





Languages
Pages
Legal


Emerging Infectious Disease Emerging Infectious Disease (EID) involving Respiratory Tract (EID) involving Respiratory Tract
Sanit Reungrongrat, MDSanit Reungrongrat, MD
Pediatrics Department, Faculty of Pediatrics Department, Faculty of Medicine, Chiang Mai UniversityMedicine, Chiang Mai University

Underlying causes for EIDUnderlying causes for EID
1.1. Generalized social changesGeneralized social changes • worldwide urbanization, IV drug abuse, worldwide urbanization, IV drug abuse,
changing sexual practicechanging sexual practice
2.2. Demographic changesDemographic changes• human mobility and refugee populationhuman mobility and refugee population
3.3. Medical careMedical care• blood transfusion, organ transplant, blood transfusion, organ transplant,
re-used syringes for antibiotic injections, re-used syringes for antibiotic injections, contamination vaccines and antibiotic contamination vaccines and antibiotic resistanceresistance
Kuiken T, et al. Curr Opin Biotech 2003;14:641

4.4. Economic and commercial trendsEconomic and commercial trends • intensive food production, extended intensive food production, extended
irrigation, liberalized trading patternirrigation, liberalized trading pattern
5.5. Climatic changesClimatic changes• global warming and regional changesglobal warming and regional changes
6.6. Ecosystem disturbanceEcosystem disturbance• deforestation, eutrophication of waterways, deforestation, eutrophication of waterways,
reduction in predators of disease vector reduction in predators of disease vector organismsorganisms
Underlying causes for EIDUnderlying causes for EID
Kuiken T, et al. Curr Opin Biotech 2003;14:641

Human MetapneumovirusHuman Metapneumovirus(hMPV)(hMPV)

hMPVhMPV
• Is a pathogen that emerged as a result of Is a pathogen that emerged as a result of increased and tenacious diagnostic effortsincreased and tenacious diagnostic efforts rather than through expansion of it range rather than through expansion of it range or transmission to a new host speciesor transmission to a new host species
• First identified in First identified in 20012001 by van den Hoogen by van den Hoogen BC, et al. (Nat Med 2001;7:719)BC, et al. (Nat Med 2001;7:719)
• Isolated from 28 young children, stored Isolated from 28 young children, stored nasopharyngeal aspiration (NPA) with RTI nasopharyngeal aspiration (NPA) with RTI over 20 years in Netherlandsover 20 years in Netherlands– New member of New member of MetapneumovirusMetapneumovirus genus genus, ,
ParamyxoviridaeParamyxoviridae family family

Classification of Viral Pathogens of Classification of Viral Pathogens of Paramyxoviridae FamilyParamyxoviridae Family
McIntosh K, McAdam AJ. N Engl J Med 2004;350:431
Paramyxoviridae
Pneumovirinae
Metapneumovirus
HumanMetapneumonvirus

Genomic Structure of hMPVGenomic Structure of hMPV
Pneumoviruses: 3Pneumoviruses: 3''-NS1-NS2-N-P--NS1-NS2-N-P-M-SH-G-F-M2-LM-SH-G-F-M2-L-5-5''
Metapneumoviruses: 3'-N-P-M-F-M2-SH-G-L-5'Metapneumoviruses: 3'-N-P-M-F-M2-SH-G-L-5'
Pneumoviruses: 3Pneumoviruses: 3''-NS1-NS2-N-P--NS1-NS2-N-P-M-SH-G-F-M2-LM-SH-G-F-M2-L-5-5''
Metapneumoviruses: 3'-N-P-M-F-M2-SH-G-L-5'Metapneumoviruses: 3'-N-P-M-F-M2-SH-G-L-5'
• 13,350 nucleotides13,350 nucleotides• Negative-sense, nonsegmented RNANegative-sense, nonsegmented RNA• PneumovirinaePneumovirinae subfamilysubfamily are distinguished from are distinguished from
ParamyxovirinaeParamyxovirinae subfamily by subfamily by– Distantly related amino acid sequencesDistantly related amino acid sequences– Significant related to F (fusion) and L (polymerase) Significant related to F (fusion) and L (polymerase)
proteinsproteins– PneumovirinaePneumovirinae encode more mRNA (8-10 vs. 6-7), and encode more mRNA (8-10 vs. 6-7), and
proteins (NS1, NS2, M2-1,M2-2) which not found in proteins (NS1, NS2, M2-1,M2-2) which not found in ParamyxovirinaeParamyxovirinae
• Metapneumovirus Metapneumovirus lack NS1, NS2 and have lack NS1, NS2 and have different positioning of the genes between M, and Ldifferent positioning of the genes between M, and L
Domachowske JB, et al. Clin Microbiol Newsletter 2003;25:17

Electron Micrograph of hMPVElectron Micrograph of hMPV
• PleomorphicPleomorphic• Average size Average size
100-600 nm100-600 nm• Nucleocapsids Nucleocapsids
rarely observedrarely observed• Envelope Envelope
projections of projections of 13-17 nm13-17 nm
Nat Med 2001;7:719
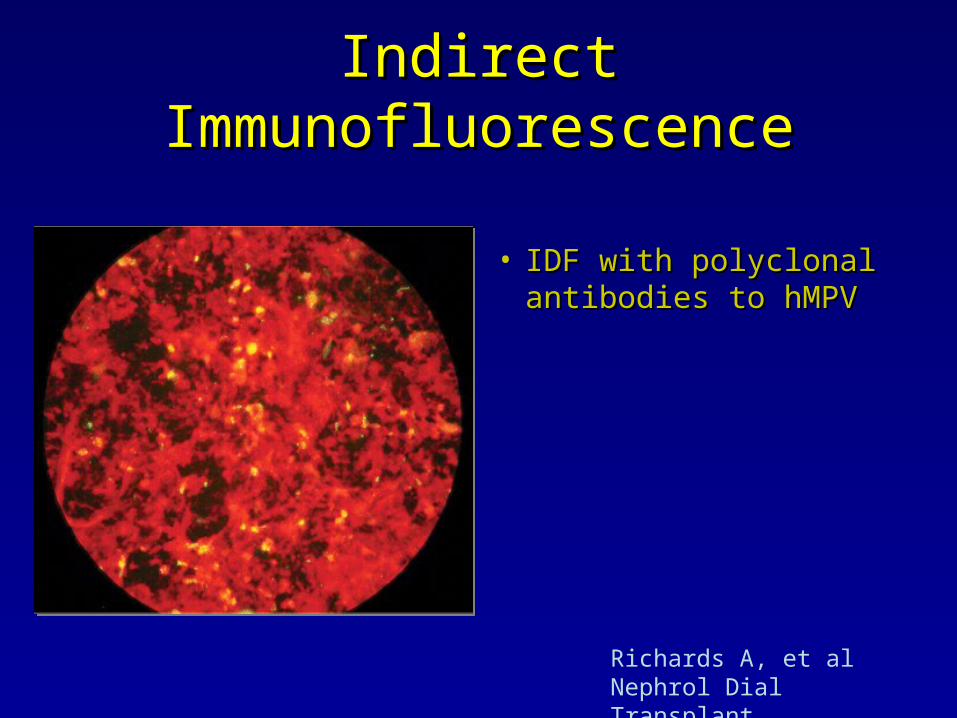
Indirect ImmunofluorescenceIndirect Immunofluorescence
• IDF with polyclonal IDF with polyclonal antibodies to hMPVantibodies to hMPV
Richards A, et al Nephrol Dial Transplant 2005;20:2848-50

Virus Isolation, Cell Culture and Growth Virus Isolation, Cell Culture and Growth Characteristics of hMPVCharacteristics of hMPV
• Identified byIdentified by RAP-PCR– Is semi-quantitative reverse
transcriptase PCR-based technique (RT-PCR) that is used to compare the entire pool of transcripts
– Real-time PCR is rapid (<2hr)
• Culture byCulture by tertiary monkey kidney cells (tMK), LLC-MK2, Vero cell lines– hMPV grows very slowlyvery slowly
(10-14 days) observe by cytopathic effect (CPE)cytopathic effect (CPE)
– hMPV replication is trypsin dependent
Nat Med 2001;7:719CPE: morphologic characteristics of monolayer change as virions replicate inside the cells

Phylogeny of hMPVPhylogeny of hMPV• Indicator for the Indicator for the
relationship between the relationship between the newly identified virus newly identified virus isolates and members of isolates and members of PneumovirinaePneumovirinae
• Phylogenetic trees were Phylogenetic trees were constructed based on the constructed based on the N, P, M and FN, P, M and F ORFsORFs of of these virusesthese viruses

Heterogeneity of hMPVHeterogeneity of hMPV
• Phylogenetic tree analysis of Phylogenetic tree analysis of sequencesequence11
– Divided in two genotypes: Divided in two genotypes: A and BA and B– Both genotypes can be divided in Both genotypes can be divided in
two subgroups: two subgroups: A1, A2, B1, B2A1, A2, B1, B2– The F proteinThe F protein revealed revealed ~95%~95%
amino acid sequence identity amino acid sequence identity between virus genotype A and Bbetween virus genotype A and B
– the G proteinthe G protein shared only shared only 30%30% identityidentity
• Virus neutralization assaysVirus neutralization assays with with genotype-specific antibody genotype-specific antibody demonstrated demonstrated 12- to >100-fold12- to >100-fold difference between genotype A difference between genotype A and Band B
• Genotype A has clinical severity Genotype A has clinical severity than genotype Bthan genotype B22
F geneF gene G geneG gene
1. Van den Hoogen BG, et al. Pediatr Infect Dis J 2004;23:S25.
2. Vicente D, et al. Clin Infect Dis 2006;42:e111.

