml 25 vials 224 Mebendazol 100 mg 500 tabs 525 Methyl dopa 250mg 500 tabs 126 Metronidazol 125 mg/5ml susp. 100ml 20027 Metronidazol 250mg 1000 caps 428 Normal saline 0.9% of 1000 ml Bag 20029 ORS for 1000 ml 50 such 4030 Paractamol 100 mg 1000 tabs 431 Paractamol 100 mg/5m syrupl 100ml 200
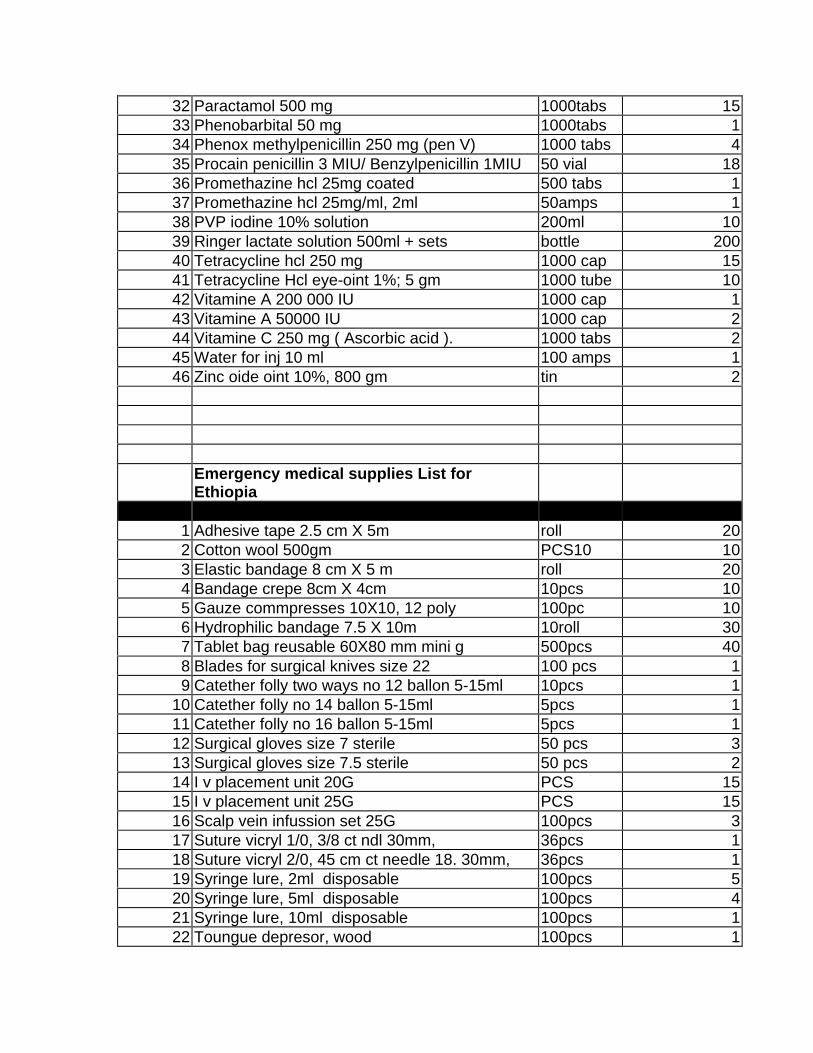
32 Paractamol 500 mg 1000tabs 1533 Phenobarbital 50 mg 1000tabs 134 Phenox methylpenicillin 250 mg (pen V) 1000 tabs 435 Procain penicillin 3 MIU/ Benzylpenicillin 1MIU 50 vial 1836 Promethazine hcl 25mg coated 500 tabs 137 Promethazine hcl 25mg/ml, 2ml 50amps 138 PVP iodine 10% solution 200ml 1039 Ringer lactate solution 500ml + sets bottle 20040 Tetracycline hcl 250 mg 1000 cap 1541 Tetracycline Hcl eye-oint 1%; 5 gm 1000 tube 1042 Vitamine A 200 000 IU 1000 cap 143 Vitamine A 50000 IU 1000 cap 244 Vitamine C 250 mg ( Ascorbic acid ). 1000 tabs 245 Water for inj 10 ml 100 amps 146 Zinc oide oint 10%, 800 gm tin 2
Emergency medical supplies List forEthiopia
S/N DESCRIPTION UNIT QTY1 Adhesive tape 2.5 cm X 5m roll 202 Cotton wool 500gm PCS10 103 Elastic bandage 8 cm X 5 m roll 204 Bandage crepe 8cm X 4cm 10pcs 105 Gauze commpresses 10X10, 12 poly 100pc 106 Hydrophilic bandage 7.5 X 10m 10roll 307 Tablet bag reusable 60X80 mm mini g 500pcs 408 Blades for surgical knives size 22 100 pcs 19 Catether folly two ways no 12 ballon 5-15ml 10pcs 1