Seroprevalence of hMPVSeroprevalence of hMPV Immunofluorescence assaysImmunofluorescence assays Virus neutralization assaysVirus neutralization assays
Age (yrs) n tested n positive (%) n tested n positive (%) titer
0.5-1 20 5 (25) 12 3 (25) 16-32
1-2 20 11 (55) 13 4 (31) 16-32
2-5 20 14 (70) 8 3 (38) 16-512
5-10 20 20 (100) 4 4 (100) 32-256
10-20 20 20 (100) 4 3 (75) 32-128
>20 20 20 (100) 4 3 (75) 32-128
8-99* 72 72 (100) 11 11 (100) 16-128
Nat Med 2001;7:719
*Sero-archeological analysis using sera collection in 1958
1.1. Serologic studies showed circulating antibodies to the virus in virtually all Serologic studies showed circulating antibodies to the virus in virtually all children age 5 years or olderchildren age 5 years or older
2.2. On the basic antibody prevalence, hMPV has circulate in the human On the basic antibody prevalence, hMPV has circulate in the human populations populations at least 45 yearsat least 45 years and more likely longer and more likely longer
Several epidemiologic studies of hMPV in most parts of the world
36 studies: 2.2-30%36 studies: 2.2-30%

5.4
27.4
5.5
16.7
30
20.1
15.7
4.7
7.3
12
7.1
5.8
11
0 5 10 15 20 25 30 35
Thai(01-03)
Taiwan(01-02)
Hongkong(01-02)
China1(02-03)
China2(02-03)
Japan(04-05)
Korea1(97-00)
Korea2(00-05)
Korea3(03-05)
India(04-05)
Austraria(01-04)
South Africa(01-03)
Yemen(02-03)
N=236,mean age 22 mo (9-38 mo)
N=116
N=587, age<18yr
N=126
N=247
N=144
N=166
N=515
N=381, age<15yr, median age 15 mo
N=97, age<5yr
N=10,025, 4mo-79yr, mean 8.2yr, median 1.37yr, 92% <5yr
N=488,01-7.7%, 02-19%, 03-2.2%, 2.7%;HIV-infected infant
N=601, age<2yr

2.2
8.5
3.1
2.8
25
21
8
2.9
14.5
17.5
17.9
13
0 5 10 15 20 25 30
UK(00-01)
France(03-04)
Italy1(02-03)
Italy2(02-03)
Italy3(00-02)
Norwy(02-03)
Finland(00-01)
Denmark(99-00)
Austria(03-04)
Germany1(Jan-May02)
Germany2(02-03)
Isarael(01-02)
N=711, all age
N=589, age<5yr
N=1,331, age<15yr
N=1,505, age<15yr
N=90, age<2yr
N=236, median age 12 mo
N=132, age 3mo-16yr
N=374
N=214, mean age 10.1 mo
N=63, age<2yr
N=116, age 3mo-16yr
N=516, age<5yr

8.1
6.4
20
5
2.6
7.1
14.8
6
14
16.2
11
0 5 10 15 20 25
USA1(01-02)
USA2(01-02)
USA3(76-01)
USA4(82-01)
USA5(01-04)
Canada1(93-01)
Canada2(01-02)
Canada3(01-02)
Spain1(00-03)
Spain2(03-04)
Argentina(98-02)
N=668, age<5yr
N=296
N=248
N=2,384; detect AOM 50%
N=1,294, all age
N=38
N=445, age 2mo-93yr)
N=208, age<3yr
N=749, age<2yr
N=211, age<1yr
N=440, age<5yr

• In the community In the community ~2.2% - 5%~2.2% - 5%
• In hospitalized children In hospitalized children ~5% - 10%~5% - 10%– Age Age <<18 years: 18 years: 2.8% - 17.9% 2.8% - 17.9% – Age Age <<5 years: 5 years: 5.5% - 13%5.5% - 13%– Age Age <<3 years: 3 years: 4.1% - 6%4.1% - 6%– Age Age <<2 years:2 years: 11% - 25%11% - 25%– Age Age <<1 year: 1 year: 16.2%16.2%
Epidemiology of hMPVEpidemiology of hMPV

Age and Seasonal Distribution of hMPV (All Age)Age and Seasonal Distribution of hMPV (All Age)(Osterhaus A, Fouchier R. Lancet 2003;361:890. (N=115)(Osterhaus A, Fouchier R. Lancet 2003;361:890. (N=115)
Age and Seasonal Distribution of hMPV (All Age)Age and Seasonal Distribution of hMPV (All Age)(Osterhaus A, Fouchier R. Lancet 2003;361:890. (N=115)(Osterhaus A, Fouchier R. Lancet 2003;361:890. (N=115)
0
5
10
15
20
25
30
0-1 1-2 2-5 5-20 20-65 >650
5
10
15
20
25
30
Jul
Aug Sep OctNov Dec Ja
nFeb M
ar AprM
ay Jun
Nu
mb
er
of
pa
tie
nt
Age range (years) Month
Netherland
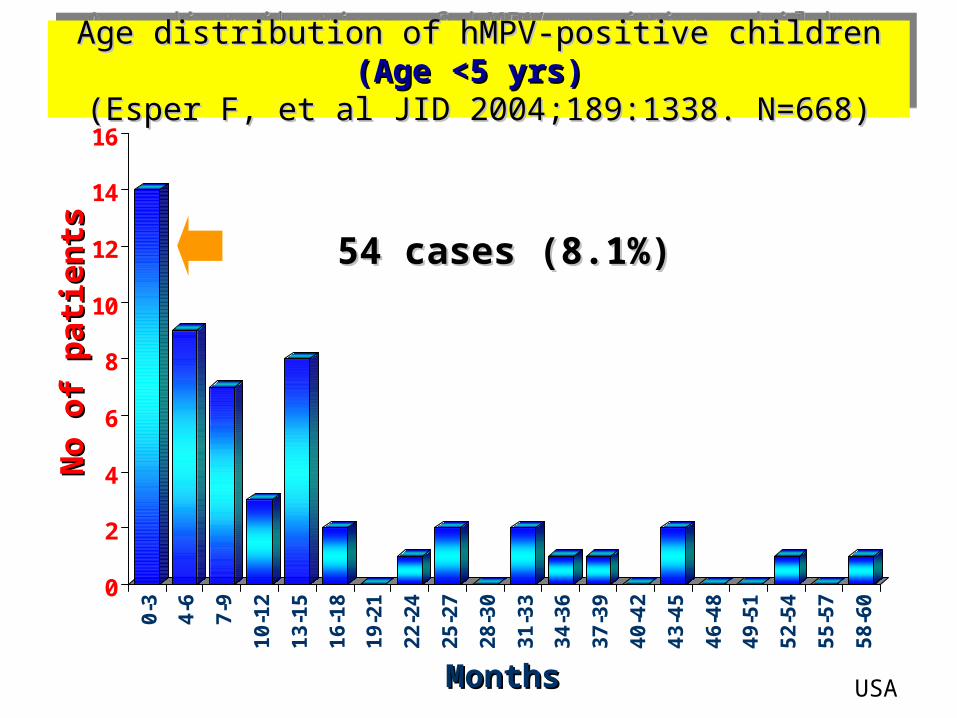
Age distribution of hMPV-positive children Age distribution of hMPV-positive children (Age <5 yrs)(Age <5 yrs) (Esper F, et al JID 2004;189:1338. N=668)(Esper F, et al JID 2004;189:1338. N=668)
Age distribution of hMPV-positive children Age distribution of hMPV-positive children (Age <5 yrs)(Age <5 yrs) (Esper F, et al JID 2004;189:1338. N=668)(Esper F, et al JID 2004;189:1338. N=668)
0
2
4
6
8
10
12
14
160
-3
4-6
7-9
10
-12
13
-15
16
-18
19
-21
22
-24
25
-27
28
-30
31
-33
34
-36
37
-39
40
-42
43
-45
46
-48
49
-51
52
-54
55
-57
58
-60
MonthsMonths
No
of
pat
ien
tsN
o o
f p
atie
nts 54 cases (8.1%)54 cases (8.1%)
USA