10 Catether folly no 14 ballon 5-15ml 5pcs 111 Catether folly no 16 ballon 5-15ml 5pcs 112 Surgical gloves size 7 sterile 50 pcs 313 Surgical gloves size 7.5 sterile 50 pcs 214 I v placement unit 20G PCS 1515 I v placement unit 25G PCS 1516 Scalp vein infussion set 25G 100pcs 317 Suture vicryl 1/0, 3/8 ct ndl 30mm, 36pcs 118 Suture vicryl 2/0, 45 cm ct needle 18. 30mm, 36pcs 119 Syringe lure, 2ml disposable 100pcs 520 Syringe lure, 5ml disposable 100pcs 421 Syringe lure, 10ml disposable 100pcs 122 Toungue depresor, wood 100pcs 1
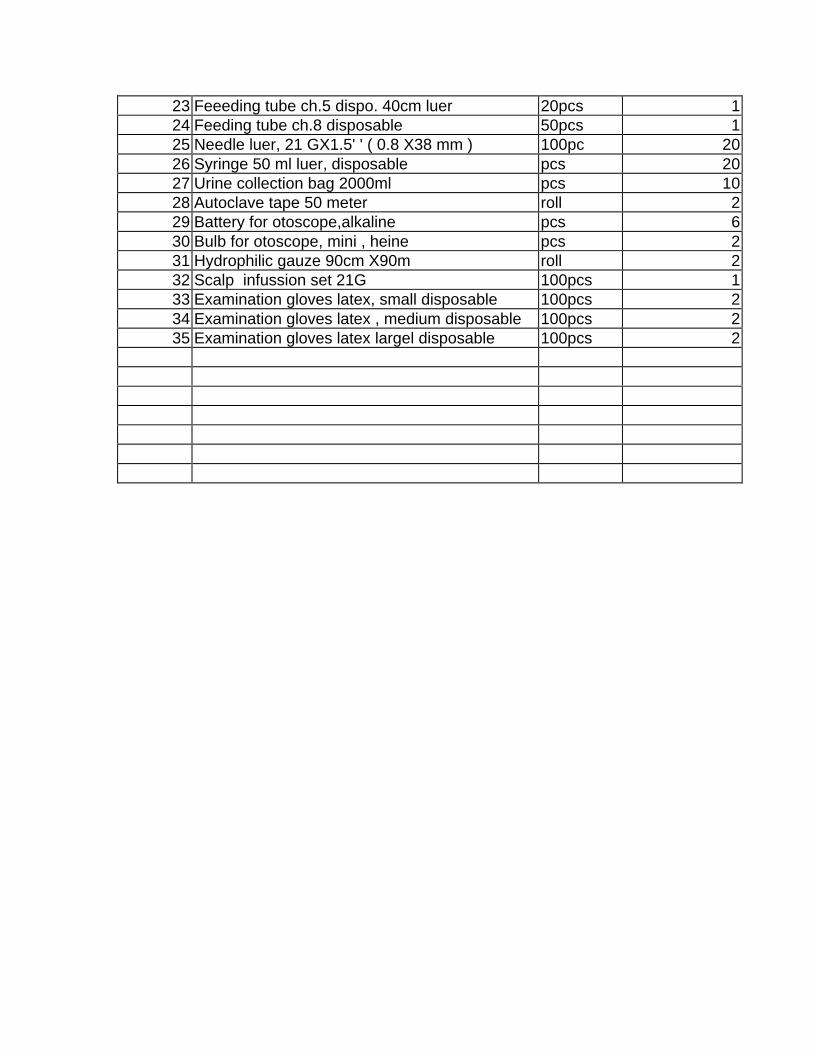
23 Feeeding tube ch.5 dispo. 40cm luer 20pcs 124 Feeding tube ch.8 disposable 50pcs 125 Needle luer, 21 GX1.5' ' ( 0.8 X38 mm ) 100pc 2026 Syringe 50 ml luer, disposable pcs 2027 Urine collection bag 2000ml pcs 1028 Autoclave tape 50 meter roll 229 Battery for otoscope,alkaline pcs 630 Bulb for otoscope, mini , heine pcs 231 Hydrophilic gauze 90cm X90m roll 232 Scalp infussion set 21G 100pcs 133 Examination gloves latex, small disposable 100pcs 234 Examination gloves latex , medium disposable 100pcs 235 Examination gloves latex largel disposable 100pcs 2
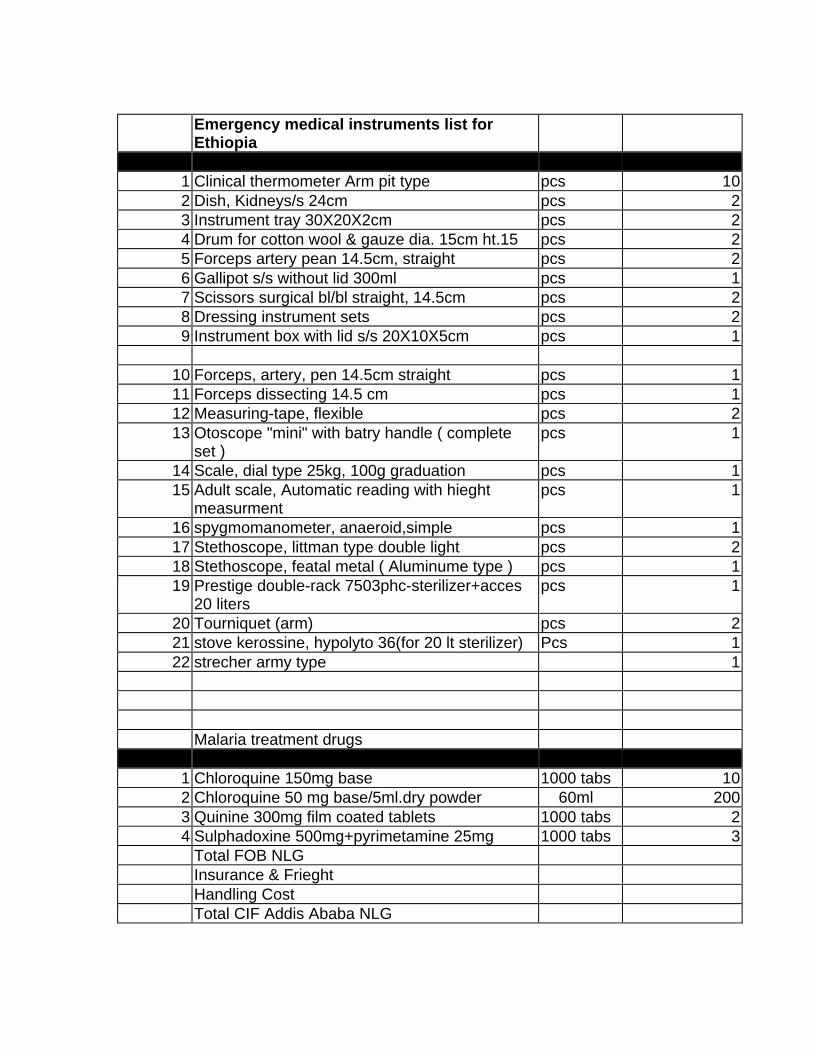
Emergency medical instruments list forEthiopia