Age distribution of hMPV-positive children Age distribution of hMPV-positive children (Age <3 yrs)(Age <3 yrs) (Boivin G, et al Emerg Infect Dis 2003;9:634. N=208)(Boivin G, et al Emerg Infect Dis 2003;9:634. N=208)
Age distribution of hMPV-positive children Age distribution of hMPV-positive children (Age <3 yrs)(Age <3 yrs) (Boivin G, et al Emerg Infect Dis 2003;9:634. N=208)(Boivin G, et al Emerg Infect Dis 2003;9:634. N=208)
0
0.5
1
1.5
2
2.5
3
3.5
40
-2
3-5
6-8
9-1
1
12
-14
15
-17
18
-20
21
-23
24
-26
27
-29
30
-32
33
-35
MonthsMonths
No
of
pat
ien
tsN
o o
f p
atie
nts 12 cases (6%)12 cases (6%)
Canada

• Year of study – vary by year or location Year of study – vary by year or location “periodic epidemics”“periodic epidemics”– North America study:North America study: more frequent in more frequent in 20012001
than than 2000 2000 (7% vs.1.5%)(7% vs.1.5%)– Italian study:Italian study: more frequent in more frequent in 20022002 and and 2000 2000
than than 20012001 (43%, 37% vs.7%) (43%, 37% vs.7%)– African study:African study: more frequent in more frequent in 20022002 than than
20012001 and and 20032003 (19% vs. 7.7%, 2.2%) (19% vs. 7.7%, 2.2%)• SeasonalitySeasonality
– Temperate region:Temperate region: late winter to spring late winter to spring– Subtropics region:Subtropics region: late spring to summer (HK) late spring to summer (HK)
Epidemiology of hMPVEpidemiology of hMPV

0
5
10
15
20
Su Au W Sp Su Au W Sp Su Au W Sp Su Au W Sp
Seasonal incidence of hMPV. Queensland Australia, 2001-Seasonal incidence of hMPV. Queensland Australia, 2001-2004 (Sloots TP, et al. Emerg Infect Dis 2006;12:1263)2004 (Sloots TP, et al. Emerg Infect Dis 2006;12:1263)
Seasonal incidence of hMPV. Queensland Australia, 2001-Seasonal incidence of hMPV. Queensland Australia, 2001-2004 (Sloots TP, et al. Emerg Infect Dis 2006;12:1263)2004 (Sloots TP, et al. Emerg Infect Dis 2006;12:1263)
Su, summer (Dec-Feb); Au, autumn (Mar-May); W, winter (Jun-Aug); Sp, spring (Sep-Nov)
N=10,025, All agesN=10,025, All ages
• Asymptomatic infection is rare• Incubation period 4-6 days, duration of
symptoms before seeking medical usually <7 days, viral shedding ~ 1-2 weeks
• Peak age 6-12 months, male predomonant• 30-85% of hospitalized children have
underlying disease– prematurity, chronic lung disease congenital
heart disease, cancer, HIV-infected, asthma, renal failure, GERD
Epidemiology of hMPVEpidemiology of hMPV

• Coinfection (5-17%) with virus or bacteria, most common is RSV– Others are influenza, parainfluenza,
adenovirus, CMV, rhinovirus, SARS, S pneumoniae, M pneumoniae, C pneumoniae, H influenzae, K pneumoniae, E coli
• Cocirculation of different hMPV genotypes in one year
Epidemiology of hMPVEpidemiology of hMPV
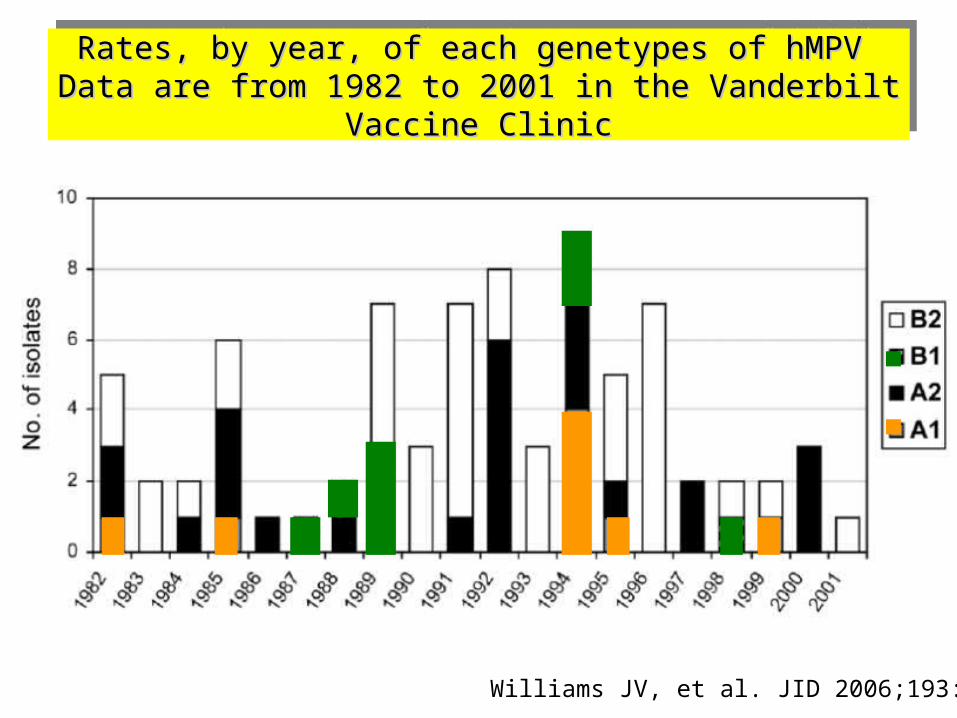
Rates, by year, of each genetypes of hMPVRates, by year, of each genetypes of hMPV Data are from 1982 to 2001 in the Vanderbilt Vaccine ClinicData are from 1982 to 2001 in the Vanderbilt Vaccine Clinic
Rates, by year, of each genetypes of hMPVRates, by year, of each genetypes of hMPV Data are from 1982 to 2001 in the Vanderbilt Vaccine ClinicData are from 1982 to 2001 in the Vanderbilt Vaccine Clinic
Williams JV, et al. JID 2006;193:387

Distribution of hMPV subtype in Distribution of hMPV subtype in Queenland, Australia, 2001-2004Queenland, Australia, 2001-2004
YearYear
Total Total samples samples testedtested
hMPV subtypeshMPV subtypes
A1A1 A2A2 B1B1 B2B2
20012001 5959 5858 2424 88 1010
20022002 122122 2020 5151 1212 1717
20032003 189189 1010 3636 3030 2424
20042004 270270 11 2323 5959 1717
Sloots TP. Et al. Emerg Infect Dis 2006;12:1263
• Clinical records: 74.4% admitted, LOS median, 3 days; mean 6.5 day, Clinical records: 74.4% admitted, LOS median, 3 days; mean 6.5 day, predominant S&S, cough, rhinorrhea, crackles, fever (N=273 cases)predominant S&S, cough, rhinorrhea, crackles, fever (N=273 cases)
• Classification severity: mild 46.8%, moderate 42.5%, severe 10.7%Classification severity: mild 46.8%, moderate 42.5%, severe 10.7%

Comparison of hMPV and RSV (1)Comparison of hMPV and RSV (1)
• Overall, hMPV is Overall, hMPV is less commonlyless commonly isolated from isolated from respiratory specimens than RSVrespiratory specimens than RSV
• RSV appears RSV appears more commonmore common than hMPV in than hMPV in infants <6 monthsinfants <6 months
• SimilarSimilar to RSV, majority of hMPV cases occur in to RSV, majority of hMPV cases occur in young (<5 yrs) and elderly (>65 yrs)young (<5 yrs) and elderly (>65 yrs)
• hMPV peaks later (hMPV peaks later (AprilApril), where as RSV peaks ), where as RSV peaks earlier (earlier (December-FebruaryDecember-February))
• hMPV and RSV have hMPV and RSV have similarsimilar clinical clinical presentation in children and elderlypresentation in children and elderly
• In 1 study In 1 study ((Greensill J, et al. Emerg Infect Dis 2003;9:372Greensill J, et al. Emerg Infect Dis 2003;9:372)), , hMPV/RSV coinfection was detected in 70%hMPV/RSV coinfection was detected in 70%

Comparison of hMPV and RSV (2)Comparison of hMPV and RSV (2)
• While both hMPV and RSV can provokes severe While both hMPV and RSV can provokes severe infections, disease severity and hospitalization infections, disease severity and hospitalization appears more common with RSVappears more common with RSV– Compared the clinical symptoms hMPV with age-Compared the clinical symptoms hMPV with age-
matched RSV infected children; matched RSV infected children; RSV-infected RSV-infected found more dyspnea, hypoxemia and feeding found more dyspnea, hypoxemia and feeding difficultiesdifficulties
– Two studies in hospitalized patients show that Two studies in hospitalized patients show that hMPV did not need PICU, contrast to some of hMPV did not need PICU, contrast to some of RSV and Influenza-infected patientsRSV and Influenza-infected patients1,21,2
– Pneumonia was Pneumonia was more oftenmore often associated with RSV associated with RSV1. Viazou S, et al. J Clin Microbiol 2003;41:3043.2. Boivin G, et al. Emerg Infect Dis 2003;9:634.

Age distribution of hMPV and RSV Age distribution of hMPV and RSV (Age <2yrs)(Age <2yrs)(Garcia-Garcia ML, et al. Arch Dis Child 2006;91:290. N=749 (Garcia-Garcia ML, et al. Arch Dis Child 2006;91:290. N=749
Age distribution of hMPV and RSV Age distribution of hMPV and RSV (Age <2yrs)(Age <2yrs)(Garcia-Garcia ML, et al. Arch Dis Child 2006;91:290. N=749 (Garcia-Garcia ML, et al. Arch Dis Child 2006;91:290. N=749
17%
12%
25%
17%
29%
14%
7%
18%
26%
35%
0
5
10
15
20
25
30
35
40
<3 Months 3-6 Months 6-9 Months 9-12 Months >12 Months
hMPVRSV
hMPV 64 cases (14%)hMPV 64 cases (14%)RSV 376 cases (76%)RSV 376 cases (76%)

Monthly Distribution of hMPV and RSV Monthly Distribution of hMPV and RSV (Age <1yr)(Age <1yr)(Ordas J, et al. J Clin Microbiol 2006:2739. N=211)(Ordas J, et al. J Clin Microbiol 2006:2739. N=211)Monthly Distribution of hMPV and RSV Monthly Distribution of hMPV and RSV (Age <1yr)(Age <1yr)(Ordas J, et al. J Clin Microbiol 2006:2739. N=211)(Ordas J, et al. J Clin Microbiol 2006:2739. N=211)
0
10
20
30
40
50
60
70
80
90
100
October
Novem
ber
Decem
ber
Januar
y
Febru
ary
Mar
chApril
RSAhMPV
hMPV 18 cases (16.2%)hMPV 18 cases (16.2%)RSV 96 cases (45.5%)RSV 96 cases (45.5%)

Clinical Manifestation of hMPV (1)Clinical Manifestation of hMPV (1)
• FeverFever 57 - 100%57 - 100%• CoughCough 63 - 100%63 - 100%• RhinorrheaRhinorrhea 46 - 92%46 - 92%• Sore throatSore throat 50 - 59.5%50 - 59.5%• HoarsenessHoarseness 1 - 6%1 - 6%• LacrimationLacrimation 25%25%• ConjunctivitisConjunctivitis 5 - 7%5 - 7%• Influenza-like illnessInfluenza-like illness50 - 53%50 - 53%• Common coldCommon cold 7 - 52%7 - 52%• Otitis mediaOtitis media 12 - 51%12 - 51%• DiarrheaDiarrhea 6 - 37.5%6 - 37.5%• VomitingVomiting 10 - 10 -
48.5%48.5%• Febrile seizureFebrile seizure 16%16%• Truncal rashTruncal rash 10 - 19%10 - 19%• Feeding difficultiesFeeding difficulties 36 - 65%36 - 65%

Clinical Manifestation of hMPV (2)Clinical Manifestation of hMPV (2)
• HypoxiaHypoxia 24 - 47%24 - 47%• WheezeWheeze 0 - 83%0 - 83%• DyspneaDyspnea 28 - 83% 28 - 83% • RetractionsRetractions 60 - 92%60 - 92%• HyperventilationHyperventilation 42%42%• CyanosisCyanosis 4 - 8%4 - 8%• RhinitisRhinitis 27 - 80%27 - 80%• RhinopharyngitisRhinopharyngitis 5%5%• PharyngitisPharyngitis 13 - 39%13 - 39%• LaryngitisLaryngitis 5%5%• TachycardiaTachycardia 23 - 57%23 - 57%• PneumoniaPneumonia 8 - 73%8 - 73%• BronchiolitisBronchiolitis 10 - 67%10 - 67%• Asthma exacerbationAsthma exacerbation 14 - 22%14 - 22%• Bronchitis Bronchitis 0 - 60%0 - 60%

Clinical Manifestation of hMPV (3)Clinical Manifestation of hMPV (3)
• CroupCroup 18%18%• AsthmaAsthma 14%14%• IrritabilityIrritability 43%43%• ApneaApnea 2 - 6%2 - 6%• Noisy breathingNoisy breathing 14%14%• TachypneaTachypnea 67%67%• RhonchiRhonchi 20%20%• Crackles (rales)Crackles (rales) 8 - 100%8 - 100%• SneezingSneezing 45.5%45.5%• Dry mouthDry mouth 23%23%• Enlarged liverEnlarged liver 6%6%• HeadacheHeadache 30%30%• AnorexiaAnorexia 45%45%• DrowsinessDrowsiness 85%85%• LethargyLethargy 26%26%

Lab InvestigationLab Investigation
• Lymphopenia (<1,500 cumm)Lymphopenia (<1,500 cumm) 29%29%
• Neutropenia (<1,00 cumm)Neutropenia (<1,00 cumm) 6.5%6.5%
• Elevated transaminaseElevated transaminase 3.3%3.3%
• WBC (cumm)WBC (cumm) 5,930 - 5,930 - 16,50016,500
• LDH (IU/L)LDH (IU/L) 269 - 649269 - 649
• CRP (mg/dL)CRP (mg/dL) 0.76 - 2.540.76 - 2.54

CXRCXR
• Abnormal CXR 28 - 87%
• Infiltrates 66%
• Air trapping 19%
• Atelectasis 40%
• Other: peribronchial cuffing, pulmonary edema, cardiomegaly, lobar pneumonia (coinfection with bacteria), pleural thickening
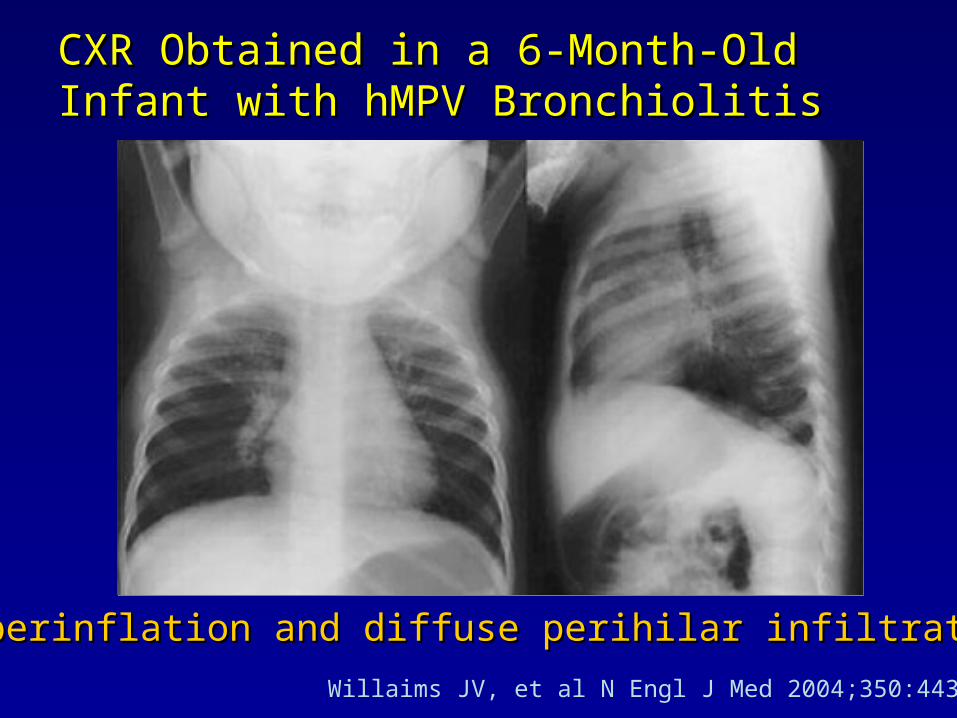
CXR Obtained in a 6CXR Obtained in a 6--MonthMonth--Old Infant with Old Infant with hMPV BronchiolitishMPV Bronchiolitis
Hyperinflation and diffuse perihilar infiltrates Hyperinflation and diffuse perihilar infiltrates
Willaims JV, et al N Engl J Med 2004;350:443-450