S/N DESCRIPTION UNIT QTY1 Clinical thermometer Arm pit type pcs 102 Dish, Kidneys/s 24cm pcs 23 Instrument tray 30X20X2cm pcs 24 Drum for cotton wool & gauze dia. 15cm ht.15 pcs 25 Forceps artery pean 14.5cm, straight pcs 26 Gallipot s/s without lid 300ml pcs 17 Scissors surgical bl/bl straight, 14.5cm pcs 28 Dressing instrument sets pcs 29 Instrument box with lid s/s 20X10X5cm pcs 1
10 Forceps, artery, pen 14.5cm straight pcs 111 Forceps dissecting 14.5 cm pcs 112 Measuring-tape, flexible pcs 213 Otoscope "mini" with batry handle ( complete
set )pcs 1
14 Scale, dial type 25kg, 100g graduation pcs 115 Adult scale, Automatic reading with hieght
measurmentpcs 1
16 spygmomanometer, anaeroid,simple pcs 117 Stethoscope, littman type double light pcs 218 Stethoscope, featal metal ( Aluminume type ) pcs 119 Prestige double-rack 7503phc-sterilizer+acces
20 literspcs 1
20 Tourniquet (arm) pcs 221 stove kerossine, hypolyto 36(for 20 lt sterilizer) Pcs 122 strecher army type 1
Malaria treatment drugsS/N DESCRIPTION UNIT QTY
1 Chloroquine 150mg base 1000 tabs 102 Chloroquine 50 mg base/5ml.dry powder 60ml 2003 Quinine 300mg film coated tablets 1000 tabs 24 Sulphadoxine 500mg+pyrimetamine 25mg 1000 tabs 3
Total FOB NLGInsurance & FrieghtHandling CostTotal CIF Addis Ababa NLG
Top Related