Pathology of hMPVPathology of hMPV
• Pathology specimens Pathology specimens of hMPV-positiveof hMPV-positive– Exam by light and Exam by light and
electron microscopyelectron microscopy– BALBAL
• BAL showedBAL showed– Epithelial degenerative Epithelial degenerative
changes and eosinophilic changes and eosinophilic cytoplasmic inclusions cytoplasmic inclusions within epithelial cells, within epithelial cells, multinucleated giant cell, multinucleated giant cell, histocytosishistocytosis
Vargas SO, et al. Pediatr Dev Pathol 2004;7:478
Red cytoplasmic inclusionRed cytoplasmic inclusion
Degenerative epithelial cellsDegenerative epithelial cells
Multi nucleatedMulti nucleatedgiant cellgiant cell

Pathology of hMPVPathology of hMPV
• Lung biopsy showedLung biopsy showed– Lipoid pneumoniaLipoid pneumonia– Chronic airway Chronic airway
inflammationinflammation– Intraalveolar foamyIntraalveolar foamy– Cholesteral cleftsCholesteral clefts– Hemosiderin-laden Hemosiderin-laden
macrophagesmacrophages
Vargas SO, et al. Pediatr Dev Pathol 2004;7:478
ManagementManagement
• Supportive care and managing airway Supportive care and managing airway obstructionobstruction
• Antiviral therapyAntiviral therapy
• Prevention Prevention

Supportive CareSupportive Care
• Administer humidified oxygenAdminister humidified oxygen
• Nasal suctioning to clear upper airwayNasal suctioning to clear upper airway
• Monitor for apnea, hypoxia and impending Monitor for apnea, hypoxia and impending respiratory failurerespiratory failure
• Normalize body temperatureNormalize body temperature
• Rehydrate with oral or intravenous fluidsRehydrate with oral or intravenous fluids
• Monitor hydration statusMonitor hydration status

Managing Airway Obstruction and Managing Airway Obstruction and Antiviral TherapyAntiviral Therapy
• BronchodilatorsBronchodilators
• CorticosteroidsCorticosteroids
• RibavirinRibavirin
• Intravenous immunoglobulinIntravenous immunoglobulin

Effect of Ribavirin and Glucocoticoid Treatment in Effect of Ribavirin and Glucocoticoid Treatment in Mouse Model of hMPV infectionMouse Model of hMPV infection
Effect of Ribavirin and Glucocoticoid Treatment in Effect of Ribavirin and Glucocoticoid Treatment in Mouse Model of hMPV infectionMouse Model of hMPV infection
A. Mean viral titers in A. Mean viral titers in lungslungs of hMPV-infected mice (BALB/c). On day 5 postinfection
B. Lung inflammationB. Lung inflammation in hMPV-infected mice evaluation with mean histopathological scores
Hamelin ME, et al Antimicrob Agents Chemother 2006;50:774

Data of ManagementData of Management
• Oxygen administrationOxygen administration 24.3 - 34.3%24.3 - 34.3%• BronchodilatorBronchodilator 30 - 32.4%30 - 32.4%• Corticosteroids Corticosteroids 8.1 - 17%8.1 - 17%• Antibiotics Antibiotics 22.2 - 94%22.2 - 94%• Mechanical ventilationMechanical ventilation 2%2%• PICUPICU 2%2%
• Duration of fever:Duration of fever: 4 (2-7) days 4 (2-7) days• Duration of hospitalization:Duration of hospitalization: 4 (3-7) days 4 (3-7) days• School absence, median (range): 10 (3-15) daysSchool absence, median (range): 10 (3-15) days
1. Wang SM, et al Clin Microbiol Infect 2006;12:1221, 2. Foulongne V, et al. Pediatr Infect Dis J 2006;25:354, 3. Takao S, et al. Jpn J Infect Dis 2003;56:127, 4. Wolf DG, et al. Pediatr Infect Dis J 2006;25:320

Clinical and Socioeconomic Impact Clinical and Socioeconomic Impact Among Household Contacts Among Household Contacts
• Disease similar to infected child (%)Disease similar to infected child (%) 16 (12.5)16 (12.5)
• Additional medical visits (%)Additional medical visits (%) 16 (12.5)16 (12.5)
• Antipyretic prescriptions (%)Antipyretic prescriptions (%) 14 (10.9)14 (10.9)
• Antibiotic prescriptions (%)Antibiotic prescriptions (%) 6 (4.7) 6 (4.7)
• Lost working days, median (range)Lost working days, median (range) 4 (2-10) 4 (2-10)
• Lost of school days, median (range)Lost of school days, median (range) 4 (3-15) 4 (3-15)
Bosis S, et al. J med Virol 2005;75:101.

PreventionPrevention
• Effort to reduce spread include:Effort to reduce spread include:– Limiting contact with infected patientsLimiting contact with infected patients– Removal from day care and group settingRemoval from day care and group setting– Proper hygiene: frequent hand washingProper hygiene: frequent hand washing– Disinfecting surface exposed to infectious Disinfecting surface exposed to infectious
secretionssecretions– Cohorting hospitalized patientsCohorting hospitalized patients
• VaccinationVaccination• ImmunoprophylaxisImmunoprophylaxis

Community-Acquired MRSACommunity-Acquired MRSA(CA-MRSA)(CA-MRSA)

CA-MRSA: DefinitionCA-MRSA: Definition
• CDC:CDC: diagnosis made in the community diagnosis made in the community setting or by culture positive for MRSA setting or by culture positive for MRSA within 48 hrs after admission to hospitalwithin 48 hrs after admission to hospital– It is known that patients may be colonized It is known that patients may be colonized
with HA-MRSA for year before developing with HA-MRSA for year before developing infectioninfection
– Nosocomial outbreak of CA-MRSA have been Nosocomial outbreak of CA-MRSA have been reports (MMWR Mar 31, 2006;55:329)reports (MMWR Mar 31, 2006;55:329)
http://www.cdc.gov/ncidod/hip/ARESIST/mrsa_comm_faq.htm

• Molecular marker (Lyon) for definitionMolecular marker (Lyon) for definition
1.1. The Panton-Valentine leukocidin (PVL) The Panton-Valentine leukocidin (PVL) genesgenes
2.2. SCC mec IVSCC mec IV
• Molecular methodsMolecular methods
1.1. Pulsed-field gel electrophoresis (PFGE)Pulsed-field gel electrophoresis (PFGE)
2.2. Multilocus sequence typing (MLST)Multilocus sequence typing (MLST)– PCR-based method CA-MRSA clones; ST1 PCR-based method CA-MRSA clones; ST1
(USA 400), ST8 (USA 300)(USA 400), ST8 (USA 300)
CA-MRSA: DefinitionCA-MRSA: Definition
Vandenesch F et al. Emerg Infect Dis 2003;9:978

CA-MRSA: HistoryCA-MRSA: History
• S aureusS aureus is gram-positive coccid bacterium, is gram-positive coccid bacterium, originally susceptible to penicillinoriginally susceptible to penicillin
• 1940s1940s: Penicillinase-producing strains appear: Penicillinase-producing strains appear
• 19591959: Methicillin introduced: Methicillin introduced
• 19611961: MRSA emerged as nosocomial : MRSA emerged as nosocomial pathogen, first at UKpathogen, first at UK
• Early 1990sEarly 1990s: CA-MRSA infections reported: CA-MRSA infections reported

Methicillin ResistanceMethicillin Resistance• Altered penicillin-binding Altered penicillin-binding
proteins (PBP2a) that had proteins (PBP2a) that had markly reduced affinity for all markly reduced affinity for all beta-lactam antibioticsbeta-lactam antibiotics
• PBP2aPBP2a is encoded by the is encoded by the mecAmecA gene which carried on gene which carried on the mobile DNA element (the the mobile DNA element (the staphylococcal cassette staphylococcal cassette chromosome chromosome mecmec (SCC (SCCmecmec))
• The other important component of SCCThe other important component of SCCmecmec– The chromosome cassette recombinase (The chromosome cassette recombinase (ccrccr) genes encodes ) genes encodes
for proteins that enable precise intregation into and excision for proteins that enable precise intregation into and excision from specific site of from specific site of S. aureusS. aureus chromosome ( chromosome (attBsccattBscc))
Foster TJ. J Clin Invest 2004;114:1693
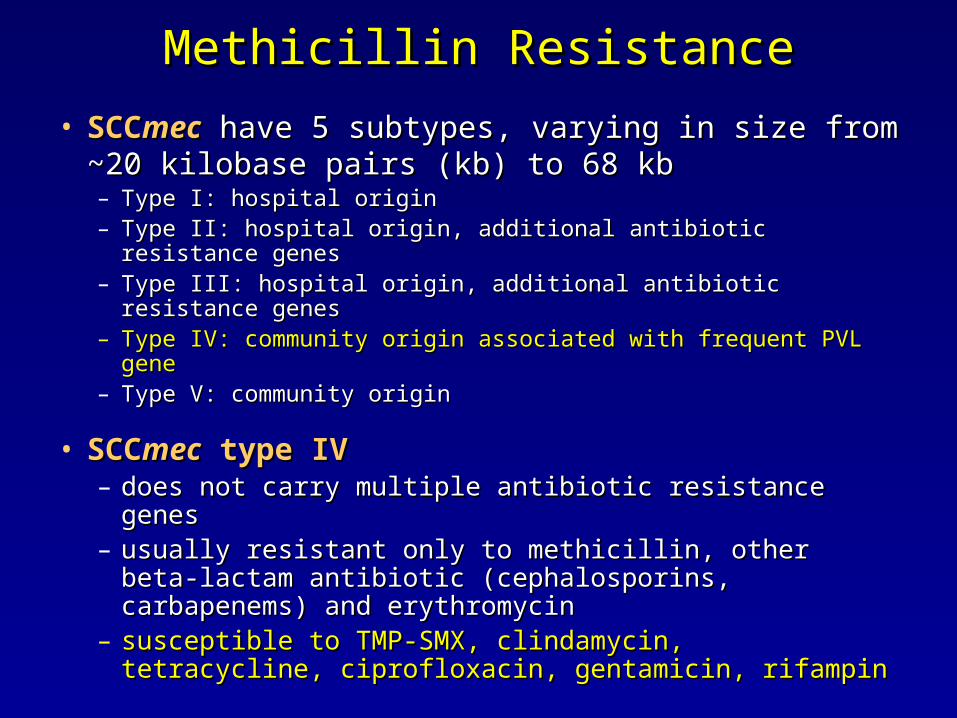
• SCCSCCmecmec have 5 subtypes, varying in size from have 5 subtypes, varying in size from ~20 kilobase pairs (kb) to 68 kb~20 kilobase pairs (kb) to 68 kb– Type I: hospital originType I: hospital origin– Type II: hospital origin, additional antibiotic resistance genesType II: hospital origin, additional antibiotic resistance genes– Type III: hospital origin, additional antibiotic resistance genesType III: hospital origin, additional antibiotic resistance genes– Type IV: community origin associated with frequent PVL geneType IV: community origin associated with frequent PVL gene– Type V: community originType V: community origin
• SCCSCCmecmec type IV type IV– does not carry multiple antibiotic resistance genesdoes not carry multiple antibiotic resistance genes– usually resistant only to methicillin, other beta-lactam usually resistant only to methicillin, other beta-lactam
antibiotic (cephalosporins, carbapenems) and antibiotic (cephalosporins, carbapenems) and erythromycinerythromycin
– susceptible to TMP-SMX, clindamycin, tetracycline, susceptible to TMP-SMX, clindamycin, tetracycline, ciprofloxacin, gentamicin, rifampinciprofloxacin, gentamicin, rifampin
Methicillin ResistanceMethicillin Resistance

Virulence FactorsVirulence FactorsSCCmec Resistant to methicillin
Collagen-adhesin protein Adherence to host cell EF,NP,arthritis,osteomyelitis
Bacteriocin of SA (bsa) interspecies EF
Superantigen
-Enterotoxin
-Staph enterotoxin
A,B,C,G,H
Activation of T cells EF, NP, TSS-like illness
-Staph exotoxin T Possible against immunity
Pore-forming toxins
-PVL (LukSPV+LukFPV)
-LukE+LukD
LukE+LukDv
-hemolysin
Necrosis, edema
Destruction of intestinal microvilli
Necrosis
Necrosis, vascular leak, shock
EF,NP
Postantibiotic diarrhea
EF
EF, NP, Bullous impetigo
Exfloliative toxin A,B
EF=epidermic furunculosis, NP=necrotizing pneumonia, TSS=toxic shock syndrome

PVLPVL
• An extracellular bicomponent An extracellular bicomponent toxintoxin that targets and induces that targets and induces leukocyte death with release leukocyte death with release of cytokines and intracellular of cytokines and intracellular proteases by creating pores in proteases by creating pores in the cell membranethe cell membrane
• PVL genes are present in the PVL genes are present in the majority of CA-MRSA isolatedmajority of CA-MRSA isolated
• Associated skin and soft Associated skin and soft tissue infection (furunculosis, tissue infection (furunculosis, abscesses) or more rarely abscesses) or more rarely necrotizing pneumonianecrotizing pneumonia
Agarose gel electrophoresis Agarose gel electrophoresis demonstrative PVL demonstrative PVL
• Lane 1:Lane 1: molecular weight marker molecular weight marker• Lane 2:Lane 2: positive PVL control strain positive PVL control strain
of of S aureusS aureus• Lane 3:Lane 3: negative PVL control strain negative PVL control strain
of of S aureusS aureus• Lane 4:Lane 4: negative clinical isolate of negative clinical isolate of S S
aureusaureus• Lane 5:Lane 5: patient isolate of patient isolate of S aureusS aureus
demonstrating a positive PCR demonstrating a positive PCR product representing PVLproduct representing PVL

Burden of MRSABurden of MRSA• Increased hospitalization (3 times)hospitalization (3 times)
– MRSA infections increase the median length of MRSA infections increase the median length of hospital stay for nosocomial infections (median: 12 hospital stay for nosocomial infections (median: 12 days for MRSA vs. 4 days for MSSA)days for MRSA vs. 4 days for MSSA)
• Increased cost (3 times)Increased cost (3 times)– MRSA infections increase per-patient hospital MRSA infections increase per-patient hospital
compared with MSSA (US$48,824 vs. US$14,141)compared with MSSA (US$48,824 vs. US$14,141)
• Increased mortality (3 times)Increased mortality (3 times)– Nosocomial MRSA infections are associated with Nosocomial MRSA infections are associated with
higher mortality compared with MSSA (21% vs. 8%)higher mortality compared with MSSA (21% vs. 8%)Abramson MA, Sexton DJ. Infect Control Hosp Epidemiol 1999;20:408, Engemann JJ et al. Clin Infect Dis 2003;36:592, Rubin RJ et al. Emerg Infect Dis 1999;5:9
CA-MRSA: EpidemiologyCA-MRSA: Epidemiology
• The first report in childrenThe first report in children (Herold BC, et al.)* (Herold BC, et al.)*– Prevalence of CA-MRSA without risk factors Prevalence of CA-MRSA without risk factors
increased from 10/10,000 in 1988-90 to 259/10,000 in increased from 10/10,000 in 1988-90 to 259/10,000 in 1993-5 (8 cases and 35 cases)1993-5 (8 cases and 35 cases)
– Cellulitis (55%), abscess (27%), pneumonia (13.5%)Cellulitis (55%), abscess (27%), pneumonia (13.5%)
• CA-MRSA outbreaks have been reported CA-MRSA outbreaks have been reported throughout the worldthroughout the world– USA, Canada, Brazil, Uruguay, Belgium, Denmark, USA, Canada, Brazil, Uruguay, Belgium, Denmark,
France, Germany, Greece, Holland, Latvia, Norway France, Germany, Greece, Holland, Latvia, Norway Sweden, Switzerland, UK, Taiwan, Korea, HK, Sweden, Switzerland, UK, Taiwan, Korea, HK, Australia, NewzelandAustralia, Newzeland
Harold BC, et al. JAMA 1998;279(8):593
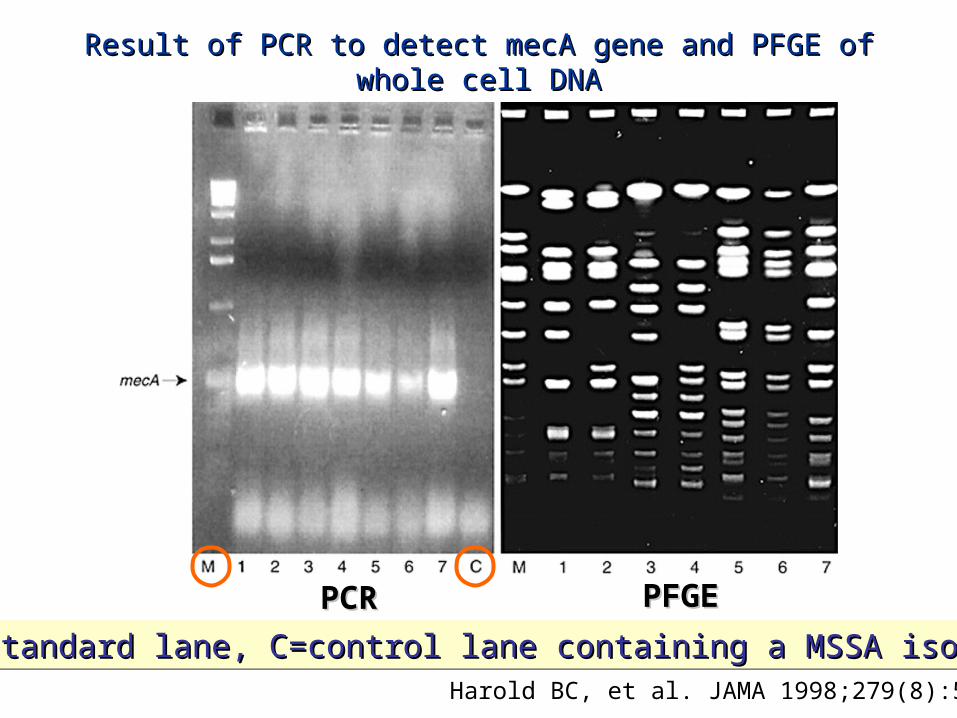
Result of PCR to detect mecA gene and PFGE of whole cell DNAResult of PCR to detect mecA gene and PFGE of whole cell DNA
PCRPCR PFGEPFGE
Harold BC, et al. JAMA 1998;279(8):593
M=standard lane, C=control lane containing a MSSA isolateM=standard lane, C=control lane containing a MSSA isolateM=standard lane, C=control lane containing a MSSA isolateM=standard lane, C=control lane containing a MSSA isolate

CA-MRSA: EpidemiologyCA-MRSA: Epidemiology
• Four pediatric deaths from CA-MRSA – Four pediatric deaths from CA-MRSA – Minnesota and North Dakota, 1997-99 (MMWR, Minnesota and North Dakota, 1997-99 (MMWR, Aug 20 1999:48;707)Aug 20 1999:48;707)
• Case reportsCase reports– 7-year-old black girl7-year-old black girl with high fever and Rt groin pain, with high fever and Rt groin pain,
she underwent surgical drainage for Rt hip infection she underwent surgical drainage for Rt hip infection and treated with and treated with cefazolin.cefazolin. On 3 On 3rdrd day antimicrobial day antimicrobial was changed to vancomycin when cultures of blood was changed to vancomycin when cultures of blood and joint fluid grew MRSA. Her course was and joint fluid grew MRSA. Her course was complicated by ARDS, pneumonia and empyema. complicated by ARDS, pneumonia and empyema. She died from pulmonary hemorrhage after 5-weeks She died from pulmonary hemorrhage after 5-weeks of hospitalizationof hospitalization

• Case reports (cont.)Case reports (cont.)– 16-month-old girl16-month-old girl with shock, high fever, seizure, diffuse with shock, high fever, seizure, diffuse
petechial rash. She was treated with petechial rash. She was treated with ceftriaxoneceftriaxone but but developed respiratory failure and cardiac arrest and died developed respiratory failure and cardiac arrest and died within 2 hourswithin 2 hours
– 13-year-old girl13-year-old girl with fever, hemoptysis and respiratory with fever, hemoptysis and respiratory distress. CXR revealed LLL infiltrate and pleural effusion. distress. CXR revealed LLL infiltrate and pleural effusion. She was treated with She was treated with cefriaxone and nafcillincefriaxone and nafcillin. Within 5 . Within 5 hours of arriving at hospital, she become hypotensive and hours of arriving at hospital, she become hypotensive and was intubated and treated with was intubated and treated with vancomycin and cefotaximevancomycin and cefotaxime. . She died on the 7She died on the 7thth hospital day from cerebral edema and hospital day from cerebral edema and MOFSMOFS
– 12-month-old boy12-month-old boy with bronchiolitis, vomiting, and with bronchiolitis, vomiting, and dehydration. He had high fever and petechial rash. On 2dehydration. He had high fever and petechial rash. On 2ndnd hospital day he has large Rt pleural effusion and treated with hospital day he has large Rt pleural effusion and treated with vancomycin, cefuroxime and ICDvancomycin, cefuroxime and ICD. He developed respiratory . He developed respiratory failure and hypotension the following day and died failure and hypotension the following day and died
CA-MRSA: EpidemiologyCA-MRSA: Epidemiology
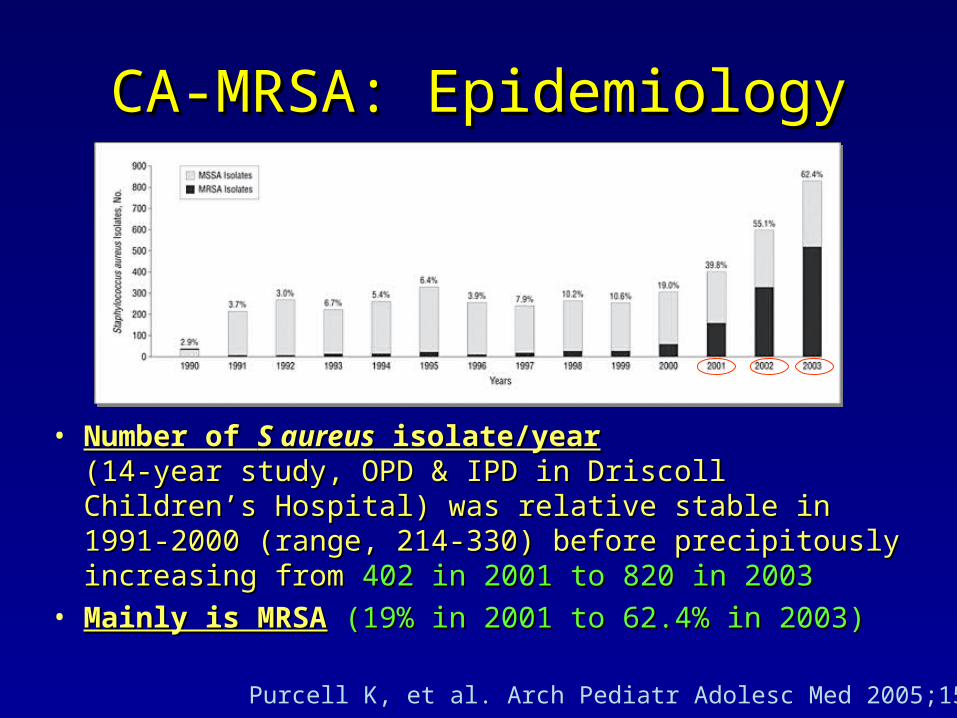
• Number of Number of S aureusS aureus isolate/year isolate/year (14-year study, OPD & IPD in Driscoll Children’s Hospital) (14-year study, OPD & IPD in Driscoll Children’s Hospital) was relative stable in 1991-2000 (range, 214-330) before was relative stable in 1991-2000 (range, 214-330) before precipitously increasing from precipitously increasing from 402 in 2001 to 820 in 2003402 in 2001 to 820 in 2003
• Mainly is MRSAMainly is MRSA (19% in 2001 to 62.4% in 2003)(19% in 2001 to 62.4% in 2003)
Purcell K, et al. Arch Pediatr Adolesc Med 2005;159:980

CA-MRSA: EpidemiologyCA-MRSA: Epidemiology
• 1,002 MRSA cases were CA-MRSA 982 cases (92.6%)1,002 MRSA cases were CA-MRSA 982 cases (92.6%)• Mean age was 7.9 yearsMean age was 7.9 years and 51.3% were male and 51.3% were male• Number of MRSA case/year was Number of MRSA case/year was 43 cases in 2000 to 43 cases in 2000 to
467 cases in 2003467 cases in 2003, this increase was solely by rise in , this increase was solely by rise in number of CA-MRSA infectionnumber of CA-MRSA infection
Purcell K, et al. Arch Pediatr Adolesc Med 2005;159:980

CA-MRSA: Risk FactorsCA-MRSA: Risk Factors
• ChildrenChildren• Overcrowed facilities: prisoners, militrary Overcrowed facilities: prisoners, militrary
recruitsrecruits• Closed contact sports: football, wrestling, Closed contact sports: football, wrestling,
fencingfencing• Low socioecomomic status, lack of sanitationLow socioecomomic status, lack of sanitation• Intravenous drugs abusers (IVDA)Intravenous drugs abusers (IVDA)• Native Americans, Aboriginal groups etc.Native Americans, Aboriginal groups etc.• Man who have sex with manMan who have sex with man

CA-MRSA: Clinical ManifestationsCA-MRSA: Clinical Manifestations
• Skin and Soft tissue infections (~70-90%)Skin and Soft tissue infections (~70-90%)– Cellulitis, Folliculitis, Furunculosis, Abscesses, Cellulitis, Folliculitis, Furunculosis, Abscesses,
Impetigo, Wound InfectionImpetigo, Wound Infection
• Invasive Infections (~10-30%)Invasive Infections (~10-30%)– Bacteremia, Toxic Shock SyndromeBacteremia, Toxic Shock Syndrome– Musculoskeletal InfectionsMusculoskeletal Infections
• Osteomyelitis, Septic arthritis, Bursitis, Osteomyelitis, Septic arthritis, Bursitis, Pyomyositis, FasciitisPyomyositis, Fasciitis
– Pneumonia, Empyema (~30-50%)Pneumonia, Empyema (~30-50%)
• Others: Lymphadenitis, Endocarditis, etc.Others: Lymphadenitis, Endocarditis, etc.
Kaplan S. Semin Pediatr Infect Dis 2006;17:113
CA-MRSA: PneumoniaCA-MRSA: Pneumonia
• Clinical findings are no different with other organisms such as S pneumoniae
• Duration of hospitalization was longer than CA-MSSA (mean, 19 vs.14 days)
• Children with primary pneumonia are younger than secondary pneumonia from infections at other sites (mean, 3.5 vs. 9.9 years)
• CA-MRSA have been associated with necrotizing pneumonia, esp. coinfected with virus (influenza or parainfluenza)
Kaplan S. Semin Pediatr Infect Dis 2006;17:113Gonzalez BE, et al. Clin Infect Dis 2005;41:583

CA-MRSA: PneumoniaCA-MRSA: Pneumonia
Necrotizing tracheobronchitis:1. sloughing of bronchial mucosa2. extensive necrosis of subepithelial connective tissue3. necrotic debris
Necrotizing pneumonia:1. patchy areas of hemorrhage2. extensive intraalveolar hemorrhage admixed with neutrophil infiltrates3. karyorrhectic debrisGonzalez BE, et al. Clin Infect Dis 2005;41:583

CA-MRSA: TreatmentCA-MRSA: Treatment
• Hospitalized, non-life-treatening invasive Hospitalized, non-life-treatening invasive or noninvasive infections and without toxic or noninvasive infections and without toxic appearanceappearance– IV ClindamycinIV Clindamycin + (I&D, if abscess is present) + (I&D, if abscess is present)
• Criticallly ill with life-treatening invasive Criticallly ill with life-treatening invasive infectionsinfections– IV Vancomycin* or IV ClindamycinIV Vancomycin* or IV Clindamycin##
– IV Clindamycin + GentamicinIV Clindamycin + Gentamicin*alternative regimen: Vancomycin + Cloxacillin, Vancomycin + 3*alternative regimen: Vancomycin + Cloxacillin, Vancomycin + 3rdrd Cephalosporin Cephalosporin#suggestion to use Vancomycin in life-treatening until known negative D-test#suggestion to use Vancomycin in life-treatening until known negative D-test
CA-MRSA: ClindamycinCA-MRSA: Clindamycin
• In patients with bacteremia, complicated In patients with bacteremia, complicated pneumonia and musculoskeletal infectionspneumonia and musculoskeletal infections– Dose:Dose: 40 mg/kg/day IV 40 mg/kg/day IV– Duration:Duration: median, 20 days (range, 10-56 days) median, 20 days (range, 10-56 days)– Complication:Complication: relatively rare relatively rare Clostridium difficileClostridium difficile
enteritis, loose stools or diarrhea is most enteritis, loose stools or diarrhea is most common, rashcommon, rash
– Inducible resistance to clindamycin detected by Inducible resistance to clindamycin detected by double-disk diffusion test (D-test)double-disk diffusion test (D-test)
Martinez-Aguilar G, et al. Pediatr Infect Dis J 2003;22:593
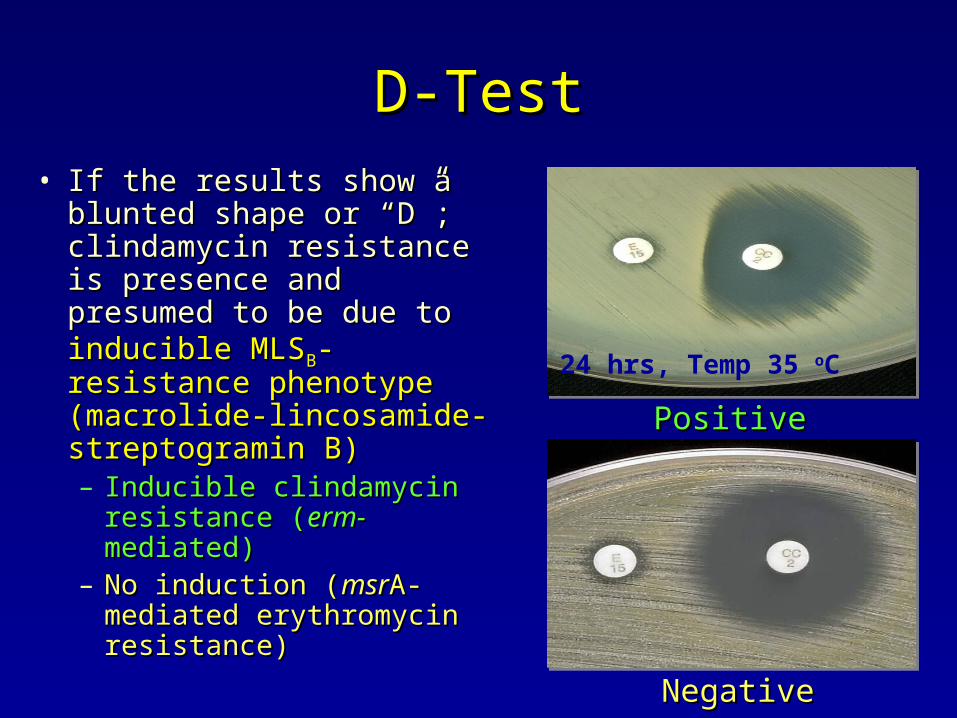
D-TestD-Test• If the results show a If the results show a
blunted shape or “D”; blunted shape or “D”; clindamycin resistance is clindamycin resistance is presence and presumed to presence and presumed to be due to be due to inducible MLSinducible MLSBB--resistance phenotyperesistance phenotype (macrolide-lincosamide-(macrolide-lincosamide-streptogramin B)streptogramin B)– Inducible clindamycin Inducible clindamycin
resistance (resistance (erm-erm-mediated)mediated)– No induction (No induction (msrmsrA-A-
mediated erythromycin mediated erythromycin resistance)resistance)
PositivePositive
NegativeNegative
24 hrs, Temp 35 oC

ConclusionsConclusions
• Available evidence suggests that CA-MRSA Available evidence suggests that CA-MRSA is an emerging problem in pediatricsis an emerging problem in pediatrics
• Clinicians should be aware that therapy with Clinicians should be aware that therapy with beta-lactam antimicrobials can no longer be beta-lactam antimicrobials can no longer be relied on as the sole empiric therapy for relied on as the sole empiric therapy for severe illness patients whose infections may severe illness patients whose infections may be CA-MRSAbe CA-MRSA
• What is the CA-MRSA situation in Thailand?What is the CA-MRSA situation in Thailand?
Top Related